
Evaluation of Gastric pH and Gastrin Concentrations in Horses Subjected to General Inhalation Anesthesia in Dorsal Recumbency
 , , , , , , , and
, , , , , , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Animals
2.2. Ethical Statement
2.3. Experimental Groups
2.4. Anesthetic Protocol
2.5. Gastric Fluid Sample Collection and Analysis
2.6. Serum Gastrin Measurement
2.7. Statistical Analysis
3. Results
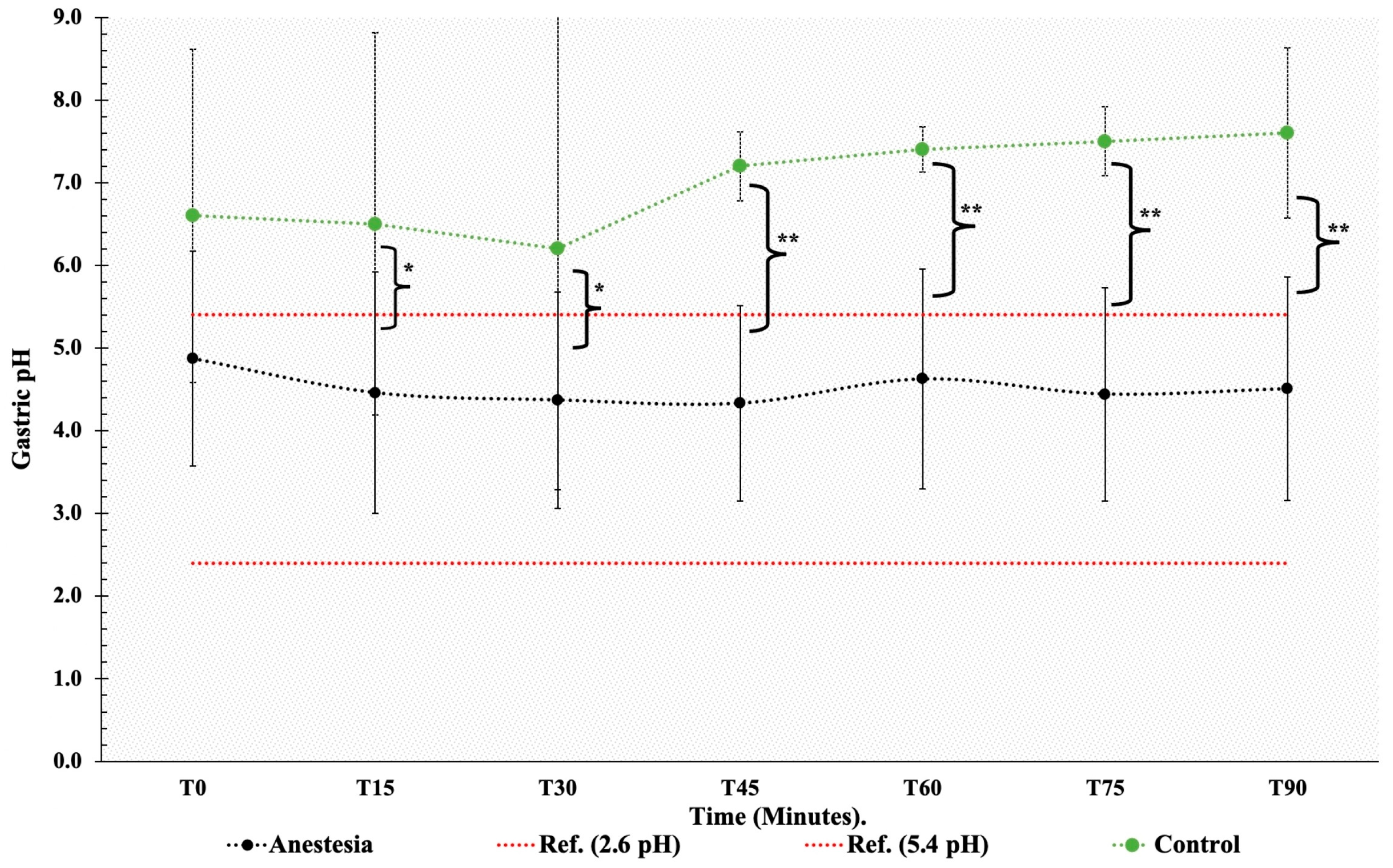
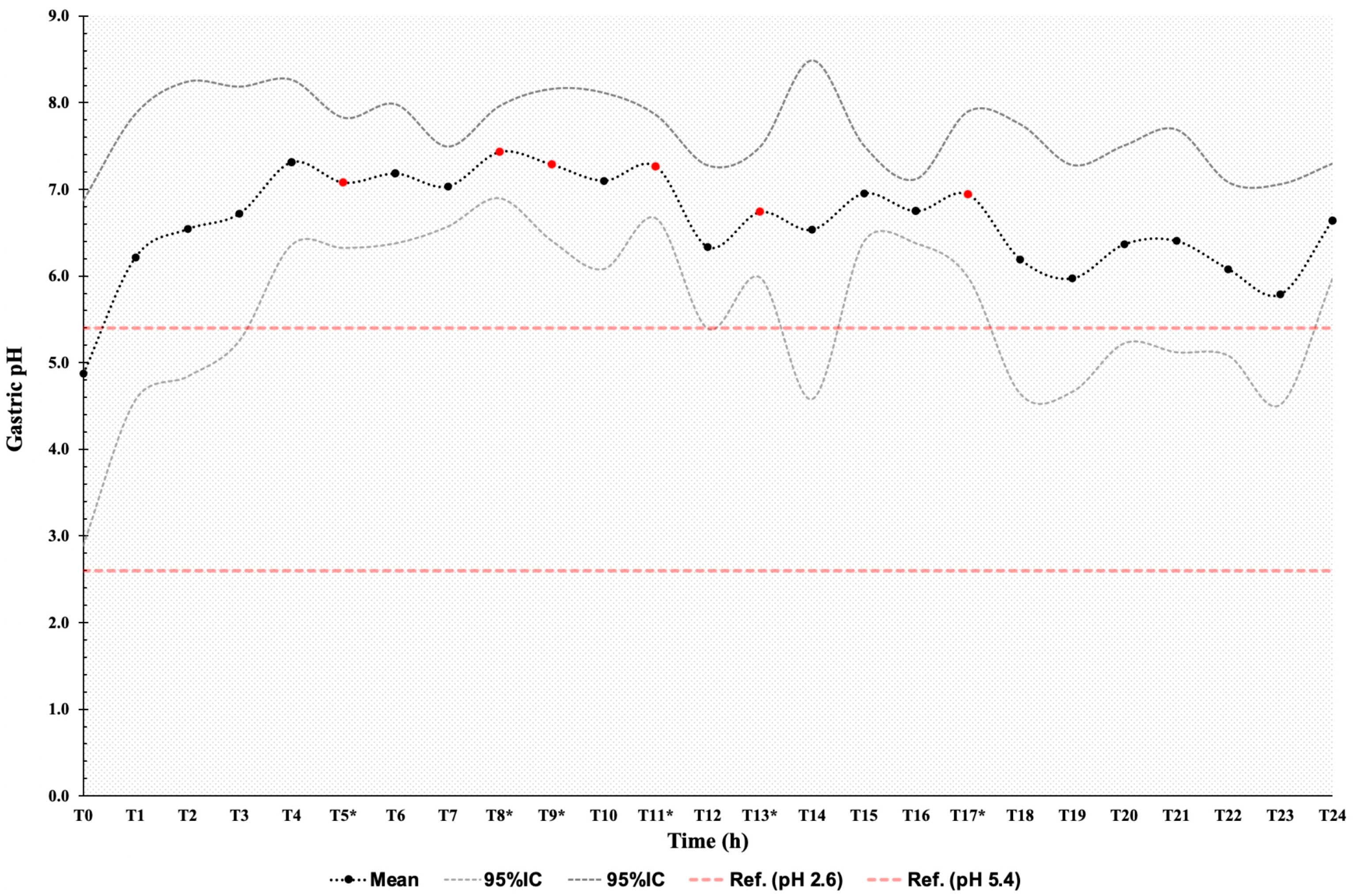
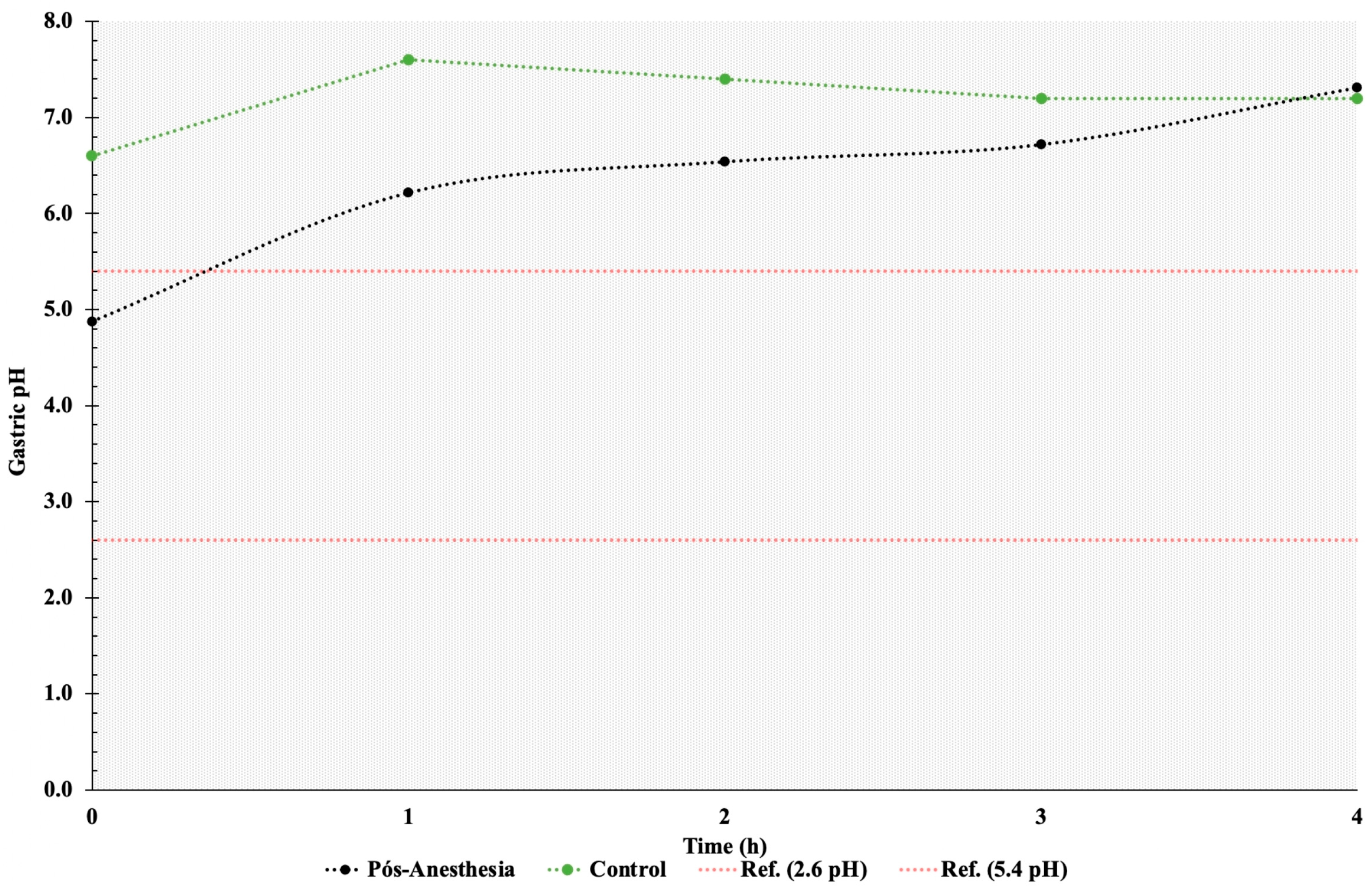
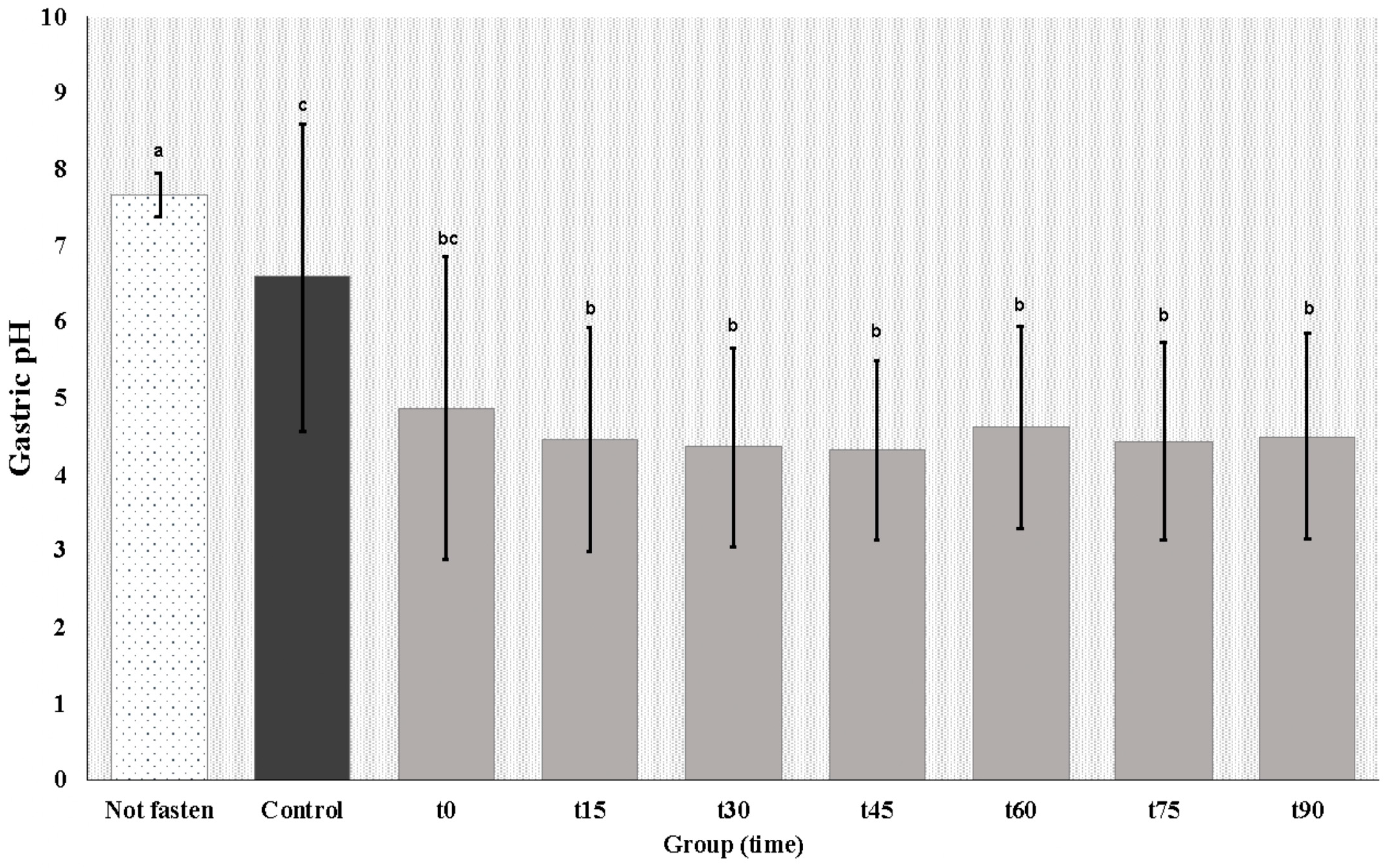
3.1. Gastric pH
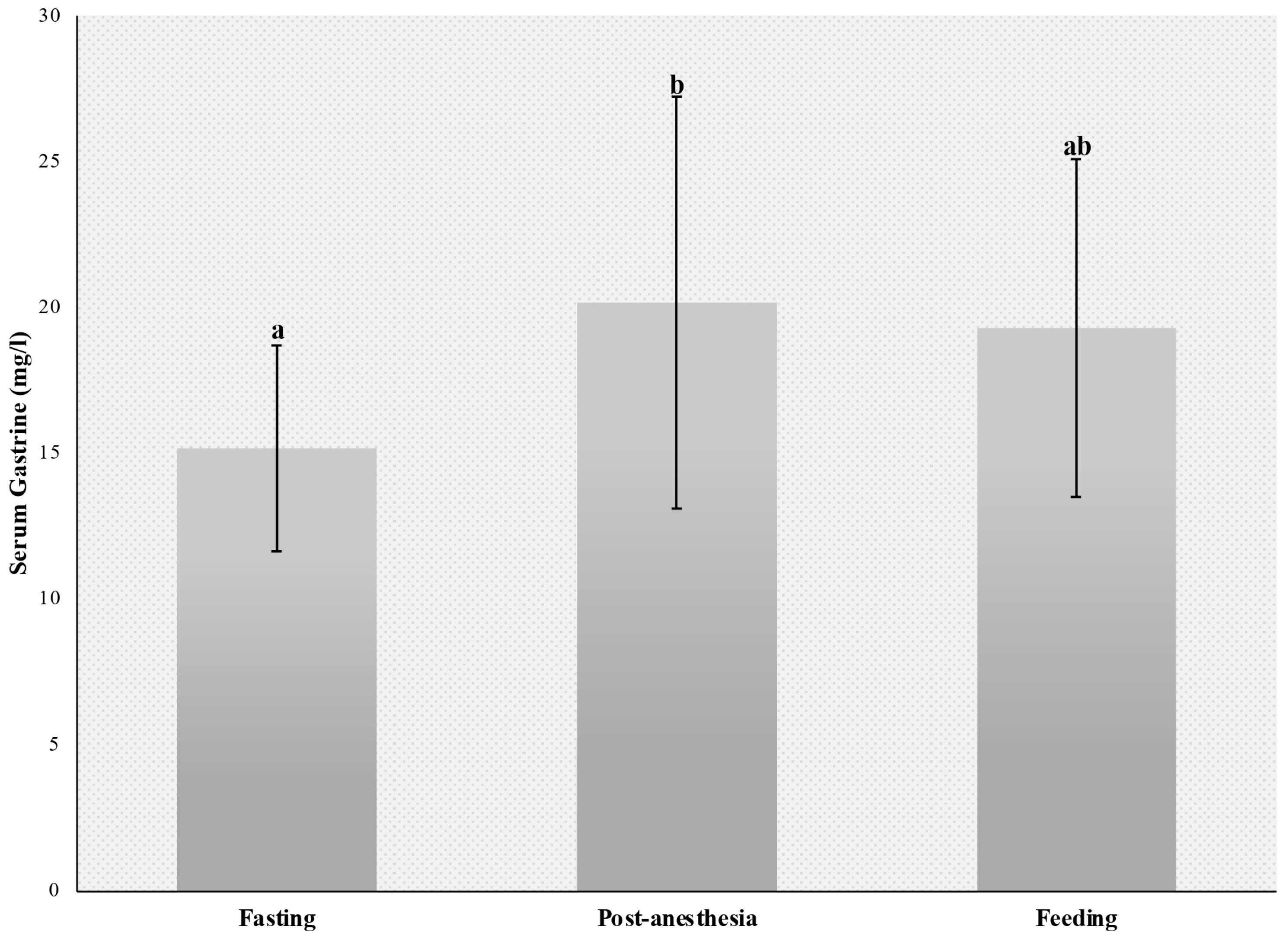
3.2. Serum Gastrin Measurement
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Camacho-Luna, P.; Buchanan, B.; Andrews, F.M. Advances in Diagnostics and Treatments in Horses and Foals with Gastric and Duodenal Ulcers. Vet. Clin. Equine Pract. 2018, 34, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, B.R.; Andrews, F.M. Treatment and prevention of equine gastric ulcer syndrome. Vet. Clin. Equine Pract. 2003, 19, 575–597. [Google Scholar] [CrossRef] [PubMed]
- Nieto, J.E.; Snyder, J.R.; Beldomenico, P.; Aleman, M.; Kerr, J.W.; Spier, S.J. Prevalence of gastric ulcers in endurance horses—A preliminary report. Vet. J. 2004, 167, 33–37. [Google Scholar] [CrossRef]
- van den Boom, R. Equine gastric ulcer syndrome in adult horses. Vet. J. 2022, 283–284, 105830. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.J.; Johnson, P.J.; David, A.; Cook, C.R. Idiopathic gastroesophageal reflux disease in an adult horse. J. Am. Vet. Med. Assoc. 2004, 224, 1967–1970+1931. [Google Scholar] [CrossRef] [PubMed]
