
Gut and Urinary Microbiota in Cats with Kidney Stones



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
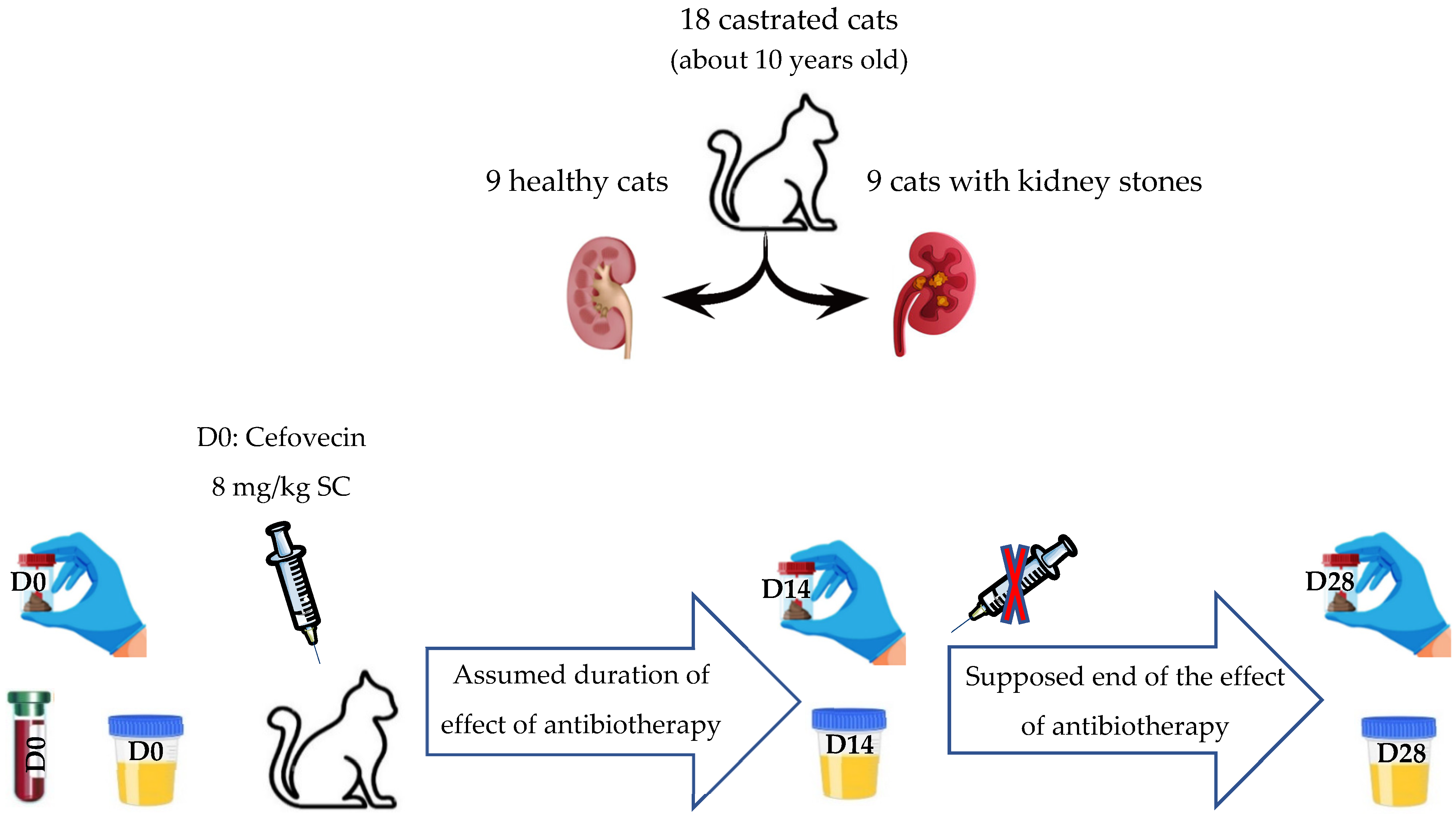
2.1. Studied Population
2.1.1. Recruitment of Cats
2.1.2. Living Conditions
2.1.3. Health Status
2.1.4. Inclusion Criteria
2.1.5. Exclusion Criteria
- privately owned cats diagnosed with lithiasis,
- cats presumed healthy but whose renal architecture was not confirmed as normal on ultrasound,
- cats that had received antibiotic treatment prior to the study,
- cats with a significant pathological history,
- cats fed a diet different from that given to the study group,
- cats that had received prebiotics, probiotics, or postbiotics before the study.
2.1.6. Follow-Up
2.2. Sample Collection
2.2.1. Collection of Fecal Samples
2.2.2. Collection of Urine Samples
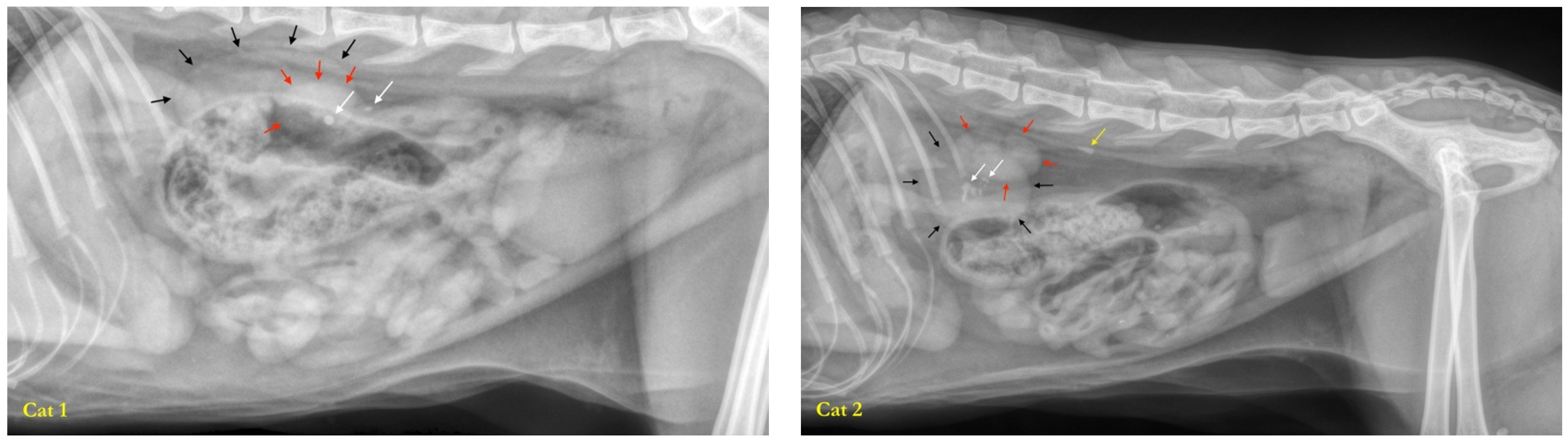
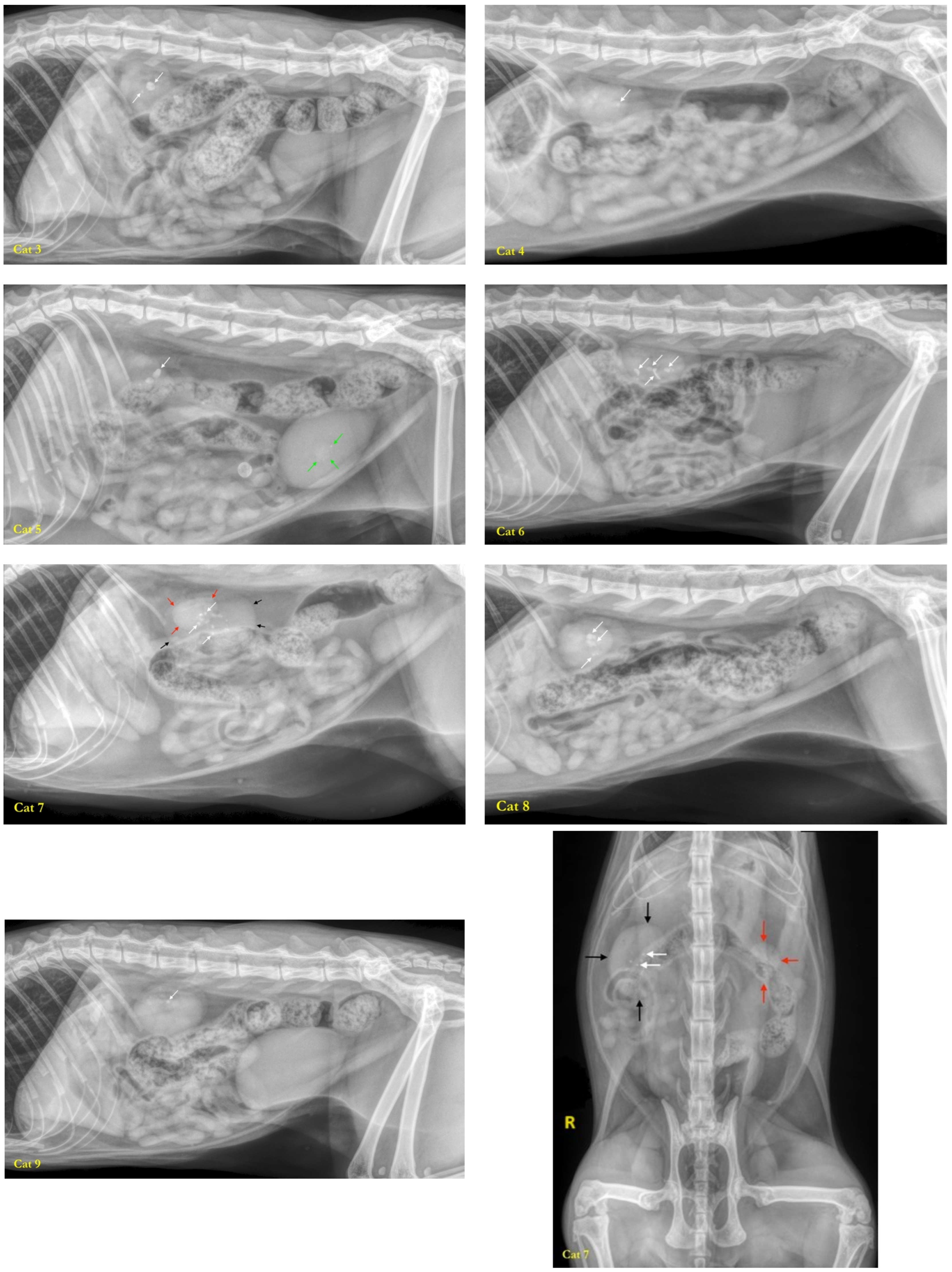
2.2.3. Collection of Calculi
2.3. Antibiotic Therapy
2.4. DNA Isolation and 16S rRNA Amplicon Sequencing
2.4.1. High-Throughput Bacterial DNA Sequencing Techniques Used
2.4.2. DNA Extraction
2.4.3. 16S rRNA Gene Amplification and Sequencing [42]
2.4.4. Data Processing
2.4.5. Statistical Analyzes
3. Results
3.1. Studied Population
3.2. Characterization of the Fecal Microbiota
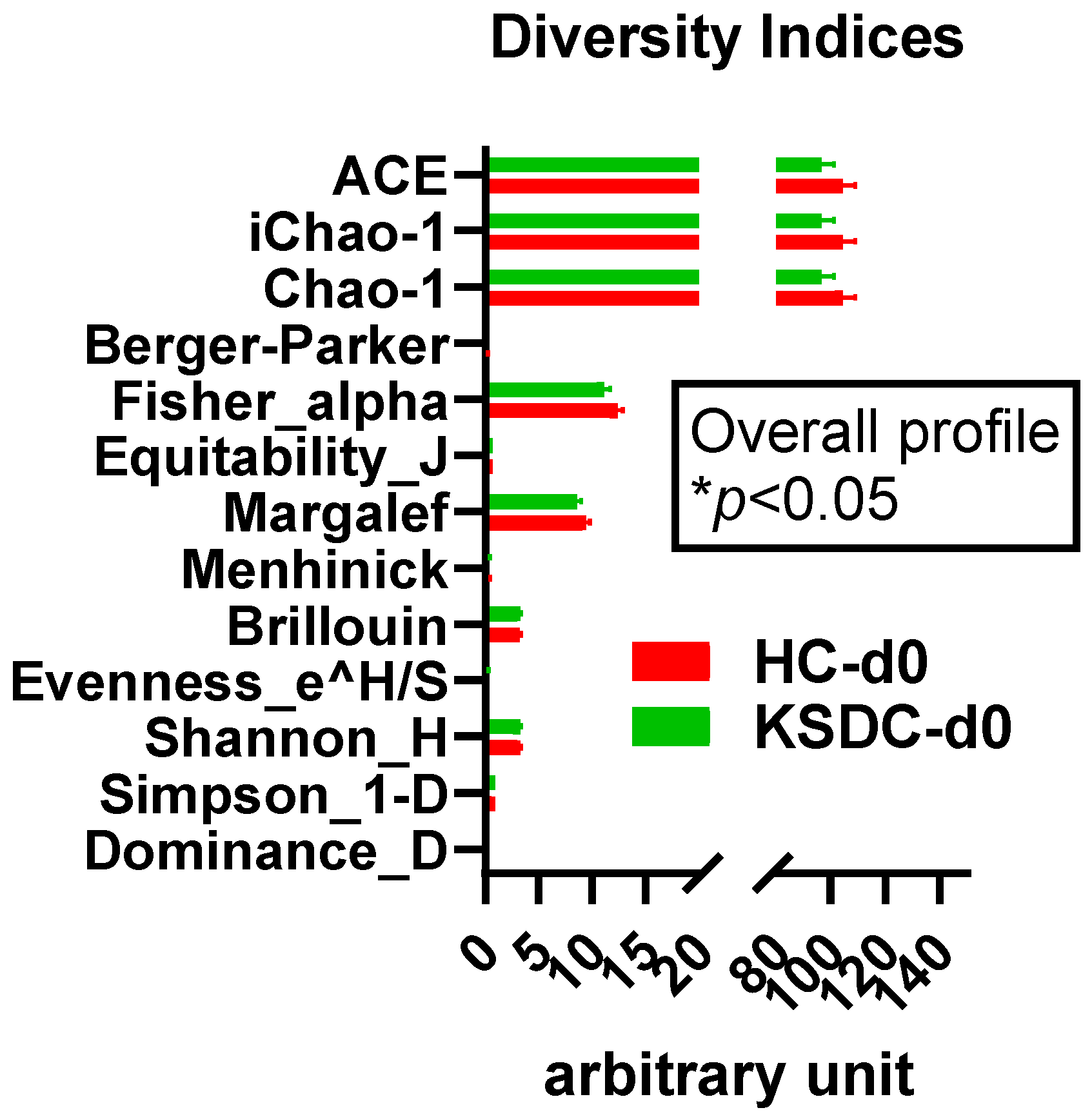
3.2.1. Alpha Diversity
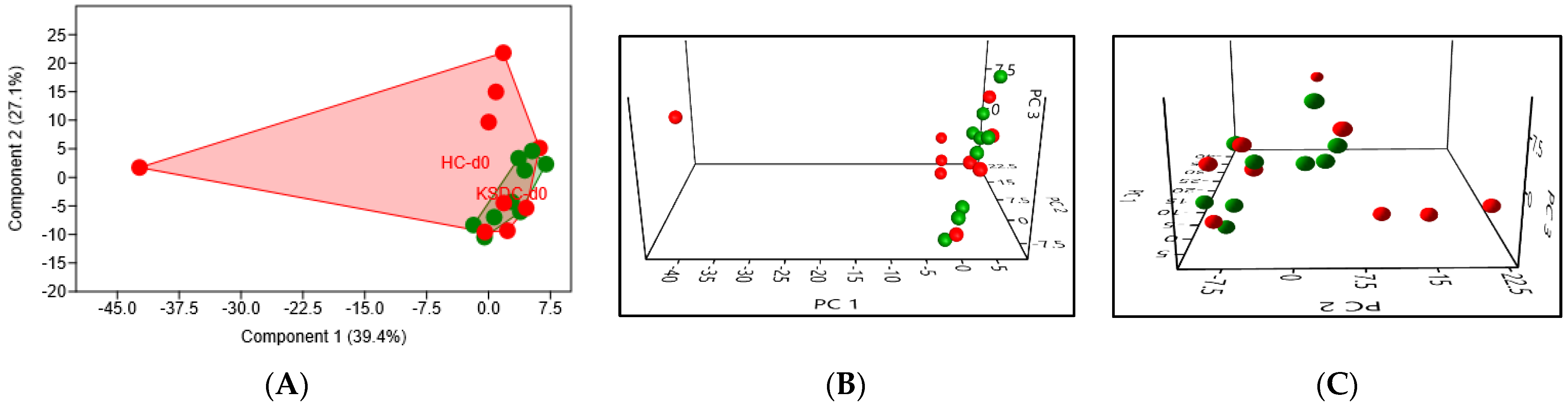
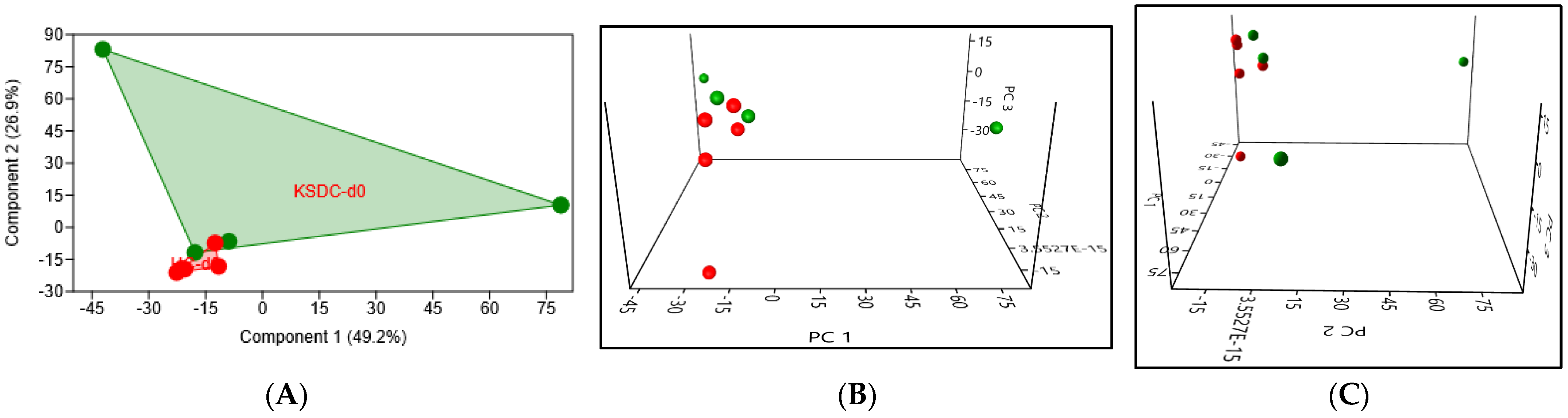
3.2.2. Beta Diversity
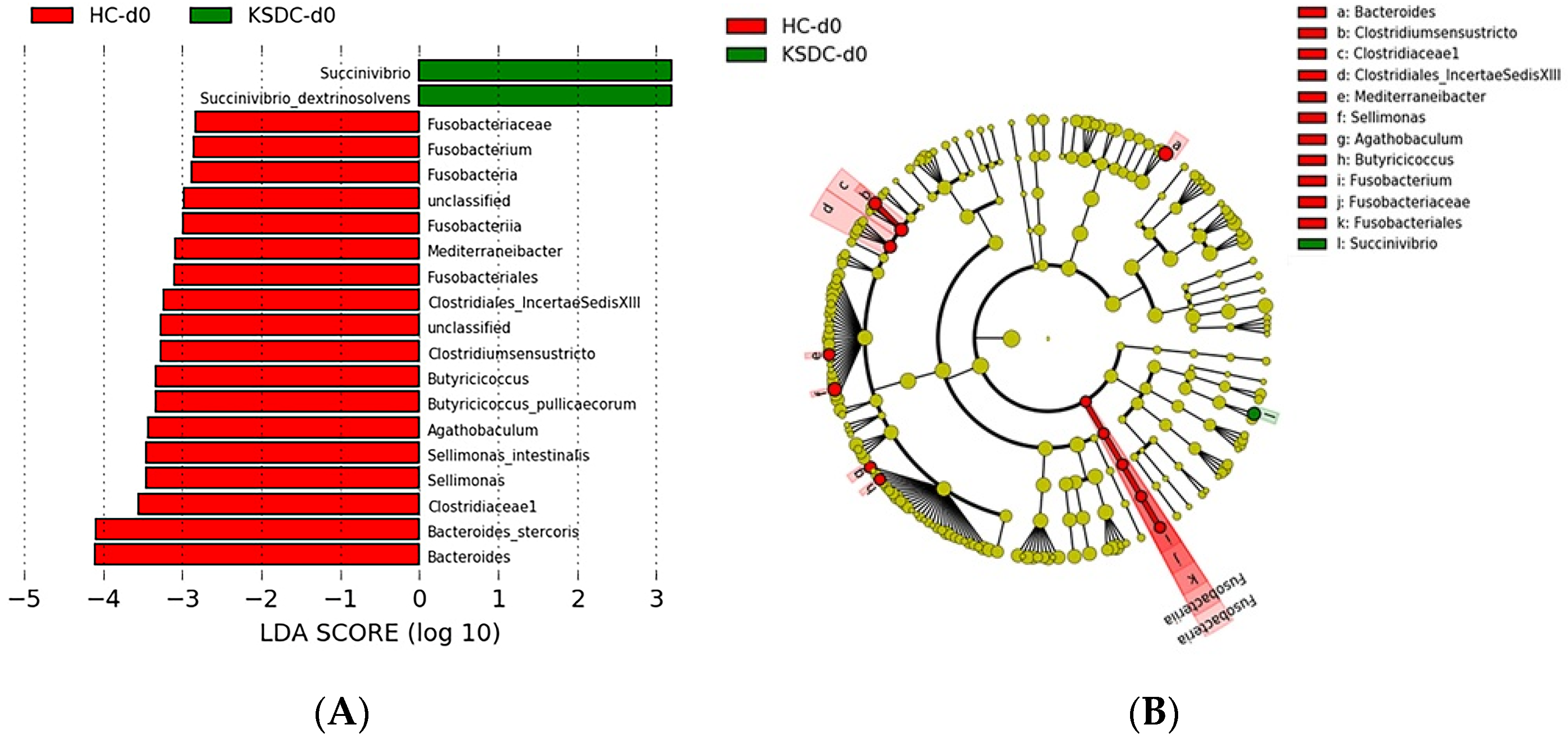
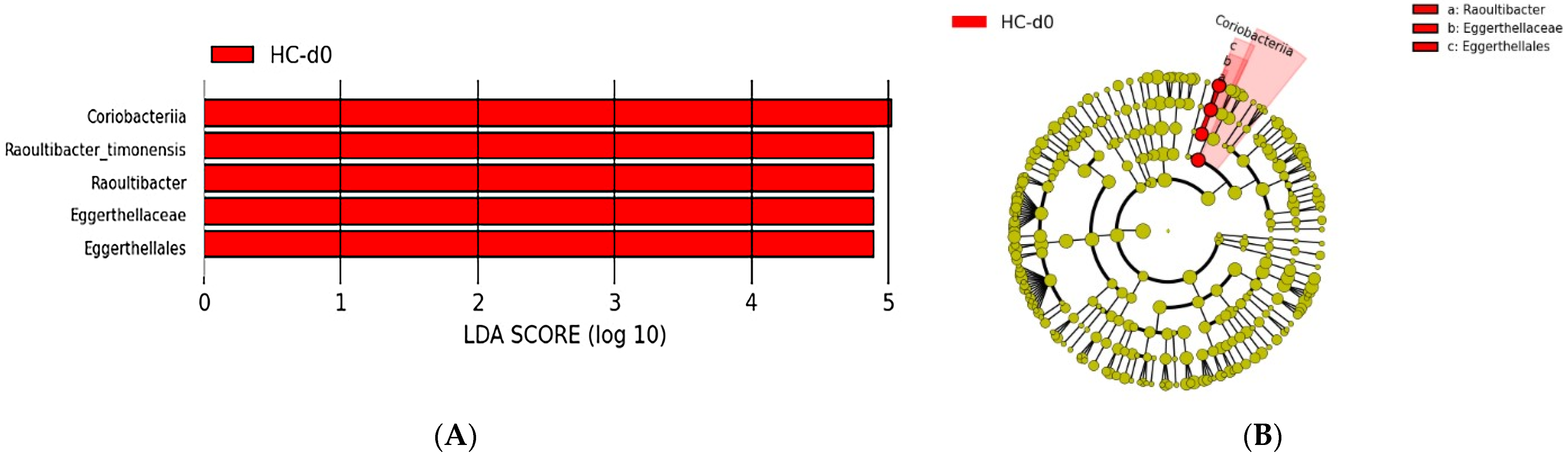
Taxonomic Analysis of the Intestinal Microbiota Composition at D0 in the Two Cat Populations
Biodiversity of the Fecal Microbiota in the Two Cat Populations
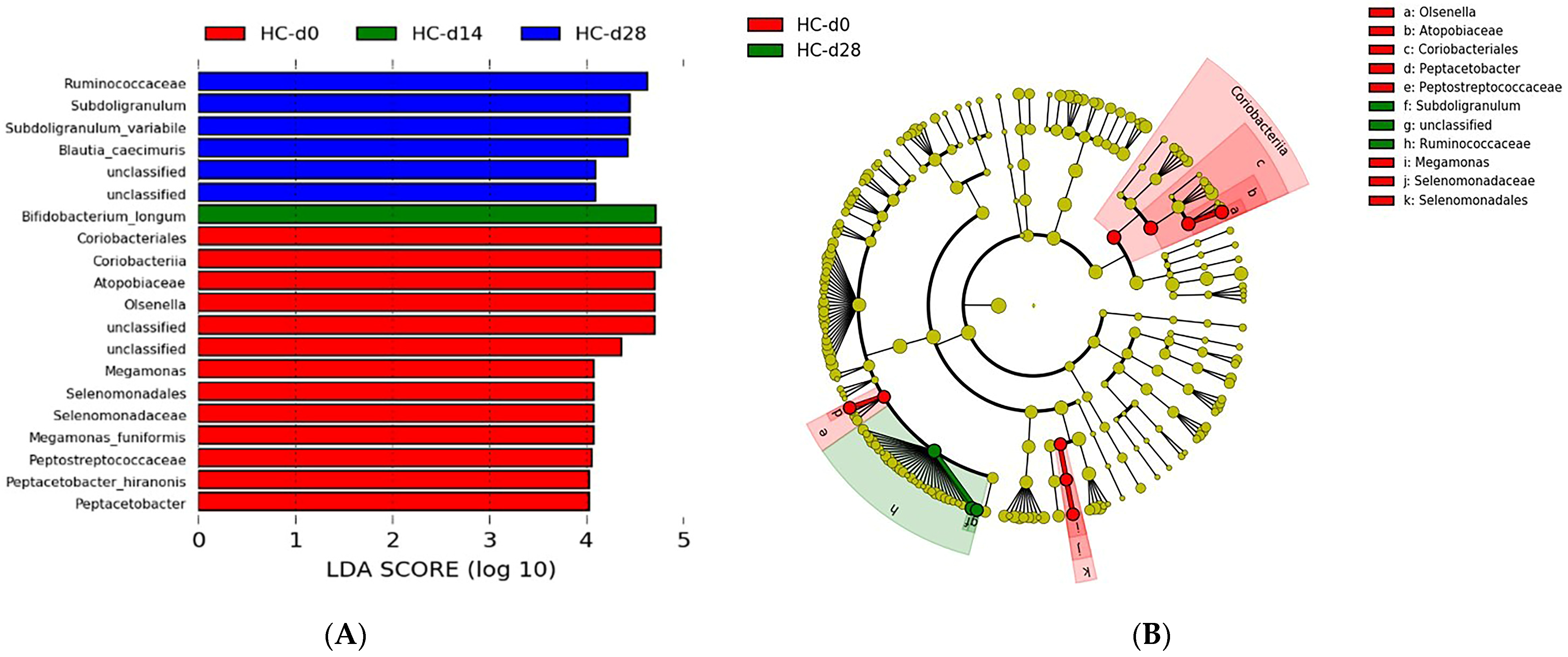
3.3. Taxonomic Analysis of the Intestinal Microbiota Composition at D0, D14, and D28 in the Healthy Cats Population
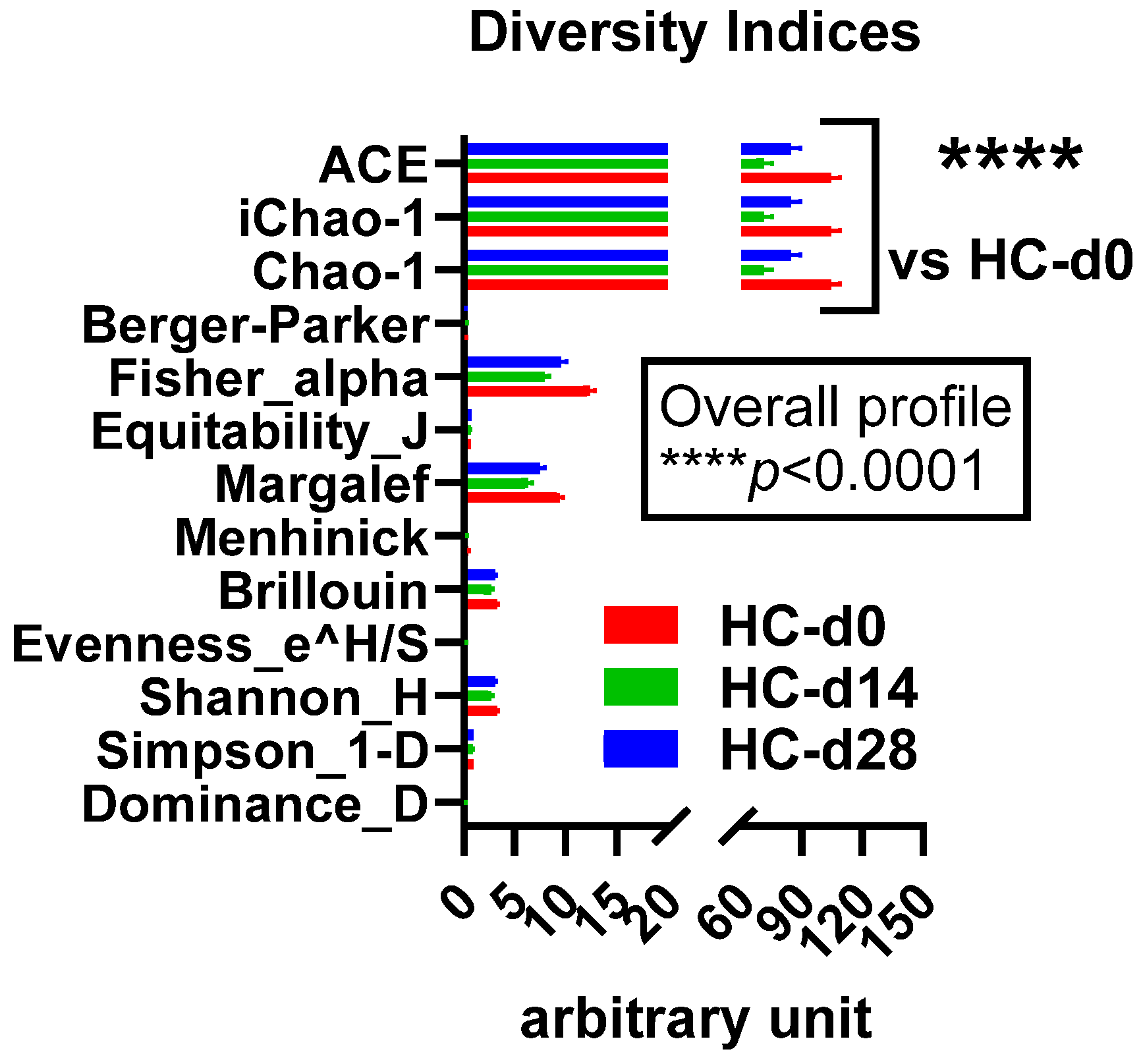
3.3.1. Alpha Diversity
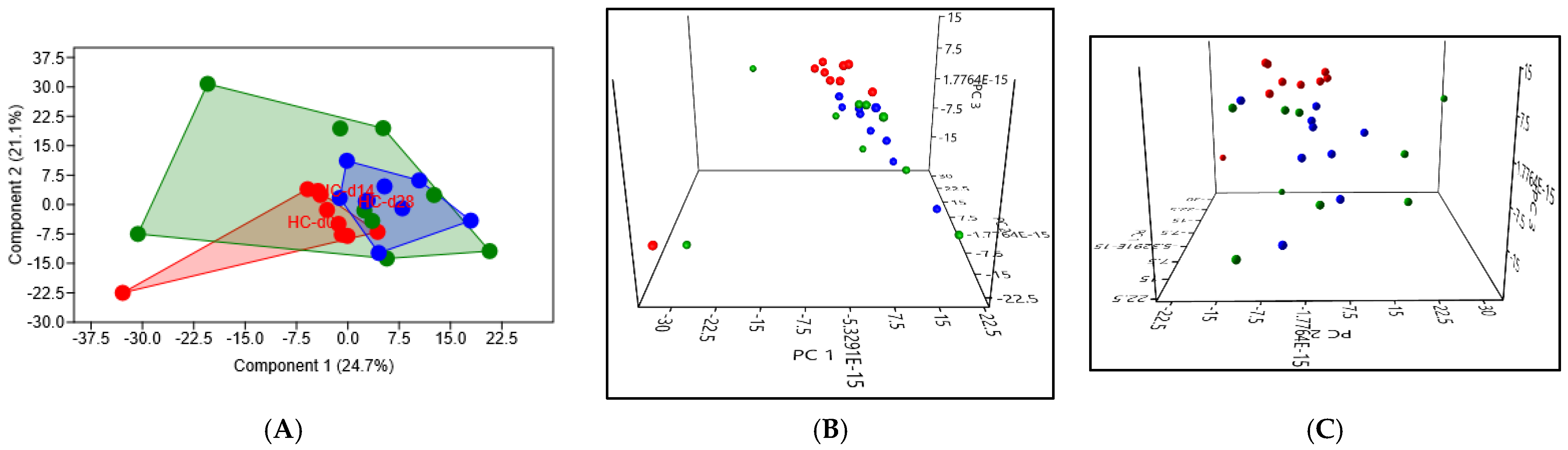
3.3.2. Beta Diversity
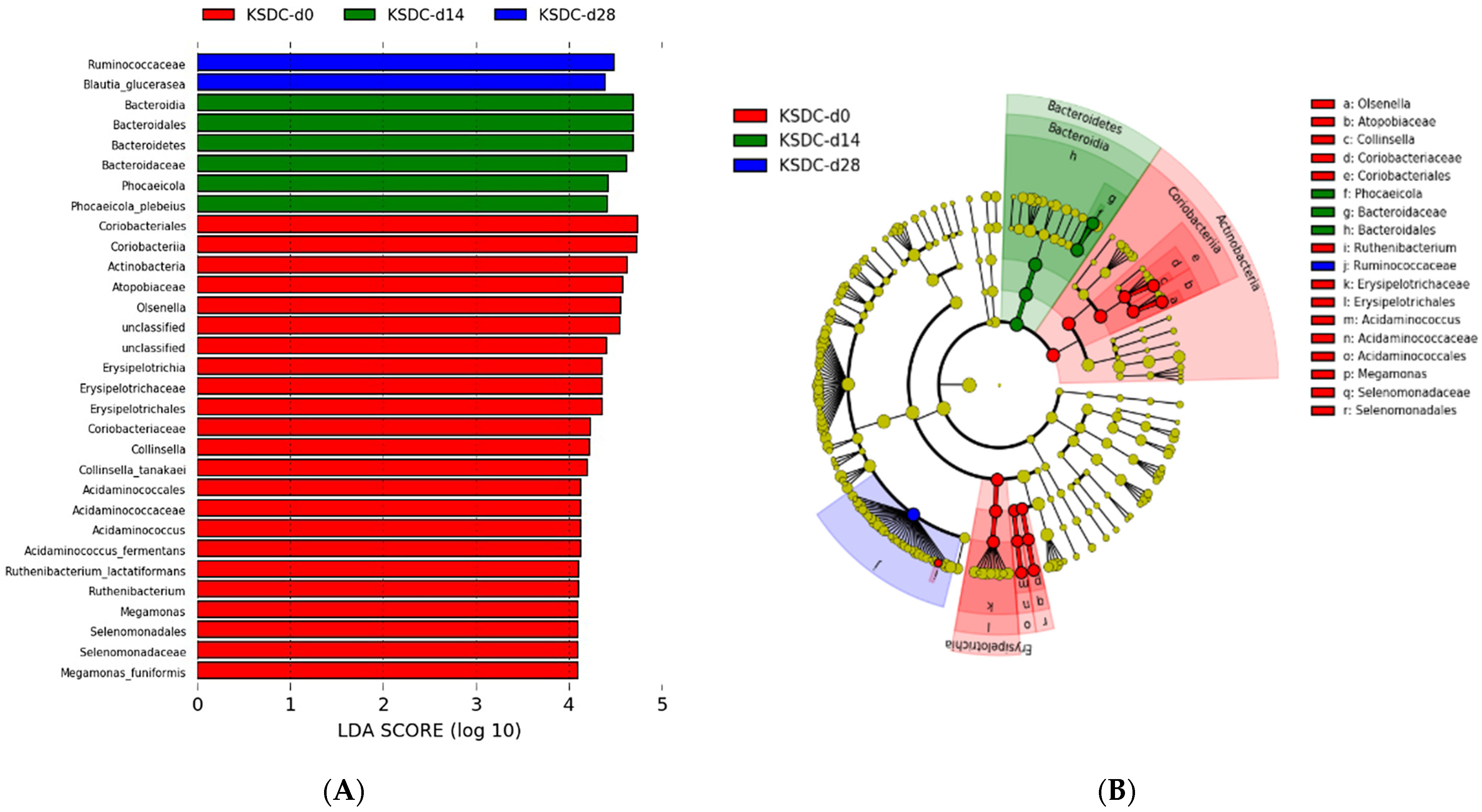
3.4. Taxonomic Analysis of the Intestinal Microbiota Composition at D0, D14, and D28 in the Population of Cats with Lithiasis
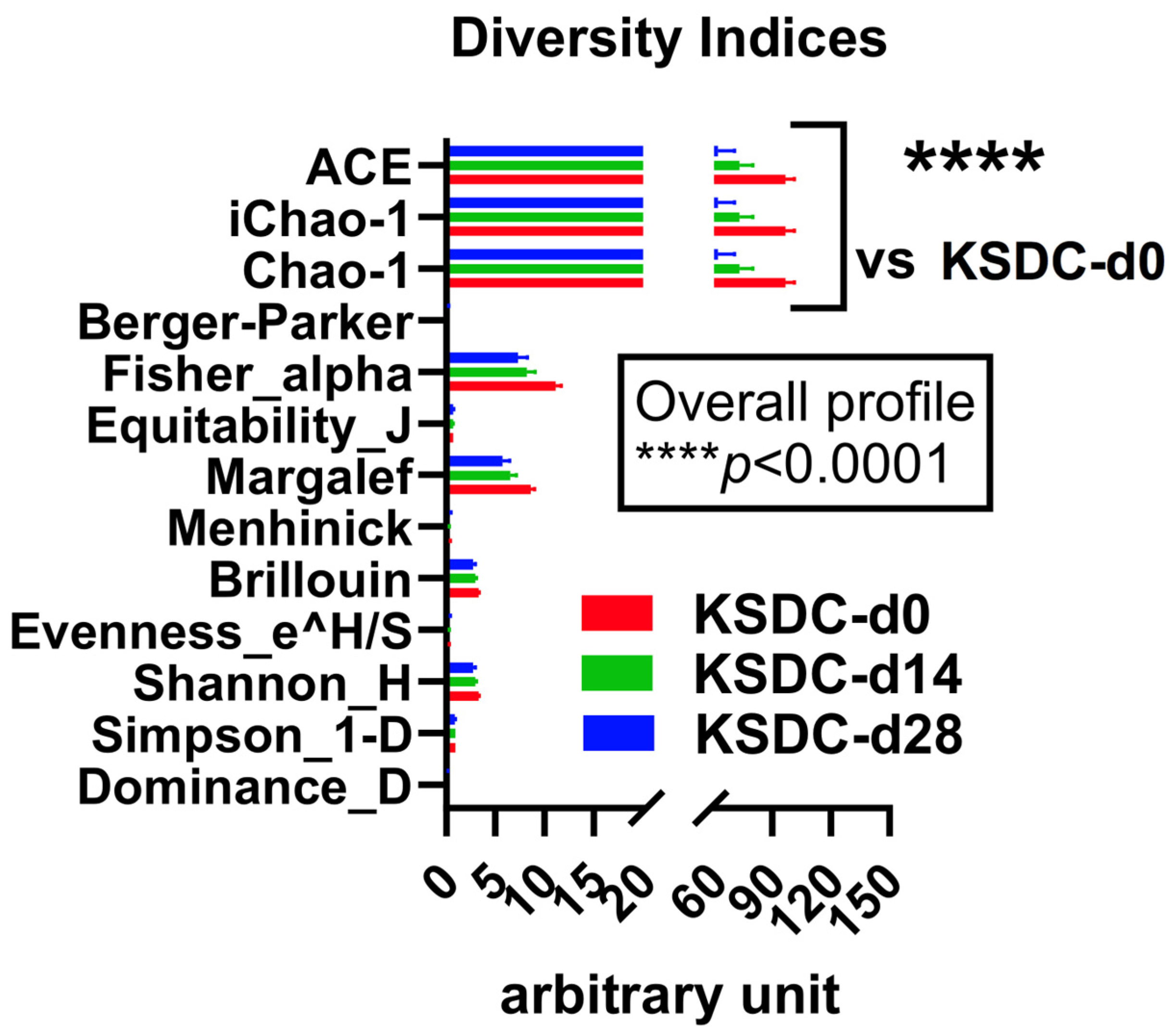
3.4.1. Alpha Diversity
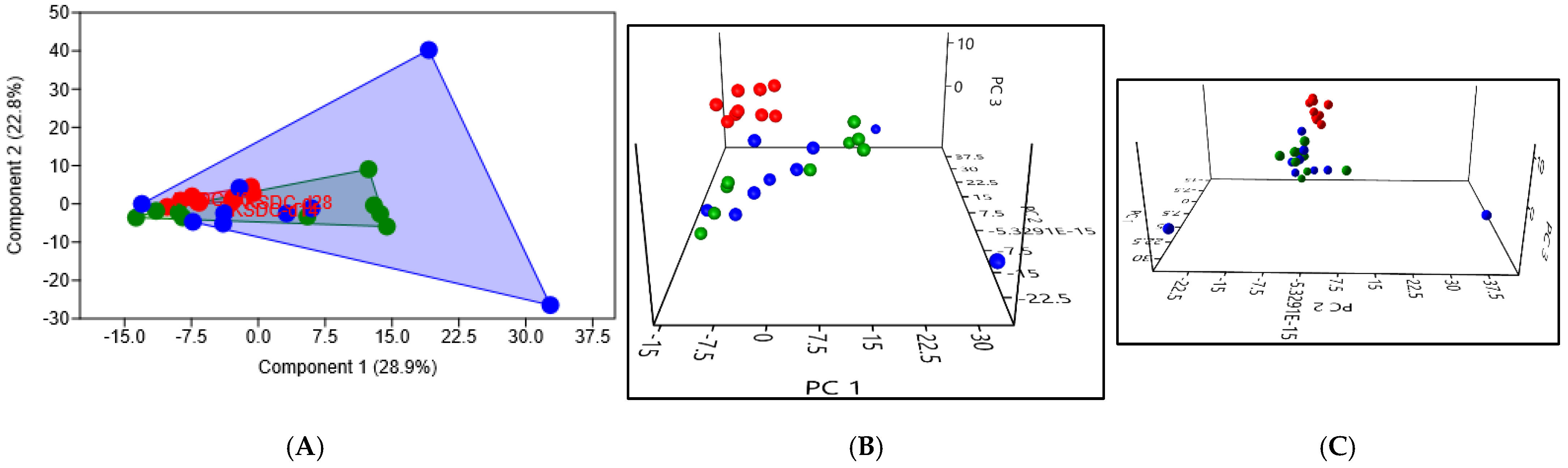
3.4.2. Beta Diversity
3.5. Characterization of the Urinary Microbiota
3.5.1. Available Results
3.5.2. Alpha Diversity
3.5.3. Beta Diversity
4. Discussion
4.1. Study of the Intestinal Microbiota in Patients with Kidney Stones
4.1.1. Previous Studies
4.1.2. Alpha Diversity
4.1.3. Beta Diversity
4.2. Impact of Antibiotic Therapy on the Intestinal Microbiota
4.2.1. Choice of Cefovecin
4.2.2. Alpha Diversity
4.2.3. Beta Diversity
4.3. Resilience
4.4. Study of the Urinary Microbiota
4.4.1. Urine Is Not Sterile in Cats
4.4.2. A Different Urobiome in the Stone Formers Cats
4.5. Advantages of This Animal Experimental Model
4.6. Limitation of This Study
4.7. A Hypothesis on the Origin of the Epidemic of Kidney Stones in Cats
