
Tele-Rehabilitation Versus Local Rehabilitation Therapies Assisted by Robotic Devices: A Pilot Study with Patients

 ,
,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Neurorehabilitation System
2.3. Virtual Task
2.4. Setup and Protocol
- •
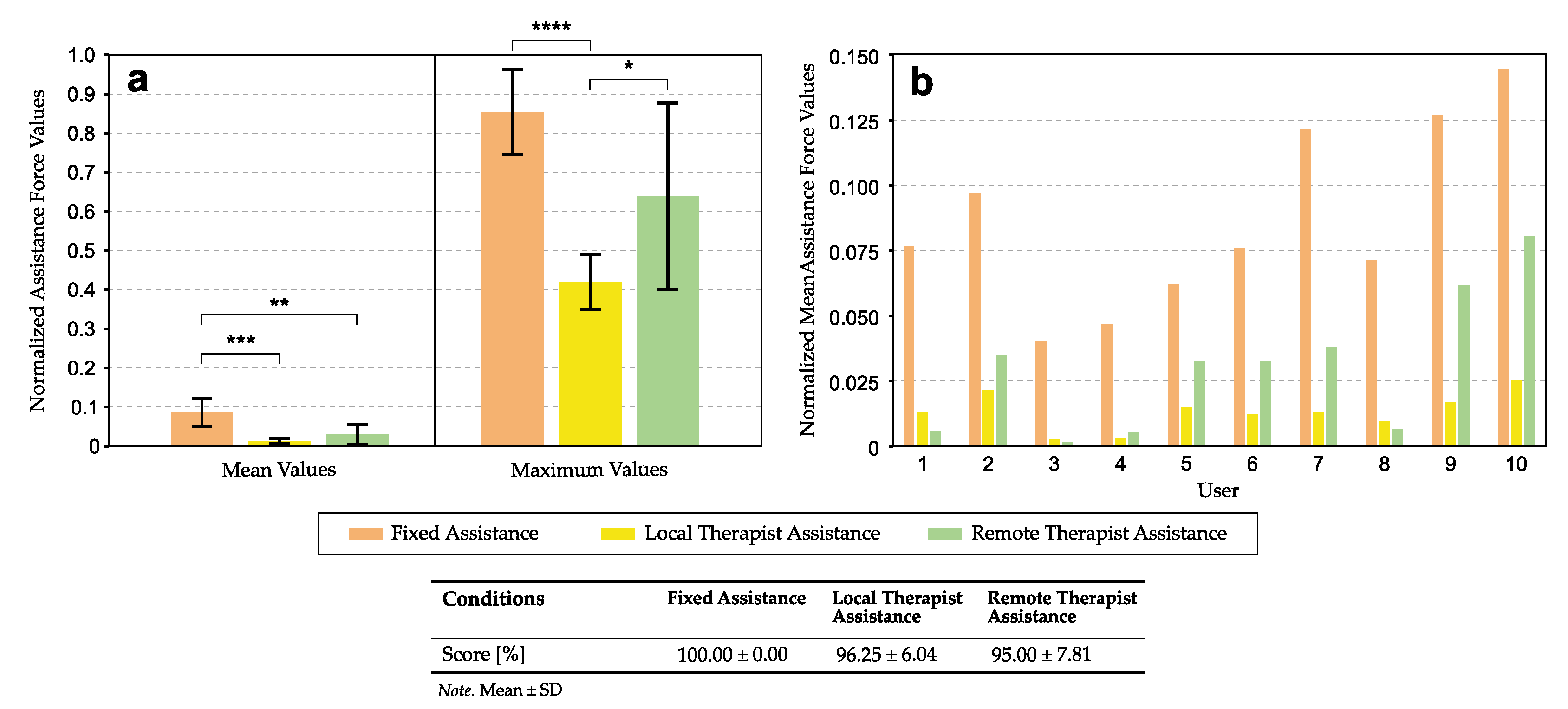
- Fixed Assistance. Fixed assistance level provided by the robot by the use of a force field.
