
Insights into Pathogenesis of Trachoma

 , , and
, , and
Abstract
:1. Introduction
2. The Causative Agent
3. Transmission
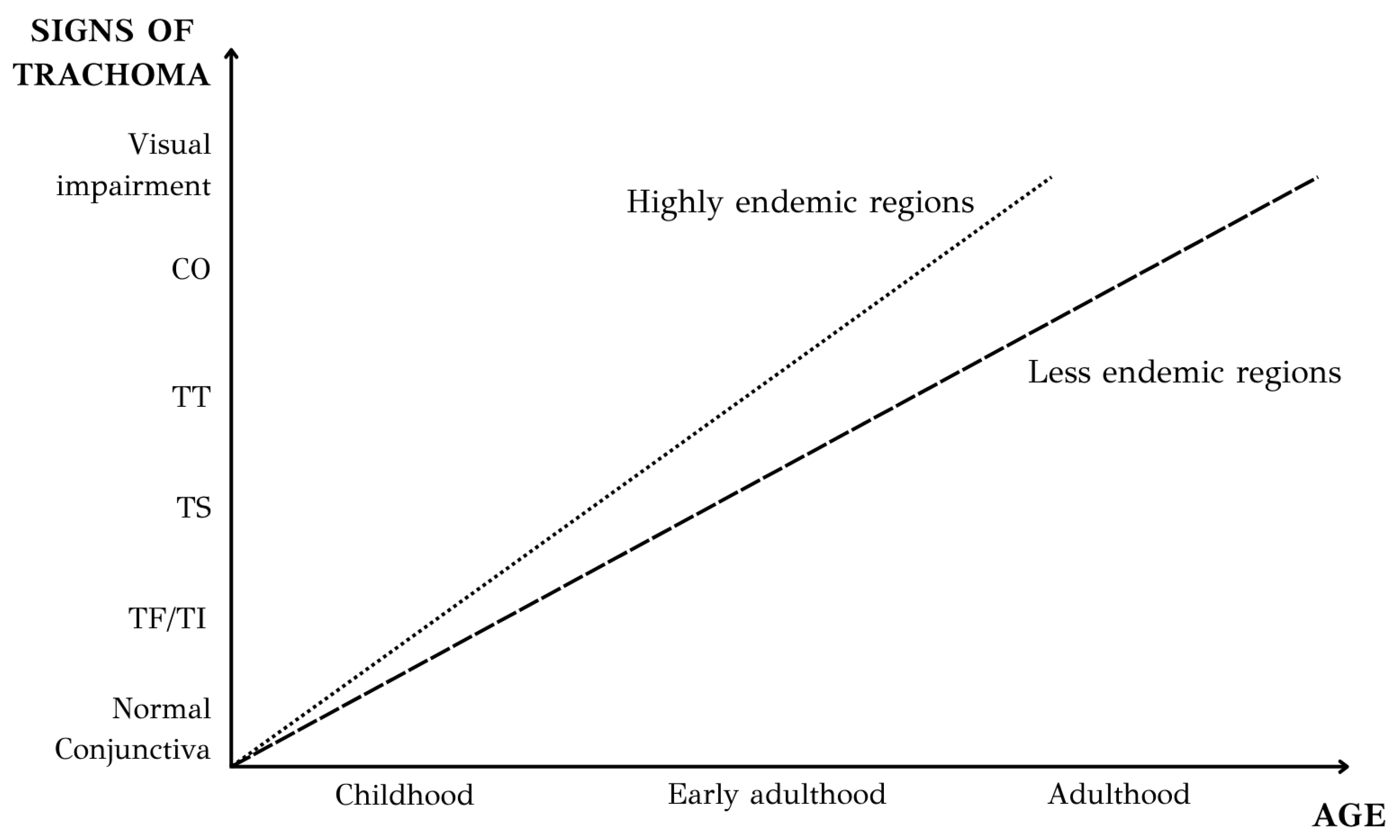
4. Natural History and Clinical Features of Trachoma
- Trachomatous Follicular (TF) inflammation: The stage of active trachoma with predominantly follicular inflammation. Diagnosing this stage requires the presence of at least five or more follicles on the upper tarsal conjunctiva, each measuring 0.5 mm or more in diameter.
