Abstract
Since the start of the COVID-19 pandemic, the top priority was to hinder the spread of the virus and prevent the collapse of the health systems. To achieve this, it was mandatory to ensure adequate supplies of personal protective equipment (PPE), which may not have been available in the short-term during the first months of the crisis. While leading manufacturing companies all over the world were retooling their factories to produce medical equipment, 3D printing offered a transition solution to quickly supply PPEs in the case of emergency. In this context, the University of Castilla-La Mancha started a new solidarity project to produce PPEs via 3D printing, especially for healthcare staff. This project was characterized by the commitment of several geographically distributed volunteers, with limitations due to confinement. The group of volunteers required an organizational model supported by ad-hoc technology to make their collaboration efficient. This article demonstrates how a centralized production model is not efficient in such a situation, and proposes a novel web system supported by an intelligent recommender, which facilitates a distributed organizational model that optimizes manufacturing and delivery times of PPEs. The results show how our proposal drastically improves the efficiency of the group of collaborators, and adequately address the high social demand concentrated in a short period. This was a crucial change for the production and distribution of over 23,500 PPEs during the first 40 days of the crisis, in one of the regions with a higher rate of COVID-19 cases in Europe.
1. Introduction
On 8 December 2019, the first case of coronavirus disease (COVID-19) was diagnosed in China [1]. The virus quickly spread around the world [2] and on January 25th, the first European case was reported: an 80-year-old man from the province of Hubei tested positive in France. One week later, the first case appeared in Spain and new cases grew exponentially throughout the continent, especially in Italy and Spain. In a few weeks, the disease became a pandemic giving rise to one of the worst health crises in recent times, subsequently causing an economic tsunami striking the world’s major economies hard [3].
As the countries decreed confinement of the population and the confirmed cases requiring intensive care multiplied, the so-called modern society was immersed in chaos with a need for organization [4], in particular regarding the supply of personal protective equipment (PPE) to health care personnel in regions/countries where the infection rate was especially large.
From the very beginning, Spain was one of the countries badly affected by COVID-19 with 213,000 confirmed cases (data updated on 1 May 2020), 24,543 deaths and 112,000 recovered patients (National Institute of Statistics (Spain) http://ine.es). However, the distribution was not homogeneous, and some regions concentrated a rather large fraction of the overall cases, such as the case of Madrid, Catalonia, or Castilla-La Mancha.
As of 1 May, Castilla-La Mancha exhibited one of the highest death rates per 100,000 inhabitants in Spain (Source: cnecovid.isciii.es/covid19/#documentaci%C3%B3n-y-datos) (see Figure 1). The reasons behind the massive contagion have not been fully confirmed, although one may highlight: (i) the proximity to the capital city, Madrid (the epicenter of the virus in Spain), and (ii) heavy traffic, some of the most important road links in Spain cross the region.
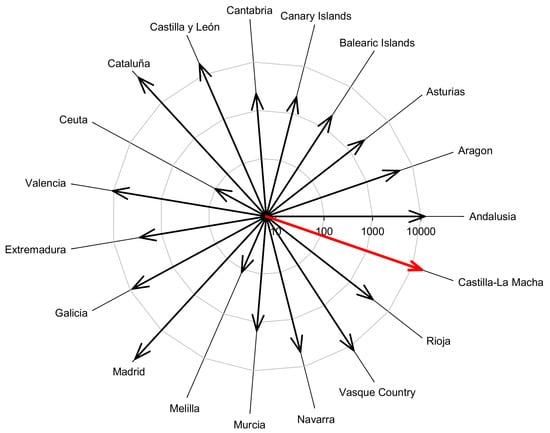
Figure 1.
Number of cumulative deaths of COVID-19. Castilla-La Mancha was the third region with more COVID-19 cases in Spain.
Castilla-La Mancha was not prepared for such an overwhelming situation and certain strategies to protect the population and prevent the virus expansion, such as the acquisition and distribution of PPEs, turned extremely difficult. This was a major issue [5], as their effective use is essential to prevent the spread of the disease between health care personnel and patients [6]. Shortage of PPEs was an unacceptable situation and implied a major risk of infection in hospitals.
The supply of PPEs in Europe largely depends on external markets, mainly China, which were soon collapsed as the cases grew in Europe and the US, leading to delivery dates of up to several weeks. As the virus rapidly expanded, such waiting periods were not acceptable and the situation in hospitals became unsustainable. Under such an emergency context, and considering that the manufacturing industry requires some time to redirect their production system to supply validated material at mass scale, several social movements and volunteered assistance promoted through digital media emerged [7,8].
These social movements are typically coordinated by groups of people aware of the critical situation searching for organization models to perform collective actions [9,10]. In times of crisis, social movements benefit from digital media to gather more people, manage activities and promote new goals, hence solutions can be offered to existing problems [11]. Unfortunately, most of these social movements perform unstructured actions and interactions among network members, with no integrated control [12,13,14]. Therefore, organization models are required to successfully perform collective actions [15,16].
One of these social movements was initiated by the University of Castilla-La Mancha (UCLM) to support the regional healthcare system in three priority areas: (a) design of low-cost ventilators for collapsed ICUs, (b) 3D printing of PPEs, and finally (c) diagnostic testing of the virus via PCR. Furthermore, the UCLM launched a crowdfunding campaign to support all the activities. On the first day, the UCLM gathered 57,000 euros in donations and, to date, the accumulated amount exceeds one million euros.
In the work presented herein, we focus on the 3D printing of PPEs to report a clear example of the impact of improved organization models upon the manufacturing and distribution of PPEs in Castilla-La Mancha (Spain). The transition from a centralized traditional system to a decentralized system (supported by a custom-developed information system) resulted in a dramatic improvement in both the manufacturing process and distribution, reducing the response times to reach the end-users. Thus, the main contribution of this work to the scientific community is a web information system that supports a distributed production model and allows the organization of volunteers located in different geographical points. The system integrates an intelligent recommender, which assigns orders of PPEs to volunteers according to their availability and manufacturing capacity. All the improvements resulted in the production of over 23,500 PPEs in 40 days, which have been distributed over 80,000 km. The time between the request by any citizen and the delivery of the material was reduced from 5.2 to 1.9 days on average. Finally, all the requests were attended to, the health sector being the main beneficiary, receiving 60% of the manufactured material (13,917 PPEs).
The rest of the paper is organized as follows: Section 2 puts into context the situation that our region faced during the first months of the crisis. Section 3 analyses in depth the main needs and problems, and describes the evolution from a centralized to a distributed production model. Section 4 then proposes a web system that supports the distributed production model, which integrates an intelligent recommender for the automatic assignment of requests to volunteers. Section 5 discusses the results obtained and compares the efficiency of the centralized and distributed production models. The paper ends in Section 6 with the conclusions.