- •
- Local Therapist Assistance. Assistance provided by the therapist.
- •
- Remote Therapist Assistance. Assistance provided by the therapist remotely (approach to a tele-rehabilitation environment).
2.5. Estimation of the Assistance Level
2.6. System Usability Scale
2.7. Subjective Assessment of Experience
2.8. Statistical Data Analysis
3. Results
3.1. Assistance Force
3.2. Intrinsic Motivation Inventory
3.3. Usability Assessment of the Assistance Modes
4. Discussion
4.1. Differences between Assistance Modes
4.2. Usability of the Assistance Modes
5. Conclusions
Symbols
| Angle formed by vectors F and | |
| d | Distance of the player cursor to the target |
| Parameter of the Greenhouse–Geisser correction method | |
| F | Current force applied by the robot |
| Assistance force vector | |
| Vector defined by trajectory towards the target | |
| r | Minimum distance to reach the target successfully |
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACM | Artery Cerebral Middle |
| ANOVA | Analysis of Variance |
| IM | Index Motor |
| IMI | Intrinsic Motivation Inventory |
| N/A | Not available value |
| ROM | Range Of Movement |
| STREAM | Stroke Rehabilitation Assessment of Movement |
| SUS | System Usability Scale |
References
- Peretti, A.; Amenta, F.; Tayebati, S.K.; Nittari, G.; Mahdi, S.S. Telerehabilitation: Review of the State-of-the-Art and Areas of Application. JMIR Rehabil. Assist. Technol. 2017, 4, e7. [Google Scholar] [CrossRef] [PubMed]
- Aprile, I.; Germanotta, M.; Cruciani, A.; Loreti, S.; Pecchioli, C.; Cecchi, F.; Montesano, A.; Galeri, S.; Diverio, M.; Falsini, C.; et al. Upper Limb Robotic Rehabilitation After Stroke: A Multicenter, Randomized Clinical Trial. J. Neurol. Phys. Ther. JNPT 2020, 44, 3–14. [Google Scholar] [CrossRef]
- Lo, K.; Stephenson, M.; Lockwood, C. Effectiveness of robotic assisted rehabilitation for mobility and functional ability in adult stroke patients: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2017, 15, 3049–3091. [Google Scholar] [CrossRef]
- Kim, J.; Sin, M.; Kim, W.S.; Min, Y.S.; Kim, W.; Park, D.; Paik, N.J.; Cho, K.; Park, H.S. Remote Assessment of Post-Stroke Elbow Function Using Internet-Based Telerobotics: A Proof-of-Concept Study. Front. Neurol. 2020, 11, 583101. [Google Scholar] [CrossRef]
- Zhang, S.; Fu, Q.; Guo, S.; Fu, Y. A Telepresence System for Therapist-in-the-Loop Training for Elbow Joint Rehabilitation. Appl. Sci. 2019, 9. [Google Scholar] [CrossRef] [Green Version]
- Sharifi, M.; Behzadipour, S.; Tavakoli, M. Cooperative modalities in robotic tele-rehabilitation using nonlinear bilateral impedance control. Control Eng. Pract. 2017, 67, 52–63. [Google Scholar] [CrossRef]
- Marchal-Crespo, L.; Reinkensmeyer, D. Review of control strategies for robotic movement training after neurologic injury. J. Neuro Eng. Rehabil. 2009, 6, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blank, A.A.; French, J.A.; Pehlivan, A.U.; O’Malley, M.K. Current trends in robot-assisted upper-limb stroke rehabilitation: Promoting patient engagement in therapy. Curr. Phys. Med. Rehabil. Rep. 2014, 2, 184–195. [Google Scholar] [CrossRef] [PubMed]