- many cats living in urban environments go out a few times or not at all, so they have fewer opportunities to seed their digestive tract in their youth with the microbiota of their prey or that of their congeners,
- they eat only industrial foods that are almost sterilized for preservation concerns,
- they are more medicalized so they receive antibiotics more often than in the past.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Osborne, C.A.; Lulich, J.P.; Kruger, J.M.; Ulrich, L.K.; Koehler, L.A. Analysis of 451,891 canine uroliths, feline uroliths, and feline urethral plugs from 1981 to 2007: Perspectives from the Minnesota Urolith Center. Vet. Clin. N. Am. Small Anim. Pract. 2009, 39, 183–197. [Google Scholar] [CrossRef] [PubMed]
- Palm, C.; Westropp, J. Cats and calcium oxalate: Strategies for managing lower and upper tract stone disease. J. Feline Med. Surg. 2011, 13, 651–660. [Google Scholar] [CrossRef] [PubMed]
- Lekcharoensuk, C.; Lulich, J.P.; Osborne, C.A.; Koehler, L.A.; Urlich, L.K.; Carpenter, K.A.; Swanson, L.L. Association between patient-related factors and risk of calcium oxalate and magnesium ammonium phosphate urolithiasis in cats. J. Am. Vet. Med. Assoc. 2000, 217, 520–525. [Google Scholar] [CrossRef] [PubMed]
- Lekcharoensuk, C.; Osborne, C.A.; Lulich, J.P.; Pusoonthornthum, R.; Kirk, C.A.; Ulrich, L.K.; Koehler, L.A.; Carpenter, K.A.; Swanson, L.L. Association between dietary factors and calcium oxalate and magnesium ammonium phosphate urolithiasis in cats. J. Am. Vet. Med. Assoc. 2001, 219, 1228–1237. [Google Scholar] [CrossRef] [PubMed]
- Lekcharoensuk, C.; Osborne, C.A.; Lulich, J.P.; Albasan, H.; Ulrich, L.K.; Koehler, L.A.; Carpenter, K.A.; Swanson, L.L.; Pederson, L.A. Trends in the frequency of calcium oxalate uroliths in the upper urinary tract of cats. J. Am. Anim. Hosp. Assoc. 2005, 41, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Cannon, A.B.; Westropp, J.L.; Ruby, A.L.; Kass, P.H. Evaluation of trends in urolith composition in cats: 5230 cases (1985–2004). J. Am. Vet. Med. Assoc. 2007, 231, 570–576. [Google Scholar] [CrossRef] [PubMed]
- Kopecny, L.; Palm, C.A.; Segev, G.; Larsen, J.A.; Westropp, J.L. Urolithiasis in cats: Evaluation of trends in urolith composition and risk factors (2005–2018). J. Vet. Intern. Med. 2021, 35, 1397–1405. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.R.; Pearle, M.S.; Robertson, W.G.; Gambaro, G.; Canales, B.K.; Doizi, S.; Traxer, O.; Tiselius, H.-G. Kidney stones. Nat. Rev. Dis. Primers 2016, 2, 16008. [Google Scholar] [CrossRef]
- Kyles, A.E.; Hardie, E.M.; Wooden, B.G.; Adin, C.A.; Stone, E.A.; Gregory, C.R.; Mathews, K.G.; Cowgill, L.D.; Vaden, S.; Nyland, T.G.; et al. Clinical, clinicopathologic, radiographic, and ultrasonographic abnormalities in cats with ureteral calculi: 163 cases (1984–2002). J. Am. Vet. Med. Assoc. 2005, 226, 932–936. [Google Scholar] [CrossRef]
- Lieske, J.C.; Rule, A.D.; Krambeck, A.E.; Williams, J.C.; Bergstralh, E.J.; Mehta, R.A.; Moyer, T.P. Stone Composition as a Function of Age and Sex. Clin. J. Am. Soc. Nephrol. 2014, 9, 2141–2146. [Google Scholar] [CrossRef]
