Lung Ultrasound Imaging, a Technical Review


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Ultrasound Spectroscopy
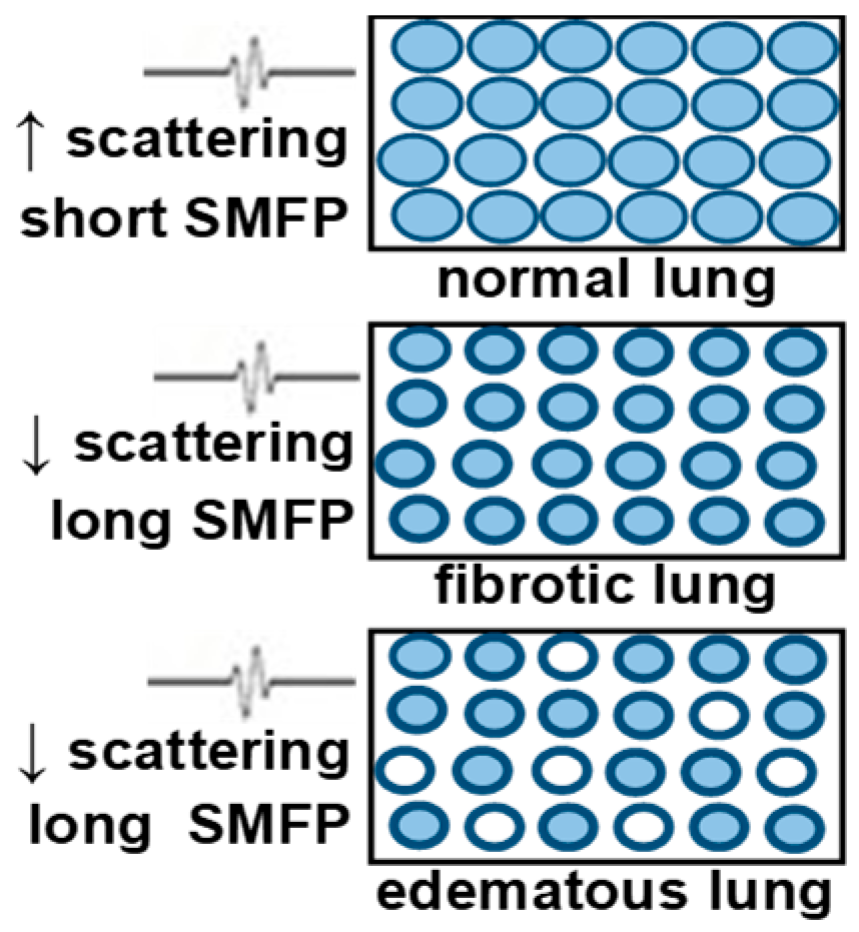
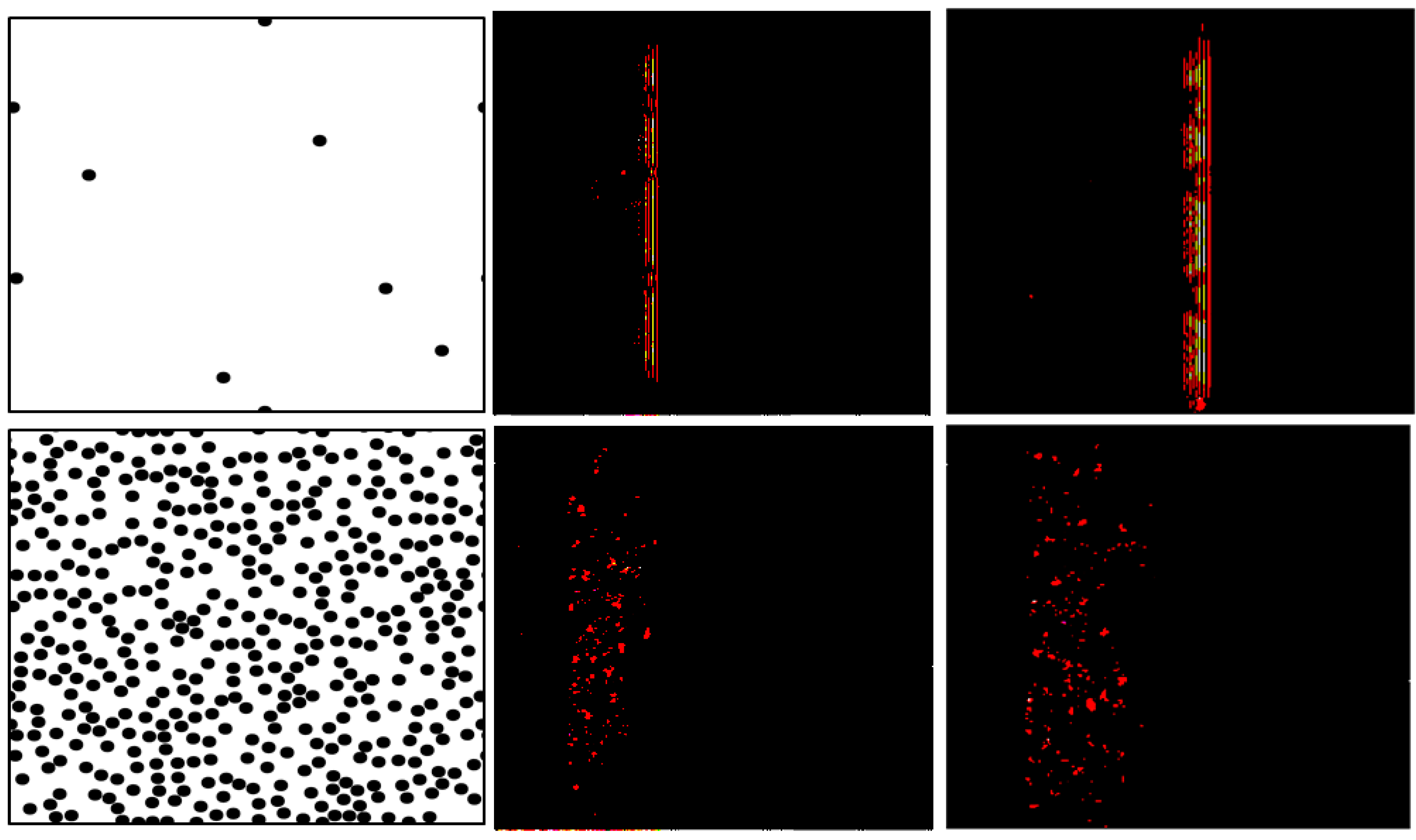
3. Ultrasound Multiple-Scattering Characterization
3.1. Measurement of the Diffusion Constant Using a Conventional Ultrasound Probe
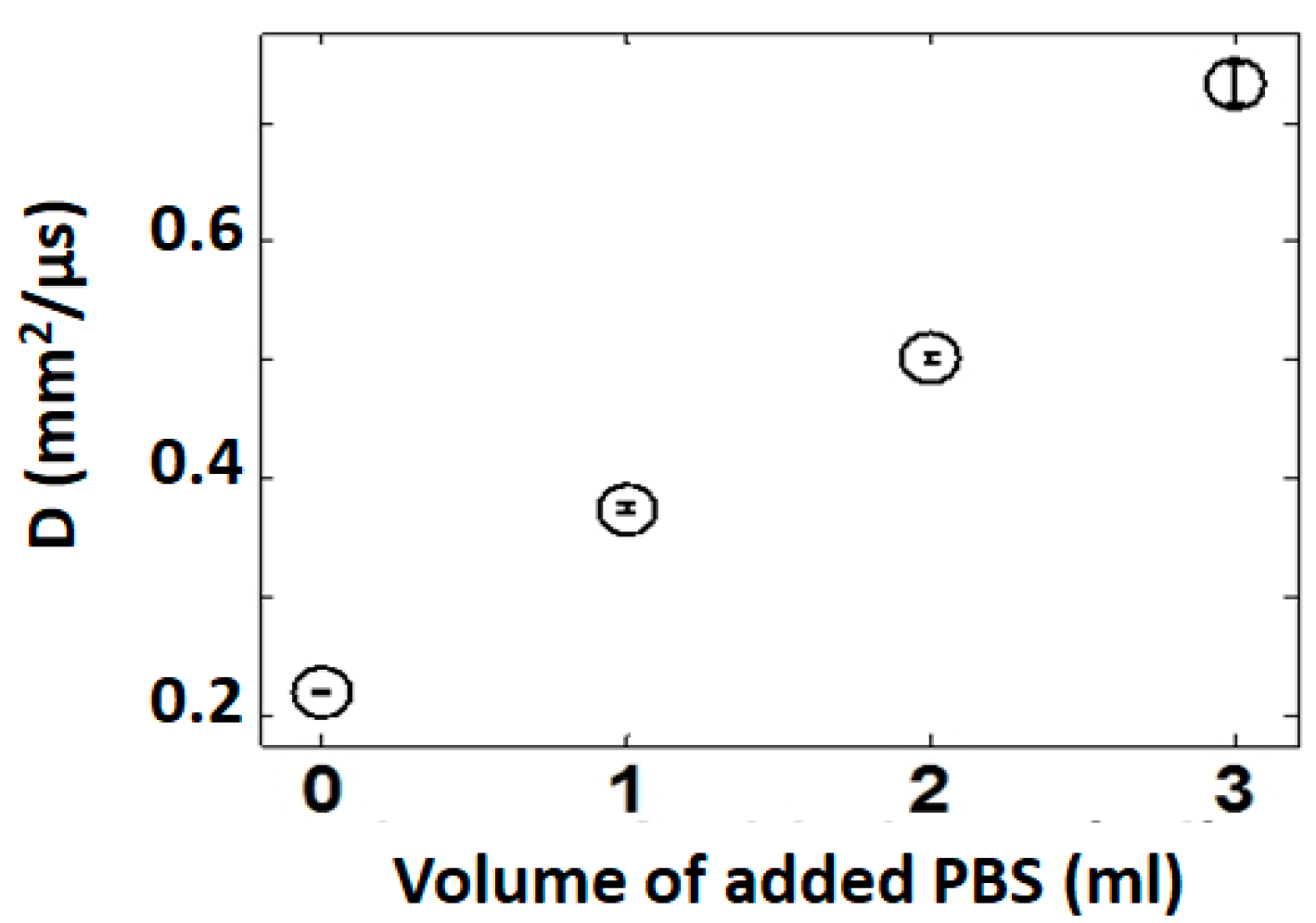
3.2. Model of Pulmonary Edema Ex Vivo
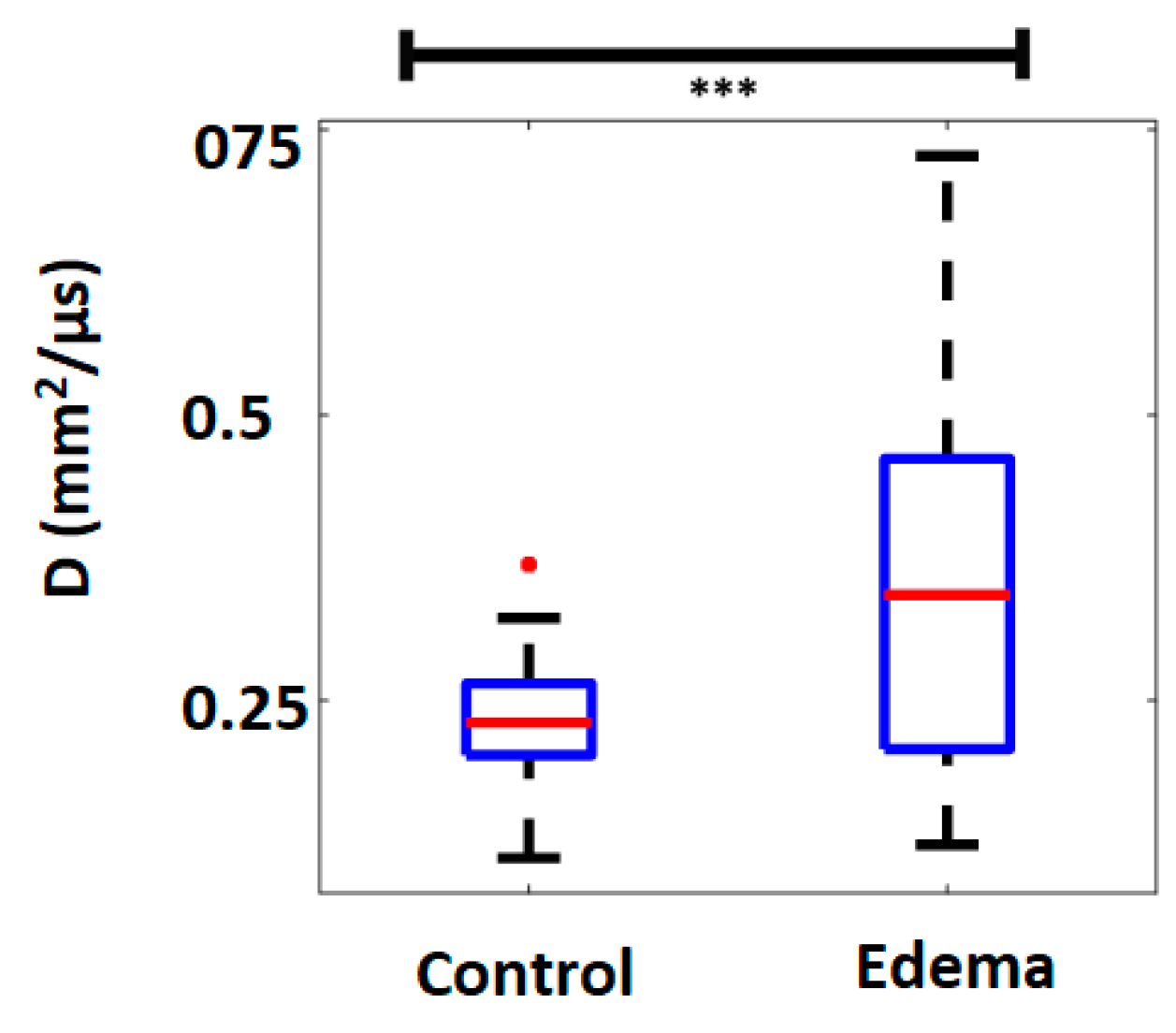
3.3. Model of Pulmonary Edema In-Vivo