- Hani, A.C.; Galindo, A.; Leguizamo, A.; Maldonado, C.; Páramo, D.; Costa, V.; Sierra, F.; Torres Amaya, M.; Pardo, R.; Otero, W.; et al. Guía de práctica clínica para la enfermedad por reflujo gastroesofágico. Rev. Colomb. Gastroenterol. 2015, 30, 1–8. [Google Scholar]
- Rubenstein, J.H.; Chen, J.W. Epidemiology of Gastroesophageal Reflux Disease. Gastroenterol. Clin. 2014, 43, 1–14. [Google Scholar] [CrossRef]
- Rojas Díaz, R.O.; Pérez Sosa, J.A.; Contreras Ruiz Velasco, R. Reflujo duodenogástrico. Definición y diagnóstico. Cir. Gen. 2015, 37, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Suárez Parga, J.M.; Erdozaín Sosa, J.C.; Comas Redondo, C.V.P.R. Enfermedad por Reflujo Gastroesofágico: Tratamiento. Prensa Med. Argent. 1999, 23, 97–103. [Google Scholar] [CrossRef]
- Boscan, P.; Cochran, S.; Monnet, E.; Webb, C.; Twedt, D. Effect of prolonged general anesthesia with sevoflurane and laparoscopic surgery on gastric and small bowel propulsive motility and pH in dogs. Vet. Anaesth. Analg. 2014, 41, 73–81. [Google Scholar] [CrossRef]
- Brosnahan, M.M.; Holbrook, T.C.; Gilliam, L.L.; Ritchey, J.W.; Confer, A.W. Intra-abdominal hypertension in two adult horses. J. Vet. Emerg. Crit. Care 2009, 19, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Andrews, F.M.; Jenkins, C.C.; Frazier, D.; Blackford, J.T. Gastric secretion in foals: Measurement by nasogastric intubation with constant infusion and aspiration. Equine Vet. J. 1992, 24, 75–79. [Google Scholar] [CrossRef]
