Ageing-Related Gait Adaptations to Knee Joint Kinetics: Implications for the Development of Knee Osteoarthritis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Setup
2.3. Protocol
2.4. Parameters
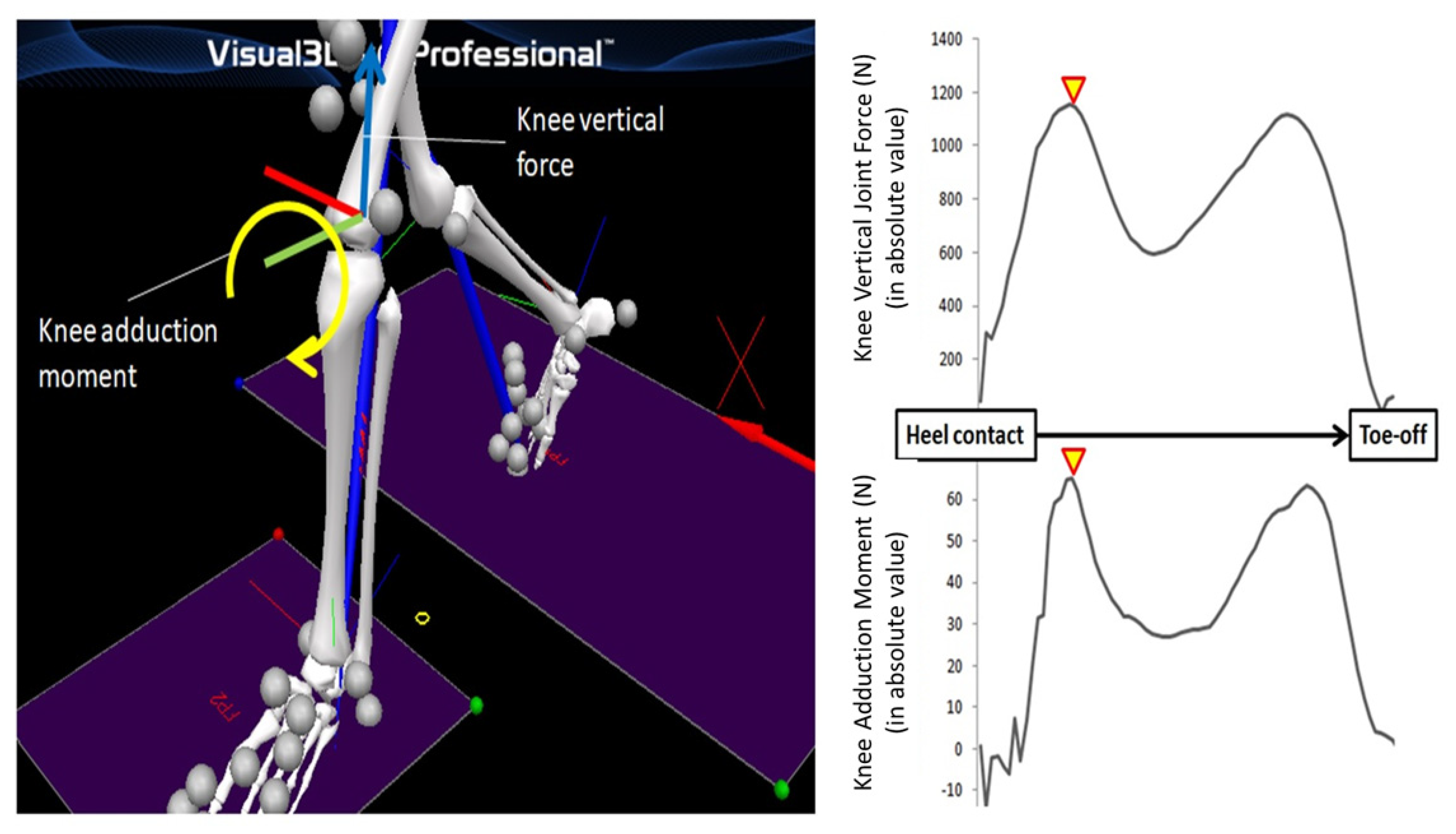
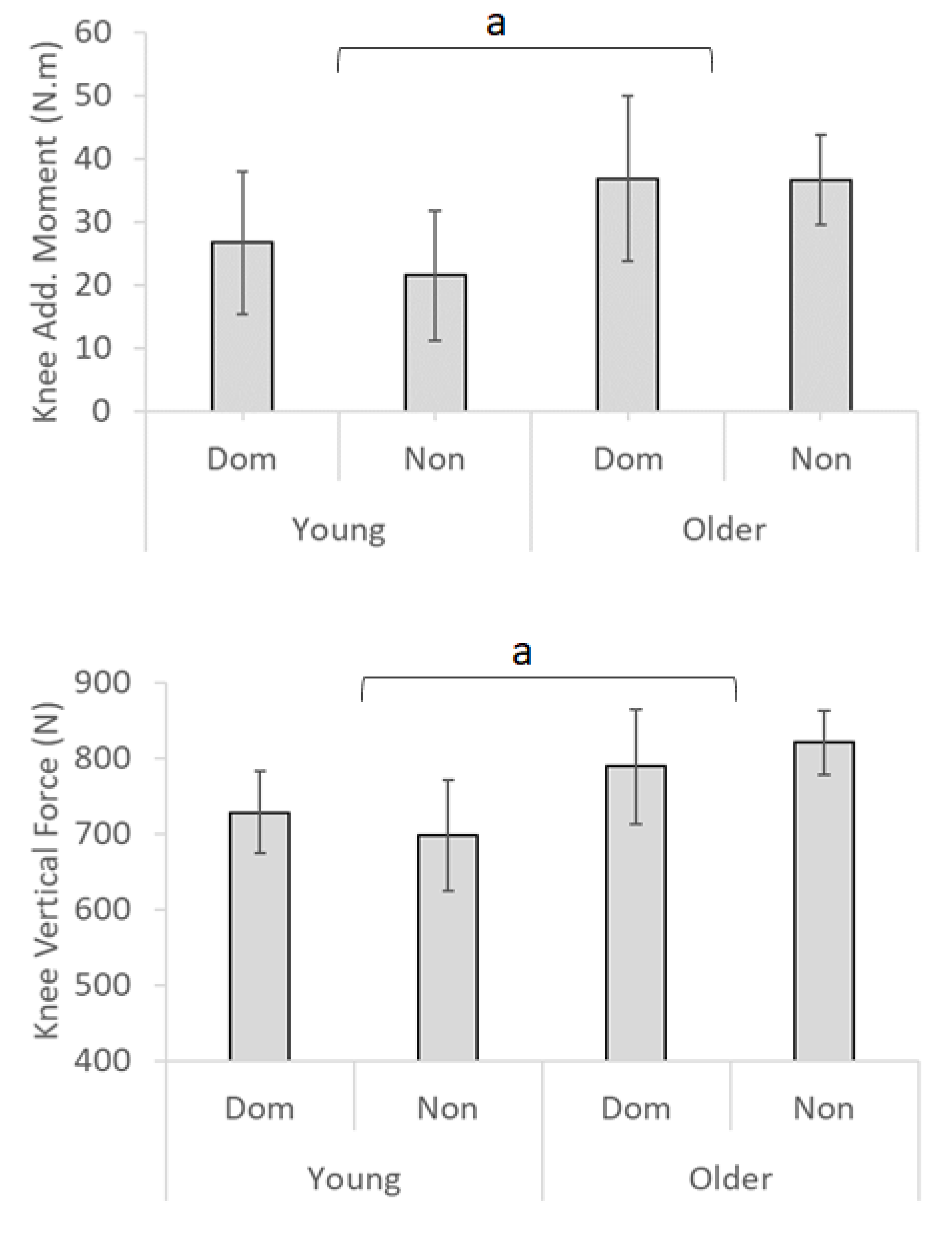
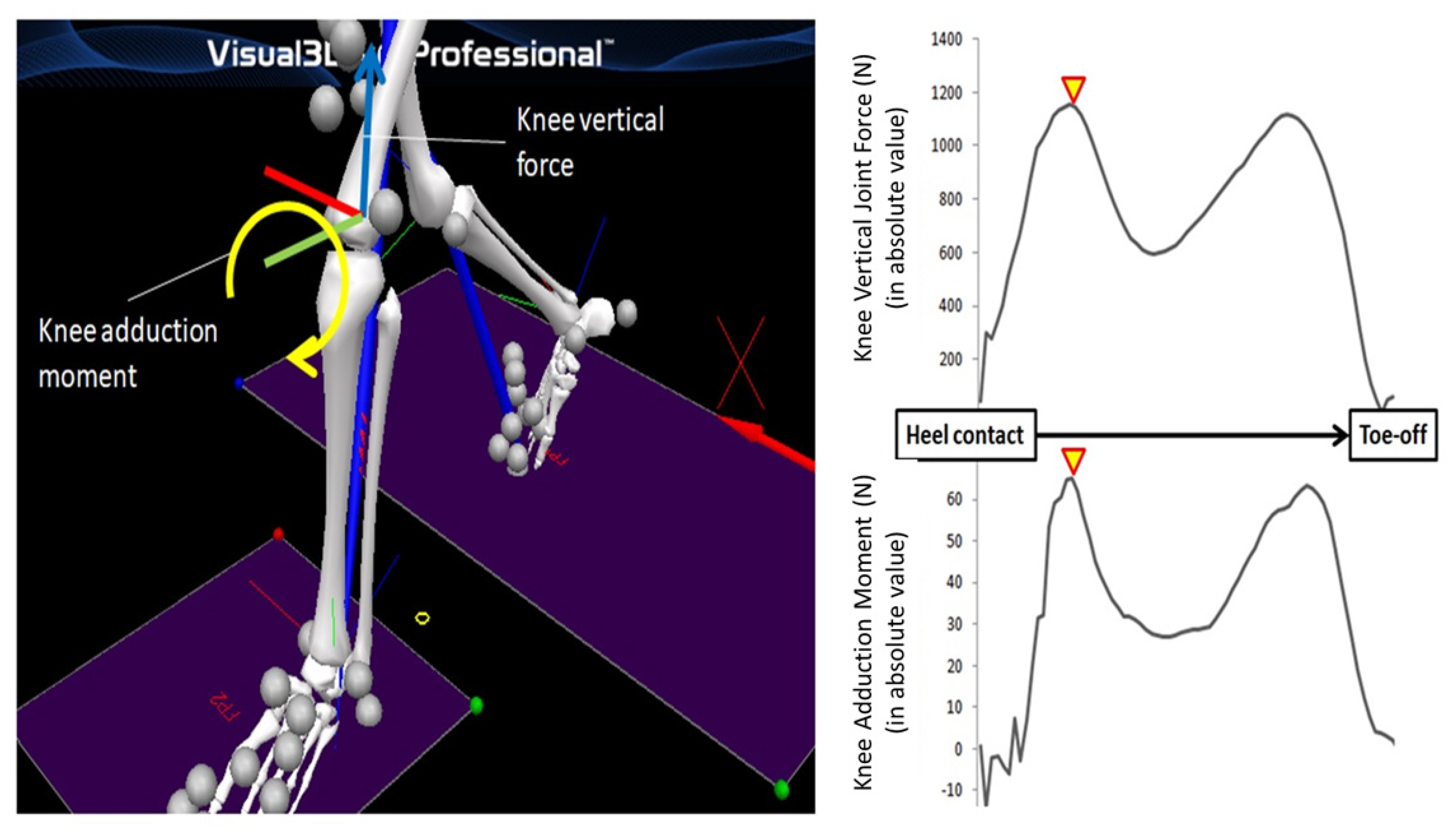
2.4.1. Knee Joint Kinetics
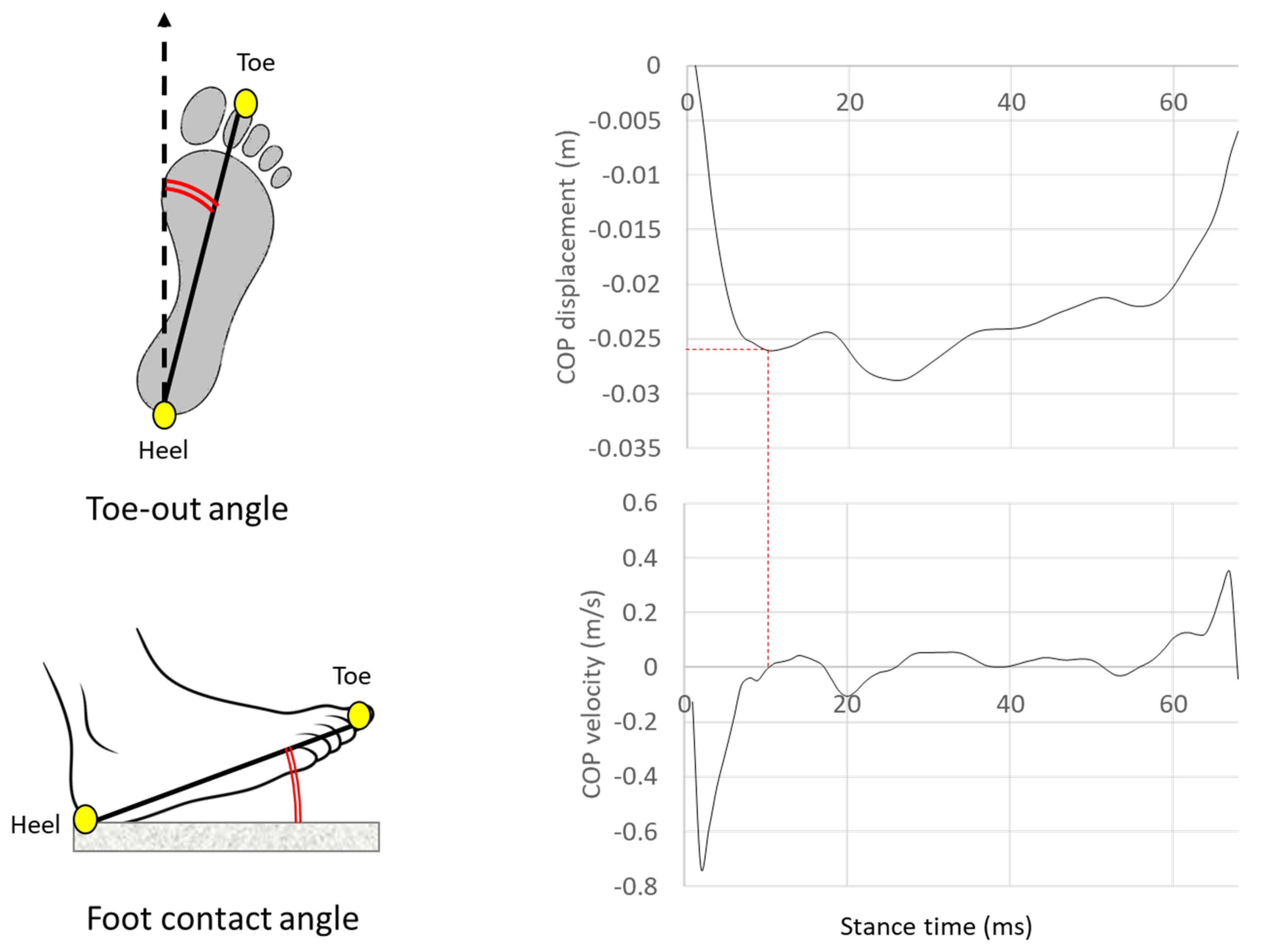
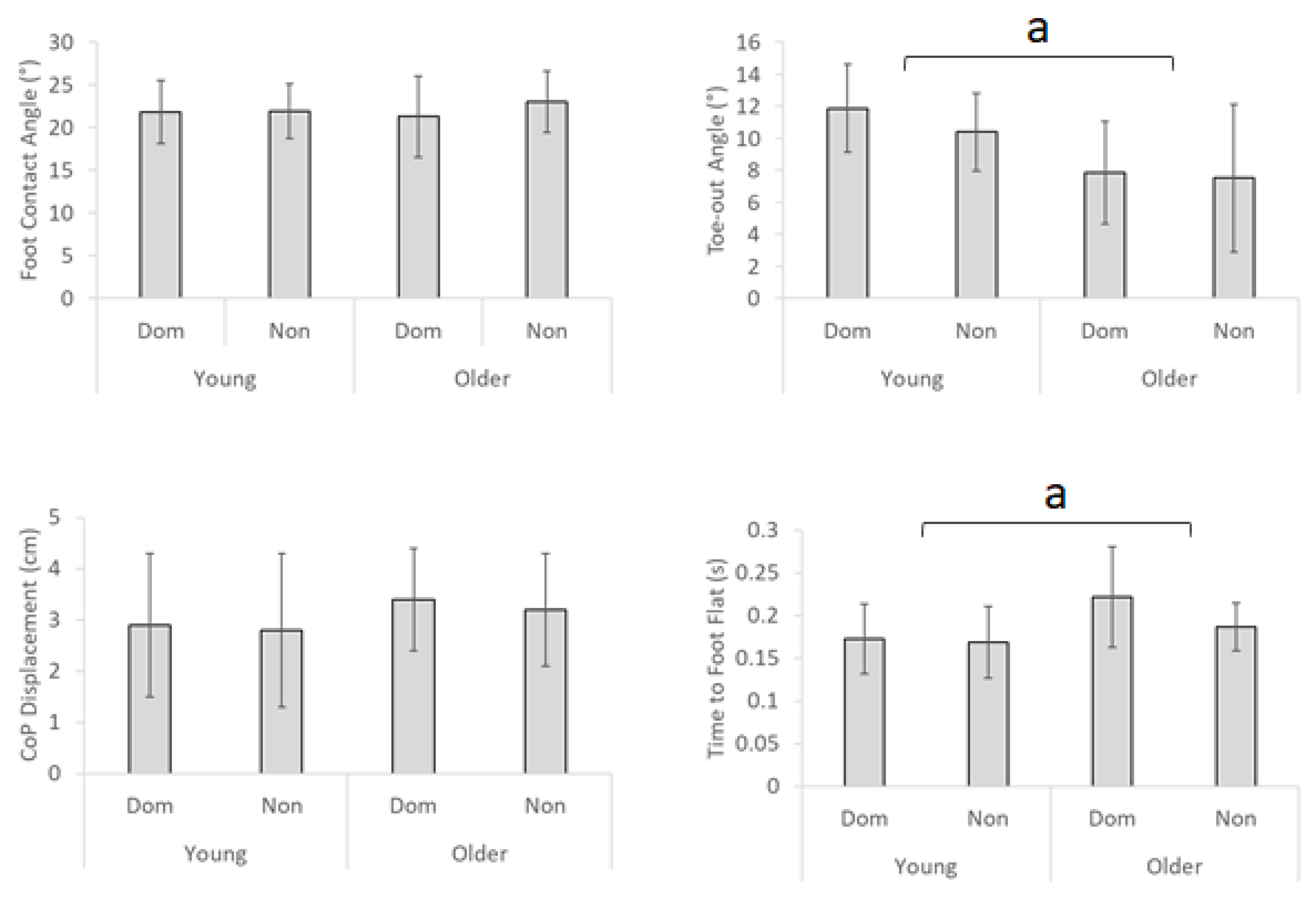
2.4.2. Foot Motion
2.4.3. COP Displacement
2.4.4. Time to Foot Flat
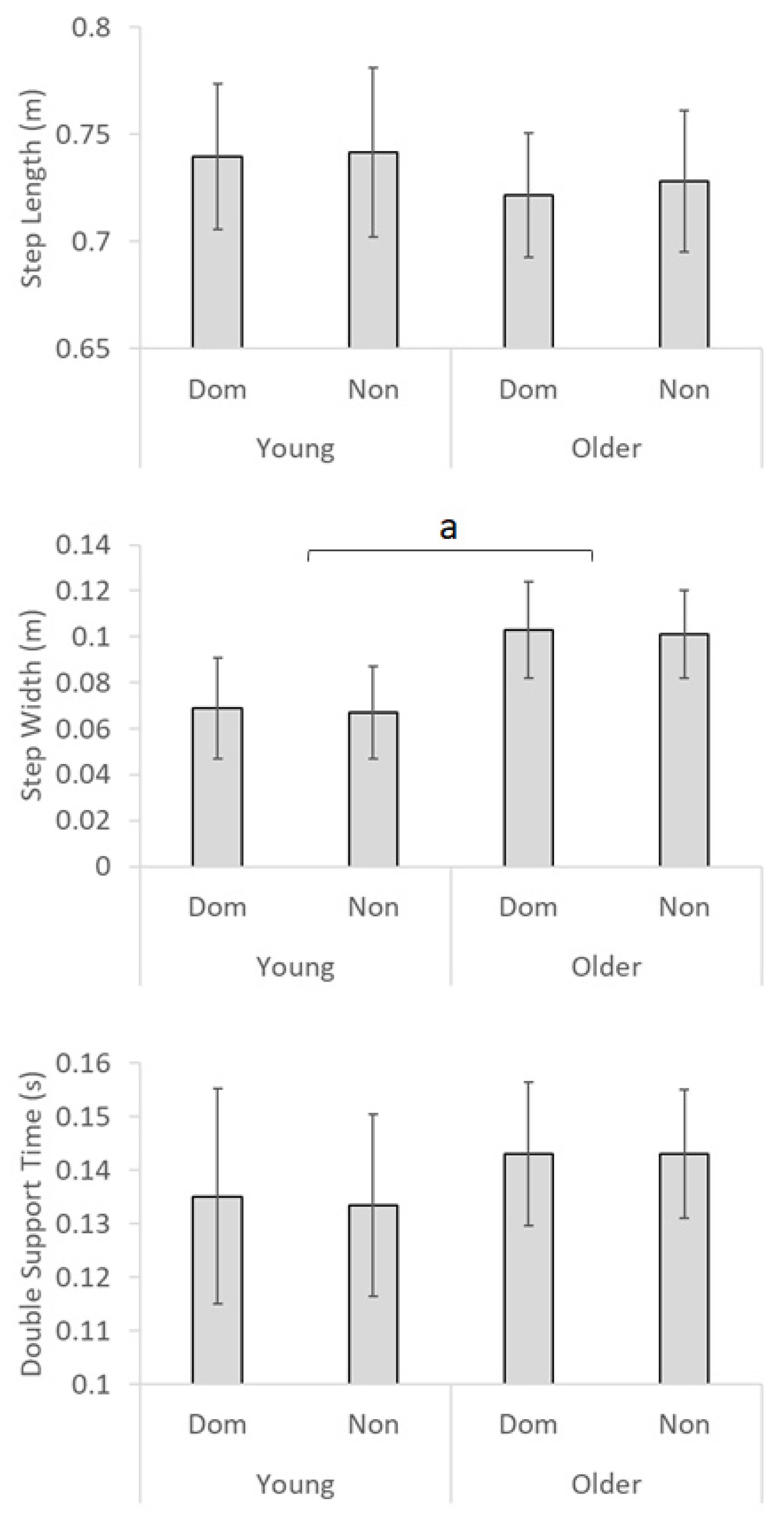
2.4.5. Spatio-Temporal Parameters
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Xie, Y.; Yu, Y.; Wang, J.-X.; Yang, X.; Zhao, F.; Ma, J.-Q.; Chen, Z.-Y.; Liang, F.-R.; Zhao, L.; Cai, D.-J.; et al. Health-related quality of life and its influencing factors in Chinese with knee osteoarthritis. Qual. Life Res. 2020, 29, 2395–2402. [Google Scholar] [CrossRef] [PubMed]
- Levinger, P.; Menz, H.B.; Morrow, A.D.; Bartlett, J.R.; Feller, J.; Bergman, N.R. Relationship between foot function and medial knee joint loading in people with medial compartment knee osteoarthritis. J. Foot Ankle Res. 2013, 6, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, T.