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Pneumonia, Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/pneumonia (accessed on 4 January 2020).
- World Health Organization (WHO). World Health Statistics 2016. Available online: https://www.who.int/en/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 4 January 2020).
- American Thoracic Society: Pulmonary Fibrosis 2019. Available online: https://www.thoracic.org/patients/lung-disease-week/2015/pulmonary-fibrosis-week/general-info.php (accessed on 4 January 2020).
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef]
- Miglioretti, D.L.; Smith-Bindman, R. Overuse of Computed Tomography and Associated Risks. Am. Fam. Physician 2011, 83, 1252–1254. [Google Scholar]
- Smith-Bindman, R. Is it Computed Tomography Safe? N. Engl. J. Med. 2010, 363, 1–4. [Google Scholar] [CrossRef]
- Davies, H.E.; Wathen, C.G.; Gleeson, F.V. Risks of exposure to radiological imaging and how to minimize them. Br. Med. J. 2011, 342, d947. [Google Scholar] [CrossRef]
- Brenner, D.J.; Hall, E.J. Computed Tomography—An Increasing Source of Radiation Exposure. N. Engl. J. Med. 2007, 29, 2277–2284. [Google Scholar] [CrossRef] [Green Version]
- Fayngersh, V.; Passero, M. Estimating Radiation Risk from Computed Tomography Scanning. Lung 2009, 187, 143–148. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Ionizing Radiation, Health Effects and Protective Measures, Fact Sheet N°371. Available online: http://www.who.int/mediacentre/factsheets/fs371/en/ (accessed on 4 January 2020).
