1. Introduction
Nowadays, partially and completely edentulous patients can be treated with implant-supported prosthesis as a reliable and predictable treatment option [
1,
2]. A pivotal contribution in reaching this goal was provided by the continuous improvement in quality of prosthetic components. As far as esthetics and function are concerned, several implant-supported prosthetic solutions can satisfy patient expectations [
3,
4]. To this purpose, Romeo et al., in their prospective longitudinal study on partial edentulism [
5], reported high prognostic rates: success ranged from 89% to 95.3% while cumulative survival ranged from 93.6% to 96.7%, after 3 to 7 years of loading, respectively.
Precisely, the most frequent long-term complications associated with dental implants are mucositis and peri-implantitis [
6]. As a matter of fact, peri-implantitis is highly prevalent and may affect 7.8–43.3% of all implants studied and reported in dental literature [
6,
7,
8,
9,
10].
On the whole, an initial peri-implant bone loss of 2–3% has been reported that is followed by a further 2–3% loss over a period of 5 years regarding implants supporting fixed partial dentures (FPDs) [
11]. On the other hand, concerning fixed prosthesis longevity, a 5 year survival rate of 96.5% for single tooth replacement, 95.4% for partial implant-supported fixed prosthesis and 90.1% for implant-tooth reconstruction were shown in several systematic reviews [
12,
13,
14].
Hence, due to the high success and survival rates available in the literature concerning dental implants, “classical” Albrektsson success criteria [
15] underwent an evolution; nowadays, clinicians and researchers all over the world are mainly paying attention to the marginal bone level changes over the years [
16,
17].
Nevertheless, it has to be highlighted that higher survival and lower complication rates also depend on a positive learning curve in implant dentistry, as reported in recent clinical studies [
18]. Related to this, it is widely reported that an internal-conical-connection between the abutment and the implant may contribute to the stability of peri-implant hard tissues, if compared to flat-to-flat interfaces [
19,
20,
21,
22]. However, recent outcomes from a systematic review and meta-analysis comparing the conical internal connection (IC) with the external hexagonal connection (EH) on the occurrence of marginal bone loss (ΔMBL) disagreed with this statement [
23]. In fact, no statistically significant differences were found for ΔMBL one, three and five at one, three and five years after loading between implant connections (
p < 0.05), and statistically significant differences were found for PD between EH and IC implants (1 year follow-up) −0.53 (95%CI −0.82 to −0.24,
p = 0.0004). On the contrary, the role of platform switching in implant abutment is still unclear [
24,
25].
The present prospective longitudinal study aimed at evaluating the radiographical and peri-implant clinical outcomes of dental implants characterized by internal-conical-connection and platform switching after an observation period of 5 years.
Moreover, several potential patient-related risk factors influencing the peri-implant tissues and implant failures were analyzed.
2. Material and Methods
Seventy-eight patients were consecutively treated between 2009 and 2017 at the Dental Clinic, Department of Medicine and Surgery, University of Milan, Italy. The fundamental principles of the Declaration of Helsinki were followed in the conduction of the study. Before participating in the study, all patients signed a specifically designed consent form. No ethical committee document was provided as the reported treatments and the follow-up procedures only consisted of standard treatments and control visits.
Inclusion criteria were as follows: partial or complete edentulism; residual ridge volume of at least 3.3 mm in diameter and 8 mm in length as evaluated both clinically and radiographically; a favorable relationship with respect to the opposing dental arches; each dental implant included in the measurements needed a minimum 5 year follow-up. Only one type of implant-supported restoration for each patient was included in the present study. There was a yearly follow-up visit, in which oral hygiene control was carefully checked.
The following exclusion criteria were considered: active periodontal disease, heart disease, coagulation or leukocyte diseases, metabolic disorders, radiotherapy in the head and neck area, parafunctions such as clenching or bruxism, a smoking habit (more than 10 cigarettes per day), alcohol or drug abuse.
Patients were restored with implants with an internal-conical-connection (Astra Tech, Mölndal, Sweden), which supported fixed prostheses.
Peri-implant tissues were evaluated for concerns regarding probing pocket depth, bleeding on probing (bleeding index score of 0 to 3), and plaque index scores (on a scale of 0 to 3) [
5].
