
Falls Are the Leading Cause of Injuries among Farmers—Limitations of Practicing Judo in Preventing These Incidents


Abstract
:1. Introduction
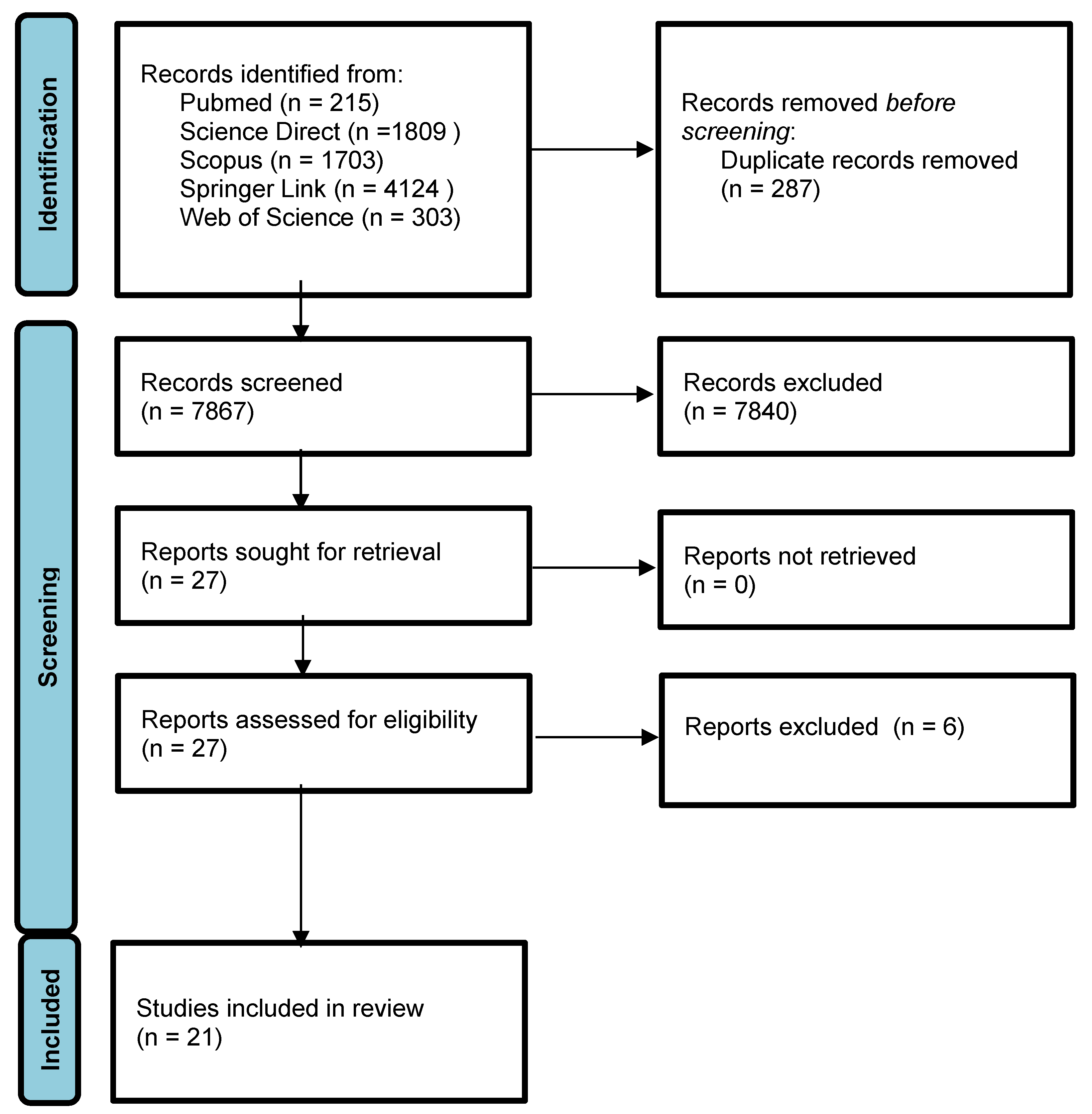
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Booth, F.W.; Chakravarthy, M.V.; Gordon, S.E.; Spangenburg, E.E. Waging war on physical inactivity: Using modern molecular ammunition against an ancient enemy. J. Appl. Physiol. 2002, 93, 3–30. [Google Scholar] [CrossRef] [Green Version]
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of Exercise Is a Major Cause of Chronic Diseases. Compr. Physiol. 2012, 2, 1143–1211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vina, J.; Sanchis-Gomar, F.; Martinez-Bello, V.; Gomez-Cabrera, M.C. Exercise acts as a drug; the pharmacological benefits of exercise. Br. J. Pharmacol. 2012, 167, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Nunan, D.; Mahtani, K.R.; Roberts, N.; Heneghan, C. Physical activity for the prevention and treatment of major chronic disease: An overview of systematic reviews. Syst. Rev. 2013, 2, 56. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. World Health Organization Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization. Guidelines on Physical Activity, Sedentary Behaviour and Sleep for Children under 5 Years of Age; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Bu, B.; Haijun, H.; Yong, L.; Chaohui, Z.; Xiaoyuan, Y.; Singh, M.F. Effects of martial arts on health status: A systematic review. J. Evid. Based Med. 2010, 3, 205–219. [Google Scholar] [CrossRef] [PubMed]
- Miyata, H.; Kobayashi, D.; Sonoda, A.; Motoike, H.; Akatsuka, S. Mindfulness and psychological health in practitioners of Japanese martial arts: A cross-sectional study. BMC Sports Sci. Med. Rehabil. 2020, 12, 75. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Skills for Health: Skills-Based Health Education Including Life Skills: An Important Component of A Child-Friendly/Health-Promoting School; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Xiang, H.; Wang, Z.; Stallones, L.; Keefe, T.J.; Huang, X.; Fu, X. Agricultural work-related injuries among farmers in Hubei, People’s Republic of China. Am. J. Public Health 2000, 90, 1269–1276. [Google Scholar] [CrossRef] [Green Version]
- Pickett, W.; Hartling, L.; Dimich-Ward, H.; Guernsey, J.R.; Hagel, L.; Voaklander, D.C.; Brison, R.J. Surveil-lance of hospitalized farm injuries in Canada. Inj. Prev. J. Int. Soc. Child Adolesc. Inj. Prev. 2001, 7, 123–128. [Google Scholar] [CrossRef] [Green Version]
- Solomon, C. Accidental injuries in agriculture in the UK. Occup. Med. 2002, 52, 461–466. [Google Scholar] [CrossRef] [Green Version]
