Prospective Randomized Controlled Clinical Trial of the Long-Term Effects of Omeprazole on Healthy Dogs

 , ,
, , {kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Design
2.3. Sample Collection
2.4. Statistical Analysis
3. Results
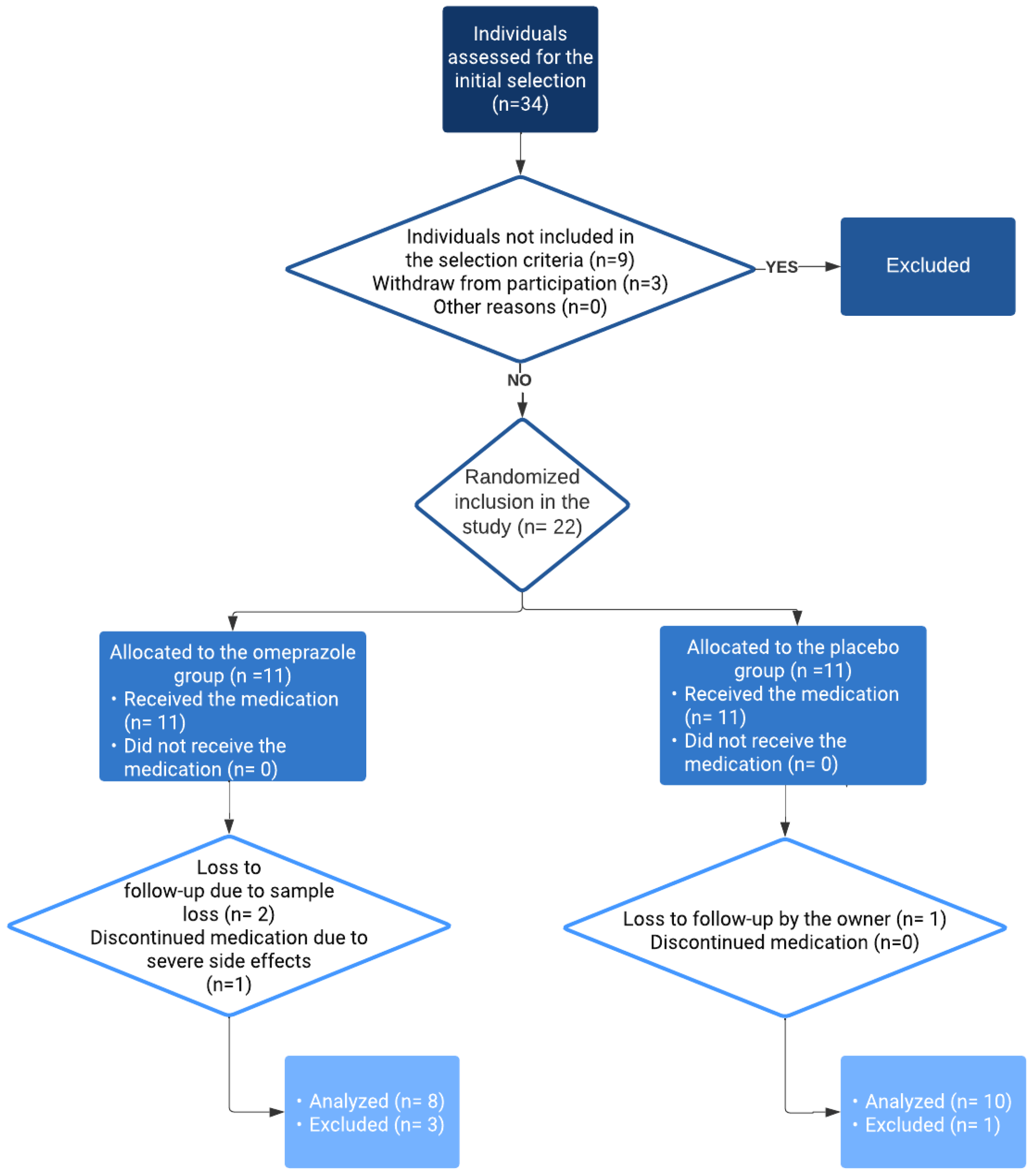
3.1. Study Population
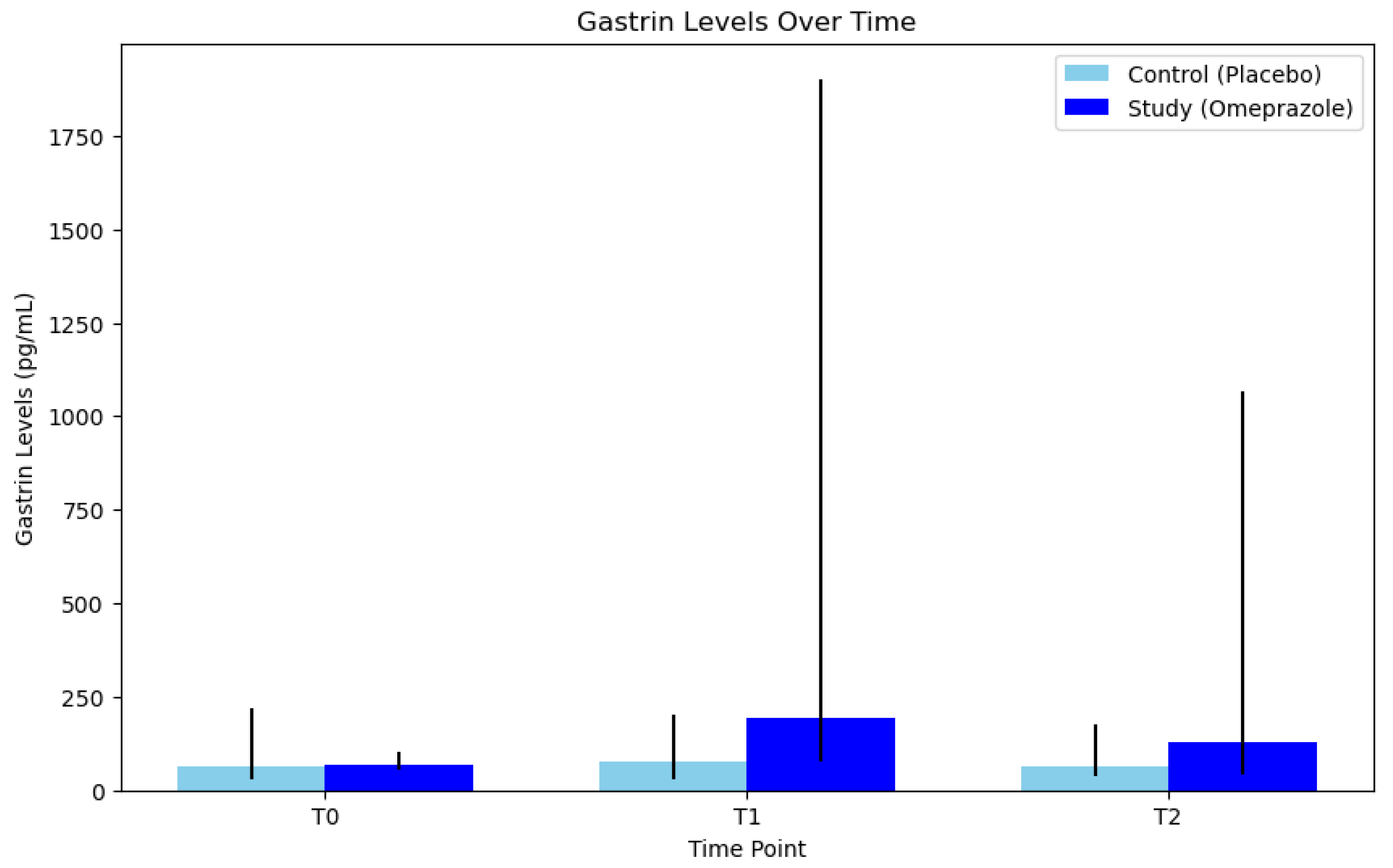
3.2. Serum Gastrin Levels
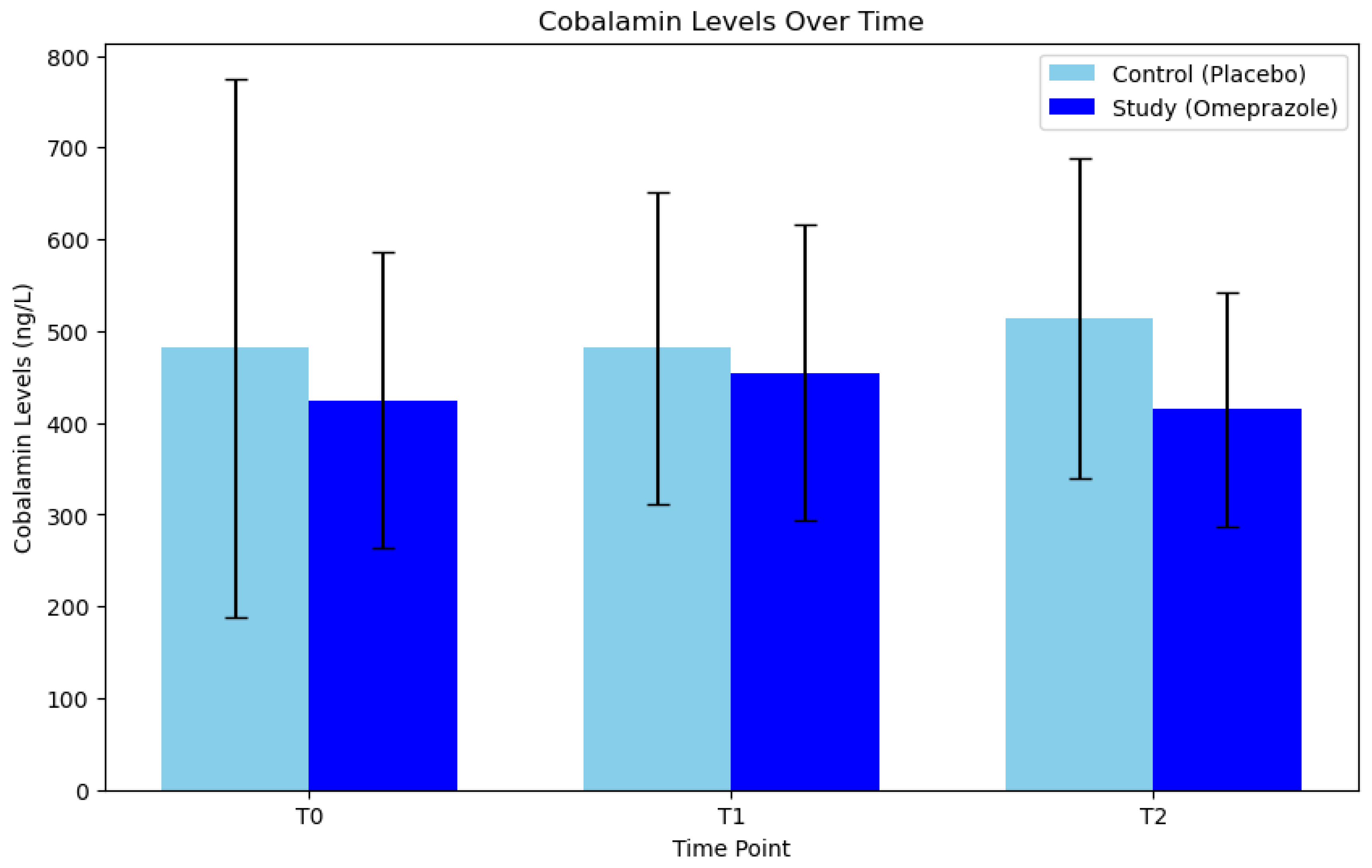
3.3. Serum Cobalamin Levels
3.4. Adverse Effects Related to Omeprazole Administration
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marks, S.L.; Kook, P.H.; Papich, M.G.; Tolbert, M.K.; Willard, M.D. ACVIM Consensus Statement: Support for Rational Administration of Gastrointestinal Protectants to Dogs and Cats. J. Vet. Intern. Med. 2018, 32, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Shaevitz, M.H.; Moore, G.E.; Fulkerson, C.M. A Prospective, Randomized, Placebo-Controlled, Double-Blinded Clinical Trial Comparing the Incidence and Severity of Gastrointestinal Adverse Events in Dogs with Cancer Treated with Piroxicam Alone or in Combination with Omeprazole or Famotidine. J. Am. Vet. Med. Assoc. 2021, 259, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Rak, M.B.; Moyers, T.D.; Price, J.M.; Whittemore, J.C. Clinicopathologic and Gastrointestinal Effects of Administration of Prednisone, Prednisone with Omeprazole, or Prednisone with Probiotics to Dogs: A Double-Blind Randomized Trial. J. Vet. Intern. Med. 2023, 37, 465–475. [Google Scholar] [CrossRef]
- Jones, S.M.; Gaier, A.; Enomoto, H.; Ishii, P.; Pilla, R.; Price, J.; Suchodolski, J.; Steiner, J.M.; Papich, M.G.; Messenger, K.; et al. The Effect of Combined Carprofen and Omeprazole Administration on Gastrointestinal Permeability and Inflammation in Dogs. J. Vet. Intern. Med. 2020, 34, 1886–1893. [Google Scholar] [CrossRef] [PubMed]
- Tuukkanen, J.; Väänänen, H.K. Omeprazole, a Specific Inhibitor of H+-K +-ATPase, Inhibits Bone Resorption In Vitro. Calcif. Tissue Int. 1986, 38, 123–125. [Google Scholar] [CrossRef]