- Trachomatous Intense (TI) inflammation: This stage of active trachoma is identified when significant inflammatory thickening of the upper tarsal conjunctiva obscures more than half of the normal deep tarsal vessels. The tarsal conjunctiva displays a reddish hue, a coarse texture, and increased thickness—the results of papillary hypertrophy. It should be mentioned that the key sign for the diagnosis of TI is thickened, velvety edematous conjunctiva, not redness.
- Trachomatous Scarring (TS): This stage is identified through the detection of scarring in the tarsal conjunctiva, which is apparent as white lines, bands, or sheets (fibrosis) in the tarsal conjunctiva. Typically, the scars exhibit a shiny and fibrous appearance, featuring straight, angular, or feathered edges. Scarring, particularly diffuse fibrosis, might obscure the blood vessels in the tarsal area, but it is crucial not to mistake this for diffuse inflammatory thickening.
- Trachomatous Trichiasis (TT): This stage is identified when at least one eyelash from the upper eyelid rubs on the eyeball, or there is evidence of recent removal of in-turned eyelashes from the upper eyelid.
- Corneal Opacity (CO): This stage is recognized when there is a clearly visible corneal opacity covering the pupil. The corneal opacity is so dense that at least part of the pupil margin is blurred when viewed through the opacity. This definition aims to identify corneal opacities that result in substantial visual impairment (Figure 4).
5. Histopathology and Immunopathology
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Flaxman, S.R.; Bourne, R.R.A.; Resnikoff, S.; Ackland, P.; Braithwaite, T.; Cicinelli, M.V.; Das, A.; Jonas, J.B.; Keeffe, J.; Kempen, J.H.; et al. Global causes of blindness and distance vision impairment 1990–2020: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e1221–e1234. [Google Scholar] [CrossRef] [PubMed]
- Solomon, A.W.; Burton, M.J.; Gower, E.W.; Harding-Esch, E.M.; Oldenburg, C.E.; Taylor, H.R.; Traore, L. Trachoma. Nat. Rev. Dis. Primers 2022, 8, 32. [Google Scholar] [CrossRef]
- World Health Organization. Trachoma. Available online: https://www.who.int/news-room/fact-sheets/detail/trachoma (accessed on 1 April 2024).
- World Health Organization. Ending the Neglect to Attain the Sustainable Development Goals: A Road Map for Neglected Tropical Diseases 2021–2030. Available online: https://www.who.int/publications/i/item/9789240052932 (accessed on 2 April 2024).
- Yaghoobi, G.; Anani Sarab, G. The History of Trachoma and Current Prevalence (Spotlight on Iran): A Review Article. Iran. J. Public Health 2018, 47, 1458–1465. [Google Scholar] [PubMed]
- Fan, H.; Scidmore, M.A. Chlamydia. In Reference Module in Biomedical Sciences; Elsevier: Amsterdam, The Netherlands, 2015. [Google Scholar] [CrossRef]
- Jury, B.; Fleming, C.; Huston, W.M.; Luu, L.D.W. Molecular pathogenesis of Chlamydia trachomatis. Front. Cell. Infect. Microbiol. 2023, 13, 1281823. [Google Scholar] [CrossRef] [PubMed]