Intraoral radiographs were taken using the paralleling technique to control projection geometry, with exposure parameters of 65 to 90 kV, 7.5 to 10 mA, and 0.22 to 0.25 seconds [
5]. They were subsequently stored on a personal computer and analyzed using the program ImageJ (US National Institute of Mental Health, Bethesda, MD, USA) to determine bone level changes. Peri-implant bone resorption was assessed both mesially and distally, taking the implant head as a reference point. Radiographs were taken at baseline (loading time) and at the 5 year follow-up visit, which were analyzed and compared to verify any change in the peri-implant marginal bone level (
Figure 1). A radiographic control was performed during the yearly follow-up visits as well.
Several reference measurements were also considered: (i) implant neck diameter; (ii) implant length as the distance between the implant neck and the most apical point of each implant, along an ideal line running parallel to the implant axis. All measurements were performed by a single calibrated operator (A.P.). Calibration consisted of three-time measurements at three different time points by assessing fifteen radiographs with another author (D.L.) acting as reference examiner. Subsequently, intra-examiner and inter-examiner reliability were calculated (k = 0.90 and k = 0.85, respectively).
After a 3 month submerged healing, transmucosal healing abutments were connected at surgical re-entry. Hence, pre-prosthetic evaluation was performed 3 months after implant placement. Two weeks after surgical re-entry, an implant impression was taken, and a provisional restoration was screwed into position. Therefore, after maturation of the peri-implant soft tissues (2–3 months after provisional delivery), a second implant impression was taken for the final implant-supported restoration. Definitive abutments were screwed into position using 35 Ncm of torque. For all the fixed prostheses, a platform switching connection between fixture and abutment was provided. Cemented prostheses were fixed with zinc oxyphosphate cement or zinc-eugenol oxide cement, while screw-retained prostheses were secured by applying a 15 Ncm torque to the abutment framework screw using a manual torque driver.
Statistical Analysis
Mean values, standard deviations (SDs) and cumulative frequencies were calculated for the above-mentioned implant-related biometric parameters. The efficacy variable was the change in the peri-implant bone-level. Clinical data were considered as descriptors. The peri-implant bone level data were analyzed at implant and patient level. Bivariate analysis was performed either considering dental implant or patient as statistical unit. Analysis of variance and post hoc analysis with Bonferroni correction when indicated were formulated in order to evaluate marginal bone level in the different time intervals, while a multilevel analysis was used to evaluate the influence of different factors affecting bone loss at implant level. A p-value less than 0.05 was considered as statistically significant. A specifically designed software (SPSS 21.0; SPSS, Inc., Chicago, IL, USA) was used for all the statistical analyses.
3. Results
Seventy-eight patients receiving 209 implants were enrolled in the present clinical investigation. Forty-three patients were male (55.1%) and thirty-five patients were female (44.9%). Patients’ mean age at time of surgery was 55.4 ± 10.7 years (range 26–84 years). Sixteen patients (20.5%) were smokers and sixty-two (79.5%) were non-smokers as reported in
Table 1.
One-hundred implants were placed in the maxilla (21 in the anterior and 79 in the posterior segment) and 109 in the mandible (25 in the anterior and 84 in the posterior segment), respectively (
Table 2).
Implants length was 8 (two implants), 9 (32), 11 (105), 13 (65) 15 (5) mm, respectively. All implants features are reported in
Table 3.
Out of 78 treated patients, 11 (14.1%) with 29 (13.9%) dental implants dropped out and were not considered in the statistical analysis (
Table 4). One patient dropped out after 1 year of follow up. Six patients were lost after two years. Four patients who received two implants each were lost after 3 years.
No implants were lost during the osseointegration period. One implant affected by peri-implantitis was removed four years post-insertion. No specific anatomical condition was detected as promoting an inflammatory status of peri-implant hard and soft tissues. On the contrary, peri-implantitis was successfully treated in two different patients (one implant each). In all cases, the patients were smokers.
The average final pocket probing depth at implant level was 2.5 ± 1.2 mm. Probing depths at mesial, distal, buccal, and lingual sites of 3 mm or less were observed at 89.4%, 89.9%, 90.4%, 90.9% of all implants, respectively. An overall success rate of 90.1% was calculated after 5 years of follow-up.
Standardized periapical radiographs were used to measure bone loss. The average final bone loss after 5 years of evaluation was 0.3 ± 0.4 mm, both at the mesial and distal aspect of the implant.
The effects of multiple implants in the same patient were analyzed and were not statistically significant (p = 0.605).