- Yavuz, O.; Arslan, H.H. Proton Pump Inhibitors in Veterinary Medicine. Am. J. Anim. Vet. Sci. 2017, 12, 132–138. [Google Scholar] [CrossRef]
- Gould, E.; Clements, C.; Reed, A.; Giori, L.; Steiner, J.M.; Lidbury, J.A.; Suchodolski, J.S.; Brand, M.; Moyers, T.; Emery, L.; et al. A Prospective, Placebo-Controlled Pilot Evaluation of the Effect of Omeprazole on Serum Calcium, Magnesium, Cobalamin, Gastrin Concentrations, and Bone in Cats. J. Vet. Intern. Med. 2016, 30, 779–786. [Google Scholar] [CrossRef] [PubMed]
- Koyyada, A. Long-Term Use of Proton Pump Inhibitors as a Risk Factor for Various Adverse Manifestations. Therapies 2021, 76, 13–21. [Google Scholar] [CrossRef]
- Lane, M.B.; Larson, J.C.; Stokes, J.E.; Tolbert, M.K. Small Animals & Exotic Continuous Radiotelemetric Monitoring of Intragastric PH in a Dog with Peptic Ulceration. J. Am. Vet. Med. Assoc. 2017, 250, 530–533. [Google Scholar] [CrossRef]
- McAtee, R.; Schmid, S.M.; Tolbert, M.K.; Hetzel, S.; Suchodolski, J.S.; Pritchard, J.C. Effect of Esomeprazole with and without a Probiotic on Fecal Dysbiosis, Intestinal Inflammation, and Fecal Short-Chain Fatty Acid Concentrations in Healthy Dogs. J. Vet. Intern. Med. 2023, 37, 2109–2118. [Google Scholar] [CrossRef]
- Tolbert, M.K.; Olin, S.; MacLane, S.; Gould, E.; Steiner, J.M.; Vaden, S.; Price, J. Evaluation of Gastric PH and Serum Gastrin Concentrations in Cats with Chronic Kidney Disease. J. Vet. Intern. Med. 2017, 31, 1414–1419. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, N. Risk of Long-Term Treatment with Proton Pump Inhibitors. Rev. Prat. 2008, 58, 1451–1454. [Google Scholar] [PubMed]
