
The Role of RANKL and Involvement of Cementum in Orthodontic Root Resorption


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Information Sources and Literature Search
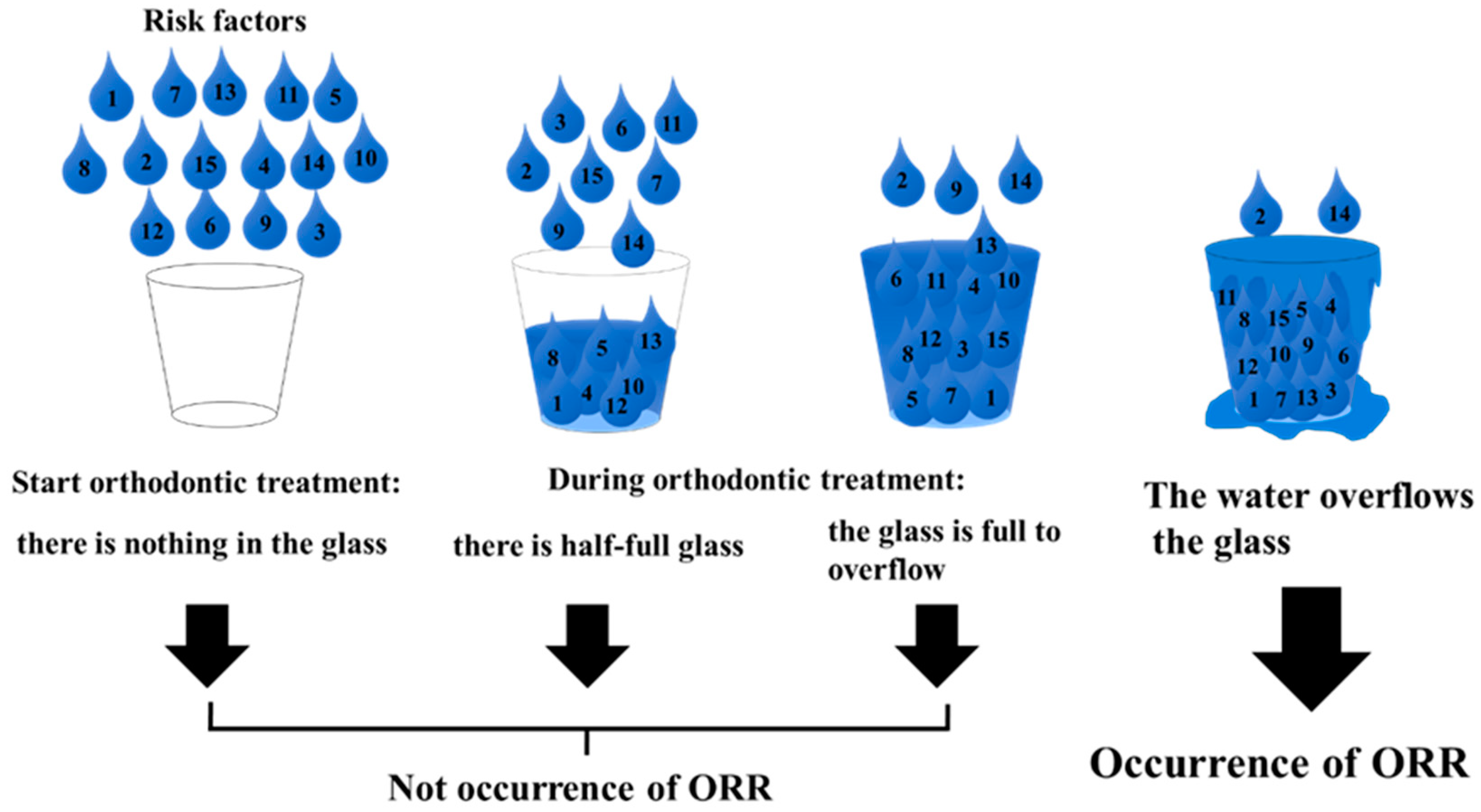
3. Risk Factors of Orthodontic Root Resorption (ORR)
4. The Receptor Activator of Nuclear Factor Kappa-B Ligand (RANKL) in Bone Resorption and Orthodontic Tooth Movement
5. RANKL Produced by PDL Cells and Cementoblasts in ORR
6. Repair of Resorbed Cementum by Cementoblasts
7. Involvement of Cementum in ORR
7.1. The Hardness of Cementum
7.2. The Difference of Chemical Composition of Cementum
8. Is Cementum the Last Bastion against ORR?
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Ottolengui, R. The physiological and pathological resorption of tooth roots. Drent. Items Interest 1914, 36, 322–362. [Google Scholar]
- Brezniak, N.; Wasserstein, A. Orthodontically induced inflammatory root resorption. Part II: The clinical aspects. Angle Orthod. 2002, 72, 180–184. [Google Scholar]
- Kaley, J.; Phillips, C. Factors related to root resorption in edgewise practice. Angle Orthod. 1991, 61, 125–132. [Google Scholar]
- Alhashimi, N.; Frithiof, L.; Brudvik, P.; Bakhiet, M. Orthodontic tooth movement and de novo synthesis of proinflammatory cytokines. Am. J. Orthod. Dentofac. Orthop. 2001, 119, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, M.; Yao-Umezawa, E.; Tanimoto, Y.; Shimizu, M.; Kikuta, J.; Hikida, T.; Takahashi-Hikida, M.; Horihata, S.; Suzuki, K.; Kasai, K. Individual Variations in the Hardness and Elastic Modulus of the Human Cementum. J. Hard Tissue Biol. 2016, 25, 345–350. [Google Scholar] [CrossRef] [Green Version]
- Yamaguchi, M.; Mishima, H. Hardness Variations and Chemical Compositional Changes in Human Cementum. J. Oral Tissue Eng. 2021, in press. [Google Scholar]
- Yao-Umezawa, E.; Yamaguchi, M.; Shimizu, M.; Kikuta, J.; Suzuki, K.; Kasai, K. Relationship between root resorption and individual variation in the calcium/phosphorous ratio of cementum. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 465–470. [Google Scholar] [CrossRef]
- Samandara, A.; Papageorgiou, S.N.; Ioannidou-Marathiotou, I.; Kavvadia-Tsatala, S.; Papadopoulos, M. Evaluation of orthodontically induced external root resorption following orthodontic treatment using cone beam computed tomography (CBCT): A systematic review and meta-analysis. Eur. J. Orthod. 2019, 41, 67–79. [Google Scholar] [CrossRef] [Green Version]
- Lacey, D.L.; Timms, E.; Tan, H.L.; Kelley, M.J.; Dunstan, C.R.; Burgess, T.; Elliott, R.; Colombero, A.; Elliott, G.; Scully, S.; et al. Osteoprotegerin ligand is a cytokine that regulates osteoclast differentiation and activation. Cell 1998, 93, 165–176. [Google Scholar] [CrossRef] [Green Version]