- Baker, S.; Gerring, E.; Fox, M. Twenty-four hour gastric pH monitoring and blood gastrin concentrations in fasted ponies. Res. Vet. Sci. 1993, 55, 261–264. [Google Scholar] [CrossRef]
- Garcia, R.; Belafsky, P.; Della Maggiore, A.; Osborn, J.; Pypendop, B.; Pierce, T.; Walker, V.; Fulton, A.; Marks, S. Prevalence of Gastroesophageal Reflux in Cats During Anesthesia and Effect of Omeprazole on Gastric pH. J. Vet. Intern. Med. 2017, 31, 734–742. [Google Scholar] [CrossRef]
- Young, D.W.; Smyth, G.B. Validation of a radioimmunoassay for measurement of gastrin in equine serum. Am. J. Vet. Res. 1988, 49, 1179–1183. [Google Scholar] [PubMed]
- Aranzales, J.R.M.; Alves, G.E.S. O estômago equino: Agressão e mecanismos de defesa da mucosa. Cienc. Rural. 2013, 43, 305–313. [Google Scholar] [CrossRef][Green Version]
- Hunt, R.H. Importance of pH Control in the Management of GERD. Arch. Intern. Med. 1999, 159, 649–657. [Google Scholar] [CrossRef]
- Murray, M.J.; Schusser, G.F. Measurement of 24-h gastric pH using an indwelling pH electrode in horses unfed, fed and treated with ranitidine. Equine Vet. J. 1993, 25, 417–421. [Google Scholar] [CrossRef] [PubMed]
- Padalino, B.; Davis, G.L.; Raidal, S.L. Effects of transportation on gastric pH and gastric ulceration in mares. J. Vet. Intern. Med. 2020, 34, 922–932. [Google Scholar] [CrossRef]
- Damkel, C.; Snyder, A.; Uhlig, A.; Coenen, M.; Schusser, G.F. Impact of diet on 24-hour intragastric pH profile in healthy horses. Berl. Munch. Tierarztl. Wochenschr. 2015, 128, 345–349. [Google Scholar]