- Heilmann, R.M.; Berghoff, N.; Grützner, N.; Parnell, N.K.; Suchodolski, J.S.; Steiner, J.M. Effect of Gastric Acid-Suppressive Therapy and Biological Variation of Serum Gastrin Concentrations in Dogs with Chronic Enteropathies. BMC Vet. Res. 2017, 13, 321–332. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Mazcorro, J.F.; Suchodolski, J.S.; Jones, K.R.; Clark-Price, S.C.; Dowd, S.E.; Minamoto, Y.; Markel, M.; Steiner, J.M.; Dossin, O. Effect of the Proton Pump Inhibitor Omeprazole on the Gastrointestinal Bacterial Microbiota of Healthy Dogs. FEMS Microbiol. Ecol. 2012, 80, 624–636. [Google Scholar] [CrossRef]
- Leonard, J.; Marshall, J.K.; Moayyedi, P. Systematic Review of the Risk of Enteric Infection in Patients Taking Acid Suppression. Am. J. Gastroenterol. 2007, 102, 2047–2056. [Google Scholar] [CrossRef]
- Sullivan, L.A.; Wakayama, J.; Boscan, P.L.; Hyatt, D.R.; Twedt, D.C.; Lappin, M.R.; Dargatz, D.A. The Effects of Omeprazole Therapy on Bacterial Colonization of the Pharynx in Healthy Dogs. J. Vet. Emerg. Crit. Care 2016, 26, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Dear, J.D. Bacterial Pneumonia in Dogs and Cats: An Update. Vet. Clin. N. Am. Small Anim. Pract. 2020, 50, 447–465. [Google Scholar] [CrossRef]
- Gupta, R.; Garg, P.; Kottoor, R.; Carlos Munoz, J.; Mazen Jamal, M.; Lambiase, L.R.; Vega, K.J. Overuse of Acid Suppression Therapy in Hospitalized Patients. South. Med. J. 2010, 103, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Hayes, K.N.; Nakhla, N.R.; Tadrous, M. Further Evidence to Monitor Long-Term Proton Pump Inhibitor Use. JAMA Netw. Open 2019, 2, 1916184. [Google Scholar] [CrossRef]
- Duxbury, S.; Sorah, E.; Tolbert, M.K. Evaluation of Proton Pump Inhibitor Administration in Hospitalized Dogs in a Tertiary Referral Hospital. J. Vet. Intern. Med. 2022, 36, 1622–1627. [Google Scholar] [CrossRef]
- Betesh, A.L.; Santa Ana, C.A.; Cole, J.A.; Fordtran, J.S. Is Achlorhydria a Cause of Iron Deficiency Anemia? Am. J. Clin. Nutr. 2015, 102, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Haffner-Luntzer, M.; Heilmann, A.; Heidler, V.; Liedert, A.; Schinke, T.; Amling, M.; Yorgan, T.A.; Vom Scheidt, A.; Ignatius, A. Hypochlorhydria-Induced Calcium Malabsorption Does Not Affect Fracture Healing but Increases Post-Traumatic Bone Loss in the Intact Skeleton. J. Orthop. Res. 2016, 34, 1914–1921. [Google Scholar] [CrossRef]