- Yasuda, H.; Shima, N.; Nakagawa, N.; Yamaguchi, K.; Kinosaki, M.; Mochizuki, S.-I.; Tomoyasu, A.; Yano, K.; Goto, M.; Murakami, A.; et al. Osteoclast differentiation factor is a ligand for osteoprotegerin/osteoclastogenesis-inhibitory factor and is identical to TRANCE/RANKL. Proc. Natl. Acad. Sci. USA 1998, 95, 3597–3602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haynes, D.R.; Atkins, G.J.; Loric, M.; Crotti, T.N.; Geary, S.M.; Findlay, D.M. Bidirectional signaling between stromal and hemopoietic cells regulates interleukin-1 expression during human osteoclast formation. Bone 1999, 25, 269–278. [Google Scholar] [CrossRef]
- Yasuda, H.; Shima, N.; Nakagawa, N.; Mochizuki, S.-I.; Yano, K.; Fujise, N.; Sato, Y.; Goto, M.; Yamaguchi, K.; Kuriyama, M.; et al. Identity of Osteoclastogenesis Inhibitory Factor (OCIF) and Osteoprotegerin (OPG): A Mechanism by which OPG/OCIF Inhibits Osteoclastogenesis in Vitro. Endocrinology 1998, 139, 1329–1337. [Google Scholar] [CrossRef]
- Bucay, N.; Sarosi, I.; Dunstan, C.R.; Morony, S.; Tarpley, J.; Capparelli, C.; Scully, S.; Tan, H.L.; Xu, W.; Lacey, D.L.; et al. osteoprotegerin-deficient mice develop early onset osteoporosis and arterial calcification. Genes Dev. 1998, 12, 1260–1268. [Google Scholar] [CrossRef]
- Kong, Y.-Y.; Yoshida, H.; Sarosi, I.; Tan, H.-L.; Timms, E.; Capparelli, C.; Morony, S.; Oliveira-Dos-Santos, A.J.; Van, G.; Itie, A.; et al. OPGL is a key regulator of osteoclastogenesis, lymphocyte development and lymph-node organogenesis. Nat. Cell Biol. 1999, 397, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, A.; Amizuka, N.; Irie, K.; Murakami, A.; Fujise, N.; Kanno, T.; Sato, Y.; Nakagawa, N.; Yasuda, H.; Mochizuki, S.; et al. Severe osteoporosis in mice lacking osteoclastogenesis inhibitory factor/osteoprotegerin. Biochem. Biophys. Res. Commun. 1998, 247, 610–615. [Google Scholar] [CrossRef] [PubMed]
- Kanzaki, H.; Chiba, M.; Shimizu, Y.; Mitani, H. Periodontal ligament cells under mechanical stress induce osteoclastogenesis by receptor activator of nuclear factor kappaB ligand up-regulation via prostaglandin E2 synthesis. J. Bone. Miner. Res. 2002, 17, 210–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishijima, Y.; Yamaguchi, M.; Kojima, T.; Aihara, N.; Nakajima, R.; Kasai, K. Levels of RANKL and OPG in gingival crevicular fluid during orthodontic tooth movement and effect of compression force on releases from periodontal ligament cells in vitro. Orthod. Craniofac. Res. 2006, 9, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, M.; Aihara, N.; Kojima, T.; Kasai, K. RANKL Increase in Compressed Periodontal Ligament Cells from Root Resorption. J. Dent. Res. 2006, 85, 751–756. [Google Scholar] [CrossRef]
- Aihara, N.; Otsuka, A.; Yamaguchi, M. Localization of RANKL and cathepsin K, B, and L in rat periodontal tissues during experimental tooth movement. Orthod. Waves 2005, 64, 107–113. [Google Scholar]