2. Context
The region of Castilla-La Mancha (Spain) is divided into five provinces: Albacete, Toledo, Ciudad Real, Cuenca and Guadalajara, and has an area of 79,463 km with 2.035 million inhabitants. The University of Castilla-La Mancha is the regional university and is present in all the provinces, except Guadalajara. The first COVID-19 case was diagnosed in the region on 29 February 2020 and the number of cases increased significantly in the following weeks (Source: http://sanidad.castillalamancha.es/ciudadanos/enfermedades-infecciosas/coronavirus/evolucion-de-coronavirus-covid-19-en-castilla-la-mancha), as shown in Figure 2. From 10 April 2020 the growth curve flattened out, and the total number of cases stabilized at around 400–500 active cases per day.
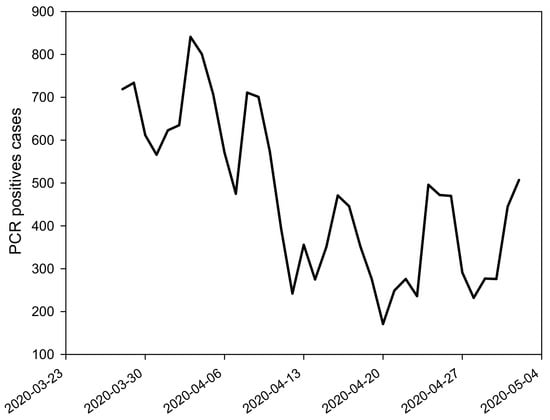
Figure 2.
Number of positives cases with a PCR test in Castilla-La Mancha between 16 March and 4 May 2020.NPC
The government did not declare the state of emergency until 14 March 2020, ordering the confinement of non-essential citizens to mitigate the virus expansion that could cause the collapse of the entire healthcare system. Statistics soon showed that the mortality rate increased notably for elderly people [17]. Indeed, 1206 elderly people (48% of the total casualties) died in Castilla-La Mancha in nursing homes, in the first 50 days since the outbreak. Despite the uncertainty of the first days, the virus transmission routes were mostly related to droplets exhaled upon breathing, talking, sneezing, or coughing. Consequently, the virus entry sites to humans are eyes, nose, and mouth. Therefore, prevention strategies must include the use of facial protective elements and, indeed, the World Health Organization (WHO) recommended the use of masks, goggles, or face shields to reduce the rate of infection [18].
Unfortunately, as mentioned above, our system was not prepared for such an outburst, and within a few days there was a shortage of PPEs, which was particularly severe in hospitals. After several initiatives to produce PPEs via 3D printing in countries such as China or Italy [19,20], some members of the UCLM used their experience and 3D printing systems to manufacture the highly demanded PPEs, such as face shields or ear-savers, in addition to other elements required by hospitals, such as valves to adapt snorkel masks to oxygenation systems, shields for ophthalmoscopes, and intubation boxes.
Additive manufacturing (AM), commonly known as 3D printing, is a set of technologies that allow the production of three-dimensional objects through the superposition of layers of various materials, typically polymers, although it has been successfully applied to metals, ceramics or composites [21]. AM provides a cost-effective and time-efficient way to produce low-volume, customized products with complicated geometries and advanced material properties and functionality [22]. Some of the advantages of 3D printing are the simplicity of use as opposed to other more sophisticated manufacturing technologies, the possibility of producing complex geometries, and low cost in the most popular systems such as Fused Deposition Modeling (FDM), which makes them affordable for domestic use. Among the disadvantages, it should be stressed out that the cost per unit is higher, the production rate much smaller, and the mechanical properties of the resulting objects are poorer compared to the traditional manufacturing technologies. In other words, the 3D printed elements cannot compete with the state-of-the-art in terms of performance or durability, but they could be considered as a short-term solution under emergency conditions [23] until the validated material arrived at the hospitals.
Regarding the production of PPEs, face shields may be partially produced by 3D printing (see Figure 3a). In particular, the headband for the face shield may be easily fabricated via FDM and then a PVC sheet is coupled. Depending on the design, some other elements may also be required, for example, elastic rubber. Face shields protect any individual from direct contact with large droplets in the short distance (coughs or sneezes), in addition to prevent physical contact with contaminated hands (see Figure 3b). This phenomenon is known as cross-contamination [24].

Figure 3.
(a) Example of a face shield manufactured with 3D printing and (b) cross-contamination.
The UCLM personnel involved in this project used 3D printers located in each of the four campus sites (Albacete, Ciudad Real, Cuenca, and Toledo). These printers had been used mostly for teaching tasks such as laboratory demonstrations in addition to research activities or projects involving Industry. Consequently, the number, distribution, and specifications of the 3D printing systems were rather heterogeneous, which resulted in asymmetric capabilities. Forty-nine 3D printers were relocated from UCLM centers (faculties and research institutes) to some of the volunteers’ places to operate during the confinement. On the other hand, 16 industrial systems were used at the 3D printing lab at the Renewable Energy Research Institute (https://www.uclm.es/centros-investigacion/ier) in Albacete as those printers could not be moved and hence special permission was granted to some researchers to fabricate PPEs.
Table 1 shows the distribution of the UCLM members, collaborating in the initiative, as well as the distribution of resources throughout the region. Undoubtedly, this dispersion of human and material resources in different geographical locations made the initiative hard to coordinate.

Table 1.
Distribution of human and material resources at the University of Castilla-La Mancha (UCLM).
This was a key issue, as each maker (a maker is a person who prints manufactured objects using a 3D printer; in this case the 3D printing lab in Albacete will also be included as a maker, though it could be considered as a fabrication lab), or fabrication unit was relevant within the network. The availability of each maker may vary as a consequence of different personal conditions such as teaching activities, research commitments, or family obligations. As mentioned above, the 3D printing systems covered a wide range of specifications, from DIY (Do-It-Yourself) kits to industrial models, which implied rather diverse production rates and PPEs with different properties (aesthetic, mechanical, etc). To summarize, the human resources and the equipment were rather heterogeneous and scattered in a rather vast region. Therefore, it was highly demanded to find out how to maximize the production capacity and define an efficient system to answer the requests in the shortest period of time. This further highlighted the need to use customized technology to facilitate the coordination among the volunteers and to ensure the delivery to the end-users. Customized technology implies a digital innovation and transformation, and is related to new services, new platforms, or even new business models in a given context [25].