- Friis-Hansen, L. Achlorhydria Is Associated with Gastric Microbial Overgrowth and Development of Cancer: Lessons Learned from the Gastrin Knockout Mouse. Scan J. Clin. Lab. Investig. 2006, 66, 607–622. [Google Scholar] [CrossRef]
- Paimela, H.; Goddard, P.J.; Silen, W. Present Views on Restitution of Gastrointestinal Epithelium. Dig. Dis. Sci. 1995, 40, 2495–2496. [Google Scholar] [CrossRef] [PubMed]
- Wallace, J.L.; Granger, D.N. The Cellular and Molecular Basis of Gastric Mucosal Defense. FASER J. 1996, 10, 731–740. [Google Scholar] [CrossRef] [PubMed]
- Kawano, S.; Tsuji, S. Role of Mucosal Blood Flow: A Conceptional Review in Gastric Mucosal Injury and Protection. J. Gastroenterol. Hepatol. 2000, 15, D1–D6. [Google Scholar] [CrossRef]
- Mccormack, R.; Olley, L.; Glanemann, B.; Swann, J.W. Prospective Observational Study of the Use of Omeprazole and Maropitant Citrate in Veterinary Specialist Care. Sci. Rep. 2020, 20, 15727. [Google Scholar] [CrossRef]
- Parente, N.L.; Bari Olivier, N.; Refsal, K.R.; Johnson, C.A. Serum Concentrations of Gastrin after Famotidine and Omeprazole Administration to Dogs. J. Vet. Intern. Med. 2014, 28, 1465–1470. [Google Scholar] [CrossRef]
- Lee, S.H.; Kim, J.W.; Lee, B.C.; Oh, H.J. Age-Specifi Variations in Hematological and Biochemical Parameters in Middle- and Large-Sized of Dogs. J. Vet. Sci. 2020, 21, e7. [Google Scholar] [CrossRef]
- Waldum, H.L.; Sørdal, Ø.; Fossmark, R. Proton Pump Inhibitors (PPIs) May Cause Gastric Cancer–Clinical Consequences. Scand. J. Gastroenterol. 2018, 53, 639–642. [Google Scholar] [CrossRef]
- Fossmark, R.; Qvigstad, G.; Waldum, H.L. Gastric Cancer: Animal Studies on the Risk of Hypoacidity and Hypergastrinemia. World J. Gastroenterol. 2008, 14, 1646–1651. [Google Scholar] [CrossRef] [PubMed]