-W.P.; Shorter, K.A.; Adamczyk, P.G.; Kuo, A.D. Mechanical and energetic consequences of reduced ankle plantar-flexion in human walking. J. Exp. Biol. 2015, 218, 3541–3550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki, K.; Neptune, R.R. Muscle mechanical work and elastic energy utilization during walking and running near the preferred gait transition speed. Gait Posture 2006, 23, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Cavagna, G.; Thys, H.; Zamboni, A. The sources of external work in level walking and running. J. Physiol. 1976, 262, 639–657. [Google Scholar] [CrossRef] [PubMed]
- Gustafson, J.A.; Anderton, W.; Sowa, G.A.; Piva, S.R.; Farrokhi, S. Dynamic knee joint stiffness and contralateral knee joint loading during prolonged walking in patients with unilateral knee osteoarthritis. Gait Posture 2019, 68, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Walter, J.P.; D’Lima, D.D.; Colwell, C.W., Jr.; Fregly, B.J. Decreased knee adduction moment does not guarantee decreased medial contact force during gait. J. Orthop. Res. 2010, 28, 1348–1354. [Google Scholar] [CrossRef] [Green Version]
- Liphardt, A.; Mündermann, A.; Koo, S.; Bäcker, N.; Andriacchi, T.; Zange, J.; Mester, J.; Heer, M. Vibration training intervention to maintain cartilage thickness and serum concentrations of cartilage oligometric matrix protein (COMP) during immobilization. Osteoarthr. Cartil. 2009, 17, 1598–1603. [Google Scholar] [CrossRef] [Green Version]