- Singh, P.; Enders, F.T.; Vaughan, L.E.; Bergstralh, E.J.; Knoedler, J.J.; Krambeck, A.E.; Lieske, J.C.; Rule, A.D. Stone Composition Among First-Time Symptomatic Kidney Stone Formers in the Community. Mayo Clin. Proc. 2015, 90, 1356–1365. [Google Scholar] [CrossRef] [PubMed]
- Robijn, S.; Hoppe, B.; Vervaet, B.A.; D’Haese, P.C.; Verhulst, A. Hyperoxaluria: A gut-kidney axis? Kidney Int. 2011, 80, 1146–1158. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.W.; Dearing, D. The metabolic and ecological interactions of oxalate-degrading bacteria in the Mammalian gut. Pathogens 2013, 2, 636–652. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, B.; Beck, B.; Gatter, N.; von Unruh, G.; Tischer, A.; Hesse, A.; Laube, N.; Kaul, P.; Sidhu, H. Oxalobacter formigenes: A potential tool for the treatment of primary hyperoxaluria type 1. Kidney Int. 2006, 70, 1305–1311. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, D.W.; Kelly, J.P.; Curhan, G.C.; Anderson, T.E.; Dretler, S.P.; Preminger, G.M.; Cave, D.R. Oxalobacter formigenes may reduce the risk of calcium oxalate kidney stones. J. Am. Soc. Nephrol. 2008, 19, 1197–1203. [Google Scholar] [CrossRef] [PubMed]
- Siva, S.; Barrack, E.R.; Reddy, G.P.; Thamilselvan, V.; Thamilselvan, S.; Menon, M.; Bhandari, M. A critical analysis of the role of gut Oxalobacter formigenes in oxalate stone disease. BJU Int. 2009, 103, 18–21. [Google Scholar] [CrossRef] [PubMed]
- Gnanandarajah, J.S.; Abrahante, J.E.; Lulich, J.P.; Murtaugh, M.P. Presence of Oxalobacter formigenes in the intestinal tract is associated with the absence of calcium oxalate urolith formation in dogs. Urol. Res. 2012, 40, 467–473. [Google Scholar] [CrossRef]
- Mehta, M.; Goldfarb, D.S.; Nazzal, L. The role of the microbiome in kidney stone formation. Int. J. Surg. 2016, 36, 607–612. [Google Scholar] [CrossRef]
- Stern, J.M.; Moazami, S.; Qiu, Y.; Kurland, I.; Chen, Z.; Agalliu, I.; Burk, R.; Davies, K.P. Evidence for a distinct gut microbiome in kidney stone formers compared to non-stone formers. Urolithiasis 2016, 44, 399–407. [Google Scholar] [CrossRef]
- Ticinesi, A.; Milani, C.; Guerra, A.; Allegri, F.; Lauretani, F.; Nouvenne, A.; Mancabelli, L.; Lugli, G.A.; Turroni, F.; Duranti, S.; et al. Understanding the gut-kidney axis in nephrolithiasis: An analysis of the gut microbiota composition and functionality of stone formers. Gut 2018, 67, 2097–2106. [Google Scholar] [CrossRef]
- Sahin, N. Oxalotrophic bacteria. Res. Microbiol. 2003, 154, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.D.; Cho, S.; Lee, J.Y. Update on the Effect of the Urinary Microbiome on Urolithiasis. Diagnostics 2023, 13, 951. [Google Scholar] [CrossRef] [PubMed]