- Abraham, W.T.; Adamson, P.B.; Bourge, R.C.; Aaron, M.F.; Costanzo, M.R.; Stevenson, L.W.; Strickland, W.; Neelagaru, S.; Raval, N.; Krueger, S.; et al. Wireless pulmonary artery haemodynamic monitoring in chronic heart failure: A randomised controlled trial. Lancet 2011, 377, 658–666. [Google Scholar] [CrossRef]
- Avruch, L.; Cooperberg, P.L. The Ring-Down Artifact. J. Ultrasound Med. 1985, 4, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, D.A.; Menu, Y. A bedside ultrasound sign ruling out pneumothorax in the critically III: Lung sliding. Chest 1995, 108, 1345–1348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lichtenstein, D.A.; Mézière, G.; Biderman, P.; Gepner, A.; Barré, O. The Comet-tail Artifact: An Ultrasound Sign of Alveolar-Interstitial Syndrome. Am. J. Respir. Crit. Care Med. 1997, 156, 1640–1646. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, D.A.; Mézière, G. A lung ultrasound sign allowing bedside distinction between pulmonary edema and COPD: The comet-tail artifact. Intensive Care Med. 1998, 24, 1331–1334. [Google Scholar] [CrossRef] [PubMed]
- Soldati, G.; Giunta, V.; SHER, S.; Melosi, F.; Dini, C. Synthetic Comets: A new Look at Lung Sonography. Ultrasound Med. Biol. 2011, 37, 1762–1770. [Google Scholar] [CrossRef] [PubMed]
- Jambrik, Z.; Monti, S.; Coppola, V.; Agricola, E.; Mottola, G.; Miniati, M.; Picano, E. Usefulness of ultrasound lung comets as non-radiologic sign of extravascular lung water. Am. J. Cardiol. 2004, 93, 1265–1270. [Google Scholar] [CrossRef] [PubMed]
- Gargani, L.; Frassi, F.; Soldati, G.; Tesorio, P.; Gheorghiade, M.; Picano, E. Ultrasound lung comets for differential diagnosis of acute cardiogenic dyspnea: A comparison with natriuretic peptides. Eur. J. Heart Fail. 2008, 10, 70–77. [Google Scholar] [CrossRef]
- Reißig, A.; Kroegel, C. Transthoracic sonography of diffuse parenchymal lung disease. J. Ultrasound Med. 2003, 22, 173–180. [Google Scholar] [CrossRef]
- Volpicelli, G.; Mussa, A.; Garofalo, G.; Cardinale, L.; Casoli, G.; Perotto, F.; Fava, C.; Frascisco, M. Bedside lung ultrasound in the assessment of alveolar interstitial syndrome. Am. J. Emerg. Med. 2006, 24, 689–696. [Google Scholar] [CrossRef]
- Copetti, R.; Soldati, G.; Copetti, P. Chest sonography: A useful tool to differentiate acute cardiogenic pulmonary edema from acute respiratory distress syndrome. Cardiovasc. Ultrasound 2008, 6, 16. [Google Scholar] [CrossRef] [Green Version]
- Volpicelli, G.; Frascisco, M.F. Sonographic detection of radio-occult interstitial lung involvement in measles pneumonitis. Am. J. Emerg. Med. 2009, 27, 128.e1–128.e3. [Google Scholar] [CrossRef]
- Soldati, G.; Copetti, R.; Sher, S. Sonographic interstitial syndrome: The sound of lung water. J. Ultrasound Med. 2009, 28, 163–174. [Google Scholar] [CrossRef]
- Bouhemad, B.; Zhang, M.; Lu, Q.; Rouby, J.J. Clinical review: Bedside lung ultrasound in critical care practice. Crit. Care 2007, 11, 205. [Google Scholar] [CrossRef]
- Sartori, S.; Tombesi, P. Emerging roles for transthoracic ultrasonography in pleuropulmonary pathology. World J. Radiol. 2010, 2, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Feller-Kopman, D. Ultrasound-guided thoracentesis. Chest 2006, 129, 1709–1714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hyacinthe, A.C.; Broux, C.; Francony, G.; Genty, C.; Bouzat, P.; Jacquot, C.; Albaladejo, P.; Ferretti, G.R.; Bosson, J.L.; Payen, J.F. Diagnostic accuracy of ultrasonography in the acute assessment of common thoracic lesions after trauma. Chest 2012, 141, 1177–1183. [Google Scholar] [CrossRef] [PubMed]