- Lorenzo-Figueras, M.; Merritt, A.M. Effects of exercise on gastric volume and pH in the proximal portion of the stomach of horses. Am. J. Vet. Res. 2002, 63, 1481–1487. [Google Scholar] [CrossRef]
- Schauvliege, S.; Binetti, A.; Duchateau, L.; van Dijk, J.J.; Gasthuys, F. Cardiorespiratory effects of a 7° reverse Trendelenburg position in anaesthetized horses: A randomized clinical trial. Vet. Anaesth. Analg. 2018, 45, 648–657. [Google Scholar] [CrossRef]
- Salciccia, A.; Gougnard, A.; Grulke, S.; de Pouyade, G.D.; Libertiaux, V.; Busoni, V.; Sandersen, C.; Serteyn, D. Gastrointestinal effects of general anaesthesia in horses undergoing non abdominal surgery: Focus on the clinical parameters and ultrasonographic images. Res. Vet. Sci. 2019, 124, 123–128. [Google Scholar] [CrossRef] [PubMed]
- de Paula, V.B.; Canola, P.A.; Rivera, G.G.; Bonacin, Y.S.; Del Rio, L.A.; Canola, J.C.; Ferraudo, A.S. Intra-abdominal Pressure Screening of Horses With Colic. J. Equine Vet. Sci. 2020, 90, 102998. [Google Scholar] [CrossRef] [PubMed]
- Lambertini, C.; Pietra, M.; Galiazzo, G.; Torresan, F.; Pinna, S.; Pisoni, L.; Romagnoli, N. Incidence of Gastroesophageal Reflux in Dogs Undergoing Orthopaedic Surgery or Endoscopic Evaluation of the Upper Gastrointestinal Tract. Vet. Sci. 2020, 7, 144. [Google Scholar] [CrossRef]
- Muir, W.W. Chapter 10-Anxiolytics, Nonopioid Sedative-Analgesics, and Opioid Analgesics. In Equine Anesth, 2nd ed.; Muir, W.W., Hubbell, J.A.E., Eds.; W.B. Saunders: Saint Louis, MO, USA, 2009; pp. 185–209. [Google Scholar] [CrossRef]
