
Oral Factors That Impact the Oral Microbiota in Parkinson’s Disease

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject Population and Study Design
2.2. Oral Health and Demographics Data Collection
2.3. Microbiota Sample Collection
2.4. Bacterial Community Sequencing and Analysis
2.5. Statistical Analysis for Demographics and Oral Health
3. Results
3.1. Subject Characteristics
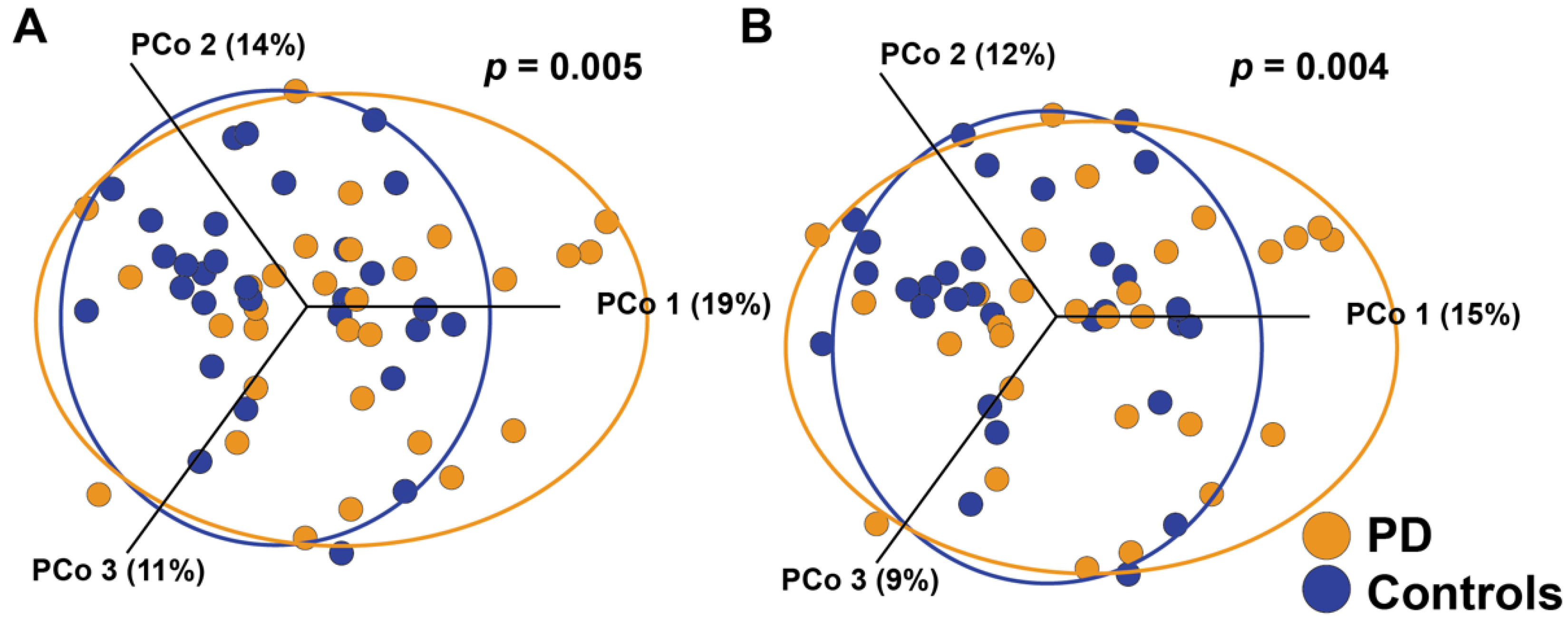
3.2. Microbiota Diversity
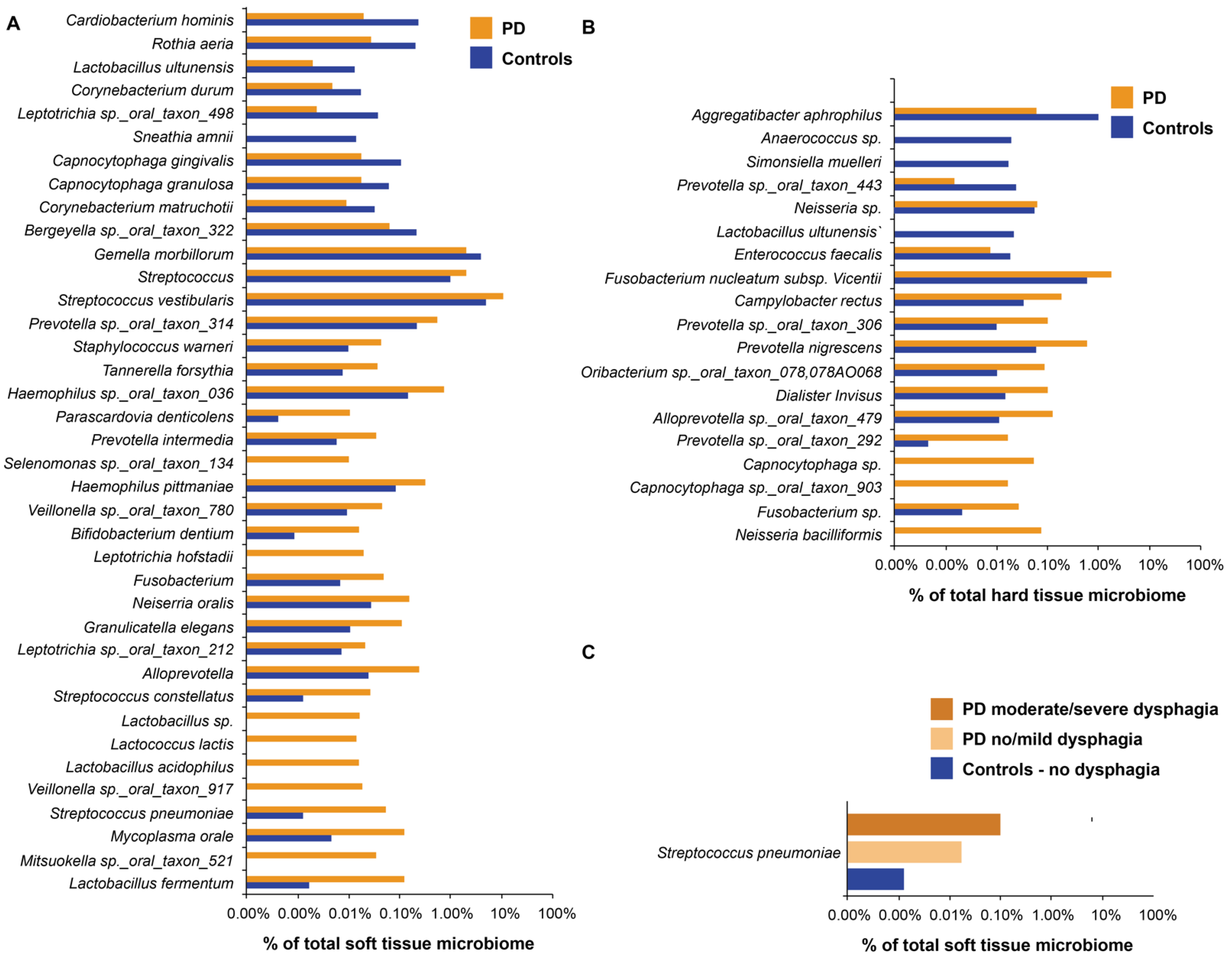
3.3. Soft Tissue Community Abundance
3.4. Hard Tissue Community Abundance
3.5. Disease Features with Impact on the Oral Microbiota in PD
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dorsey, E.R.; Elbaz, A.; Nichols, E.; Abd-Allah, F.; Abdelalim, A.; Adsuar, J.C.; Ansha, M.G.; Brayne, C.; Choi, J.-Y.J.; Collado-Mateo, D.; et al. Global, regional, and national burden of Parkinson’s disease, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 939–953. [Google Scholar] [CrossRef] [Green Version]
- Jeter, C.B.; Rozas, N.S.; Sadowsky, J.M.; Jones, D.J. Parkinson’s Disease Oral Health Module: Interprofessional Coordination of Care. MedEdPORTAL J. Teach. Learn. Resour. 2018, 14, 10699. [Google Scholar] [CrossRef] [PubMed]
- Barbe, A.G.; Bock, N.; Derman, S.H.M.; Felsch, M.; Timmermann, L.; Noack, M.J. Self-assessment of oral health, dental health care and oral health-related quality of life among Parkinson’s disease patients. Gerodontology 2017, 34, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Rozas, N.S.; Sadowsky, J.M.; Jones, D.J.; Jeter, C.B. Incorporating oral health into interprofessional care teams for patients with Parkinson’s disease. Parkinsonism Relat. Disord. 2017, 43, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Pradeep, A.R.; Singh, S.P.; Martande, S.S.; Raju, A.P.; Rustagi, T.; Suke, D.K.; Naik, S.B. Clinical evaluation of the periodontal health condition and oral health awareness in Parkinson’s disease patients. Gerodontology 2015, 32, 100–106. [Google Scholar] [CrossRef]
- Einarsdóttir, E.R.; Gunnsteinsdóttir, H.; Hallsdóttir, M.H.; Sveinsson, S.; Jónsdóttir, S.R.; Ólafsson, V.G.; Bragason, T.H.; Sæmundsson, S.R.; Holbrook, W.P. Dental health of patients with Parkinson’s disease in Iceland. Spec. Care Dent. 2009, 29, 123–127. [Google Scholar] [CrossRef]