- Dawson, K.A.; Allison, M.J.; Hartman, P.A. Isolation and some characteristics of anaerobic oxalate-degrading bacteria from the rumen. Appl. Environ. Microbiol. 1980, 40, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Ellis, M.E.; Mobley, J.A.; Holmes, R.P.; Knight, J. Proteome Dynamics of the Specialist Oxalate Degrader Oxalobacter formigenes. J. Proteomics Bioinform. 2016, 9, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Herve, V.; Junier, T.; Bindschedler, S.; Verrecchia, E.; Junier, P. Diversity and ecology of oxalotrophic bacteria. World J. Microbiol. Biotechnol. 2016, 32, 28. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Zhang, Y.; Zhang, J.; Deng, Q.; Liang, H. Recent advances on the mechanisms of kidney stone formation (Review). Int. J. Mol. Med. 2021, 48, 149. [Google Scholar] [CrossRef] [PubMed]
- Gnanandarajah, J.S.; Johnson, T.J.; Kim, H.B.; Abrahante, J.E.; Lulich, J.P.; Murtaugh, M.P. Comparative faecal microbiota of dogs with and without calcium oxalate stones. J. Appl. Microbiol. 2012, 113, 745–756. [Google Scholar] [CrossRef]
- Suryavanshi, M.V.; Bhute, S.S.; Gune, R.P.; Shouche, Y.S. Functional eubacteria species along with trans-domain gut inhabitants favour dysgenic diversity in oxalate stone disease. Sci. Rep. 2018, 8, 16598. [Google Scholar] [CrossRef]
- Miller, A.W.; Choy, D.; Penniston, K.L.; Lange, D. Inhibition of urinary stone disease by a multi-species bacterial network ensures healthy oxalate homeostasis. Kidney Int. 2019, 96, 180–188. [Google Scholar] [CrossRef]
- Ticinesi, A.; Nouvenne, A.; Chiussi, G.; Castaldo, G.; Guerra, A.; Meschi, T. Calcium Oxalate Nephrolithiasis and Gut Microbiota: Not just a Gut-Kidney Axis. A Nutritional Perspective. Nutrients 2020, 12, 548. [Google Scholar] [CrossRef]
- Miller, A.W.; Penniston, K.L.; Fitzpatrick, K.; Agudelo, J.; Tasian, G.; Lange, D. Mechanisms of the intestinal and urinary microbiome in kidney stone disease. Nat. Rev. Urol. 2022, 19, 695–707. [Google Scholar] [CrossRef]
- Yuan, T.; Xia, Y.; Li, B.; Yu, W.; Rao, T.; Ye, Z.; Yan, X.; Song, B.; Li, L.; Lin, F.; et al. Gut microbiota in patients with kidney stones: A systematic review and meta-analysis. BMC Microbiol. 2023, 23, 143. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.W.; Oakeson, K.F.; Dale, C.; Dearing, M.D. Microbial Community Transplant Results in Increased and Long-Term Oxalate Degradation. Microb. Ecol. 2016, 72, 470–478. [Google Scholar] [CrossRef] [PubMed]
- Canales, B.K.; Hatch, M. Oxalobacter formigenes colonization normalizes oxalate excretion in a gastric bypass model of hyperoxaluria. Surg. Obes. Relat. Dis. 2017, 13, 1152–1157. [Google Scholar] [CrossRef]
- Liu, Y.; Jin, X.; Hong, H.G.; Xiang, L.; Jiang, Q.; Ma, Y.; Chen, Z.; Cheng, L.; Jian, Z.; Wei, Z.; et al. The relationship between gut microbiota and short chain fatty acids in the renal calcium oxalate stones disease. FASEB J. 2020, 34, 11200–11214. [Google Scholar] [CrossRef]
- Stern, J.M.; Burk, R.D.; Asplin, J.; Krieger, N.S.; Suadicani, S.O.; Wang, Y.; Usyk, M.; Lee, J.A.; Chen, L.; Becker, J.; et al. Kidney stone formation and the gut microbiome are altered by antibiotics in genetic hypercalciuric stone-forming rats. Urolithiasis 2021, 49, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Tian, L.; Liu, Y.; Xu, X.; Jiao, P.; Hu, G.; Cui, Y.; Chen, J.; Ma, Y.; Jin, X.; Wang, K.; et al. Lactiplantibacillus plantarum J-15 reduced calcium oxalate kidney stones by regulating intestinal microbiota, metabolism, and inflammation in rats. FASEB J. 2022, 36, e22340. [Google Scholar] [CrossRef]