- McCabe, M.E.; Dilly, C.K. New Causes for the Old Problem of Bile Reflux Gastritis. Clin. Gastroenterol. Hepatol. 2018, 16, 1389–1392. [Google Scholar] [CrossRef]
- Sandin, A.; Andrews, F.M.; Nadeau, J.; Nilsson, G. Effect of nervous excitation on acid secretion in horses. Acta Physiol. Scand. 2000, 168, 437–442. [Google Scholar] [CrossRef]
- Sutton, D.G.M.; Preston, T.; Christley, R.M.; Cohen, N.D.; Love, S.; Roussel, A.J. The effects of xylazine, detomidine, acepromazine and butorphanol on equine solid phase gastric emptying rate. Equine Vet. J. 2002, 34, 486–492. [Google Scholar] [CrossRef]
- Kitchen, D.L.; Burrow, J.A.; Heartless, C.S.; Merritt, A.M. Effect of pyloric blockade and infusion of histamine or pentagastrin on gastric secretion in horses. Am. J. Vet. Res. 2000, 61, 1133–1139. [Google Scholar] [CrossRef] [PubMed]
- Cruz, A.M.; Li, R.; Kenney, D.G.; Monteith, G. Effects of indwelling nasogastric intubation on gastric emptying of a liquid marker in horses. Am. J. Vet. Res. 2006, 67, 1100–1104. [Google Scholar] [CrossRef]
- Londong, W.; Angerer, M.; Bosch, R.; Koelzow, H. Standardization of Electrode Positioning and Composition of Meals for Long-Term Intragastric pH Metry in Man. Dig. Dis. 1990, 8 (Suppl. S1), 46–53. [Google Scholar] [CrossRef]