The effects of the prosthesis type on marginal bone loss were analyzed, even if no statistical difference was noticed (p = 0.092). Three different sub-groups were considered for the statistical analysis: single tooth (79 prostheses), partial (98) and full (32) prostheses, respectively. Similarly, no statistical difference was calculated for each sub-group (p = 0.103, 0.098 and 0.127, respectively).
Moreover, sex was not correlated to peri-implant marginal bone loss (
p = 0.125). Prosthesis type and distribution are reported in
Table 5.
Furthermore, smoking and its potential effect on implant peri-implant bone stability was analyzed. To this purpose, an average marginal bone loss of 0.3 ± 0.3 mm was calculated for implants placed in non-smoker patients while implants placed in smoker patients showed an average marginal bone loss of 0.5 ± 0.5 mm. Such difference was statistically significant (p = 0.021).
Data on different parameters and the respective effect on marginal bone loss are reported in
Table 6.
Moreover, the site of implant placement and the respective effect on the bone loss was considered. In the anterior maxilla, an average bone remodeling of 0.3 ± 0.3 mm was found while an average bone remodeling of 0.4 ± 0.6 mm was found in the posterior maxilla. Similarly, in anterior and posterior mandibula, a mean bone remodeling of 0.5 ± 0.4 and 0.3 ± 0.4 mm were calculated, respectively. All these comparisons were not statistically significant (p > 0.05).
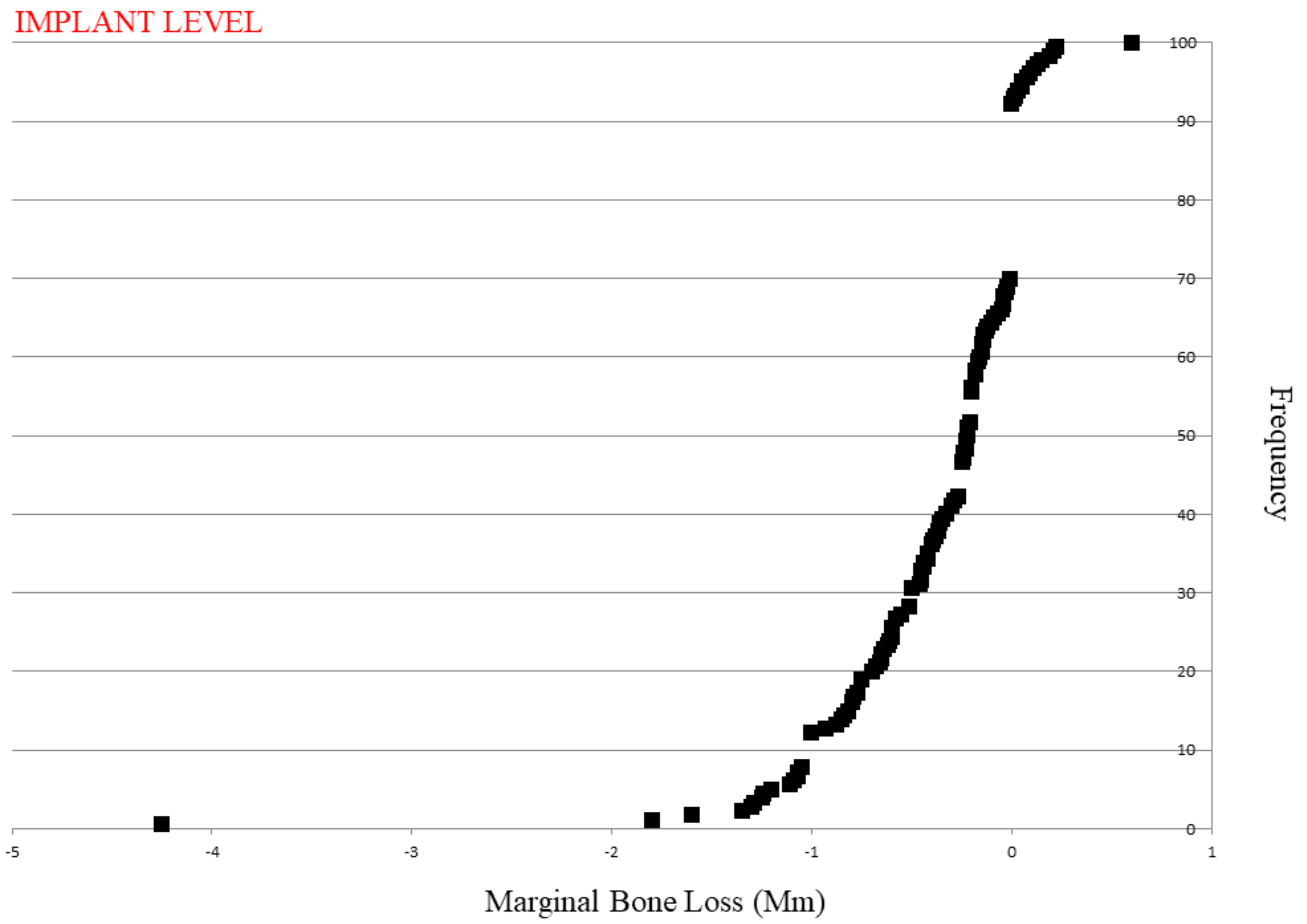
Average bone loss cumulative frequency distribution at implant level is presented in
Figure 2 while cumulative frequency distribution of average bone loss at patient level is reported in
Figure 3. After five years of loading, 12.2% of implants showed a mean 1 mm of marginal bone loss; at the same time, 30% of implants showed 0.5 mm of radiographic bone loss, while 8% of implants showed a marginal bone gaining.