- Lledó, L.D.; Díez, J.A.; Bertomeu-Motos, A.; Ezquerro, S.; Badesa, F.J.; Sabater-Navarro, J.M.; García-Aracil, N. A Comparative Analysis of 2D and 3D Tasks for Virtual Reality Therapies Based on Robotic-Assisted Neurorehabilitation for Post-stroke Patients. Front. Aging Neurosci. 2016, 8, 205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohannon, R.W. Motricity index scores are valid indicators of paretic upper extremity strength following stroke. J. Phys. Ther. Sci. 1999, 11, 59–61. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, S.; Mayo, N.E.; Higgins, J.; Salbach, N.M.; Finch, L.; Wood-Dauphinee, S.L. The Stroke Rehabilitation Assessment of Movement (STREAM): A Comparison With Other Measures Used to Evaluate Effects of Stroke and Rehabilitation. Phys. Ther. 2003, 83, 617–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Díaz, I.; Catalan, J.M.; Badesa, F.J.; Justo, X.; Lledo, L.D.; Ugartemendia, A.; Gil, J.J.; Díez, J.; García-Aracil, N. Development of a robotic device for post-stroke home tele-rehabilitation. Adv. Mech. Eng. 2018, 10, 1687814017752302. [Google Scholar] [CrossRef] [Green Version]
- Catalan, J.M.; Garcia, J.V.; Lopez, D.; Ugartemendia, A.; Diaz, I.; Lledo, L.D.; Blanco, A.; Barios, J.; Bertomeu, A.; Garcia-Aracil, N. Evaluation of an Upper-Limb Rehabilitation Robotic Device for Home Use from Patient Perspective. In Converging Clinical and Engineering Research on Neurorehabilitation III; Masia, L., Micera, S., Akay, M., Pons, J.L., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 449–453. [Google Scholar] [CrossRef]
- iDRhA. Available online: https://idrha.es/ (accessed on 1 July 2021).
- da Silva, L.D.; Pereira, T.F.; Leithardt, V.R.; Seman, L.O.; Zeferino, C.A. Hybrid Impedance-Admittance Control for Upper Limb Exoskeleton using Electromyography. Appl. Sci. 2020, 10, 7146. [Google Scholar] [CrossRef]
- Brooke, J. Usability Evaluation in Industry. In Sus: A “Quick and Dirty” Usability; CRC Press: Boca Raton, FL, USA, 1996; Volume 189, pp. 1–252. [Google Scholar]
- Likert, R. A Method of Constructing an ATTITUDE Scale; Aldine Publishing: Chicago, IL, USA, 1974; pp. 233–243. [Google Scholar]
- Bangor, A.; Kortum, P.; Miller, J. Determining what individual SUS scores mean: Adding an adjective rating scale. J. Usability Stud. 2009, 4, 114–123. [Google Scholar]
- Bangor, A.; Kortum, P.T.; Miller, J.T. An empirical evaluation of the system usability scale. Intl. J. Hum. Comput. Interact. 2008, 24, 574–594. [Google Scholar] [CrossRef]
- Monardo, G.; Pavese, C.; Giorgi, I.; Godi, M.; Colombo, R. Evaluation of Patient Motivation and Satisfaction During Technology-Assisted Rehabilitation: An Experiential Review. Games Health J. 2021, 10, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Goršič, M.; Hlucny, S.D.; Novak, D. Effects of Different Opponent Types on Motivation and Exercise Intensity in a Competitive Arm Exercise Game. Games Health J. 2020, 9, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Goršič, M.; Cikajlo, I.; Goljar, N.; Novak, D. A multisession evaluation of an adaptive competitive arm rehabilitation game. J. Neuroeng. Rehabil. 2017, 14. [Google Scholar] [CrossRef] [PubMed]