- Coley, B.D. Chest sonography in children: Current indications, techniques, and imaging findings. Radiol. Clin. N. Am. 2011, 49, 825–846. [Google Scholar] [CrossRef] [PubMed]
- Kreuter, M.; Mathis, G. Emergency Ultrasound of the Chest. Respiration 2014, 87, 89–97. [Google Scholar] [CrossRef] [Green Version]
- Lichtenstein, D.A.; Goldstein, I.; Mourgeon, E.; Cluzel, P.; Grenier, P.; Rouby, J.J. Comparative diagnostic performances of auscultation, chest radiography, and lung ultrasonography in acute respiratory distress syndrome. Anesthesiology 2004, 100, 9–15. [Google Scholar] [CrossRef]
- Volpicelli, G.; Elbarbary, M.; Blaivas, M.; Lichtenstein, D.A.; Mathis, G.; Kirkpatrick, A.W.; Melniker, L.; Gargani, L.; Noble, V.E.; Via, G.; et al. International Liaison Committee on Lung Ultrasound (ILC-LUS) for the International Consensus Conference on Lung Ultrasound (ICC-LUS). International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012, 38, 577–591. [Google Scholar] [CrossRef] [Green Version]
- Lichtenstein, D.A. Lung ultrasound in the critically ill. Ann. Intensive Care 2014, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Anderson, K.; Fields, J.M.; Panebianco, N.; Jeng, K.; Marin, J.; Dean, A.J. Inter-Rater Reliability of Quantifying Pleural B-Lines Using Multiple Counting Methods. J. Ultrasound Med. 2013, 32, 115–120. [Google Scholar] [CrossRef]
- Sperandeo, M.; Trovato, G.M.; Catalano, D. Quantifying B-lines on lung sonography: Insufficient evidence as an objective, constructive, and educational tool. J. Ultrasound Med. 2014, 33, 362–365. [Google Scholar] [CrossRef]
- Zanforlin, A.; Smargiassi, A.; Inchingolo, R.; Sher, S.; Ramazzina, E.; Corbo, G.M.; Soldati, G. B-Lines: To Count or Not to Count. J. Am. Coll. Cardiol. Cadiovasc. Imaging 2014, 7, 635–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soldati, G.; Demi, M.; Inchingolo, R.; Smargiassi, A.; Demi, L. On the physical basis of pulmonary sonographic interstitial syndrome. J. Ultrasound Med. 2016, 35, 2075–2086. [Google Scholar] [CrossRef] [PubMed]
- Soldati, G.; Demi, M.; Smargiassi, A.; Inchingolo, R.; Demi, L. The role of ultrasound lung artefacts in thediagnosis of respiratory diseases. Expert Rev. Respir. Med. 2019, 13, 162–172. [Google Scholar] [CrossRef] [PubMed]
- Dunn, F.; Fry, W.J. Ultrasonic absorption and reflection by lung tissue. Phys. Med. Biol. 1961, 5, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Bauld, T.J.; Schwan, H.P. Attenuation and reflection of ultrasound in canine lung tissue. J. Acoust. Soc. Am. 1974, 56, 1630–1637. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, P.C.; Ozcan, H.S. Ultrasound properties of lung tissue and their Measurements. Ultrasound Med. Biol. 1986, 12, 483–499. [Google Scholar] [CrossRef]
- Dunn, F. Attenuation and speed of ultrasound in lung: Dependence upon frequency and inflation. J. Acoust. Soc. Am. 1986, 80, 1248–1250. [Google Scholar] [CrossRef]
- Dunn, F. Attenuation and speed of ultrasound in lung. J. Acoust. Soc. Am. 1974, 56, 1638–1639. [Google Scholar] [CrossRef]
- Mikhak, Z.; Pedersen, P.C. Acoustic attenuation properties of the lung: An open question. Ultrasound Med. Biol. 2002, 28, 1209–1216. [Google Scholar] [CrossRef]
- Demi, L.; van Hoeve, W.; van Sloun, R.J.G.; Soldati, G.; Demi, M. Determination of a potential quantitative measure of the state of the lung using lung ultrasound spectroscopy. Nat. Sci. Rep. 2017, 7, 12746. [Google Scholar] [CrossRef]