- Wang, Y.; Sun, J.; Xie, S.; Zhou, Y.; Wang, T.; Liu, Z.; Li, C.; Gao, L.; Pan, T. Increased abundance of bacteria of the family Muribaculaceae achieved by fecal microbiome transplantation correlates with the inhibition of kidney calcium oxalate stone deposition in experimental rats. Front. Cell Infect. Microbiol. 2023, 13, 1145196. [Google Scholar] [CrossRef]
- Coffey, E.L.; Gomez, A.M.; Burton, E.N.; Granick, J.L.; Lulich, J.P.; Furrow, E. Characterization of the urogenital microbiome in Miniature Schnauzers with and without calcium oxalate urolithiasis. J. Vet. Intern. Med. 2022, 36, 1341–1352. [Google Scholar] [CrossRef]
- Kachroo, N.; Lange, D.; Penniston, K.L.; Stern, J.; Tasian, G.; Bajic, P.; Wolfe, A.J.; Suryavanshi, M.; Ticinesi, A.; Meschi, T.; et al. Standardization of microbiome studies for urolithiasis: An international consensus agreement. Nat. Rev. Urol. 2021, 18, 303–311. [Google Scholar] [CrossRef]
- Fraher, M.H.; O’Toole, P.W.; Quigley, E.M. Techniques used to characterize the gut microbiota: A guide for the clinician. Nat. Rev. Gastroenterol. Hepatol. 2012, 9, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Lemberger, U.; Pjevac, P.; Hausmann, B.; Berry, D.; Moser, D.; Jahrreis, V.; Ozsoy, M.; Shariat, S.F.; Veser, J. The microbiome of kidney stones and urine of patients with nephrolithiasis. Urolithiasis 2023, 51, 27. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.R-project.org (accessed on 23 April 2024).
- Suryavanshi, M.V.; Bhute, S.S.; Jadhav, S.D.; Bhatia, M.S.; Gune, R.P.; Shouche, Y.S. Hyperoxaluria leads to dysbiosis and drives selective enrichment of oxalate metabolizing bacterial species in recurrent kidney stone endures. Sci. Rep. 2016, 6, 34712. [Google Scholar] [CrossRef] [PubMed]
- Tang, R.; Jiang, Y.; Tan, A.; Ye, J.; Xian, X.; Xie, Y.; Wang, Q.; Yao, Z.; Mo, Z. 16S rRNA gene sequencing reveals altered composition of gut microbiota in individuals with kidney stones. Urolithiasis 2018, 46, 503–514. [Google Scholar] [CrossRef]
- Chen, F.; Bao, X.; Liu, S.; Ye, K.; Xiang, S.; Yu, L.; Xu, Q.; Zhang, Y.; Wang, X.; Zhu, X.; et al. Gut microbiota affect the formation of calcium oxalate renal calculi caused by high daily tea consumption. Appl. Microbiol. Biotechnol. 2021, 105, 789–802. [Google Scholar] [CrossRef] [PubMed]
- Zhao, E.; Zhang, W.; Geng, B.; You, B.; Wang, W.; Li, X. Intestinal dysbacteriosis leads to kidney stone disease. Mol. Med. Rep. 2021, 23, 180. [Google Scholar] [CrossRef]
- Xiang, L.; Jin, X.; Liu, Y.; Ma, Y.; Jian, Z.; Wei, Z.; Li, H.; Li, Y.; Wang, K. Prediction of the occurrence of calcium oxalate kidney stones based on clinical and gut microbiota characteristics. World J. Urol. 2022, 40, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Yuan, C.; Jin, X.; He, Y.; Liu, Y.; Xiang, L.; Wang, K. Association of dietary patterns with gut microbiota in kidney stone and non-kidney stone individuals. Urolithiasis 2022, 50, 389–399. [Google Scholar] [CrossRef]