In addition, the UCLM must address some further issues:
- Promotion of the initiative throughout the region to reach all potential users requiring PPEs.
- Development of a mechanism to facilitate people applying for PPEs.
- Fundraising to purchase raw materials.
Certainly, in this context, customized technology may help considerably to address the problems outlined above.
3. Organizational Model and Problem Analysis
At the beginning of the confinement on 14 March 2020, the UCLM urgently established the COVID-19 Monitoring Committee (https://www.uclm.es/misiones/lauclm/institucional/uclmsaludable/saludentornolaboral/covid-19) to monitor any activities related to the health crisis, which involved the use of scientific infrastructure or participation of university staff. The manufacture of PPEs via 3D printing became a hot topic.
Next, we present the organization models followed during this initiative. Two stages are distinguished: an initial stage, from 23 March to 5 April, with the goal to ensure the initiative began and first urgent requests were addressed, and a second stage (from 6 April to 2 May), to optimize the fabrication and delivery of the 3D printed parts.
3.1. Initial Stage: Centralized Model (from 23 March to 5 April)
Because of the emergency, the UCLM commission initially opted for a centralized management model in the Toledo campus to meet all the requests from the region. For this purpose, a simple web form was provided to allow institutions to formally request the manufacture of PPEs. The communication among makers was conducted through a mailing list and data were stored in local spreadsheets. The different fabrication units (makers) had to report the number of PPEs produced daily to have an estimate of the available stock.
During the first days of the crisis, numerous requests were received from hospitals, health centers, retirement homes, judiciary and law enforcement bodies, civil protection, etc. Occasionally, some of these requests involved the fabrication of up 1000 units, mostly face shields. Considering that a basic FDM-3D printing kit requires an average of 1 h to manufacture a headband, orders above 100 units implied the coordination of several fabrication units, which sent their stock to Toledo. Once in Toledo, the products were distributed to the end-users. The limitations of that model were obvious, as the printed objects had to travel from various locations in the region to Toledo, and then to travel again to their final destinations, which could be relatively close to some of the fabrication units. This was clearly inefficient and fabrication units with larger production capacities, i.e., the 3D printing lab in Albacete, could not work correctly under this model and was forced to attend large orders outside the system to shorten delivery dates. At this point, it must be stressed that quick responses were mandatory, as PPEs were urgently needed in hospitals and health centers about to collapse. Additionally, it should be pointed out that the centralized model also implied higher shipping/transport costs. To sum up, this system caused a rather poor service in terms of response time and costs.
From the management point of view, this system also implied an important load of work for the team responsible for the coordination in Toledo, as they were in charge of:
- Management of all the requests for the entire region.
- Permanent contact with each fabrication unit to know their production rate as this may not be constant in time and stock must be monitored.
- Collection of the fabricated PPEs from each fabrication unit.
- Preparation of the orders and distribution to end-users.
In addition, at an internal level the coordinators must:
- Ensure stock and distribution of the raw materials required by each fabrication unit.
- Give technical support to the fabrication units in case of faults/breakdowns in domestic 3D printers.
Consequently, Toledo became the bottleneck of the system hindering a quick and effective response to all the requests coming from a rather vast region. A summary of the problems that arose during this initial stage is listed in Table 2. As the coordination was extremely complicated and the system was clearly inefficient, we proposed several changes in the organization to maximize the production and minimize the time of response and costs associated.
Table 2.
Problems derived from the initial management model.
3.2. Stabilization Stage: Decentralized Model (from 6 April to 2 May)
Despite all the drawbacks, the centralized model and the tools implemented allowed most of the collaborators to initiate their fabrication processes quickly. However, the problems highlighted in Table 2 inevitably led to a new management model that should be supported by an information system developed ad-hoc.
The desired system must avoid the bottleneck produced by the central management system. For this purpose, the system must provide automatic recommendations for assignments between requests and production units that optimize production and delivery times. As an option, the system must also offer the fabrication units the possibility of self-assigning requests. Based on the premise that each fabrication unit is adequate to estimate its expertise and manufacturing capacity, dedication, and stock of raw material, the possibility of decentralizing management and distributing simple tasks among all participants in the manufacturing network was considered.
Such a decentralized model required the development of a web-based information system that would allow the management required in addition to addressing the issues included in Table 2.
4. Web System for the Optimization of Manufacturing and Distribution of Materials
The ad-hoc development of a web information system (https://impresion3d.uclm.es) between the third and fourth week gave support for the new model management:
- Providing an accessible site to order PPEs for both institutions: formal/official orders and individuals.
- Facilitating the decentralized management of requests by the fabrication units.
- Capacity to auto-assign and self-assign orders in real-time according to production capability and availability. The system was also flexible allowing reassignments when appropriate.
- Controlling the life cycle of an order.
- Managing the fabrication units.
- Storing the information in a relational database protected according to various security protocols. The database management system also provided efficient information retrieval.
Furthermore, the system should:
- Follow the aesthetics and style lines of the UCLM. The site must be quickly associated with the institution.
- Accessible from anywhere with an Internet connection, on any device, any time. Due to the confinement of society, this was essential.
- Ensure positioning in the first places of the most popular search engines. It was important to reach the largest number of individuals, particularly within the healthcare system.
- Attract more potential fabrication units within the UCLM community.
- Record the activity of each fabrication unit. At the end of the initiative, the UCLM must publish a public memory of all the activities performed to justify the use of funding raised.
- Comply with current legislation on data protection.
4.1. Brief Description of the Developed System
A group of Computer Engineers from the School of Computer Science (https://esi.uclm.es), supported by personnel from the Technology, Information, and Communications area of the UCLM, were in charge of the design and development of the system. The group developed within one week a web information system that was a perfect answer to the problem described above. During the following week, the web system team continued refining the website, fixing some bugs, and adding improvements while the system was in use.
Figure 4 shows the general scheme of the proposed system. Individuals and institutions, from different locations, register PPE requests through the web interface. All the information is recorded in a database, which is managed in the persistence layer of the system. On the other hand, fabrication units that are geographically distributed can self-assign requests or follow the indications of the recommending system. The recommending system tries to determine the best fit between requests and fabrication units based on the volume of the request and the capacity of the units to handle it. Once the 3D parts are manufactured, these are sent to the destination (origin of the request).
