
Real-World, Multicenter Case Series of Patients Treated with Isavuconazole for Invasive Fungal Disease in China

Abstract
:1. Introduction
2. Materials and Methods
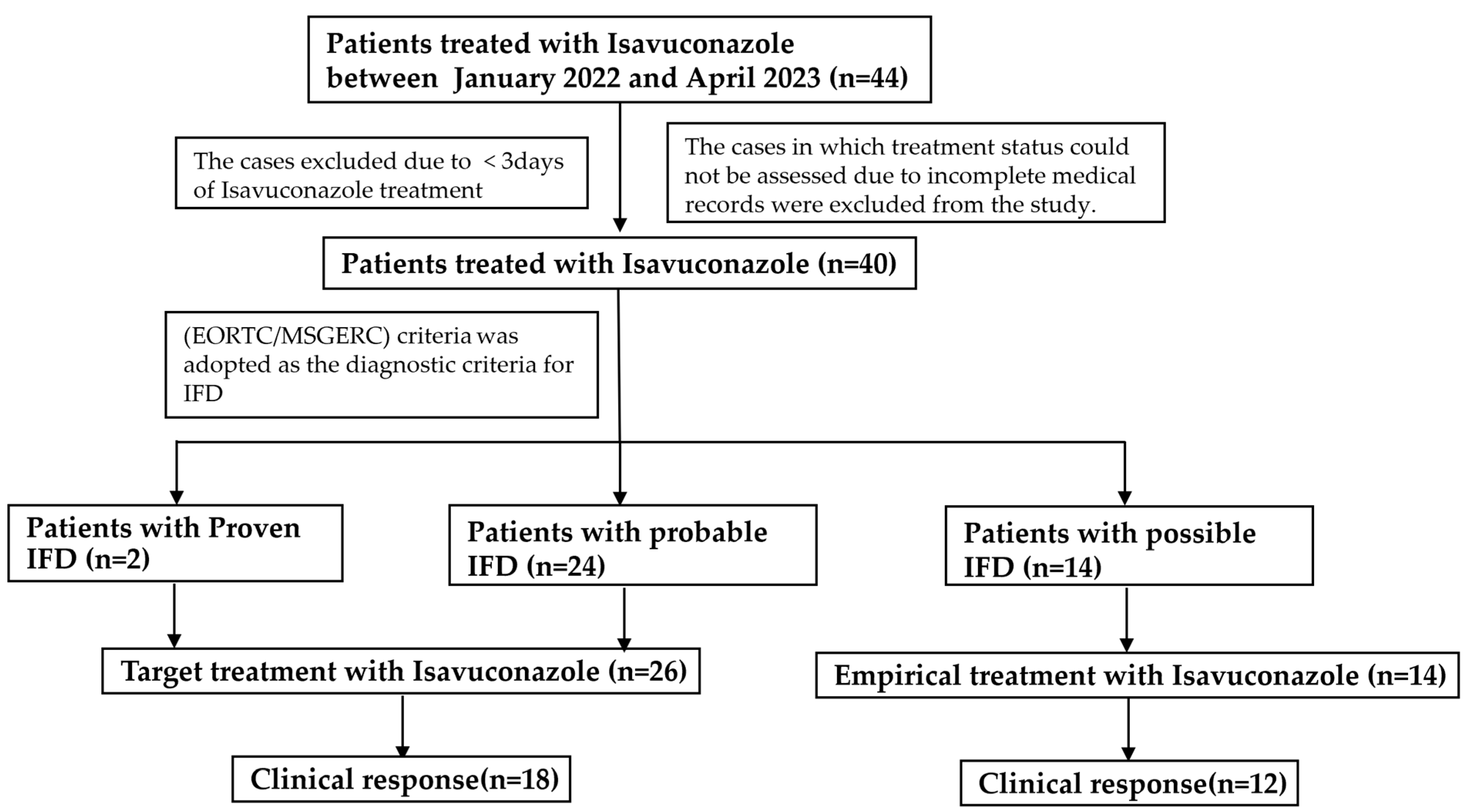
2.1. Patient Population
2.2. Definitions
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Patients Included in the Study
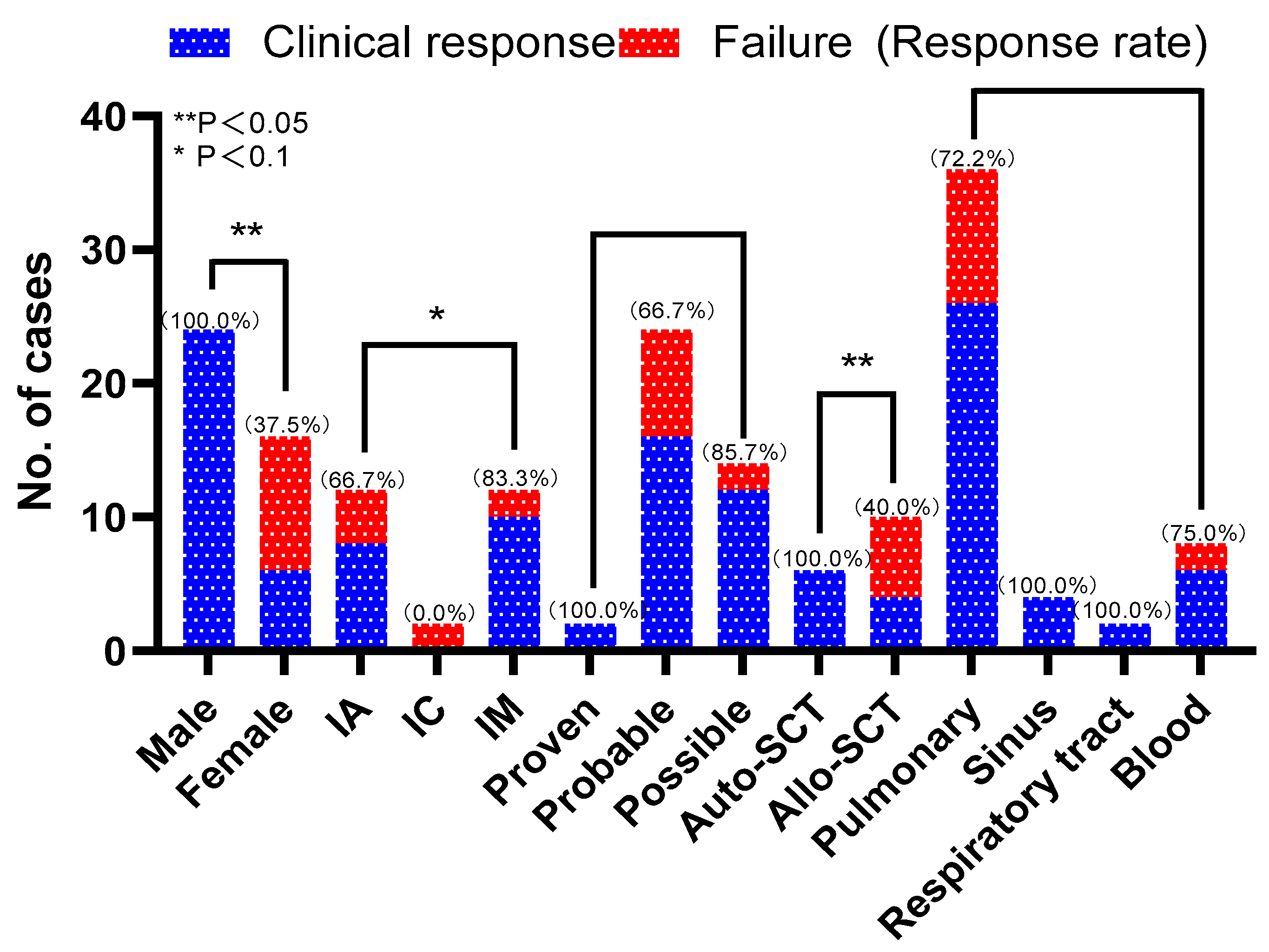
3.2. Treatment of ISA and Occurrence of IFD
3.3. Side Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Chinese Association Hematologists; Chinese Invasive Fungal Infection Working Group. The Chinese guidelines for the diagnosis and treatment of invasive fungal disease in patients with hematological disorders and cancers (the 6th revision). Zhonghua Nei Ke Za Zhi 2020, 59, 754–763. [Google Scholar] [CrossRef]
- Gow, N.A.R.; Johnson, C.; Berman, J.; Coste, A.T.; Cuomo, C.A.; Perlin, D.S.; Bicanic, T.; Harrison, T.S.; Wiederhold, N.; Bromley, M.; et al. The importance of antimicrobial resistance in medical mycology. Nat. Commun. 2022, 13, 5352. [Google Scholar] [CrossRef] [PubMed]
- Lamoth, F.; Chung, S.J.; Damonti, L.; Alexander, B.D. Changing Epidemiology of Invasive Mold Infections in Patients Receiving Azole Prophylaxis. Clin. Infect. Dis. 2017, 64, 1619–1621. [Google Scholar] [CrossRef]
- Sun, Y.; Huang, H.; Chen, J.; Li, J.; Ma, J.; Li, J.; Liang, Y.; Wang, J.; Li, Y.; Yu, K.; et al. Invasive fungal infection in patients receiving chemotherapy for hematological malignancy: A multicenter, prospective, observational study in China. Tumour Biol. 2015, 36, 757–767. [Google Scholar] [CrossRef]
- Patterson, T.F.; Thompson, G.R., 3rd; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 63, e1–e60. [Google Scholar] [CrossRef]
- Garcia-Vidal, C.; Alastruey-Izquierdo, A.; Aguilar-Guisado, M.; Carratalà, J.; Castro, C.; Fernández-Ruiz, M.; Aguado, J.M.; Fernández, J.M.; Fortún, J.; Garnacho-Montero, J.; et al. Executive summary of clinical practice guideline for the management of invasive diseases caused by Aspergillus: 2018 Update by the GEMICOMED-SEIMC/REIPI. Enfermedades Infecc. Y Microbiol. Clin. Engl. Ed. 2019, 37, 535–541. [Google Scholar] [CrossRef]
- Cornely, O.A.; Alastruey-Izquierdo, A.; Arenz, D.; Chen, S.C.A.; Dannaoui, E.; Hochhegger, B.; Hoenigl, M.; Jensen, H.E.; Lagrou, K.; Lewis, R.E.; et al. Global guideline for the diagnosis and management of mucormycosis: An initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect. Dis. 2019, 19, e405–e421. [Google Scholar] [CrossRef]