- Fukaya, T.; Mutsuzaki, T.; Mori, K. Relations between external moment and movement of the knee joint during the stance phase in patients with severe knee osteoarthritis. J. Orthop. 2019, 16, 101–104. [Google Scholar] [CrossRef]
- Shull, P.B.; Shultz, R.; Silder, A.; Dragoo, J.L.; Besier, T.F.; Cutkosky, M.R.; Delp, S.L. Toe-in gait reduces the first peak knee adduction moment in patients with medial compartment knee osteoarthritis. J. Biomech. 2013, 46, 122–128. [Google Scholar] [CrossRef]
- Messier, S.; Legault, C.; Loeser, R.F.; Van Arsdale, S.J.; Davis, C.; Ettinger, W.H.; DeVita, P. Does high weight loss in older adults with knee osteoarthritis affect bone-on-bone joint loads and muscle forces during walking? Osteoarthr. Cartil. 2011, 19, 272–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tajima, T.; Tateuchi, H.; Koyama, Y.; Ikezoe, T.; Ichihashi, N. Gait strategies to reduce the dynamic joint load in the lower limbs during a loading response in young healthy adults. Hum. Mov. Sci. 2018, 58, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Obrębska, P.; Skubich, J.; Piszczatowski, S. Gender differences in the knee joint loadings during gait. Gait Posture 2020, 79, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Zheng, J.J.Y.; Li, G.; Yuan, J.; Ebert, J.; Li, H.; Papadimitriou, J.; Wang, Q.; Wood, D.; Jones, C.W.; et al. Pathogenesis and clinical management of obesity-related knee osteoarthritis: Impact of mechanical loading. J. Orthop. Transl. 