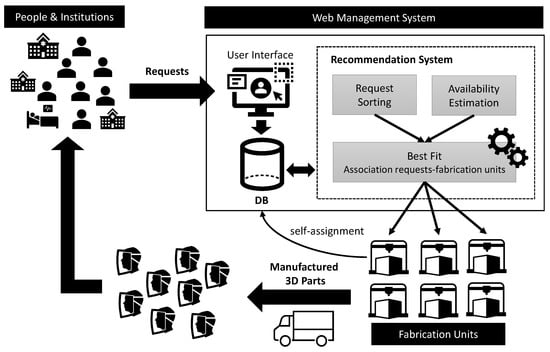
Figure 4.
General scheme of the designed and developed system.
The web solution consisted of a frontend, which was accessible by anyone, anywhere, and anytime. Using the frontend, any organism/individual could register their requests. On the other hand, a backend in which the functionality depends on the user’s profile.
The frontend displayed public information about the initiative and was divided into several sections: who we are?, how can I help?, partners, beneficiaries, and finally the contact section. Moreover, the website frontend showed the 3D parts fabricated (see Figure 5). Figure 6 shows the three products (face shields, ear-savers, and intubation boxes) that UCLM offered, although upon request some other elements such as valves for oxygenation systems, shields for medical instruments, etc., were also produced.
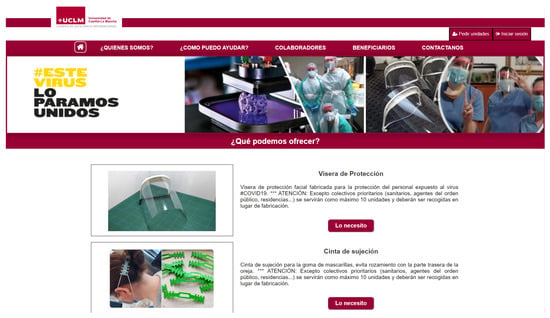
Figure 5.
Home page displayed on the frontend of the web information system.
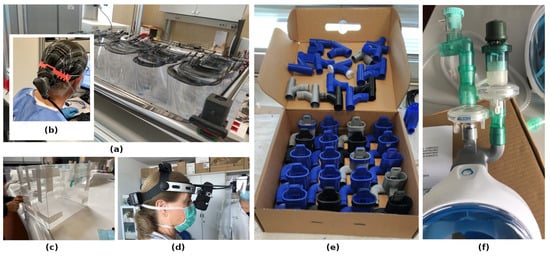
Figure 6.
Some products manufactured by UCLM in the solidarity project. (a) Face shields, (b) ear-savers, (c) personal protective equipment (PPE) box for the protection of healthcare professionals in the process of intubation, (d) customized face shield coupled to ophthalmoscopes, (e) detail of Charlotte valve coupled to air filters, and (f) Charlotte valves and Dave coupling for oxygenation systems based on Decathlon snorkel masks.
To facilitate the process of selecting 3D parts, we used a procedure similar to any online shopping experience. Nowadays, most users are familiar with online shopping and this kind of virtual market. In this type of environment, products are grouped in a virtual shopping cart. Once the products have been chosen, the request is confirmed (see Figure 7). The applicant’s contact details are recorded while the PPEs are selected, i.e., without a prior registration process. This means that the user did not have to go through a laborious registration process beforehand. The main idea was to simplify the overall application process as much as possible, especially since the users who requested the material did not have much spare time.
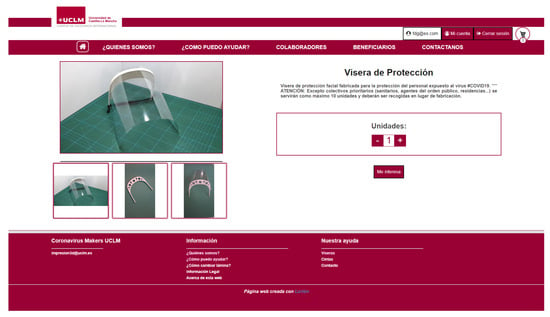
Figure 7.
PPE request (type and quantity of units) in the web information system.
On the other hand, the backend is the private area of the web information system where the UCLM members carried out their activity. The backend allowed the creation of users with two possible associated roles: administrator and fabrication unit. The administrator had superior privileges and was responsible for aspects of customization and configuration of the system. On the other hand, each fabrication unit had access to all orders and received suggestions from the recommendation system to meet requests that fit well with its profile; also the system gave the possibility of self-assigning requests. When a fabrication unit accepted a suggested request or self-assigned one of them, it automatically became responsible for both the manufacture and delivery to the end-user. From the backend, a fabrication unit could access the specific details of each order, i.e., the product card. Such a product card showed the items ordered, the quantities, and destination, including the contact details. The system also highlighted the orders that had not yet been fulfilled, those that had been assigned, and the status of each order (see Figure 8).
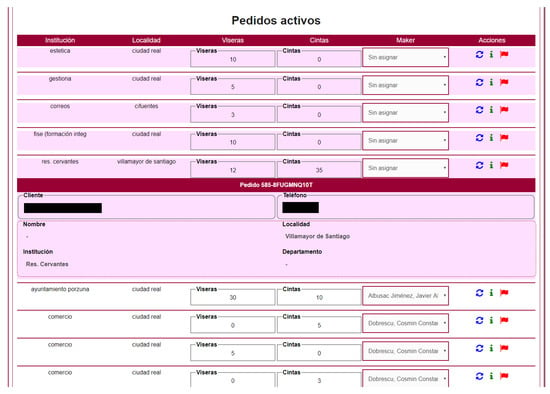
Figure 8.
Listing of products in the manufacturing process. Access to the product detail. Monitoring of the status of each product.
Regarding the process of self-assignment, each fabrication unit must satisfy the following criteria:
- Requests must be geographically close to the fabrication unit. A fabrication unit could give support to remote locations if there was no closer fabrication alternative.
- The manufacturing process and delivery should be completed within two days. If this was not possible, the fabrication unit must transfer the request to another unit to keep delivery times in two days (priority target).
Orders could vary between three states: unassigned, assigned, and closed. When an order was assigned to a fabrication unit, then its status changed to assigned. The order was then moved from the pending list to the list of orders in production. When the order was finally delivered, the status changed to closed and disappeared from the list of orders in production. Therefore, the system had three lists where any order could be found according to its current state: non-assigned, in production, and closed.
The delivery of the manufactured PPEs was performed via three possible routes: (a) the applicant had to pick the material up at the manufacturing location (preferred), (b) the material was transported with the help of police or civil protection (second-best) and, finally, (c) if neither of the two previous methods was possible, a private delivery service was used. The first two methods were at no cost from the production point of view, while the third implied extra cost, i.e., part of the funds raised had to be invested in this concept.