- Kanzaki, H.; Chiba, M.; Takahashi, I.; Haruyama, N.; Nishimura, M.; Mitani, H. Local OPG Gene Transfer to Periodontal Tissue Inhibits Orthodontic Tooth Movement. J. Dent. Res. 2004, 83, 920–925. [Google Scholar] [CrossRef]
- Kanzaki, H.; Chiba, M.; I Arai, K.; Takahashi, I.; Haruyama, N.; Nishimura, M.; Mitani, H. Local RANKL gene transfer to the periodontal tissue accelerates orthodontic tooth movement. Gene Ther. 2006, 13, 678–685. [Google Scholar] [CrossRef] [Green Version]
- Yamaguchi, M. RANK/RANKL/OPG during orthodontic tooth movement. Orthod. Craniofac. Res. 2009, 12, 113–119. [Google Scholar] [CrossRef]
- Long, P.; Liu, F.; Piesco, N.P.; Kapur, R.; Agarwal, S. Signaling by mechanical strain involves transcriptional regulation of proinflammatory genes in human periodontal ligament cells in vitro. Bone 2002, 30, 547–552. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, T.; Kita, M.; Kimura, I.; Oseko, F.; Terauchi, R.; Takahashi, K.; Kubo, T.; Kanamura, N. Mechanical stress induces expression of cytokines in human periodontal ligament cells. Oral Dis. 2006, 12, 171–175. [Google Scholar] [CrossRef]
- Kunii, R.; Yamaguchi, M.; Tanimoto, Y.; Asano, M.; Yamada, K.; Goseki, T.; Kasai, K. Role of interleukin-6 in orthodontically induced inflammatory root resorption in humans. Korean J. Orthod. 2013, 43, 294–301. [Google Scholar] [CrossRef] [Green Version]
- Tsukada, M.; Kikuta, J.; Shimizu, M.; Hikida, T.; Nakayama, E.; Iwane, T.; Kasai, K. TGF-β1 Induces Orthodontic Root Resorption through RANKL and IL-6 Production in hPDL Cells. Int. J. Oral-Med. Sci. 2021, 19, 278–287. [Google Scholar] [CrossRef]
- Fukushima, H.; Jimi, E.; Okamoto, F.; Motokawa, W.; Okabe, K. IL-1induced receptor activator of NF-kappa B ligand in human periodontal ligament cells involves ERK-dependent PGE2 production. Bone 2005, 36, 267–275. [Google Scholar] [CrossRef]
- Kikuta, J.; Yamaguchi, M.; Shimizu, M.; Yoshino, T.; Kasai, K. Notch Signaling Induces Root Resorption via RANKL and IL-6 from hPDL Cells. J. Dent. Res. 2014, 94, 140–147. [Google Scholar] [CrossRef]
- Mitsuhashi, M.; Yamaguchi, M.; Kojima, T.; Nakajima, R.; Kasai, K. Effects of HSP70 on the compression force-induced TNF-α and RANKL expression in human periodontal ligament cells. Inflamm. Res. 2011, 60, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Diercke, K.; Kohl, A.; Lux, C.J.; Erber, R. IL-1beta and compressive forces lead to a significant induction of RANKL-expression in primary human cementoblasts. J. Orofac. Orthop. 2012, 73, 397–412. [Google Scholar] [CrossRef]
- Minato, Y.; Yamaguchi, M.; Shimizu, M.; Kikuta, J.; Hikida, T.; Hikida, M.; Suemitsu, M.; Kuyama, K.; Kasai, K. Effect of caspases and RANKL induced by heavy force in orthodontic root resorption. Korean J. Orthod. 2018, 48, 253–261. [Google Scholar] [CrossRef]