2020, 24, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Bennett, H.J.; Shen, G.; Cates, H.E.; Zhang, S. Effects of toe-in and toe-in with wider step width on level walking knee biomechanics in varus, valgus, and neutral knee alignments. Knee 2017, 24, 1326–1334. [Google Scholar] [CrossRef] [PubMed]
- Simic, M.; Hinman, R.S.; Wrigley, T.V.; Bennell, K.L.; Hunt, M.A. Gait modification strategies for altering medial knee joint load: A systematic review. Arthritis Rheum. 2010, 63, 405–426. [Google Scholar] [CrossRef] [PubMed]
- Ota, S.; Ueda, M.; Aimoto, K.; Suzuki, Y.; Sigward, S. Acute influence of restricted ankle dorsiflexion angle on knee joint mechanics during gait. Knee 2014, 21, 669–675. [Google Scholar] [CrossRef]
- Goryachev, Y.; Debbi, E.M.; Haim, A.; ROzen, N.; Wolf, A. Foot center of pressure manipulation and gait therapy in fluence lower limb muscle activation in patients with osteoarthritis of the knee. J. Electromyogr. Kinesiol. 2011, 21, 704–711. [Google Scholar] [CrossRef]
- Seeley, M.; Umberger, B.R.; Shapiro, R. A test of the functional asymmetry hypothesis in walking. Gait Posture 2008, 28, 24–28. [Google Scholar] [CrossRef]