- Nakayama, Y.; Washio, M.; Mori, M. Oral health conditions in patients with Parkinson’s disease. J. Epidemiol. 2004, 14, 143–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wade, W.G. The oral microbiome in health and disease. Pharmacol. Res. 2013, 69, 137–143. [Google Scholar] [CrossRef]
- Pereira, P.A.B.; Aho, V.T.E.; Paulin, L.; Pekkonen, E.; Auvinen, P.; Scheperjans, F. Oral and nasal microbiota in Parkinson’s disease. Park. Relat. Disord. 2017, 38, 61–67. [Google Scholar] [CrossRef] [Green Version]
- Mihaila, D.; Donegan, J.; Barns, S.; LaRocca, D.; Du, Q.; Zheng, D.; Vidal, M.; Neville, C.; Uhlig, R.; Middleton, F.A. The oral microbiome of early stage Parkinson’s disease and its relationship with functional measures of motor and non-motor function. PLoS ONE 2019, 14, e0218252. [Google Scholar] [CrossRef]
- Fleury, V.; Zekeridou, A.; Lazarevic, V.; Gaïa, N.; Giannopoulou, C.; Genton, L.; Cancela, J.; Girard, M.; Goldstein, R.; Bally, J.F.; et al. Oral Dysbiosis and Inflammation in Parkinson’s Disease. J. Parkinsons. Dis. 2021, 11, 619–631. [Google Scholar] [CrossRef]
- Batista, L.M.; Portela de Oliveira, M.T.; Magalhaes, W.B.; Bastos, P.L. Oral Hygiene in Patients with Parkinson’s Disease. R. I. Med. J. 2015, 98, 35–37. [Google Scholar]
- Carneiro, D.; das Graças Wanderley de Sales Coriolano, M.; Belo, L.R.; de Marcos Rabelo, A.R.; Asano, A.G.; Lins, O.G. Quality of life related to swallowing in Parkinson’s disease. Dysphagia 2014, 29, 578–582. [Google Scholar] [CrossRef]
- Suttrup, I.; Warnecke, T. Dysphagia in Parkinson’ s Disease. Dys 2016, 31, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Pinter, B.; Diem-Zangerl, A.; Wenning, G.K.; Scherfler, C.; Oberaigner, W.; Seppi, K.; Poewe, W. Mortality in Parkinson’s disease: A 38-year follow-up study. Mov. Disord. 2015, 30, 266–269. [Google Scholar] [CrossRef]
- Goh, K.-H.; Acharyya, S.; Ng, S.Y.-E.; Boo, J.P.-L.; Kooi, A.H.-J.; Ng, H.-L.; Li, W.; Tay, K.-Y.; Au, W.-L.; Tan, L.C.-S. Risk and prognostic factors for pneumonia and choking amongst Parkinson’s disease patients with dysphagia. Parkinsonism Relat. Disord. 2016, 29, 30–34. [Google Scholar] [CrossRef]