- Hepler, R.W.; Nahas, D.D.; Lucas, B.; Kaufhold, R.; Flynn, J.A.; Galli, J.D.; Swoyer, R.; Wagner, J.M.; Espeseth, A.S.; Joyce, J.G.; et al. Spectroscopic analysis of chlamydial major outer membrane protein in support of structure elucidation. Protein Sci. 2018, 27, 1923–1941. [Google Scholar] [CrossRef]
- Grygiel-Gorniak, B.; Folga, B.A. Chlamydia trachomatis—An Emerging Old Entity? Microorganisms 2023, 11, 1283. [Google Scholar] [CrossRef] [PubMed]
- Lesiak-Markowicz, I.; Schotta, A.M.; Stockinger, H.; Stanek, G.; Markowicz, M. Chlamydia trachomatis serovars in urogenital and ocular samples collected 2014–2017 from Austrian patients. Sci. Rep. 2019, 9, 18327. [Google Scholar] [CrossRef] [PubMed]
- Makker, K.; Nassar, G.N.; Kaufman, E.J. Neonatal Conjunctivitis. In StatPearls; Ineligible Companies: Treasure Island, FL, USA, 2024. [Google Scholar]
- Lee, W.A.; Chen, C.C. Adult inclusion conjunctivitis diagnosed by polymerase chain reaction and Giemsa stain. IDCases 2022, 27, e01367. [Google Scholar] [CrossRef] [PubMed]
- Abdelsamed, H.; Peters, J.; Byrne, G.I. Genetic variation in Chlamydia trachomatis and their hosts: Impact on disease severity and tissue tropism. Future Microbiol. 2013, 8, 1129–1146. [Google Scholar] [CrossRef]
- Fehlner-Gardiner, C.; Roshick, C.; Carlson, J.H.; Hughes, S.; Belland, R.J.; Caldwell, H.D.; McClarty, G. Molecular basis defining human Chlamydia trachomatis tissue tropism. A possible role for tryptophan synthase. J. Biol. Chem. 2002, 277, 26893–26903. [Google Scholar] [CrossRef]
- Caldwell, H.D.; Wood, H.; Crane, D.; Bailey, R.; Jones, R.B.; Mabey, D.; Maclean, I.; Mohammed, Z.; Peeling, R.; Roshick, C.; et al. Polymorphisms in Chlamydia trachomatis tryptophan synthase genes differentiate between genital and ocular isolates. J. Clin. Investig. 2003, 111, 1757–1769. [Google Scholar] [CrossRef] [PubMed]
- Elwell, C.; Mirrashidi, K.; Engel, J. Chlamydia cell biology and pathogenesis. Nature reviews. Microbiology 2016, 14, 385–400. [Google Scholar]
- Versteeg, B.; Vasileva, H.; Houghton, J.; Last, A.; Shafi Abdurahman, O.; Sarah, V.; Macleod, D.; Solomon, A.W.; Holland, M.J.; Thomson, N.; et al. Viability PCR shows that non-ocular surfaces could contribute to transmission of Chlamydia trachomatis infection in trachoma. PLoS Negl. Trop. Dis. 2020, 14, e0008449. [Google Scholar] [CrossRef] [PubMed]
- Last, A.; Versteeg, B.; Shafi Abdurahman, O.; Robinson, A.; Dumessa, G.; Abraham Aga, M.; Shumi Bejiga, G.; Negussu, N.; Greenland, K.; Czerniewska, A.; et al. Detecting extra-ocular Chlamydia trachomatis in a trachoma-endemic community in Ethiopia: Identifying potential routes of transmission. PLoS Negl. Trop. Dis. 2020, 14, e0008120. [Google Scholar] [CrossRef]
- Emerson, P.M.; Lindsay, S.W.; Alexander, N.; Bah, M.; Dibba, S.M.; Faal, H.B.; Lowe, K.O.; McAdam, K.P.; Ratcliffe, A.A.; Walraven, G.E.; et al. Role of flies and provision of latrines in trachoma control: Cluster-randomised controlled trial. Lancet 2004, 363, 1093–1098. [Google Scholar] [CrossRef]
- Brewer, N.; McKenzie, M.S.; Melkonjan, N.; Zaky, M.; Vik, R.; Stoffolano, J.G.; Webley, W.C. Persistence and Significance of Chlamydia trachomatis in the Housefly, Musca domestica L. Vector Borne Zoonotic Dis. 2021, 21, 854–863. [Google Scholar] [CrossRef]