- Koehler, P.; Bassetti, M.; Chakrabarti, A.; Chen, S.C.A.; Colombo, A.L.; Hoenigl, M.; Klimko, N.; Lass-Flörl, C.; Oladele, R.O.; Vinh, D.C.; et al. Defining and managing COVID-19-associated pulmonary aspergillosis: The 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect. Dis. 2021, 21, e149–e162. [Google Scholar] [CrossRef]
- Anti-infection Group of Hematology Branch of Chinese Medical Association; Hematology Hospital, Chinese Academy of Medical Sciences; Department of Hematology, Nanfang Hospital, Southern Medical University. Consensus recommendations for the clinical application of isavuconazole. Lin Chuang Xue Ye Xue Za Zhi 2023, 36, 295–302. [Google Scholar] [CrossRef]
- Medical Mycology Society of Chinese Medicine and Education Association; Chinese Society of Hematology, Chinese Medical Association. Chinese expert consensus for invasive fungal disease in patients after hematopoietic stem cell transplantation. Zhonghua Xue Ye Xue Za Zhi 2023, 44, 92–97. [Google Scholar] [CrossRef]
- Medical Mycology Society of Chinese Medicine and Education Association; Chinese Mucormycosis Expert Consensus Group. Expert consensus on diagnosis and management of mucormycosis in China. Zhonghua Nei Ke Za Zhi 2023, 62, 597–605. [Google Scholar] [CrossRef]
- Ananda-Rajah, M.R.; Kontoyiannis, D. Isavuconazole: A new extended spectrum triazole for invasive mold diseases. Future Microbiol. 2015, 10, 693–708. [Google Scholar] [CrossRef] [PubMed]
- Decembrino, N.; Perruccio, K.; Zecca, M.; Colombini, A.; Calore, E.; Muggeo, P.; Soncini, E.; Comelli, A.; Molinaro, M.; Goffredo, B.M.; et al. A Case Series and Literature Review of Isavuconazole Use in Pediatric Patients with Hemato-oncologic Diseases and Hematopoietic Stem Cell Transplantation. Antimicrob. Agents Chemother. 2020, 64, e01783-19. [Google Scholar] [CrossRef] [PubMed]
- Marty, F.M.; Cornely, O.A.; Mullane, K.M.; Ostrosky-Zeichner, L.; Maher, R.M.; Croos-Dabrera, R.; Lu, Q.; Lademacher, C.; Oren, I.; Schmitt-Hoffmann, A.H.; et al. Isavuconazole for treatment of invasive fungal diseases caused by more than one fungal species. Mycoses 2018, 61, 485–497. [Google Scholar] [CrossRef]
- Maertens, J.A.; Raad, I.I.; Marr, K.A.; Patterson, T.F.; Kontoyiannis, D.P.; Cornely, O.A.; Bow, E.J.; Rahav, G.; Neofytos, D.; Aoun, M.; et al. Isavuconazole versus voriconazole for primary treatment of invasive mould disease caused by Aspergillus and other filamentous fungi (SECURE): A phase 3, randomised-controlled, non-inferiority trial. Lancet 2016, 387, 760–769. [Google Scholar] [CrossRef]