- Goršič, M.; Cikajlo, I.; Novak, D. Competitive and cooperative arm rehabilitation games played by a patient and unimpaired person: Effects on motivation and exercise intensity. J. Neuroeng. Rehabil. 2017, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAuley, E.; Duncan, T.; Tammen, V.V. Psychometric properties of the Intrinsic Motivation Inventory in a competitive sport setting: A confirmatory factor analysis. Res. Q. Exerc. Sport 1989, 60, 48–58. [Google Scholar] [CrossRef]
- Darzi, A.; Novak, D. Using Physiological Linkage for Patient State Assessment In a Competitive Rehabilitation Game. In Proceedings of the 2019 IEEE 16th International Conference on Rehabilitation Robotics (ICORR), Toronto, ON, Canada, 24–28 June 2019; pp. 1031–1036. [Google Scholar] [CrossRef]
- Norouzi-Gheidari, N.; Levin, M.F.; Fung, J.; Archambault, P. Interactive virtual reality game-based rehabilitation for stroke patients. In Proceedings of the 2013 International Conference on Virtual Rehabilitation (ICVR), Philadelphia, PA, USA, 26–29 August 2013; pp. 220–221. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | Sex | Age (Years) | Diagnostic | Laterality | Demeurisse MI | STREAM |
|---|---|---|---|---|---|---|
| 1 | Male | 72 | Abdominal Dystension | Right | N/A | 10/16 |
| 2 | Male | 51 | Basal Ganglia hematoma | Right | 33.5 | 11/16 |
| 3 | Male | 70 | Bilateral SARS-CoV2 pneumonia | Left | N/A | N/A |
| 4 | Male | 78 | Ischemic stroke atherothrombotic | Right | 84.5 | 11/16 |
| 5 | Female | 84 | Ischemic stroke | Right | 17.5 | 7/16 |
| 6 | Male | 69 | Protuberance ischemic stroke | Left | 31.5 | 7/16 |
| 7 | Male | 69 | Thalamic capsule-lacunar stroke | Right | 15 | 0/16 |
| 8 | Male | 62 | Chronic ischemic heart disease | Right | 59 | 8/16 |
| 9 | Male | 54 | Ischemic stroke in ACM | Right | 17.5 | 0/16 |
| 10 | Male | 72 | Atherothrombotic stroke | Right | N/A | 9/16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Catalán, J.M.; García-Pérez, J.V.; Blanco, A.; Ezquerro, S.; Garrote, A.; Costa, T.; Bertomeu-Motos, A.; Díaz, I.; García-Aracil, N. Tele-Rehabilitation Versus Local Rehabilitation Therapies Assisted by Robotic Devices: A Pilot Study with Patients. Appl. Sci. 2021, 11, 6259. https://doi.org/10.3390/app11146259
Catalán JM, García-Pérez JV, Blanco A, Ezquerro S, Garrote A, Costa T, Bertomeu-Motos A, Díaz I, García-Aracil N. Tele-Rehabilitation Versus Local Rehabilitation Therapies Assisted by Robotic Devices: A Pilot Study with Patients. Applied Sciences. 2021; 11(14):6259. https://doi.org/10.3390/app11146259
Chicago/Turabian StyleCatalán, José M., José V. García-Pérez, Andrea Blanco, Santiago Ezquerro, Alicia Garrote, Teresa Costa, Arturo Bertomeu-Motos, Iñaki Díaz, and Nicolás García-Aracil. 2021. "Tele-Rehabilitation Versus Local Rehabilitation Therapies Assisted by Robotic Devices: A Pilot Study with Patients" Applied Sciences 11, no. 14: 6259. https://doi.org/10.3390/app11146259
APA StyleCatalán, J. M., García-Pérez, J. V., Blanco, A., Ezquerro, S., Garrote, A., Costa, T., Bertomeu-Motos, A., Díaz, I., & García-Aracil, N. (2021). Tele-Rehabilitation Versus Local Rehabilitation Therapies Assisted by Robotic Devices: A Pilot Study with Patients. Applied Sciences, 11(14), 6259. https://doi.org/10.3390/app11146259