- Robinson, A.; Bristow, J.; Holl, M.V.; Makalo, P.; Alemayehu, W.; Bailey, R.L.; Macleod, D.; Birkett, M.A.; Caulfield, J.C.; Sarah, V.; et al. Responses of the putative trachoma vector, Musca sorbens, to volatile semiochemicals from human faeces. PLoS Negl. Trop. Dis. 2020, 14, e0007719. [Google Scholar] [CrossRef]
- Ageed, A.; Khan, M. Eliminating Trachoma in Africa: The Importance of Environmental Interventions. Cureus 2024, 16, e52358. [Google Scholar] [CrossRef]
- Chen, X.; Munoz, B.; Wolle, M.A.; Woods, G.; Odonkor, M.; Naufal, F.; Mkocha, H.; West, S.K. Environmental factors and hygiene behaviors associated with facial cleanliness and trachoma in Kongwa, Tanzania. PLoS Negl. Trop. Dis. 2021, 15, e0009902. [Google Scholar] [CrossRef] [PubMed]
- Churko, C.; Asfaw, M.A.; Zerdo, Z. Knowledge, Attitude, Practices and Associated Factors towards Trachoma among People Living in Arba Minch Zuria District, Gamo Zone, Southern Ethiopia. Clin. Ophthalmol. 2021, 15, 3075–3085. [Google Scholar] [CrossRef]
- Bailey, R.; Osmond, C.; Mabey, D.C.; Whittle, H.C.; Ward, M.E. Analysis of the household distribution of trachoma in a Gambian village using a Monte Carlo simulation procedure. Int. J. Epidemiol. 1989, 18, 944–951. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, B.; Patel, B.C. Trachoma. In StatPearls; StatPearls Publishing Copyright © 2024; StatPearls Publishing LLC/Ineligible Companies: Treasure Island, FL, USA, 2024. [Google Scholar]
- Wright, H.R.; Taylor, H.R. Clinical examination and laboratory tests for estimation of trachoma prevalence in a remote setting: What are they really telling us? Lancet Infect. Dis. 2005, 5, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Grassly, N.C.; Ward, M.E.; Ferris, S.; Mabey, D.C.; Bailey, R.L. The natural history of trachoma infection and disease in a Gambian cohort with frequent follow-up. PLoS Negl. Trop. Dis. 2008, 2, e341. [Google Scholar] [CrossRef] [PubMed]
- Gambhir, M.; Basáñez, M.G.; Burton, M.J.; Solomon, A.W.; Bailey, R.L.; Holland, M.J.; Blake, I.M.; Donnelly, C.A.; Jabr, I.; Mabey, D.C.; et al. The development of an age-structured model for trachoma transmission dynamics, pathogenesis and control. PLoS Negl. Trop. Dis. 2009, 3, e462. [Google Scholar] [CrossRef] [PubMed]
- Hu, V.H.; Holland, M.J.; Burton, M.J. Trachoma: Protective and pathogenic ocular immune responses to Chlamydia trachomatis. PLoS Negl. Trop. Dis. 2013, 7, e2020. [Google Scholar] [CrossRef] [PubMed]
- Hu, V.H.; Weiss, H.A.; Ramadhani, A.M.; Tolbert, S.B.; Massae, P.; Mabey, D.C.; Holland, M.J.; Bailey, R.L.; Burton, M.J. Innate immune responses and modified extracellular matrix regulation characterize bacterial infection and cellular/connective tissue changes in scarring trachoma. Infect. Immun. 2012, 80, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Burton, M.J.; Rajak, S.N.; Bauer, J.; Weiss, H.A.; Tolbert, S.B.; Shoo, A.; Habtamu, E.; Manjurano, A.; Emerson, P.M.; Mabey, D.C.; et al. Conjunctival transcriptome in scarring trachoma. Infect. Immun. 2011, 79, 499–511. [Google Scholar] [CrossRef] [PubMed]