- Dagher, H.; Hachem, R.; Chaftari, A.M.; Jiang, Y.; Ali, S.; Deeba, R.; Shah, S.; Raad, I. Real-World Use of Isavuconazole as Primary Therapy for Invasive Fungal Infections in High-Risk Patients with Hematologic Malignancy or Stem Cell Transplant. J. Fungi 2022, 8, 74. [Google Scholar] [CrossRef]
- Cattaneo, C.; Busca, A.; Gramegna, D.; Farina, F.; Candoni, A.; Piedimonte, M.; Fracchiolla, N.; Pagani, C.; Principe, M.I.D.; Tisi, M.C.; et al. Isavuconazole in Hematological Patients: Results of a Real-Life Multicentre Observational Seifem Study. HemaSphere 2019, 3, e320. [Google Scholar] [CrossRef]
- Monforte, A.; Los-Arcos, I.; Martín-Gómez, M.T.; Campany-Herrero, D.; Sacanell, J.; Berastegui, C.; Márquez-Algaba, E.; Sempere, A.; Nuvials, X.; Deu, M.; et al. Safety and Effectiveness of Isavuconazole Treatment for Fungal Infections in Solid Organ Transplant Recipients (ISASOT Study). Microbiol. Spectr. 2022, 10, e0178421. [Google Scholar] [CrossRef]
- Fernández-Ruiz, M.; Bodro, M.; Gutiérrez Martín, I.; Rodriguez-Álvarez, R.; Ruiz-Ruigómez, M.; Sabé, N.; López-Viñau, T.; Valerio, M.; Illaro, A.; Fortún, J.; et al. Isavuconazole for the Treatment of Invasive Mold Disease in Solid Organ Transplant Recipients: A Multicenter Study on Efficacy and Safety in Real-life Clinical Practice. Transplantation 2023, 107, 762–773. [Google Scholar] [CrossRef]
- Zurl, C.; Waller, M.; Schwameis, F.; Muhr, T.; Bauer, N.; Zollner-Schwetz, I.; Valentin, T.; Meinitzer, A.; Ullrich, E.; Wunsch, S.; et al. Isavuconazole Treatment in a Mixed Patient Cohort with Invasive Fungal Infections: Outcome, Tolerability and Clinical Implications of Isavuconazole Plasma Concentrations. J. Fungi 2020, 6, 90. [Google Scholar] [CrossRef] [PubMed]
- Marty, F.M.; Ostrosky-Zeichner, L.; Cornely, O.A.; Mullane, K.M.; Perfect, J.R.; Thompson, G.R., 3rd; Alangaden, G.J.; Brown, J.M.; Fredricks, D.N.; Heinz, W.J.; et al. Isavuconazole treatment for mucormycosis: A single-arm open-label trial and case-control analysis. Lancet Infect. Dis. 2016, 16, 828–837. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [PubMed]
- Segal, B.H.; Herbrecht, R.; Stevens, D.A.; Ostrosky-Zeichner, L.; Sobel, J.; Viscoli, C.; Walsh, T.J.; Maertens, J.; Patterson, T.F.; Perfect, J.R.; et al. Defining responses to therapy and study outcomes in clinical trials of invasive fungal diseases: Mycoses Study Group and European Organization for Research and Treatment of Cancer consensus criteria. Clin. Infect. Dis. 2008, 47, 674–683. [Google Scholar] [CrossRef]