Information was stored in a MySQL relational database, which was hosted on a Microsoft Azure server, with security control. The agile access and recovery of the information were fundamental for the following reasons: (a) prevent attending duplicated requests. During the crisis period, it was a rather common situation having several employees of the same institution working in different units and making independent requests, which overlapped. (b) During the project, there had also been attempts to make fake applications in the name of real institutions, to subsequently put the manufactured and donated parts on sale. The system detected requests from institutions that have already been served, and they were dealt with special attention. (c) As mentioned before, there was a need to record the production statistics to report weekly to the COVID-19 monitoring committee of the University of Castilla-La Mancha.
Finally, the system managed the supply of raw materials to each fabrication unit (PLA, ABS, PVC sheets, rubber bands, and EVA), as the corresponding stocks were collected and monitored to ensure adequate supply and not to stop the fabrication process.
4.2. Recommender System for the Effective Assignment of Requests and Optimization of Delivery Times
The core of the web system includes a recommender subsystem that aims at automatically assigning requests and optimizing manufacturing and delivery times. The main goal is to reduce the time between a request and its delivery to a maximum of two days. The algorithm takes into account the current workload of the collaborators (fabrication units) and tries to find an optimal planning in which the times are minimized.
Each time a person or institution orders one or several 3D parts, a request is generated into the system. A request r is defined as the tuple , i.e., , where p is the priority of the request, is the number of items requested (or 3D parts), d is the date of request and is the place of request.
The priority is established according to the type of applicant and will take values in the range [1–5], with five being the highest priority. Table 3 summarizes the association between priorities and the different sectors.
Table 3.
Association of priorities to the sectors.
The system has a finite set of fabrication units, . That is, places where 3D parts are made (homes or laboratories). A fabrication unit j denoted as is defined as the pair , i.e., , where is the place where is located the fabrication unit and is its production capacity. The concept of production capacity captures how many items are being produced over an hour. Each fabrication unit has one or more 3D printers, each with different features and production capacity. Production capacity of the unit will be calculated as:
where is the production capacity of the 3D printer, of which the type is i and n is the number of them available in the unit. The value is the number of items that an i type printer can produce per hour. On the other hand, L is a list of ordered requests according to the following criterion:
To make the assignment of the first request of the list L to one fabrication unit, the following steps are done:
1. Calculate the estimated manufacturing time of the requested items in for each available fabrication unit . The estimated time is noted as , and the distance between the place of manufacture and the point where the request is made, it is noted as . The value is calculated as:
where is the number of items of the request and is the production capacity of the fabrication unit .
2. Calculate for each fabrication unit available and its suitability for the request, it will be noted as and calculated as:
where and are two parameters used to weight the importance of each of the factors affecting the calculation (manufacturing time and distance). We set them to and to penalize the cost of transport more than completion time. In other words, it was more important for us to deal with the request early than the effort it might take to send them to the destination. Parameters and meet the following restrictions: (1) and (2) .
3. Select the fabrication unit which has the best suitability for the request:
4. Update the resources available in the fabrication unit by removing those assigned to the last request .
As long as there are requests on the list L, these steps will be repeated.
4.3. Other Problems Solved
In addition to the development of the technology to support the initiative, it was necessary to enhance the visibility and, of course, raise funding. The following sections describe in more detail how both aspects were addressed.
4.3.1. Dissemination of the Initiative
In order to reach the largest number of institutions/people requiring PPEs, two goals must be achieved: (1) the website had to appear in the top positions of popular search engines, especially in searches from the region. Therefore, we worked on both on-page and off-page factors. (2) Give visibility to the initiative in social networks.
Once the system was developed and opened on the Internet, it was disseminated through social networks, both in the official accounts of the UCLM, as well as through the personal Twitter and Facebook accounts of the members of the UCLM fabrication network. In addition, the system was linked from the official website of the university (www.uclm.es). The initiative was well-received by society and spread quickly through the networks and media (television, radio, and newspapers). As an example, one of the Tweets (https://twitter.com/jalbusac/status/1249278511749136385) published on 12 April promoting the initiative was retweeted 797 times, received 447 likes, had a total of 93,598 impressions in one day, and 10,711 interactions.
The website was rapidly positioned in the top positions of popular search engines and the goal of reaching the largest number of people was achieved. As visibility increased, new requests came from other regions such as Madrid, Barcelona, Valencia or even South America. External requests were never met because they fell outside the scope of the project, and similar social movements existed in their regions. Another consequence of the increased visibility was the involvement of volunteers from outside the UCLM. These groups decided to call all the retirement homes in Castilla-La Mancha, which had not yet been contacted and registered these latter requests on the website. As of 3 May, most of the priority services in the region, including the healthcare system, judicial and law enforcement bodies, civil protection, and retirement homes, have been served by manufacturing over 23,500 3D parts.
4.3.2. Fundraising
Obviously, the fabrication of thousands of PPEs required funding and as the number of requests grew, minor donations coming from the fabrication units could not cover the expenses. Therefore, the UCLM launched an extraordinary crowdfunding campaign (https://www.uclm.es/perfiles/empresa/colaboracionmecenazgo/patrocinioymecenazgo/ayudascovid19-uclm) to fund the solidarity initiatives already mentioned. On the first day, the UCLM raised 57,000 euros to support those projects. At present, the total of donations received exceeds one million euros and 18,500 euros had been destined for the manufacture of PPEs by means of 3D printing.
As transparency is a major issue in public organisms such as the UCLM, the web system also automatically published in the frontend the places where the manufactured products were destined and the quantities. Consequently, any citizen can always check the destination of the donations.
5. Results
The most relevant results of the UCLM social project to fight against the COVID-19 pandemic in Castilla-La Mancha (Spain) via 3D printing of PPEs will be presented in this section. These results will be analyzed considering the impact of switching organizational models between an initial centralized model and a decentralized model assisted by a collaborative web information system for the stabilization stage. These two organizational models have been analyzed by QGIS (QGIS Geographic Information System, Open Source Geospatial Foundation, v3.12) considering lineal spatial interpolation, P coefficient of 2, and the value of 0.001 for both X and Y resolutions.
During the first 40 days of this work, the UCLM manufactured and delivered 12,363 face shields and 10,867 ear-savers. In the initial stage (from 23 March to 5 April), 5160 face shields were produced, whilst 7266 face shields and 10,867 ear-savers were manufactured in the stabilization stage (from 6 April to 2 May).