- Ortega, O.; Sakwinska, O.; Combremont, S.; Berger, B.; Sauser, J.; Parra, C.; Zarcero, S.; Nart, J.; Carrión, S.; Clavé, P. High prevalence of colonization of oral cavity by respiratory pathogens in frail older patients with oropharyngeal dysphagia. Neurogastroenterol. Motil. 2015, 27, 1804–1816. [Google Scholar] [CrossRef]
- Kalf, J.G.; Borm, G.F.; de Swart, B.J.; Bloem, B.R.; Zwarts, M.J.; Munneke, M. Reproducibility and validity of patient-rated assessment of speech, swallowing, and saliva control in Parkinson’s disease. Arch. Phys. Med. Rehabil. 2011, 92, 1152–1158. [Google Scholar] [CrossRef]
- Kayser-Jones, J.; Bird, W.F.; Paul, S.M.; Long, L.; Schell, E.S. An instrument to assess the oral health status of nursing home residents. Gerontologist 1995, 35, 814–824. [Google Scholar] [CrossRef]
- Greene, J.G.; Vermillion, J.R. The Simplified Oral Hygiene Index. J. Am. Dent. Assoc. 1964, 68, 7–13. [Google Scholar] [CrossRef]
- Rozas, N.S.; Sadowsky, J.M.; Stanek, J.A.; Jeter, C.B. Oral Health Assessment by Lay Personnel for Older Adults. J. Vis. Exp. 2020. [Google Scholar] [CrossRef]
- Human Microbiome Project Consortium. Structure, function and diversity of the healthy human microbiome. Nature 2012, 486, 207–214. [Google Scholar] [CrossRef] [Green Version]
- Chen, T.; Yu, W.; Izard, J.; Baranova, O.V.; Lakshmanan, A.; Dewhirst, F.E. The Human Oral Microbiome Database: A web accessible resource for investigating oral microbe taxonomic and genomic information. Database 2010, 2010, baq013. [Google Scholar] [CrossRef]
- Socransky, S.S.; Haffajee, A.D. Periodontal microbial ecology. Periodontology 2005, 38, 135–187. [Google Scholar] [CrossRef] [PubMed]
- Müller, T.; Palluch, R.; Ackowski, J.J. Caries and periodontal disease in patients with Parkinson’s disease. Spec. Care Dent. 2011, 31, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.L.; Park, M. Socioeconomic and racial/ethnic oral health disparities among US older adults: Oral health quality of life and dentition. J. Public Health Dent. 2015, 75, 85–92. [Google Scholar] [CrossRef] [Green Version]
- Sharma, N.; Bhatia, S.; Sodhi, A.S.; Batra, N. Oral microbiome and health. AIMS Microbiol. 2018, 4, 42–66. [Google Scholar] [CrossRef] [PubMed]