- Wei, L.W.; Zhu, P.Q.; Chen, X.Q.; Yu, J. Mucormycosis in Mainland China: A Systematic Review of Case Reports. Mycopathologia 2022, 187, 1–14. [Google Scholar] [CrossRef]
- Stern, A.; Su, Y.; Lee, Y.J.; Seo, S.; Shaffer, B.; Tamari, R.; Gyurkocza, B.; Barker, J.; Bogler, Y.; Giralt, S.; et al. A Single-Center, Open-Label Trial of Isavuconazole Prophylaxis against Invasive Fungal Infection in Patients Undergoing Allogeneic Hematopoietic Cell Transplantation. Biol. Blood Marrow Transplant. 2020, 26, 1195–1202. [Google Scholar] [CrossRef]
- Vu, C.A.; Rana, M.M.; Jacobs, S.E.; Saunders-Hao, P. Isavuconazole for the prophylaxis and treatment of invasive fungal disease: A single-center experience. Transpl. Infect. Dis. 2021, 23, e13469. [Google Scholar] [CrossRef]
- Scott, S.A.; Perry, C.; Mahmoudjafari, Z.; Martin, G.A.; Boyd, S.; Thompson, J.; Thomas, B. Incidence of breakthrough fungal infections on isavuconazole prophylaxis compared to posaconazole and voriconazole. Transpl. Infect. Dis. 2023, 25, e14045. [Google Scholar] [CrossRef]
- Hassouna, H.; Athans, V.; Brizendine, K.D. Real-world use-Isavuconazole at a large academic medical center. Mycoses 2019, 62, 534–541. [Google Scholar] [CrossRef]
- Maschmeyer, G.; Patterson, T.F. Our 2014 approach to breakthrough invasive fungal infections. Mycoses 2014, 57, 645–651. [Google Scholar] [CrossRef] [PubMed]
- Lerolle, N.; Raffoux, E.; Socie, G.; Touratier, S.; Sauvageon, H.; Porcher, R.; Bretagne, S.; Bergeron, A.; Azoulay, E.; Molina, J.M.; et al. Breakthrough invasive fungal disease in patients receiving posaconazole primary prophylaxis: A 4-year study. Clin. Microbiol. Infect. 2014, 20, O952–O959. [Google Scholar] [CrossRef]
- Ashkenazi-Hoffnung, L.; Bilavsky, E.; Levy, I.; Grisaru, G.; Sadot, E.; Ben-Ami, R.; Novikov, A.; Fischer, S.; Nahum, E.; Scheuerman, O. Isavuconazole As Successful Salvage Therapy for Mucormycosis in Pediatric Patients. Pediatr. Infect. Dis. J. 2020, 39, 718–724. [Google Scholar] [CrossRef]
- Autmizguine, J.; Guptill, J.T.; Cohen-Wolkowiez, M.; Benjamin, D.K., Jr.; Capparelli, E.V. Pharmacokinetics and pharmacodynamics of antifungals in children: Clinical implications. Drugs 2014, 74, 891–909. [Google Scholar] [CrossRef] [PubMed]
- Hamed, K.; Engelhardt, M.; Kovanda, L.L.; Huang, J.J.; Yan, J.; Aram, J.A. Post-hoc analysis of the safety and efficacy of isavuconazole in older patients with invasive fungal disease from the VITAL and SECURE studies. Sci. Rep. 2023, 13, 6730. [Google Scholar] [CrossRef]