- Nagano, H.; Begg, R.K.; Sparrow, W.A.; Taylor, S. A Comparison of Treadmill and Overground Walking Effects on Step Cycle Asymmetry in Young and Older Individuals. J. Appl. Biomech. 2013, 29, 188–193. [Google Scholar] [CrossRef]
- Fusco, N.; Cretual, A. Instantaneous treadmill speed determination using subject’s kinematic data. Gait Posture 2008, 28, 663–667. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, C.M.; Thorpe, S.K.; O’Malley, M.J.; Vaughan, C.L. Automatic detection of gait events using kinematic data. Gait Posture 2007, 25, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Osaki, Y.; Kunin, M.; Cohen, B.; Raphan, T. Three-dimensional kinematics and dynamics of the foot during walking: A model of central control mechanisms. Exp. Brain Res. 2006, 176, 476–496. [Google Scholar] [CrossRef] [PubMed]
- Mariani, B.; Rouhani, H.; Crevoisier, X.; Aminian, K. Quantitative estimation of foot-flat and stance phase of gait using foot-worn inertial sensors. Gait Posture 2013, 37, 229–234. [Google Scholar] [CrossRef]
- Nagano, H.; Begg, R.K. Shoe-Insole Technology for Injury Prevention in Walking. Sensors 2018, 18, 1468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zafar, A.Q.; Zamani, R.; Akrami, M. The effectiveness of foot orthoses in the treatment of medial knee osteoarthritis: A systematic review. Gait Posture 2020, 76, 238–251. [Google Scholar] [CrossRef] [PubMed]