As mentioned above, the first stage of the project was carried out according to a central distribution model based in Toledo (see Figure 9), following the initial instructions given by the COVID-19 Monitoring Committee of the UCLM. The 5160 facial shields manufactured during this stage in the 29 fabrication units were sent to Toledo and then distributed to 37 destinations (see Table 4). Table 5 shows the relation between production and demand in each province. As can be seen, Albacete was the most demanded campus (57.1% see Figure 10) and led the production of face shields (67.9%). As their production capacity was higher, this allowed them to back up the other campuses as is shown by the flux () in Table 5.
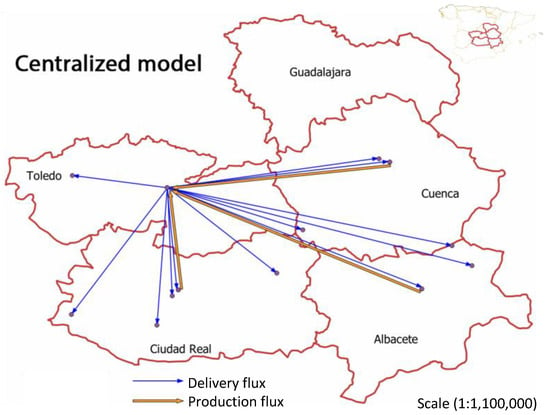
Figure 9.
Flux map of the face shields production (orange arrows) and deliveries (blue arrows) from the central distribution model.
Table 4.
PPE destinations for centralized and decentralized models.
Table 5.
Production and requesting of face shields per province in the central distribution model.
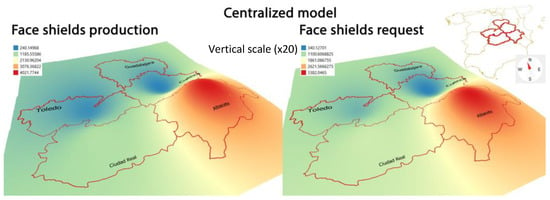
Figure 10.
3D production volume and delivery maps of face shields in the central distribution model with the same perspective point and vertical scale (×20).
This was rather paradoxical as the production from Albacete should have been sent to Toledo for the distribution and, in the case of requests from locations close to Albacete, sent them back. Obviously, this strategy could not be applied and Albacete had to work out of the system being the main producer. This caused a rather chaotic situation that complicated the processing of orders, preventing them from working at full capacity and delaying deliveries. To sum up, and as previously stated (see Section 3.1), this centralized model settle in Toledo was the bottleneck hindering a quick and effective response to all the requests coming from a rather vast region (see Figure 9).
The second stage of the project used a decentralized distribution model based on a collaborative web information system, where each fabrication unit self-assigned the requests according to their capacity and availability, taking care of the entire process, i.e., from production to delivery (see Figure 10). Thus, the previous organizational bottleneck was eliminated, and the overall process improved as the orders could be attended in real-time and the fabrication units could establish defined timetables and plan their activity carefully. This helped to increase the productivity and therefore reduce the delivery times, as well as to reach a greater number of towns in the region. A further advantage of the web system was the possibility of attending requests from remote locations, small towns, or villages. In the initial model, as orders were centralized in Toledo following a protocol, which included formal communication, there were barely requests from small towns or villages and most of the orders were from highly populated areas. As collected in Table 4 the number of destinations markedly increased from 37 to 242. Consequently, changing to the web system facilitated access to any individual no matter the location, facilitating direct interaction between the fabrication unit and the end-user.
Moreover, at this stage a new element was manufactured: the ear-savers which, as mentioned above, is not a protective item, but improves the well-being of the healthcare professionals. This new product further increased the number of requests, and the number of 3D parts per request because some of them included face shields in addition to ear-savers.
Table 6 shows the relation between production and demand in each province corresponding to the second stage. As can be seen, each fabrication unit attended preferentially the requests made in their province. The net flux and , Table 6) shows as the provinces with demands above their capacity for face shields were supported by Albacete, which remained as the campus with the highest production capacity (see Figure 11). The analysis of the PPE flux reveals Ciudad Real, Cuenca, and Toledo as receiving 3D parts by the top producer Albacete. Ciudad Real (224%), Cuenca (288%) and Toledo (115%) increase their face shield requests in the decentralized model compared to the initial stage. However, the number of face shield requests in Albacete decreased by 59% during the second stage, which implied that most of the requests were already met during the initial stage, and allowed to back the other provinces up.
Table 6.
Production and requesting of face shields and ear-savers per province in the decentralized distribution model.
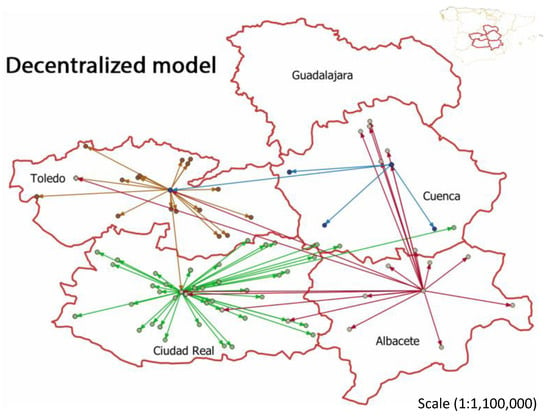
Figure 11.
Flux map of the PPE production and delivery in a decentralized organizational model.
As per the individual PPEs (Figure 12), Albacete and Toledo had an overproduction of face shields, whereas Ciudad Real and Cuenca could not meet their demand. The situation was similar in the case of the ear-savers, as there was an overproduction in Albacete and Ciudad Real, whereas Toledo and Cuenca were underproducing (see Figure 13). However, the analysis for the deliveries for both products reveals a homogeneous distribution, mainly focused in the capital cities where the main hospitals of the region are located, except in the case of the Toledo province, with two equally populated cities: Toledo and Talavera de la Reina.
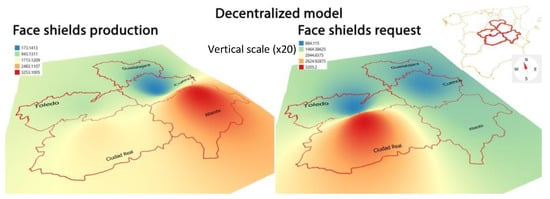
Figure 12.
Flux map of the face shields production and delivery in the decentralized organizational model.
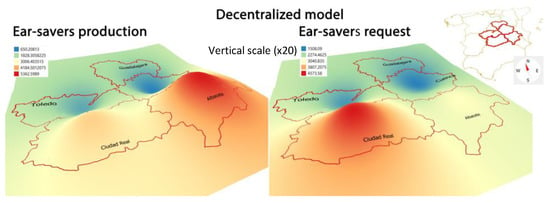
Figure 13.