- Bakke, M.; Larsen, S.L.; Lautrup, C.; Karlsborg, M. Orofacial function and oral health in patients with Parkinson’s disease. Eur. J. Oral Sci. 2011, 119, 27–32. [Google Scholar] [CrossRef]
- DeBowes, S.L.; Tolle, S.L.; Bruhn, A.M. Parkinson’s disease: Considerations for dental hygienists. Int. J. Dent. Hyg. 2013, 11, 15–21. [Google Scholar] [CrossRef]
- Hill-burns, E.M.; Debelius, J.W.; Morton, J.T.; Wissemann, W.T.; Lewis, M.R.; Wallen, Z.D.; Peddada, S.D.; Factor, S.A.; Molho, E.; Zabetian, C.P.; et al. Parkinson’s Disease and Parkinson’s Disease Medications Have Distinct Signatures of the Gut Microbiome. Mov. Disord. 2017, 32, 739–749. [Google Scholar] [CrossRef]
- Kalf, J.G.; de Swart, B.J.M.; Bloem, B.R.; Munneke, M. Prevalence of oropharyngeal dysphagia in Parkinson’s disease: A meta-analysis. Parkinsonism Relat. Disord. 2012, 18, 311–315. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| PD (n = 30) | Controls (n = 30) | p-Value † | Jaccard p-Value | Bray-Curtis p-Value | Weighted Unifrac p-Value | Unweighted Unifrac p-Value | |
|---|---|---|---|---|---|---|---|
| Gender (%) | 0.43 | 0.97 | 0.97 | 0.81 | 0.63 | ||
| Female | 37 | 43 | |||||
| Male | 63 | 57 | |||||
| Age (years, mean ± SD) | 69.2 ± 9.4 | 69.1 ± 8.4 | 0.94 | 0.76 | 0.76 | 0.67 | 0.80 |
| Race/Ethnicity (%) | 0.13 | 0.06 | 0.10 | 0.11 | 0.46 | ||
| Black | 17 | 17 | |||||
| Hispanic/Latino | 10 | 20 | |||||
| White | 73 | 63 | |||||
| Education (%) | 0.42 | 0.85 | 0.86 | 0.94 | 0.37 | ||
| ≤High school diploma | 27 | 33.3 | |||||
| Some college/Associates degree | 23 | 33.3 | |||||
| ≥Bachelor’s degree | 50 | 33.3 | |||||
| BMI (mean ± SD) | 27 ± 6.0 | 28.6 ± 6.6 | 0.33 | 0.8 | 0.8 | 0.9 | 0.5 |
| PD Medications (%) | 0.04 ‡,* | 0.03 ‡,* | 0.36 ‡ | 0.66 ‡ | |||
| Levadopa and/or Carbidopa | 63 | 0 | |||||
| COMT inhibitor | 20 | 0 | |||||
| Dopamine agonist | 13 | 0 | |||||
| MAO inhibitor | 17 | 0 | |||||
| Aticholinergic | 3 | 0 | |||||
| None | 30 | 100 | |||||
| Other medications (%) | |||||||
| Aspirin | 20 | 43 | 0.03 * | 0.21 | 0.27 | 0.25 | 0.10 |
| Statins (heart disease) | 13 | 30 | 0.12 | 0.48 | 0.54 | 0.25 | 0.23 |
| Metformin (diabetes) | 6 | 23 | 0.07 | 0.16 | 0.17 | 0.49 | 0.05 |