- Iwane, T.; Kikuta, J. Notch Signaling Response to Heavy Compression Force Induces Orthodontic Root Resorption via RANKL and IL-6 from Cementoblasts. Int. J. Oral-Med. Sci. 2020, 18, 287–295. [Google Scholar] [CrossRef]
- Brudvik, P.; Rygh, P. Transition and determinants of orthodontic root resorption—Repair sequence. Eur. J. Orthod. 1995, 17, 177–188. [Google Scholar] [CrossRef]
- Brudvik, P.; Rygh, P. The repair of orthodontic root resorption: An ultrastructural study. Eur. J. Orthod. 1995, 17, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Sahara, N.; Toyoki, A.; Ashizawa, A.; Deguchi, T.; Suzuki, K. Cytodifferentiation of the odontoclast prior to the shedding of human deciduous teeth: An ultrastructural and cytochemical study. Anat. Rec. 1996, 244, 33–49. [Google Scholar] [CrossRef]
- Noxon, S.J.; King, G.J.; Gu, G.; Huang, G. Osteoclast clearance from periodontal tissues during orthodontic tooth movement. Am. J. Orthod. Dentofac. Orthop. 2001, 120, 466–476. [Google Scholar] [CrossRef]
- Jäger, A.; Kunert, D.; Friesen, T.; Zhang, D.; Lossdörfer, S.; Götz, W. Cellular and extracellular factors in early root resorption repair in the rat. Eur. J. Orthod. 2008, 30, 336–345. [Google Scholar] [CrossRef] [Green Version]
- Bosshardt, D.D.; Zalzal, S.; Mckee, M.D.; Nanci, A. Developmental appearance and distribution of bone sialoprotein and osteopontin in human and rat cementum. Anat. Rec. 1998, 250, 13–33. [Google Scholar] [CrossRef]
- Owman-Moll, P.; Kurol, J.; Lundgren, D. Repair of orthodontically induced root resorption in adolescents. Angle Orthod. 1995, 65, 403–410. [Google Scholar] [CrossRef]
- Bosshardt, D.D.; Schroeder, H.E. Cementogenesis reviewed: A comparison between human premolars and rodent molars. Anat. Rec. 1996, 245, 267–292. [Google Scholar] [CrossRef]
- Chan, E.; Darendeliler, M.A. Physical properties of root cementum: Part 5. Volumetric analysis of root resorption craters after application of light and heavy orthodontic forces. Am. J. Orthod. Dentofac. Orthop. 2005, 127, 186–195. [Google Scholar] [CrossRef]
- Chutimanutskul, W.; Darendeliler, M.A.; Swain, M.V.; Shen, G.; Petocz, P. Physical properties of human premolar cementum: Hardness and elasticity. Aust. Orthod. J. 2005, 21, 117–121. [Google Scholar]
- Malek, S.; Darendeliler, M.A.; Swain, M. Physical properties of root cementum: Part I. A new method for 3-dimensional evaluation. Am. J. Orthod. Dentofac. Orthop. 2001, 120, 198–208. [Google Scholar] [CrossRef] [PubMed]
- Darendeliler, M.A.; Kharbanda, O.P.; Chan, E.K.; Srivicharnkul, P.; Rex, T.; Swain, M.V.; Jones, A.S.; Petocz, P. Root resorption and its association with alterations in physical properties, mineral contents and resorption craters in human premolars fol-lowing application of light and heavy controlled orthodontic forces. Orthod. Craniofac. Res. 2004, 7, 79–97. [Google Scholar] [CrossRef]