- Charlton, J.M.; Hatfield, G.L.; Guenette, J.A.; Hunt, M.A. Toe-in and toe-out walking require different lower limb neuromuscular patterns in people with knee osteoarthritis. J. Biomech. 2018, 76, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.J.; Khan, S.S.; Usman, J.; Khana, S.J.; Khana, S.S.; Usmana, J. The effects of toe-out and toe-in postures on static & dynamic balance, risk of fall and TUG score in healthy adults. Foot 2019, 39, 122–128. [Google Scholar] [CrossRef]
- Perry, M.C.; Carville, S.F.; Smith, I.C.H.; Rutherford, O.M.; Newham, D.J. Strength, power output and symmetry of leg muscles: Effect of age and history of falling. Graefe’s Arch. Clin. Exp. Ophthalmol. 2006, 100, 553–561. [Google Scholar] [CrossRef]
- Nagano, H.; Tatsumi, I.; Sarashina, E.; Sparrow, W.; Begg, R.K. Modelling knee flexion effects on joint power absorption and adduction moment. Knee 2015, 22, 490–493. [Google Scholar] [CrossRef]
- Schmitz, R.J.; Harrison, D.; Wang, H.-M.; Shultz, S.J. Sagittal-Plane Knee Moment during Gait and Knee Cartilage Thickness. J. Athl. Train. 2017, 52, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Sonoo, M.; Iijima, H.; Kanemura, N. Altered sagittal plane kinematics and kinetics during sit-to-stand in individuals with knee osteoarthritis: A systematic review and meta-analysis. J. Biomech. 2019, 96, 109331. [Google Scholar] [CrossRef] [PubMed]