- Hu, V.H.; Macleod, D.; Massae, P.; Afwamba, I.; Weiss, H.A.; Mabey, D.C.W.; Bailey, R.L.; Burton, M.J. Non-Chlamydial Bacterial Infection and Progression of Conjunctival Scarring in Trachoma. Investig. Ophthalmol. Vis. Sci. 2018, 59, 2339–2344. [Google Scholar] [CrossRef] [PubMed]
- Rajak, S.N.; Habtamu, E.; Weiss, H.A.; Bedri, A.; Gebre, T.; Bailey, R.L.; Mabey, D.C.; Khaw, P.T.; Gilbert, C.E.; Emerson, P.M.; et al. The clinical phenotype of trachomatous trichiasis in Ethiopia: Not all trichiasis is due to entropion. Investig. Ophthalmol. Vis. Sci. 2011, 52, 7974–7980. [Google Scholar] [CrossRef]
- Bowman, R.J.; Faal, H.; Myatt, M.; Adegbola, R.; Foster, A.; Johnson, G.J.; Bailey, R.L. Longitudinal study of trachomatous trichiasis in the Gambia. Br. J. Ophthalmol. 2002, 86, 339–343. [Google Scholar] [CrossRef]
- Burton, M.J.; Bowman, R.J.; Faal, H.; Aryee, E.A.; Ikumapayi, U.N.; Alexander, N.D.; Adegbola, R.A.; Mabey, D.C.; Foster, A.; Johnson, G.J.; et al. The long-term natural history of trachomatous trichiasis in the Gambia. Investig. Ophthalmol. Vis. Sci. 2006, 47, 847–852. [Google Scholar] [CrossRef] [PubMed]
- Burton, M.J.; Kinteh, F.; Jallow, O.; Sillah, A.; Bah, M.; Faye, M.; Aryee, E.A.; Ikumapayi, U.N.; Alexander, N.D.; Adegbola, R.A.; et al. A randomised controlled trial of azithromycin following surgery for trachomatous trichiasis in the Gambia. Br. J. Ophthalmol. 2005, 89, 1282–1288. [Google Scholar] [CrossRef] [PubMed]
- Solomon, A.W.; Kello, A.B.; Bangert, M.; West, S.K.; Taylor, H.R.; Tekeraoi, R.; Foster, A. The simplified trachoma grading system, amended. Bull. World Health Organ. 2020, 98, 698–705. [Google Scholar] [CrossRef] [PubMed]
- West, S.K.; Munoz, B.; Turner, V.M.; Mmbaga, B.B.; Taylor, H.R. The epidemiology of trachoma in central Tanzania. Int. J. Epidemiol. 1991, 20, 1088–1092. [Google Scholar] [CrossRef] [PubMed]
- Ngondi, J.; Onsarigo, A.; Adamu, L.; Matende, I.; Baba, S.; Reacher, M.; Emerson, P.; Zingeser, J. The epidemiology of trachoma in Eastern Equatoria and Upper Nile States, southern Sudan. Bull. World Health Organ. 2005, 83, 904–912. [Google Scholar] [PubMed]
- Ngondi, J.; Gebre, T.; Shargie, E.B.; Adamu, L.; Ejigsemahu, Y.; Teferi, T.; Zerihun, M.; Ayele, B.; Cevallos, V.; King, J.; et al. Evaluation of three years of the SAFE strategy (Surgery, Antibiotics, Facial cleanliness and Environmental improvement) for trachoma control in five districts of Ethiopia hyperendemic for trachoma. Trans. R. Soc. Trop. Med. Hyg. 2009, 103, 1001–1010. [Google Scholar] [CrossRef] [PubMed]
- Gebrie, A.; Alebel, A.; Zegeye, A.; Tesfaye, B.; Wagnew, F. Prevalence and associated factors of active trachoma among children in Ethiopia: A systematic review and meta-analysis. BMC Infect. Dis. 2019, 19, 1073. [Google Scholar] [CrossRef] [PubMed]