- Rex, T.; Kharbanda, O.P.; Petocz, P.; Darendeliler, M.A. Physical properties of root cementum: Part Quantitative analysis of the mineral composition of human premolar cementum. Am. J. Orthod. Dentofac. Orthop. 2005, 127, 177–185. [Google Scholar] [CrossRef]
- Gasga, J.R.; Carbajal-De-La-Torre, G.; Bres, E.; Gil-Chavarria, I.M.; Rodríguez-Hernández, A.G.; García-García, R. STEM-HAADF electron microscopy analysis of the central dark line defect of human tooth enamel crystallites. J. Mater. Sci. Mater. Med. 2008, 19, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Schüpbach, P.; Oppenheim, F.G.; Lendenmann, U.; Lamkin, M.S.; Yao, Y.; Guggenheim, B. Electron-microscopic demonstration of proline-rich proteins, statherin, and histatins in acquired enamel pelliclesin vitro. Eur. J. Oral Sci. 2001, 109, 60–68. [Google Scholar] [CrossRef]
- Alvarez-Pérez, M.A.; Alvarez-Fregoso, O.; Ortiz-López, J.; Arzate, H. X-ray microanalysis of human cementum. Microsc. Microanal. 2005, 11, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Beck, B.W.; Harris, E.F. Apical root resorption in orthodontically treated subjects: Analysis of edgewise and light wire mechanics. Am. J. Orthod. Dentofac. Orthop. 1994, 105, 350–361. [Google Scholar] [CrossRef]
- Weiland, F. External root resorptions and orthodontic forces: Correlations and clinical consequences. Prog. Orthod. 2006, 7, 156–163. [Google Scholar]
- Owman-Moll, P.; Kurol, J.; Lundgren, D. The effects of a four-fold increased orthodontic force magnitude on tooth movement and root resorptions. An intraindividual study in adolescents. Eur. J. Orthod. 1996, 18, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Paetyangkul, A.; Türk, T.; Elekdag-Turk, S.; Jones, A.S.; Petocz, P.; Cheng, L.L.; Darendeliler, M.A. Physical properties of root cementum: Part 16. Comparisons of root resorption and resorption craters after the application of light and heavy continuous and controlled orthodontic forces for 4, 8, and 12 weeks. Am. J. Orthod. Dentofac. Orthop. 2011, 139, e279–e284. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamaguchi, M.; Mishima, H. The Role of RANKL and Involvement of Cementum in Orthodontic Root Resorption. Appl. Sci. 2021, 11, 7244. https://doi.org/10.3390/app11167244
Yamaguchi M, Mishima H. The Role of RANKL and Involvement of Cementum in Orthodontic Root Resorption. Applied Sciences. 2021; 11(16):7244. https://doi.org/10.3390/app11167244
Chicago/Turabian StyleYamaguchi, Masaru, and Hiroyuki Mishima. 2021. "The Role of RANKL and Involvement of Cementum in Orthodontic Root Resorption" Applied Sciences 11, no. 16: 7244. https://doi.org/10.3390/app11167244
APA StyleYamaguchi, M., & Mishima, H. (2021). The Role of RANKL and Involvement of Cementum in Orthodontic Root Resorption. Applied Sciences, 11(16), 7244. https://doi.org/10.3390/app11167244