- Pieragostini, R.; Xhaard, A.; Sauvageon, H.; Madelaine, I.; Touratier, S.; Denis, B. Context of instauration and evolution under isavuconazole, a 2-year prospective real-life study. Med. Mycol. 2023, 61, myad033. [Google Scholar] [CrossRef] [PubMed]
- Groll, A.H.; Townsend, R.; Desai, A.; Azie, N.; Jones, M.; Engelhardt, M.; Schmitt-Hoffman, A.H.; Brüggemann, R.J.M. Drug-drug interactions between triazole antifungal agents used to treat invasive aspergillosis and immunosuppressants metabolized by cytochrome P450 3A4. Transpl. Infect. Dis. 2017, 19, e12751. [Google Scholar] [CrossRef]
- Groll, A.H.; Desai, A.; Han, D.; Howieson, C.; Kato, K.; Akhtar, S.; Kowalski, D.; Lademacher, C.; Lewis, W.; Pearlman, H.; et al. Pharmacokinetic Assessment of Drug-Drug Interactions of Isavuconazole With the Immunosuppressants Cyclosporine, Mycophenolic Acid, Prednisolone, Sirolimus, and Tacrolimus in Healthy Adults. Clin. Pharmacol. Drug Dev. 2017, 6, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Townsend, R.; Dietz, A.; Hale, C.; Akhtar, S.; Kowalski, D.; Lademacher, C.; Lasseter, K.; Pearlman, H.; Rammelsberg, D.; Schmitt-Hoffmann, A.; et al. Pharmacokinetic Evaluation of CYP3A4-Mediated Drug-Drug Interactions of Isavuconazole With Rifampin, Ketoconazole, Midazolam, and Ethinyl Estradiol/Norethindrone in Healthy Adults. Clin. Pharmacol. Drug Dev. 2017, 6, 44–53. [Google Scholar] [CrossRef]
- Keirns, J.; Desai, A.; Kowalski, D.; Lademacher, C.; Mujais, S.; Parker, B.; Schneidkraut, M.J.; Townsend, R.; Wojtkowski, T.; Yamazaki, T.; et al. QT Interval Shortening With Isavuconazole: In Vitro and In Vivo Effects on Cardiac Repolarization. Clin. Pharmacol. Ther. 2017, 101, 782–790. [Google Scholar] [CrossRef]
- DiPippo, A.J.; Rausch, C.R.; Kontoyiannis, D.P. Tolerability of isavuconazole after posaconazole toxicity in leukaemia patients. Mycoses 2019, 62, 81–86. [Google Scholar] [CrossRef]
- Sun, Y.; Meng, F.; Han, M.; Zhang, X.; Yu, L.; Huang, H.; Wu, D.; Ren, H.; Wang, C.; Shen, Z.; et al. Epidemiology, management, and outcome of invasive fungal disease in patients undergoing hematopoietic stem cell transplantation in China: A multicenter prospective observational study. Biol. Blood Marrow Transplant. 2015, 21, 1117–1126. [Google Scholar] [CrossRef]
- Desai, A.V.; Han, D.; Kowalski, D.L.; Lademacher, C.; Pearlman, H.; Yamazaki, T. No Dose Adjustment for Isavuconazole Based on Age or Sex. Antimicrob. Agents Chemother. 2019, 63, e02629. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristics | Value |
|---|---|
| Age, y, median (range) | 45.8 (9–72) |
| Male sex, n (%) | 16 (40%) |
| Weight, Kg, median (range) | 59 (35–96) |
| Disease type (%) | |