Flux map of the ear-savers production and delivery in the decentralized organizational model.
As for the number of requests and units produced, Albacete (4753 face shields) and Ciudad Real (4639 face shields) were both the most demanding, around three times more than Cuenca (1320 face shields) or Toledo (1651 face shields). Toledo is the most populated province (see Table 7) but the levels of demand were much lower. These results suggest that the decentralized model favors the supply criteria of proximity as the top producing centers coincide with the top demanding areas. This also implies lower costs and quicker responses.
Table 7.
Province population and PPE total delivered of each production province.
The estimation of the health sector (Source: https://www.ine.es/covid/covid_salud.htm) in each province (Table 8) provides the ratio of healthcare professionals, which have received 3D printed PPEs within this project. From these data, some conclusions may be extracted. On the one hand, the overall number of face shields delivered to the healthcare system may have been enough to protect the entire population of health professionals (physicians, nurses) in a region with 25.62 people/km. The distribution was not homogeneous and, in some cases, the number of face shields exceeded the overall number of health professionals, whilst in some others the percentage of medical staff with access to the 3D printed PPEs was rather low. Several factors may explain this trend, such as the different production capacity of the fabrication units and, in the case of Toledo, the proximity to Madrid and its metropolitan area may have an important impact, as the fabrication capacities (industrial or solidarity initiatives) nearby the capital city are much stronger.
Table 8.
Health sector and PPE 3D printed ratios.
It should be pointed out that there are some other workers in the system that require protection, such as cleaning staff, cooks, and janitors, that can be considered as non-medical staff. The requests received did not discern between medical and non-medical staff and that would explain why the number of requests could be higher than the population of medical staff. Nevertheless, considering that the breakdown of the beneficiaries of the initiative (Table 9) indicate that 60% of the PPEs produced went to the healthcare system, one may assume that this initiative could have largely supplied PPEs for all medical and non-medical staff in the region if focused exclusively to this sector. This is clear evidence of the impact of this project for Castilla-La Mancha.
Table 9.
Beneficiaries of 3D parts organized by sector.
On the other hand, Figure 14 shows the evolution of the production rate in both stages during 40 days. This evolution is presented by relating the number of requests per week, the unmet requests per week and, finally, the number of manufactured parts per week. From 6 April, when the organizational changes were implemented and the web information system was enabled, a significant increase in the production rate took place. During this growth interval, both new requests were attended to and pending works from the previous weeks were attended to. As can be observed, all requests were totally met as of 13 April once the system recovered from the previous poor management. It should be noted that this was achieved when the requests were peaking, which is further evidence of the benefits of the web-based decentralized model.
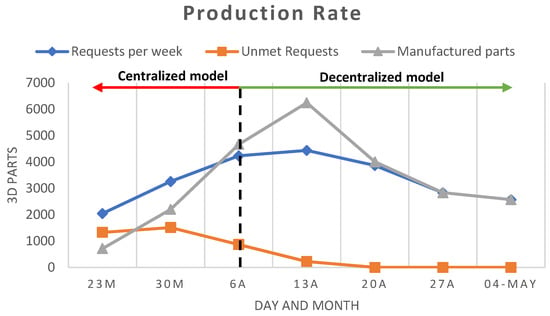
Figure 14.
Production rate of both centralized and decentralized systems within the studied/considered period. The relation among requests per week (blue line), unmet requests per week (orange line), and manufactured parts (grey line) per week is shown.
Furthermore, the increase in the production rate led to a reduction in the average delivery time. Figure 15 shows the reduction of the average response time down to two days. The two previous indicators, productivity and average delivery time, are two clear indicators that the measures taken helped to enhance the efficiency of the production system, hence improving the use of available resources.
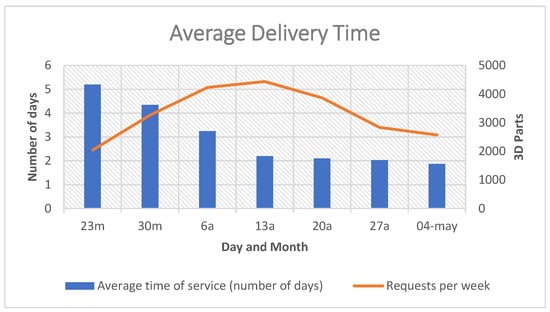
Figure 15.
Average time of services (number of days). Average time, in days, needed to attend the applications. The data are recorded per week, from 16 March to 4 May 2020.
Finally, regarding the economic cost of the initiative only considering the materials required in the fabrication process, i.e., excluding electricity costs (which were assumed by the volunteers), shipping/transport costs (higher in the first days with the centralized model and not exceeding 1000 euros), replacement and repair of breakdowns in 3D printers (close to 200 euros), i.e., paying only attention to the manufactured elements, face shields were produced at 0.8 cents/unit (10,969.6 euros in total) and the ear savers at 0.11 cents/unit (1030 euros in total). This makes a total of 11,999.6 euros in materials for the period of time considered in this study.
6. Conclusions
In a context of emergency due to COVID-19 expansion and shortage of PPEs supply in the healthcare system, a solidarity project carried out by the UCLM produced 23,500 3D parts in 40 days assisted by FDM 3D printing to cover the needs of Castilla-La Mancha (Spain).
During the first days of the project, the requests were attended via a centralized model, which was highly inefficient and caused delays in deliveries. Therefore, a web information system was developed ad-hoc to help in the transition towards a decentralized model. During the second stage, and despite the increasing number of requests, the times of response were quickly reduced down to two days, facilitating planning of the fabrication units and reducing costs related to distribution. The use of the web information system also allowed reaching more destinations and remote areas that could not be attended to during the first stage.
The design of a recommender module for the assignment of requests to fabrication units, according to their workload or availability and the distance between origins and destinations, has also been an important contribution resulting in significant benefits in terms of time and costs. This experience shows the advantages of using technology to develop systems that improve internal processes in any social cooperation. In particular, this work aims to be an example that encourages non-profit associations to consider the need to undertake the digital transformation to improve their processes and achieve their objectives.
The project has allowed protecting healthcare professionals in about 280 locations in the region, mainly in the provincial capitals, manufacturing about 13,000 face protection items and about 11,000 ear-savers. The healthcare and law enforcement sectors have been the main beneficiaries. In particular, 13,917 PPEs have been supplied for health professionals (60.4% of the total), and 2733 for law enforcement officers (11.79% of the total).