- Albanese, V.; Munsterman, A.; Klohnen, A. Prevalence of Gastric Ulceration in Horses with Enterolithiasis Compared with Horses with Simple Large Intestinal Obstruction. Vet. Sci. 2022, 9, 587. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.J.; Grodinsky, C.; Anderson, C.W.; Radue, P.F.; Schmidt, G.R. Gastric ulcers in horses: A comparison of endoscopic findings in horses with and without clinical signs. Equine Vet. J. 1989, 21, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo-Figueras, M.; Morisset, S.M.; Morisset, J.; Lainé, J.; Merritt, A.M. Digestive enzyme concentrations and activities in healthy pancreatic tissue of horses. Am. J. Vet. Res. 2007, 68, 1070–1072. [Google Scholar] [CrossRef]
- Wickens, C.L.; McCall, C.A.; Bursian, S.; Hanson, R.; Heleski, C.R.; Liesman, J.S.; McElhenney, W.H.; Trottier, N.L. Assessment of Gastric Ulceration and Gastrin Response in Horses with History of Crib-Biting. J. Equine Vet. Sci. 2013, 33, 739–745. [Google Scholar] [CrossRef]
- Campbell-Thompson, M.L.; Merritt, A.M. Basal and pentagastrin-stimulated gastric secretion in young horses. Am. J. Physiol. Regul. Integr. Comp. Physiol. 1990, 259, R1259–R1266. [Google Scholar] [CrossRef] [PubMed]
- Norlén, P.; Kitano, M.; Lindström, E.; Håkanson, R. Anaesthetic agents inhibit gastrin-stimulated but not basal histamine release from rat stomach ECL cells. Br. J. Pharmacol. 2000, 130, 725–730. [Google Scholar] [CrossRef]
- Norlén, P.; Ericsson, P.; Kitano, M.; Ekelund, M.; Håkanson, R. The vagus regulates histamine mobilization from rat stomach ECL cells by controlling their sensitivity to gastrin. J. Physiol. 2005, 564, 895–905. [Google Scholar] [CrossRef] [PubMed]