| Levothyroxine sodium (thyroid) | 3 | 23 | 0.02 * | 0.52 | 0.48 | 0.60 | 0.89 |
| PD (n = 30) | Controls (n = 30) | p-Value † | Jaccard p-Value | Bray-Curtis p-Value | Weighted Unifrac p-Value | Unweighted Unifrac p-Value | |
|---|---|---|---|---|---|---|---|
| Total BOHSE (mean ± SD) | 4.61 ± 0.5 | 2.97 ± 0.5 | 0.02 * | 0.14 | 0.17 | 0.03 * | 0.31 |
| OHI-S (mean ± SD) | |||||||
| Before TB | 1.6 ± 0.13 | 1.0 ± 0.16 | 0.006 * | 0.84 | 0.83 | 0.94 | 0.19 |
| After TB | 0.54 ± 0.08 | 0.39 ± 0.11 | 0.29 | 0.53 | 0.45 | 0.84 | 0.16 |
| Total Change | 1 ± 0.1 | 0.62 ± 0.1 | 0.01 * | 0.85 | 0.90 | 0.99 | 0.12 |
| ROMP (mean ± SD) | |||||||
| Swallowing score | 11.5 ± 1.0 | 7.0 ± 0.03 | <0.001 * | 0.02 * | 0.02 * | 0.04 * | 0.19 |
| Saliva score | 15.8 ± 1.3 | 9.2 ± 0.1 | <0.001 * | 0.19 | 0.17 | 0.02 * | 0.03 * |
| Salivary pH (mean ± SD) | 6.7 ± 0.19 | 7.1 ± 0.16 | 0.08 | 0.001 * | <0.001 * | 0.001 * | 0.004 * |
| Oral hygiene (%) | |||||||
| TB ≥ 2X/day | 60 | 73 | 0.27 | 0.69 | 0.68 | 0.71 | 0.69 |
| Flosses ≥ 1X/day | 47 | 50 | 0.80 | 0.21 | 0.28 | 0.42 | 0.14 |
| Dental visits ≥ 2X/year | 57 | 50 | 0.60 | 0.12 | 0.16 | 0.09 | 0.12 |
| Diet (%) | |||||||
| Eats ≥ 4 snacks/day | 23 | 3 | 0.02 * | 0.12 | 0.13 | 0.13 | 0.15 |
| Never eats foods with sugar added | 13 | 40 | 0.02 * | 0.55 | 0.58 | 0.55 | 0.27 |
| Never sugary drinks | 33 | 20 | 0.24 | 0.11 | 0.13 | 0.27 | 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rozas, N.S.; Tribble, G.D.; Jeter, C.B. Oral Factors That Impact the Oral Microbiota in Parkinson’s Disease. Microorganisms 2021, 9, 1616. https://doi.org/10.3390/microorganisms9081616
Rozas NS, Tribble GD, Jeter CB. Oral Factors That Impact the Oral Microbiota in Parkinson’s Disease. Microorganisms. 2021; 9(8):1616. https://doi.org/10.3390/microorganisms9081616
Chicago/Turabian StyleRozas, Natalia S., Gena D. Tribble, and Cameron B. Jeter. 2021. "Oral Factors That Impact the Oral Microbiota in Parkinson’s Disease" Microorganisms 9, no. 8: 1616. https://doi.org/10.3390/microorganisms9081616
APA StyleRozas, N. S., Tribble, G. D., & Jeter, C. B. (2021). Oral Factors That Impact the Oral Microbiota in Parkinson’s Disease. Microorganisms, 9(8), 1616. https://doi.org/10.3390/microorganisms9081616