Author Contributions
Conceptualization, M.C.-G. and J.C.-V.; Formal analysis, J.A., J.J.C.-S. and J.C.P.-F.; Funding acquisition, J.A.; Investigation, J.A., J.J.C.-S., J.C.P.-F. and J.C.-V.; Methodology, J.A., J.J.C.-S. and J.C.-V.; Resources, J.C.P.-F. and J.C.-V.; Software, J.A. and J.J.C.-S.; Supervision, J.A., J.J.C.-S. and J.C.-V.; Validation, J.A., M.C.-G. and J.C.P.-F.; Visualization, M.C.-G.; Writing–original draft, J.A. and J.C.P.-F.; Writing–review and editing, J.J.C.-S., M.C.-G. and J.C.-V. All authors read and agreed to the published version of the manuscript.
Funding
The authors would like to thank every individual, company or institution for their financial support via the UCLM crowdfunding campaign. Thanks also to our colleagues at UCLM for their contribution coordinating, manufacturing and distributing the 3D printed materials. The authors are also very grateful to the civil protection service and different bodies of the police for their help to distribute the produced PPEs, especially during the lockdown.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Yang, Z.; Dang, Z.; Meng, C.; Huang, J.; Meng, H.; Wang, D.; Chen, G.; Zhang, J.; Peng, H. Propagation analysis and prediction of the COVID-19. medRxiv 2020. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, N. Economic Effects of Coronavirus Outbreak (COVID-19) on the World Economy. 2020. Available online: https://ssrn.com/abstract=3557504 (accessed on 23 October 2020). [CrossRef]
- Wang, W.T. Knowledge management adoption in times of crisis. Ind. Manag. Data Syst. 2009, 4, 445–462. [Google Scholar] [CrossRef]
- Newman, M. Covid-19: Doctors’ leaders warn that staff could quit and may die over lack of protective equipment. BMJ 2020, 368. [Google Scholar] [CrossRef] [PubMed]
- Livingston, E.; Desai, A.; Berkwits, M. Sourcing Personal Protective Equipment During the COVID-19 Pandemic. JAMA 2020. [Google Scholar] [CrossRef] [PubMed]
- Davis, G.F.; Zald, M.N. Social Change, Social Theory, and The Convergence of Movements and Organizations. In Social Movements and Organization Theory; Davis, G.F., McAdam, D., Scott, W.R., Zald, M.N., Eds.; Cambridge Studies in Contentious Politics; Cambridge University Press: Cambridge, UK, 2005; pp. 335–350. [Google Scholar] [CrossRef]
- Young, A.; Selander, L.; Vaast, E. Digital organizing for social impact: Current insights and future research avenues on collective action, social movements, and digital technologies. Inf. Organ. 2019, 29, 100257. [Google Scholar] [CrossRef]
- Stein, L. Social movement web use in theory and practice: A content analysis of US movement websites. New Media Soc. 2009, 11, 749–771. [Google Scholar] [CrossRef]
- George, J.J.; Leidner, D.E. From clicktivism to hacktivism: Understanding digital activism. Inf. Organ. 2019, 29, 100249. [Google Scholar] [CrossRef]
- Benjamin, V.; Chen, H.; Zimbra, D. Bridging the virtual and real: The relationship between web content, linkage, and geographical proximity of social movements. J. Assoc. Inf. Sci. Technol. 2014, 65, 2210–2222. [Google Scholar] [CrossRef]
- Wasko, M.M.; Faraj, S. Why should I share? Examining social capital and knowledge contribution in electronic networks of practice. MIS Q. 2005, 29, 35–57. [Google Scholar] [CrossRef]
- Wasko, M.M.; Faraj, S.; Teigland, R. Collective action and knowledge contribution in electronic networks of practice. J. Assoc. Inf. Syst. 2004, 5, 493–513. [Google Scholar] [CrossRef]
- Nan, N.; Lu, Y. Harnessing the power of self-organization in an online community during organizational crisis. Mis Q. 2014, 38, 1135–1158. [Google Scholar] [CrossRef]
- Hargrave, T.J.; Ven, A.H.V.D. A Collective Action Model of Institutional Innovation. Acad. Manag. Rev. 2006, 31, 864–888. [Google Scholar] [CrossRef]
- Shirky, C. Here COMES Everybody: The Power of Organizing without Organizations; Penguin Books: London, UK; New York, NY, USA, 2008. [Google Scholar]
- Li, X.; Shu, C.; Liu, X.; Yu, B.; Yang, L.; Zhang, H.; Huang, G.; Tang, L.; Xu, M.; Zhou, J.; et al. Comparison of Clinical Features in Octogenarian and Non-Octogenarian Adults with Severe COVID-19 Pneumonia. Available online: https://www.researchsquare.com/article/rs-18587/v1 (accessed on 23 October 2020).
- WHO. Modes of Transmission of Virus Causing COVID-19: Implications for IPC Precaution Recommendations: Scientific Brief, 27 March 2020; Technical Report; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Cavallo, L.; Marcianò, A.; Cicciù, M.; Oteri, G. 3D Printing beyond Dentistry during COVID 19 Epidemic: A Technical Note for Producing Connectors to Breathing Devices. Prosthesis 2020, 2, 46–52. [Google Scholar] [CrossRef]
- Javaid, M.; Haleem, A.; Vaishya, R.; Bahl, S.; Suman, R.; Vaish, A. Industry 4.0 technologies and their applications in fighting COVID-19 pandemic. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 419–422. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Morales, J.; Tarancón, A.; Canales-Vázquez, J.; Méndez-Ramos, J.; Hernández-Afonso, L.; Acosta-Mora, P.; Rueda, J.M.; Fernández-González, R. Three dimensional printing of components and functional devices for energy and environmental applications. Energy Environ. Sci. 2017, 10, 846–859. [Google Scholar] [CrossRef]
- Huang, Y.; Leu, M.C.; Mazumder, J.; Donmez, A. Additive Manufacturing: Current State, Future Potential, Gaps and Needs, and Recommendations. J. Manuf. Sci. Eng. 2015, 137. [Google Scholar] [CrossRef]
- Lipson, H.; Kurman, M. Fabricated: The New world of 3D Printing; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Montville, R.; Schaffner, D. Inoculum size influences bacterial cross contamination between surfaces. Appl. Environ. Microbiol. 2003, 69, 7188–7193. [Google Scholar] [CrossRef] [PubMed]
- Nambisan, S.; Lyytinen, K.; Majchrzak, A.; Song, M. Digital Innovation Management: Reinventing innovation management research in a digital world. Mis Q. 2017, 41, 223–238. [Google Scholar] [CrossRef]















Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).