- Hakanson, R.; Blom, H.; Carlsson, E.; Larsson, H.; Ryberg, B.; Sundler, F. Hypergastrinaemia Produces Trophic Effects in Stomach but Not in Pancreas and Intestines. Regul. Pept. 1986, 13, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Sundlera, F.; Hakansona Carlssonb, R.E.; Larssonb, H.; Mattssonb, H. Hypergastrinemia after Blockade of Acid Secretion in the Rat: Trophic Effects. Digestion 1986, 35, 56–69. [Google Scholar] [CrossRef] [PubMed]
- Larsson, H.; Carlsson, E.; Mattsson, H.; Lundell, L.; Sundler, F.; Sundell, G.; Wallmark, B.; Watanabe, T.; Håkanson, R. Plasma Gastrin and Gastric Enterochromaffinlike Cell Activation and Proliferation. Studies with Omeprazole and Ranitidine in Intact and Antrectomized Rats. Gastroenterology 1986, 90, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Termanini, B.; Gibril, F.; Sutliff, V.E.; Yu, F.; Venzon, D.J.; Jensen, R.T. Effect of Long-Term Gastric Acid Suppressive Therapy on Serum Vitamin B 12 Levels in Patients with Zollinger-Ellison Syndrome. Am. J. Med. 1998, 104, 422–430. [Google Scholar] [CrossRef] [PubMed]
- Saltzman, J.R.; Kowdley, K.V.; Pedrosa, M.C.; Sepe, T.; Golner, B.; Perrone, G.; Russell, R.M. Bacterial Overgrowth Without Clinical Hypochlorhydric Subjects Malabsorption in Elderly. Gastroenterology 1994, 106, 615–623. [Google Scholar] [CrossRef] [PubMed]
- Marcuard, S.P.; Albernaz, L.; Khazanie, P.G.; East, F. Omeprazole Therapy Causes Malabsorption of Cyanocobalamin (Vitamin B 12). Ann. Intern. Med. 1994, 120, 211–215. [Google Scholar] [CrossRef]
- Den Elzen, W.P.J.; Groeneveld, Y.; De Ruijter, W.; Souverijn, J.H.M.; Le Cessieà, S.; Assendelft, W.J.J.; Gussekloo, J. Long-Term Use of Proton Pump Inhibitors and Vitamin B12 Status in Elderly Individuals. Aliment. Pharmacol. Ther. 2008, 27, 491–497. [Google Scholar] [CrossRef]