| Diffuse large B-cell lymphoma | 8 (20%) |
| Acute myeloid leukemia | 10 (25%) |
| Natural/killer T-cell lymphoma | 2 (5%) |
| Follicular lymphoma | 2 (5%) |
| Aplastic anemia | 2 (5%) |
| T-cell lymphoblastic lymphoma | 2 (5%) |
| Mixed-phenotype acute leukemia | 2 (5%) |
| Hemophagocytic syndrome | 4 (10%) |
| Sepsis | 2 (5%) |
| Fungal sinusitis | 2 (5%) |
| Pulmonary mycosis | 4 (10%) |
| IFD | |
| Invasive aspergillosis | 12 (30%) |
| Invasive candidiasis | 2 (5%) |
| Invasive mucormycosis | 12 (30%) |
| Unknown | 14 (35%) |
| Morbidities | |
| Diabetes mellitus | 10 (25%) |
| Hepatic insufficiency | 8 (20%) |
| Renal insufficiency | 16 (40%) |
| Graft-versus-host disease | 6 (15%) |
| Respiratory failure | 4 (10%) |
| Autologous | 6 (15%) |
| Allogeneic | 10 (25%) |
| Site of infection | |
| Pulmonary | 36 (90%) |
| Paranasal sinuses | 4 (10%) |
| Respiratory tract | 2 (5%) |
| Bloodstream infections | 6 (15%) |
| Classifications—IFD | |
| Proven | 2 (5%) |
| Probable | 24 (60%) |
| Possible | 14 (35%) |
| Outcome | |
| Diagnosis of IFD | |
| Partial remission | 30 (75%) |
| Progression | 7 (10%) |
| Dead | 3 (15%) |
| Type of IFD | |
| Invasive aspergillosis | 8/12 (66.7%) |
| Invasive candidiasis | 0/2 (0%) |
| Invasive mucormycosis | 10/12 83.3%) |
| Site of infection | |
| Pulmonary | 26/36 (72.2%) |
| Paranasal sinuses | 4/4 (100%) |
| Respiratory tract | 2/2 (100%) |
| Bloodstream infections | 6/8 (75%) |
| Therapy | |
| Target treatment | 18/26 (69.2%) |
| Empirical treatment | 12/14 (85.7%) |
| NO | Gender | Age | Disease Type | Outcome | Site | Key Evidence | Diagnosis |
|---|---|---|---|---|---|---|---|
| 1 | Female | 59 | AML | dead | pulmonary | CT; Candida albicans determined via phlegm culture | Probable |
| 2 | Male | 43 | hemophagocytic syndrome | partial remission | pulmonary | CT; febrile neutropenia | Possible |
| 3 | Female | 42 | AML | progression | pulmonary | Aspergillus determined via BAL fluid culture | Probable |
| 4 | Male | 54 | natural/killer T-cell lymphoma | partial remission | pulmonary | Aspergillus determined via blood mNGS; CT | Probable |
| 5 | Male | 72 | DLBCL | partial remission | pulmonary/respiratory tract | CT; Aspergillus determined via phlegm culture | Probable |
| 6 | Female | 43 | aplastic anemia | dead | pulmonary/bloodstream infections | Rhizomucor pusillus determined via blood mNGS; CT | Probable |
| 7 | Male | 52 | DLBCL | partial remission | pulmonary | CT; febrile neutropenia | Possible |
| 8 | Male | 22 | AML | partial remission | pulmonary | CT; febrile neutropenia | Possible |