- Ellison, J.S.; Atkinson, S.N.; Hayward, M.; Hokanson, E.; Sheridan, K.R.; Salzman, N. The intestinal microbiome of children with initial and recurrent nephrolithiasis: A pilot study and exploratory analysis. J. Pediatr. Urol. 2024, 20, 18–25. [Google Scholar] [CrossRef]
- Dethlefsen, L.; Huse, S.; Sogin, M.L.; Relman, D.A. The pervasive effects of an antibiotic on the human gut microbiota, as revealed by deep 16S rRNA sequencing. PLoS Biol. 2008, 6, e280. [Google Scholar] [CrossRef]
- Panda, S.; El khader, I.; Casellas, F.; Lopez Vivancos, J.; Garcia Cors, M.; Santiago, A.; Cuenca, S.; Guarner, F.; Manichanh, C. Short-term effect of antibiotics on human gut microbiota. PLoS ONE 2014, 9, e95476. [Google Scholar] [CrossRef]
- Schell, M.A.; Karmirantzou, M.; Snel, B.; Vilanova, D.; Berger, B.; Pessi, G.; Zwahlen, M.C.; Desiere, F.; Bork, P.; Delley, M.; et al. The genome sequence of Bifidobacterium longum reflects its adaptation to the human gastrointestinal tract. Proc. Natl. Acad. Sci. USA 2002, 99, 14422–14427. [Google Scholar] [CrossRef] [PubMed]
- Federici, F.; Vitali, B.; Gotti, R.; Pasca, M.R.; Gobbi, S.; Peck, A.B.; Brigidi, P. Characterization and heterologous expression of the oxalyl coenzyme A decarboxylase gene from Bifidobacterium lactis. Appl. Environ. Microbiol. 2004, 70, 5066–5073. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, P.; Curtis, N. The effect of antibiotics on the composition of the intestinal microbiota—A systematic review. J. Infect. 2019, 79, 471–489. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, J.; Guarner, F.; Bustos Fernandez, L.; Maruy, A.; Sdepanian, V.L.; Cohen, H. Antibiotics as Major Disruptors of Gut Microbiota. Front. Cell Infect. Microbiol. 2020, 10, 572912. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Zhang, Y.; Wu, J.; Gao, M.; Zhu, Z.; Chen, H. Causal relationship between kidney stones and gut microbiota contributes to the gut-kidney axis: A two-sample Mendelian randomization study. Front. Microbiol. 2023, 14, 1204311. [Google Scholar] [CrossRef] [PubMed]
- Stegemann, M.R.; Sherington, J.; Coati, N.; Brown, S.A.; Blanchflower, S. Pharmacokinetics of cefovecin in cats. J. Vet. Pharmacol. Ther. 2006, 29, 513–524. [Google Scholar] [CrossRef] [PubMed]
- Joshi, S.; Goldfarb, D.S. The use of antibiotics and risk of kidney stones. Curr. Opin. Nephrol. Hypertens. 2019, 28, 311–315. [Google Scholar] [CrossRef]
- Miller, A.W.; Orr, T.; Dearing, D.; Monga, M. Loss of function dysbiosis associated with antibiotics and high fat, high sugar diet. ISME J. 2019, 13, 1379–1390. [Google Scholar] [CrossRef]
- Tasian, G.; Miller, A.; Lange, D. Antibiotics and Kidney Stones: Perturbation of the Gut-Kidney Axis. Am. J. Kidney Dis. 2019, 74, 724–726. [Google Scholar] [CrossRef]