- Qorraj-Bytyqi, H.; Hoxha, R.; Sadiku, S.; Bajraktari, I.H.; Sopjani, M.; Thaçi, K.; Thaçi, S.; Bahtiri, E. Proton Pump Inhibitors Intake and Iron and Vitamin B12 Status: A Prospective Comparative Study with a Follow up of 12 Months. J. Med. Sci. 2018, 6, 442–446. [Google Scholar] [CrossRef]
- Williamson, K.; Payton, M.; Davis, M. Efficacy of Omeprazole versus High-Dose Famotidine for Prevention of Exercise-Induced Gastritis in Racing Alaskan Sled Dogs. J. Vet. Intern. Med. 2010, 24, 285–288. [Google Scholar] [CrossRef]
- Wallace, J.L.; Syer, S.; Denou, E.; De Palma, G.; Vong, L.; McKnight, W.; Jury, J.; Bolla, M.; Bercik, P.; Collins, S.M.; et al. Proton Pump Inhibitors Exacerbate NSAID-Induced Small Intestinal Injury by Inducing Dysbiosis. Gastroenterology 2011, 141, 1314–1322. [Google Scholar] [CrossRef] [PubMed]
- Lo, W.K.; Chan, W.W. Proton Pump Inhibitor Use and the Risk of Small Intestinal Bacterial Overgrowth: A Meta-Analysis. Clin. Gastroenterol. Hepatol. 2013, 11, 483–490. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gil-Vicente, L.; Martín, G.; Soler, C.; Vila, A.; Saiz, M.R.; Navarro, P.F. Prospective Randomized Controlled Clinical Trial of the Long-Term Effects of Omeprazole on Healthy Dogs. Animals 2024, 14, 1168. https://doi.org/10.3390/ani14081168
Gil-Vicente L, Martín G, Soler C, Vila A, Saiz MR, Navarro PF. Prospective Randomized Controlled Clinical Trial of the Long-Term Effects of Omeprazole on Healthy Dogs. Animals. 2024; 14(8):1168. https://doi.org/10.3390/ani14081168
Chicago/Turabian StyleGil-Vicente, Laura, Germán Martín, Carme Soler, Anna Vila, María Rocío Saiz, and Paula F. Navarro. 2024. "Prospective Randomized Controlled Clinical Trial of the Long-Term Effects of Omeprazole on Healthy Dogs" Animals 14, no. 8: 1168. https://doi.org/10.3390/ani14081168
APA StyleGil-Vicente, L., Martín, G., Soler, C., Vila, A., Saiz, M. R., & Navarro, P. F. (2024). Prospective Randomized Controlled Clinical Trial of the Long-Term Effects of Omeprazole on Healthy Dogs. Animals, 14(8), 1168. https://doi.org/10.3390/ani14081168