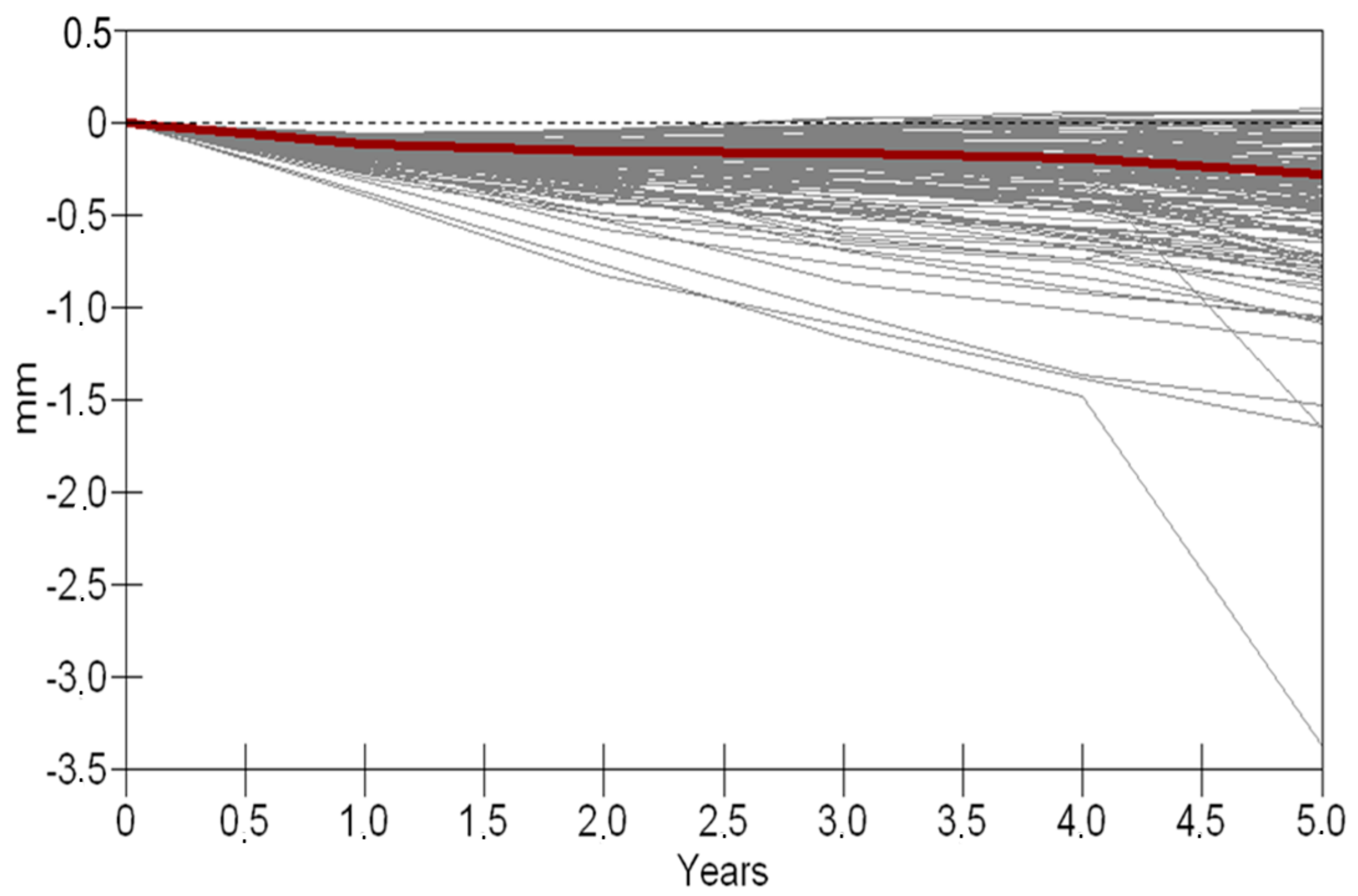
The 5 year marginal bone loss (MBL) changes from the implant loading are shown in
Figure 4.