- Tasian, G.E.; Jemielita, T.; Goldfarb, D.S.; Copelovitch, L.; Gerber, J.S.; Wu, Q.; Denburg, M.R. Oral Antibiotic Exposure and Kidney Stone Disease. J. Am. Soc. Nephrol. 2018, 29, 1731–1740. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, P.M.; Curhan, G.C.; Gambaro, G.; Taylor, E.N. Antibiotic Use and Risk of Incident Kidney Stones in Female Nurses. Am. J. Kidney Dis. 2019, 74, 736–741. [Google Scholar] [CrossRef]
- Zampini, A.; Nguyen, A.H.; Rose, E.; Monga, M.; Miller, A.W. Defining Dysbiosis in Patients with Urolithiasis. Sci. Rep. 2019, 9, 5425. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, A.J.; Brubaker, L. “Sterile Urine” and the Presence of Bacteria. Eur. Urol. 2015, 68, 173–174. [Google Scholar] [CrossRef] [PubMed]
- Tang, J. Microbiome in the urinary system-a review. AIMS Microbiol. 2017, 3, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, A.J.; Brubaker, L. Urobiome updates: Advances in urinary microbiome research. Nat. Rev. Urol. 2019, 16, 73–74. [Google Scholar] [CrossRef] [PubMed]
- Dornbier, R.A.; Bajic, P.; Van Kuiken, M.; Jardaneh, A.; Lin, H.; Gao, X.; Knudsen, B.; Dong, Q.; Wolfe, A.J.; Schwaderer, A.L. The microbiome of calcium-based urinary stones. Urolithiasis 2020, 48, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Suarez Arbelaez, M.C.; Monshine, J.; Porto, J.G.; Shah, K.; Singh, P.K.; Roy, S.; Amin, K.; Marcovich, R.; Herrmann, T.R.W.; Shah, H.N. The emerging role of the urinary microbiome in benign noninfectious urological conditions: An up-to-date systematic review. World J. Urol. 2023, 41, 2933–2948. [Google Scholar] [CrossRef]
- Balboni, A.; Franzo, G.; Bano, L.; De Arcangeli, S.; Rizzardi, A.; Urbani, L.; Segatore, S.; Serafini, F.; Dondi, F.; Battilani, M. Culture-Dependent and Sequencing Methods Revealed the Absence of a Bacterial Community Residing in the Urine of Healthy Cats. Front. Vet. Sci. 2020, 7, 438. [Google Scholar] [CrossRef] [PubMed]
- Lund, H.S.; Skogtun, G.; Sørum, H.; Eggertsdóttir, A.V. Absence of bacterial DNA in culture-negative urine from cats with and without lower urinary tract disease. J. Feline Med. Surg. 2015, 17, 909–914. [Google Scholar] [CrossRef]
- Kim, Y.; Carrai, M.; Leung, M.H.Y.; Chin, J.; Li, J.; Lee, P.K.H.; Beatty, J.A.; Pfeiffer, D.U.; Barrs, V.R. Dysbiosis of the Urinary Bladder Microbiome in Cats with Chronic Kidney Disease. mSystems 2021, 6, e0051021. [Google Scholar] [CrossRef] [PubMed]
- Burton, E.N.; Cohn, L.A.; Reinero, C.N.; Rindt, H.; Moore, S.G.; Ericsson, A.C. Characterization of the urinary microbiome in healthy dogs. PLoS ONE 2017, 12, e0177783. [Google Scholar] [CrossRef] [PubMed]
- Mrofchak, R.; Madden, C.; Evans, M.V.; Hale, V.L. Evaluating extraction methods to study canine urine microbiota. PLoS ONE 2021, 16, e0253989. [Google Scholar] [CrossRef] [PubMed]
- Coffey, E.L.; Gomez, A.M.; Ericsson, A.C.; Burton, E.N.; Granick, J.L.; Lulich, J.P.; Furrow, E. The impact of urine collection method on canine urinary microbiota detection: A cross-sectional study. BMC Microbiol. 2023, 23, 101. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.; Huang, J.S.; Huang, X.J.; Peng, J.M.; Yu, Z.; Yuan, Y.Q.; Xiao, K.F.; Guo, J.N. Profiling the urinary microbiome in men with calcium-based kidney stones. BMC Microbiol. 2020, 20, 41. [Google Scholar] [CrossRef] [PubMed]