| 9 | Female | 70 | DLBCL | partial remission | pulmonary | CT; febrile neutropenia | Possible |
| 10 | Female | 48 | AML | progression | pulmonary | CT; Aspergillus determined via phlegm culture | Probable |
| 11 | Male | 38 | T-cell lymphoblastic lymphoma | partial remission | pulmonary | CT; Aspergillus determined via BAL fluid mNGS | Probable |
| 12 | Male | 57 | sepsis | partial remission | pulmonary/bloodstream infections | Rhizopus oryzae determined via mNGS; CT | Probable |
| 13 | Male | 20 | mixed phenotype acute leukemia | partial remission | pulmonary | Aspergillus determined via BAL fluid culture; CT | Probable |
| 14 | Male | 9 | AML | partial remission | pulmonary | CT; febrile neutropenia | Possible |
| 15 | Female | 40 | hemophagocytic syndrome | partial remission | pulmonary/bloodstream infections | Rhizomucor determined via mNGS; CT | Probable |
| 16 | Female | 66 | DLBCL | dead | pulmonary | CT; fever | Possible |
| 17 | Male | 61 | follicular lymphoma | partial remission | Bloodstream infections/paranasal sinuses | CT; Lichtheimia corymbifera determined via mNGS | Probable |
| 18 | Female | 33 | pulmonary mycosis | partial remission | pulmonary | History of Mycosis infection | Possible |
| 19 | Male | 52 | fungal sinusitis | partial remission | paranasal sinuses | Histopathology showing true hyphae (IM) | Proven |
| 20 | Male | 48 | pulmonary mycosis | partial remission | pulmonary | CT; Rhizopus delemar identified using fluid mNGS | Probable |
| 21 | Female | 58 | DLBCL | progression | pulmonary | CT; Candida albicans determined via phlegm culture | Probable |
| 22 | Male | 44 | AML | partial remission | pulmonary | CT; febrile neutropenia | Possible |
| 23 | Male | 50 | hemophagocytic syndrome | partial remission | pulmonary | CT; Fever | Possible |
| 24 | Female | 40 | AML | progression | pulmonary | Aspergillus determined via BAL fluid culture | Probable |
| 25 | Male | 56 | natural/killer T-cell lymphoma | partial remission | pulmonary | Blood GM test positive 1 time (IA); CT | Probable |
| 26 | Male | 16 | AML | partial remission | pulmonary | CT; febrile neutropenia | Possible |
| 27 | Male | 72 | hemophagocytic syndrome | partial remission | pulmonary/respiratory tract | Rhizopus oryzae determined via mNGS; CT | Probable |
| 28 | Female | 45 | aplastic anemia | progression | pulmonary/bloodstream infections | Rhizomucor determined via mNGS; CT | Probable |
| 29 | Male | 48 | pulmonary mycosis | partial remission | pulmonary | CT; Rhizopus delemar identified using fluid mNGS | Probable |