4. Discussion
The present retrospective longitudinal study aimed to evaluate the outcome of implant-supported restorations after 5 years of function. Regarding the present study outcomes, the marginal bone level stability measurements could be addressed to the implant to abutment stability. This is directly influenced by the type of connection, even if platform switching may help achieve ridge dimension preservation and enhance the stability of peri-implant soft tissues [
26]. In fact, the role of platform switching on the stability of the peri-implant hard tissue is still unclear [
24,
25,
27,
28], and controversy on hard tissue preservation with the platform switching technique remains unsolved [
29]. Nevertheless, bone-level implants have been created with many connection configurations. Locking-taper conical connection implants have proven superior to buttress joint implants at achieving a tight seal and eliminating the micro-gap at the implant-to-abutment junction and have demonstrated improvements in crestal bone maintenance. According to these findings, the internal-conical-connection of the implants included in the present report seemed to positively influence the peri-implant bone stability [
19,
20,
21,
22].
Several potential risk factors that might influence peri-implant tissues and implant failures were also evaluated. Other studies by Wennström et al. [
26] reported a similar 5 year failure rate, specifically a failure rate of 5.3% at the PFD (partial fixed dentures) level and 2.7% at implant level were calculated and a good medium-term prognosis of implant-supported rehabilitations was confirmed.
Only a smoking habit, even related to smokers that smoke up to 10 cigarettes per day, was found to be statistically significant as far as bone loss is concerned. Indeed, 0.5 ± 0.5 mm of bone loss was suffered by implants placed in smoker patients while non-smoker patients experienced an average marginal bone loss of 0.3 ± 0.3 mm. It could be assumed that patients reporting to be light smokers stated facts that were not entirely true. Similarly, a systematic review conducted by Moraschini et al. in 2016 [
30] agreed with such outcomes, reporting a statistically significant difference of marginal bone loss when considering smokers versus non-smokers. To be more precise, a range of bone loss between 0.07 and 0.9 mm with a mean value of 0.5 mm was reported. Nevertheless, the clinical significance of 0.2 mm of bone loss might be questioned. Since smoking was the only statistically significant risk factor, no multilevel analysis was performed to compare other variables. In the end, average bone loss around implants might not be affected by factors such as sex, insertion site and prosthesis type. In this respect, the same parameters were evaluated in a prospective study accounting for 630 patients and 1569 implants, which was conducted by Rammelsberg et al. [
31] in 2017. The authors reported that incidence of implant-related complications was not significantly influenced by implant location, age, sex, or implant placement associated with GBR procedures.
In the present study,
Figure 3 on 5 year bone loss changes could be superimposed to the outcomes of Fransson and Tomasi [
16]. In such a scenario, the authors analyzed the bone loss pattern of peri-implantitis-associated bone loss on 419 implants with up to 23 years of observation. To summarize, a tendency of 0.15 mm peri-implant bone loss per year was predicted by the authors. In the present analysis, a similar trend is displayed.
Finally, implant-supported restorations showed a high success rate and a tendency of implant loss similar to previous studies considering at least 5 years of function [
1,
2,
3,
4,
5]. Smoking was the only variable showing statistical significance with respect to bone loss. Nevertheless, it should be highlighted that this finding might not be correlated to a poorer prognosis from a clinician’s point of view.
5. Conclusions
Within the limits of the present clinical study, dental implants with internal-conical-connection showed stable peri-implant bone levels at the medium-term follow-up (5 years). Nevertheless, further clinical studies with adequate methodology and sample size and with a more consistent observation period are warranted to confirm the trends and results found in the present report.



 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}