- Teng, H.-L.; MacLeod, T.D.; Link, T.M.; Majumdar, S.; Souza, R.B. Higher Knee Flexion Moment during the Second Half of the Stance Phase of Gait Is Associated With the Progression of Osteoarthritis of the Patellofemoral Joint on Magnetic Resonance Imaging. J. Orthop. Sports Phys. Ther. 2015, 45, 656–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tiku, M.L.; Sabaawy, H.E. Cartilage regeneration for treatment of osteoarthritis: A paradigm for nonsurgical intervention. Ther. Adv. Musculoskelet. Dis. 2015, 7, 76–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Add Moment | Vertical Force | ||||
|---|---|---|---|---|---|
| Young | Older | Young | Older | ||
| Knee joint kinetics | Adduction Moment | - | - | - | - |
| Adduction Moment (SD) | 0.552 ** | 0.795 ** | −0.389 * | −0.288 | |
| Knee Vertical Force | −0.405 * | −0.199 | - | - | |
| Knee Vertical Force (SD) | 0.346 * | −0.020 | 0.068 | −0.180 | |
| Foot motion | Foot Contact Angle | 0.223 | 0.511 * | −0.271 | −0.358 |
| Foot Contact Angle (SD) | −0.078 | 0.212 | .084 | −0.031 | |
| Toe-out Angle | −0.182 | 0.422 * | .097 | 0.007 | |
| Toe-out Angle (SD) | −0.064 | 0.292 | .071 | 0.162 | |