- Schusser, G.F.; Obermayer-Pietsch, B. Plasma gastrin levels in horses with colic. Tierarztl. Prax. 1992, 20, 395–398. [Google Scholar] [PubMed]
- Fykse, V.; Solligard, E.; Bendheim, M.O.; Chen, D.; Gronbech, J.E.; Sandvik, A.K.; Waldum, H.L. ECL cell histamine mobilization and parietal cell stimulation in the rat stomach studied by microdialysis and electron microscopy. Acta Physiol. 2006, 186, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Johnsen, A.H.; Sandin, A.; Rourke, I.J.; Bundgaard, J.R.; Nilsson, G.; Rehfeld, J.F. Unique progastrin processing in equine G-cells suggests marginal tyrosyl sulfotransferase activity. Eur. J. Biochem. 1998, 255, 432–438. [Google Scholar] [CrossRef]
- Marambio, A.; Watkins, G.; Jans, J. Gastrina: Hormona de múltiples funciones. Rev. Hosp. Clín. Univ. Chile 2012, 23, 139–186. [Google Scholar]
- Wilson, A.D.; Badnell-Waters, A.J.; Bice, R.; Kelland, A.; Harris, P.A.; Nicol, C.J. The effects of diet on blood glucose, insulin, gastrin and the serum tryptophan: Large neutral amino acid ratio in foals. Vet. J. 2007, 174, 139–146. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group and Time | pH | p-Value (vs. Not Fasten) | p-Value (vs. Control) |
|---|---|---|---|
| Non-fasted T0 | 7.67 ± 0.13 a | Ref. | 0.0119 |
| Control T0 * | 6.6 ± 0.63 c | 0.0119 | Ref. |
| Anaesthetized T0 * | 4.88 ± 0.84 bc | 0.0006 | 0.1056 |
| T15 | 4.46 ± 0.62 b | <0.0001 | 0.028 |
| T30 | 4.37 ± 0.55 b | <0.0001 | 0.0168 |
| T45 | 4.33 ± 0.50 b | <0.0001 | 0.0111 |
| T60 | 4.63 ± 0.56 b | <0.0001 | 0.0286 |
| T75 | 4.44 ± 0.55 b | <0.0001 | 0.0186 |