| 30 | Male | 55 | sepsis | partial remission | pulmonary/bloodstream infections | CT; Rhizomucor determined via mNGS | Probable |
| 31 | Male | 22 | mixed phenotype acute leukemia | partial remission | pulmonary | CT; febrile neutropenia | Possible |
| 32 | Male | 24 | AML | partial remission | pulmonary | CT; febrile neutropenia | Possible |
| 33 | Female | 68 | AML | partial remission | pulmonary | Aspergillus determined via BAL fluid culture; CT | Probable |
| 34 | Female | 50 | fungal sinusitis | progression | pulmonary | CT; Fever | Possible |
| 35 | Male | 40 | T-cell lymphoblastic lymphoma | partial remission | pulmonary | Histopathology showing true hyphae (IM) | Proven |
| 36 | Male | 30 | DLBCL | partial remission | paranasal sinuses | CT; Aspergillus determined via BAL fluid mNGS | Probable |
| 37 | Female | 44 | DLBCL | partial remission | pulmonary/Bloodstream infections | CT; Aspergillus determined via phlegm culture | Probable |
| 38 | Female | 53 | follicular lymphoma | progression | pulmonary | CT; Aspergillus determined via phlegm culture | Probable |
| 39 | Male | 36 | DLBCL | partial remission | Bloodstream infections/paranasal sinuses | CT; Rhizomucor determined via mNGS | Probable |
| 40 | Female | 55 | pulmonary mycosis | partial remission | pulmonary | History of Mycosis infection | Possible |
| Characteristics | Clinical Response (n/Median, IQR) | Clinical Failure (n/Median, IQR) | p |
|---|---|---|---|
| Age | 44.4 (9–72) | 50.4 (40–66) | 0.235 |
| Gender (male/female) | 24/6 | 0/10 | 0.000 ** |
| Allogeneic/autologous | 6/4 | 0/6 | 0.027 ** |
| Target treatment/empirical treatment | 18/12 | 8/2 | 0.446 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, L.; Li, S.; Gao, W.; Zhu, X.; Luo, P.; Xu, D.; Liu, D.; He, Y. Real-World, Multicenter Case Series of Patients Treated with Isavuconazole for Invasive Fungal Disease in China. Microorganisms 2023, 11, 2229. https://doi.org/10.3390/microorganisms11092229
Wu L, Li S, Gao W, Zhu X, Luo P, Xu D, Liu D, He Y. Real-World, Multicenter Case Series of Patients Treated with Isavuconazole for Invasive Fungal Disease in China. Microorganisms. 2023; 11(9):2229. https://doi.org/10.3390/microorganisms11092229
Chicago/Turabian StyleWu, Lisha, Shougang Li, Weixi Gao, Xiaojian Zhu, Pan Luo, Dong Xu, Dong Liu, and Yan He. 2023. "Real-World, Multicenter Case Series of Patients Treated with Isavuconazole for Invasive Fungal Disease in China" Microorganisms 11, no. 9: 2229. https://doi.org/10.3390/microorganisms11092229