- Solomon, A.W.; Holland, M.J.; Burton, M.J.; West, S.K.; Alexander, N.D.; Aguirre, A.; Massae, P.A.; Mkocha, H.; Muñoz, B.; Johnson, G.J.; et al. Strategies for control of trachoma: Observational study with quantitative PCR. Lancet 2003, 362, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Taylor, H.R.; Siler, J.A.; Mkocha, H.A.; Muñoz, B.; Velez, V.; Dejong, L.; West, S. Longitudinal study of the microbiology of endemic trachoma. J. Clin. Microbiol. 1991, 29, 1593–1595. [Google Scholar] [CrossRef]
- Congdon, N.; West, S.; Vitale, S.; Katala, S.; Mmbaga, B.B. Exposure to children and risk of active trachoma in Tanzanian women. Am. J. Epidemiol. 1993, 137, 366–372. [Google Scholar] [CrossRef]
- Dolin, P.J.; Faal, H.; Johnson, G.J.; Ajewole, J.; Mohamed, A.A.; Lee, P.S. Trachoma in the Gambia. Br. J. Ophthalmol. 1998, 82, 930–933. [Google Scholar] [CrossRef]
- Courtright, P.; Sheppard, J.; Schachter, J.; Said, M.E.; Dawson, C.R. Trachoma and blindness in the Nile Delta: Current patterns and projections for the future in the rural Egyptian population. Br. J. Ophthalmol. 1989, 73, 536–540. [Google Scholar] [CrossRef] [PubMed]
- Shumway, C.L.; Motlagh, M.; Wade, M. Anatomy, Head and Neck, Eye Conjunctiva. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- el-Asrar, A.M.; Van den Oord, J.J.; Geboes, K.; Missotten, L.; Emarah, M.H.; Desmet, V. Immunopathology of trachomatous conjunctivitis. Br. J. Ophthalmol. 1989, 73, 276–282. [Google Scholar] [CrossRef]
- Abu el-Asrar, A.M.; Geboes, K.; al-Kharashi, S.A.; Tabbara, K.F.; Missotten, L. Collagen content and types in trachomatous conjunctivitis. Eye 1998, 12 Pt 4, 735–739. [Google Scholar] [CrossRef]
- al-Rajhi, A.A.; Hidayat, A.; Nasr, A.; al-Faran, M. The histopathology and the mechanism of entropion in patients with trachoma. Ophthalmology 1993, 100, 1293–1296. [Google Scholar] [CrossRef] [PubMed]
- Hu, V.H.; Holland, M.J.; Cree, I.A.; Pullin, J.; Weiss, H.A.; Massae, P.; Makupa, W.; Mabey, D.C.; Bailey, R.L.; Burton, M.J.; et al. In vivo confocal microscopy and histopathology of the conjunctiva in trachomatous scarring and normal tissue: A systematic comparison. Br. J. Ophthalmol. 2013, 97, 1333–1337. [Google Scholar] [CrossRef]
- Hu, V.H.; Luthert, P.J.; Derrick, T.; Pullin, J.; Weiss, H.A.; Massae, P.; Mtuy, T.; Makupa, W.; Essex, D.; Mabey, D.C.; et al. Immunohistochemical Analysis of Scarring Trachoma Indicates Infiltration by Natural Killer and Undefined CD45 Negative Cells. PLoS Negl. Trop. Dis. 2016, 10, e0004734. [Google Scholar] [CrossRef] [PubMed]
- Derrick, T.; Luthert, P.J.; Jama, H.; Hu, V.H.; Massae, P.; Essex, D.; Holland, M.J.; Burton, M.J. Increased Epithelial Expression of CTGF and S100A7 with Elevated Subepithelial Expression of IL-1β in Trachomatous Trichiasis. PLoS Negl. Trop. Dis. 2016, 10, e0004752. [Google Scholar] [CrossRef]
- Stephens, R.S. The cellular paradigm of chlamydial pathogenesis. Trends Microbiol. 2003, 11, 44–51. [Google Scholar] [CrossRef]
- Rasmussen, S.J.; Eckmann, L.; Quayle, A.J.; Shen, L.; Zhang, Y.X.; Anderson, D.J.; Fierer, J.; Stephens, R.S.; Kagnoff, M.F. Secretion of proinflammatory cytokines by epithelial cells in response to Chlamydia infection suggests a central role for epithelial cells in chlamydial pathogenesis. J. Clin. Investig. 1997, 99, 77–87. [Google Scholar] [CrossRef]