| T90 | 4.51 ± 0.57 b | <0.0001 | 0.0244 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guerrero, J.L.S.; Brito, P.H.S.; Ferreira, M.A.; Arantes, J.d.A.; Rusch, E.; Oliveira, B.V.d.S.; Velasco-Bolaños, J.; Carregaro, A.B.; Dória, R.G.S. Evaluation of Gastric pH and Gastrin Concentrations in Horses Subjected to General Inhalation Anesthesia in Dorsal Recumbency. Animals 2024, 14, 1183. https://doi.org/10.3390/ani14081183
Guerrero JLS, Brito PHS, Ferreira MA, Arantes JdA, Rusch E, Oliveira BVdS, Velasco-Bolaños J, Carregaro AB, Dória RGS. Evaluation of Gastric pH and Gastrin Concentrations in Horses Subjected to General Inhalation Anesthesia in Dorsal Recumbency. Animals. 2024; 14(8):1183. https://doi.org/10.3390/ani14081183
Chicago/Turabian StyleGuerrero, Jesus Leonardo Suarez, Pedro Henrique Salles Brito, Marília Alves Ferreira, Julia de Assis Arantes, Elidiane Rusch, Brenda Valéria dos Santos Oliveira, Juan Velasco-Bolaños, Adriano Bonfim Carregaro, and Renata Gebara Sampaio Dória. 2024. "Evaluation of Gastric pH and Gastrin Concentrations in Horses Subjected to General Inhalation Anesthesia in Dorsal Recumbency" Animals 14, no. 8: 1183. https://doi.org/10.3390/ani14081183
APA StyleGuerrero, J. L. S., Brito, P. H. S., Ferreira, M. A., Arantes, J. d. A., Rusch, E., Oliveira, B. V. d. S., Velasco-Bolaños, J., Carregaro, A. B., & Dória, R. G. S. (2024). Evaluation of Gastric pH and Gastrin Concentrations in Horses Subjected to General Inhalation Anesthesia in Dorsal Recumbency. Animals, 14(8), 1183. https://doi.org/10.3390/ani14081183