- Kachroo, N.; Monga, M.; Miller, A.W. Comparative functional analysis of the urinary tract microbiome for individuals with or without calcium oxalate calculi. Urolithiasis 2022, 50, 303–317. [Google Scholar] [CrossRef] [PubMed]
- Flannigan, R.; Choy, W.H.; Chew, B.; Lange, D. Renal struvite stones--pathogenesis, microbiology, and management strategies. Nat. Rev. Urol. 2014, 11, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Chutipongtanate, S.; Sutthimethakorn, S.; Chiangjong, W.; Thongboonkerd, V. Bacteria can promote calcium oxalate crystal growth and aggregation. J. Biol. Inorg. Chem. 2013, 18, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Jewell, D.E.; Tavener, S.K.; Hollar, R.L.; Panickar, K.S. Metabolomic changes in cats with renal disease and calcium oxalate uroliths. Metabolomics 2022, 18, 68. [Google Scholar] [CrossRef]
- Galan-Llopis, J.A.; Sanchez-Pellicer, P.; Navarro-Lopez, V. Role of microbiome in kidney stone disease. Curr. Opin. Urol. 2023, 33, 84–89. [Google Scholar] [CrossRef]
- Hall, J.A.; Jackson, M.I.; Jewell, D.E.; Ephraim, E. Chronic kidney disease in cats alters response of the plasma metabolome and fecal microbiome to dietary fiber. PLoS ONE 2020, 15, e0235480. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Unno, T.; Kim, B.Y.; Park, M.S. Sex Differences in Gut Microbiota. World J. Mens. Health 2020, 38, 48–60. [Google Scholar] [CrossRef] [PubMed]
- Zhernakova, A.; Kurilshikov, A.; Bonder, M.J.; Tigchelaar, E.F.; Schirmer, M.; Vatanen, T.; Mujagic, Z.; Vila, A.V.; Falony, G.; Vieira-Silva, S.; et al. Population-based metagenomics analysis reveals markers for gut microbiome composition and diversity. Science 2016, 352, 565–569. [Google Scholar] [CrossRef] [PubMed]
- Erik, I.; Peter, C.; Jim, L.; John, L.; Anna, P.; Srinivasa Vittal, K. Causal inference and effect estimation using observational data. J. Epidemiol. Community Health 2022, 76, 960. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Joubran, P.; Roux, F.A.; Serino, M.; Deschamps, J.-Y. Gut and Urinary Microbiota in Cats with Kidney Stones. Microorganisms 2024, 12, 1098. https://doi.org/10.3390/microorganisms12061098
Joubran P, Roux FA, Serino M, Deschamps J-Y. Gut and Urinary Microbiota in Cats with Kidney Stones. Microorganisms. 2024; 12(6):1098. https://doi.org/10.3390/microorganisms12061098
Chicago/Turabian StyleJoubran, Patrick, Françoise A. Roux, Matteo Serino, and Jack-Yves Deschamps. 2024. "Gut and Urinary Microbiota in Cats with Kidney Stones" Microorganisms 12, no. 6: 1098. https://doi.org/10.3390/microorganisms12061098
APA StyleJoubran, P., Roux, F. A., Serino, M., & Deschamps, J.-Y. (2024). Gut and Urinary Microbiota in Cats with Kidney Stones. Microorganisms, 12(6), 1098. https://doi.org/10.3390/microorganisms12061098