- Sagm, K.B.; Rhyne, T.L.; Myers, G.S.; Lees, R.S. Characterization of Normal and Abnormal Pulmonary Surface by Reflected Ultrasound. Chest 1978, 74, 29–33. [Google Scholar]
- Demi, M.; Prediletto, R.; Soldati, G.; Demi, L. Physical mechanisms providing clinical information from ultrasound lung images: Hypotheses and early confirmations. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2019. [Google Scholar] [CrossRef] [PubMed]
- van Sloun, R.J.G.; Demi, L. Localizing B-lines in Lung Ultrasonography by Weakly-Supervised Deep Learning, in-vivo results. IEEE J. Biomed. Health Inform. 2019. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, K.; Blackwell, J.; Egan, T.; Muller, M. Characterization of the Lung Parenchyma Using Ultrasound Multiple Scattering. Ultrasound Med. Biol. 2017, 43, 993–1003. [Google Scholar] [CrossRef] [PubMed]
- Doanes, M.; Yuan, Y.; Jin, J.; Egan, T. Gene expression analysis of rat lung ischemia-reperfusion injury (Abstract). Am. J. Resp. Crit. Care Med. 2004, 169, A72. [Google Scholar]
- Zanotti, G.; Casiraghi, M.; Abano, J.B.; Tatreau, J.R.; Sevala, M.; Berlin, H.; Smyth, S.; Funkhouser, W.K.; Burridge, K.; Randell, S.H.; et al. Novel critical role of toll-like receptor 4 in lung ischemia-reperfusion injury and edema. Am. J. Physiol. Lung Cell. Mol. Physiol. 2009, 297, L52–L63. [Google Scholar] [CrossRef] [Green Version]
- King, T.E., Jr.; Bradford, W.Z.; Castro-Bernardini, S.; Fagan, E.A.; Glaspole, I.; Glassberg, M.K.; Lederer, D.J.; Gorina, E.; Hopkins, P.M.; Kardatzke, D.; et al. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. N. Engl. J. Med. 2014, 370, 2083–2092. [Google Scholar] [CrossRef] [Green Version]
- Noble, P.W.; Albera, C.; Bradford, W.Z.; Costabel, U.; Glassberg, M.K.; Kardatzke, D.; Lancaster, L.; Sahn, S.A.; Szwarcberg, J.; Valeyre, D.; et al. Pirfenidone in patients with idiopathic pulmonary fibrosis (CAPACITY): Two randomised trials. Lancet 2011, 377, 1760–1769. [Google Scholar] [CrossRef]
- Zhang, X.; Osborn, T.; Zhou, B.; Meixner, D.; Kinnick, R.R.; Bartholmai, B.; Greenleaf, J.F.; Kalra, S. Lung Ultrasound Surface Wave Elastography: A Pilot Clinical Study. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2017, 64, 1298–1304. [Google Scholar] [CrossRef]
- Child, S.Z.; Hartman, C.L.; Schery, L.A.; Carstensen, E.L. Lung damage from exposure to pulsed ultrasound. Ultrasound Med. Biol. 1990, 16, 817–825. [Google Scholar] [CrossRef]
- Frizzell, L.A.; Chen, E.; Lee, C. Effects of pulsed ultrasound on the mouse neonate: Hind limb paralysis and lung hemorrhage. Ultrasound Med. Biol. 1994, 20, 53–63. [Google Scholar] [CrossRef]
- Church, C.C.; O’Brien, W.D., Jr. Evaluation of the threshold for lung hemorrhage by diagnostic ultrasound and a proposed new safety index. Ultrasound Med. Biol. 2007, 33, 810–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]








© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demi, L.; Egan, T.; Muller, M. Lung Ultrasound Imaging, a Technical Review. Appl. Sci. 2020, 10, 462. https://doi.org/10.3390/app10020462
Demi L, Egan T, Muller M. Lung Ultrasound Imaging, a Technical Review. Applied Sciences. 2020; 10(2):462. https://doi.org/10.3390/app10020462
Chicago/Turabian StyleDemi, Libertario, Thomas Egan, and Marie Muller. 2020. "Lung Ultrasound Imaging, a Technical Review" Applied Sciences 10, no. 2: 462. https://doi.org/10.3390/app10020462
APA StyleDemi, L., Egan, T., & Muller, M. (2020). Lung Ultrasound Imaging, a Technical Review. Applied Sciences, 10(2), 462. https://doi.org/10.3390/app10020462