- Burton, M.J.; Bailey, R.L.; Jeffries, D.; Mabey, D.C.; Holland, M.J. Cytokine and fibrogenic gene expression in the conjunctivas of subjects from a Gambian community where trachoma is endemic. Infect. Immun. 2004, 72, 7352–7356. [Google Scholar] [CrossRef] [PubMed]
- Natividad, A.; Freeman, T.C.; Jeffries, D.; Burton, M.J.; Mabey, D.C.; Bailey, R.L.; Holland, M.J. Human conjunctival transcriptome analysis reveals the prominence of innate defense in Chlamydia trachomatis infection. Infect. Immun. 2010, 78, 4895–4911. [Google Scholar] [CrossRef] [PubMed]
- Ramadhani, A.M.; Derrick, T.; Macleod, D.; Massae, P.; Mtuy, T.; Jeffries, D.; Roberts, C.H.; Bailey, R.L.; Mabey, D.C.W.; Holland, M.J.; et al. Immunofibrogenic Gene Expression Patterns in Tanzanian Children with Ocular Chlamydia trachomatis Infection, Active Trachoma and Scarring: Baseline Results of a 4-Year Longitudinal Study. Front. Cell. Infect. Microbiol. 2017, 7, 406. [Google Scholar] [CrossRef] [PubMed]
- Taylor, H.R.; Johnson, S.L.; Schachter, J.; Caldwell, H.D.; Prendergast, R.A. Pathogenesis of trachoma: The stimulus for inflammation. J. Immunol. 1987, 138, 3023–3027. [Google Scholar] [CrossRef] [PubMed]
- Vicetti Miguel, R.D.; Quispe Calla, N.E.; Pavelko, S.D.; Cherpes, T.L. Intravaginal Chlamydia trachomatis Challenge Infection Elicits TH1 and TH17 Immune Responses in Mice That Promote Pathogen Clearance and Genital Tract Damage. PLoS ONE 2016, 11, e0162445. [Google Scholar] [CrossRef] [PubMed]
- Burton, M.J.; Rajak, S.N.; Hu, V.H.; Ramadhani, A.; Habtamu, E.; Massae, P.; Tadesse, Z.; Callahan, K.; Emerson, P.M.; Khaw, P.T.; et al. Pathogenesis of progressive scarring trachoma in Ethiopia and Tanzania and its implications for disease control: Two cohort studies. PLoS Negl. Trop. Dis. 2015, 9, e0003763. [Google Scholar] [CrossRef]
- Natividad, A.; Cooke, G.; Holland, M.J.; Burton, M.J.; Joof, H.M.; Rockett, K.; Kwiatkowski, D.P.; Mabey, D.C.; Bailey, R.L. A coding polymorphism in matrix metalloproteinase 9 reduces risk of scarring sequelae of ocular Chlamydia trachomatis infection. BMC Med. Genet. 2006, 7, 40. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biovars | Serovars | Main Diseases |
|---|---|---|
| Trachoma | A–C * | Trachoma |
| Genital | D–K | Neonatal conjunctivitis Adult inclusion conjunctivitis Pneumonia (neonates) |
| LGV | L1–L3 | LGV |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toumasis, P.; Vrioni, G.; Tsinopoulos, I.T.; Exindari, M.; Samonis, G. Insights into Pathogenesis of Trachoma. Microorganisms 2024, 12, 1544. https://doi.org/10.3390/microorganisms12081544
Toumasis P, Vrioni G, Tsinopoulos IT, Exindari M, Samonis G. Insights into Pathogenesis of Trachoma. Microorganisms. 2024; 12(8):1544. https://doi.org/10.3390/microorganisms12081544
Chicago/Turabian StyleToumasis, Panagiotis, Georgia Vrioni, Ioannis T. Tsinopoulos, Maria Exindari, and George Samonis. 2024. "Insights into Pathogenesis of Trachoma" Microorganisms 12, no. 8: 1544. https://doi.org/10.3390/microorganisms12081544