| COP Displacement | −0.047 | 0.250 | .064 | 0.052 | |
| COP Displacement (SD) | −0.110 | −0.003 | −0.212 | −0.194 | |
| Time to Foot Flat | −0.005 | −0.037 | 0.276 | 0.318 | |
| Time to Foot Flat (SD) | −0.184 | −0.002 | 0.269 | 0.295 | |
| Spatio-temporal parameters | Step Length | 0.113 | 0.258 | −0.445 ** | −0.703 ** |
| Step Length (SD) | −0.347 * | −0.082 | 0.045 | 0.052 | |
| Step Width | 0.174 | −0.426 * | −0.282 | 0.074 | |
| Step Width (SD) | −0.095 | −0.005 | 0.156 | 0.021 | |
| Double Support Time | 0.056 | 0.052 | 0.139 | 0.352 | |
| Double Support Time (SD) | −0.155 | 0.016 | 0.220 | −0.027 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagano, H.; Begg, R. Ageing-Related Gait Adaptations to Knee Joint Kinetics: Implications for the Development of Knee Osteoarthritis. Appl. Sci. 2020, 10, 8881. https://doi.org/10.3390/app10248881
Nagano H, Begg R. Ageing-Related Gait Adaptations to Knee Joint Kinetics: Implications for the Development of Knee Osteoarthritis. Applied Sciences. 2020; 10(24):8881. https://doi.org/10.3390/app10248881
Chicago/Turabian StyleNagano, Hanatsu, and Rezaul Begg. 2020. "Ageing-Related Gait Adaptations to Knee Joint Kinetics: Implications for the Development of Knee Osteoarthritis" Applied Sciences 10, no. 24: 8881. https://doi.org/10.3390/app10248881