- Little, D.C.; Vermillion, J.M.; Dikis, E.J.; Little, R.J.; Custer, M.D.; Cooney, D.R. Life on the Farm—Children at Risk. J. Pediatr. Surg. 2003, 38, 804–807. [Google Scholar] [CrossRef]
- McCurdy, S.A.; Farrar, J.A.; Beaumont, J.J.; Samuels, S.J.; Green, R.S.; Scott, L.C.; Schenker, M.B. Nonfatal occupational injury among California farm operators. J. Agric. Saf. Health 2004, 10, 103–119. [Google Scholar] [CrossRef]
- Moshiro, C.; Heuch, I.; Astrøm, A.N.; Setel, P.; Hemed, Y.; Kvåle, G. Injury morbidity in an urban and a rural area in Tanzania: An epidemiological survey. BMC Public Health 2005, 5, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nogalski, A.; Lübek, T.; Sompor, J.; Karski, J. Agriculture and forestry work-related injuries among farmers admitted to an Emergency Department. Ann. Agric. Environ. Med. 2007, 14, 253–258. [Google Scholar]
- Solomon, C.; Poole, J.; Palmer, K.T.; Coggon, D. Non-fatal occupational injuries in British agriculture. Occup. Environ. Med. 2007, 64, 150–154. [Google Scholar] [CrossRef] [Green Version]
- Sosnowska, S.; Kostka, T. Incidence and Nature of Farm-related Injuries among Children Aged 6–15 during a 10-year Period in One Region in Poland. Central Eur. J. Public Health 2007, 15, 33–37. [Google Scholar] [CrossRef] [Green Version]
- Taattola, K.; Rautiainen, R.H.; Karttunen, J.P.; Suutarinen, J.; Viluksela, M.K.; Louhelainen, K.; Mäittälä, J. Risk Factors for Occupational Injuries among Full-Time Farmers in Finland. J. Agric. Saf. Health 2012, 18, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Pfortmueller, C.A.; Kradolfer, D.; Kunz, M.; Lehmann, B.; Linder, G.; Exadaktylos, A.K. Injuries in agriculture—Injury severity and mortality. Swiss Med. Wkly. 2013, 143, w13846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paton, G.R.; Hagel, L.; Fourney, D.R. Hospitalized Head and Spine Injuries on Saskatchewan Farms. Can. J. Neurol. Sci./J. Can. Des. Sci. Neurol. 2014, 41, 436–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baksh, K.; Ganpat, W.; Narine, L. Occupational Health and Safety Issues among Vegetable Farmers in Trinidad and the Implications for Extension. J. Agric. Saf. Health 2015, 21, 159–171. [Google Scholar] [CrossRef]
- Missikpode, C.; Peek-Asa, C.; Young, T.; Swanton, A.; Leinenkugel, K.; Torner, J.C. Trends in non-fatal agricultural injuries requiring trauma care. Inj. Epidemiol. 2015, 2, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Momose, Y.; Suenaga, T. Gender differences in the occurrence of nonfatalagricultural injuries among farmers in Fukuoka, Japan. J. Rural. Med. 2015, 10, 57–64. [Google Scholar] [CrossRef] [Green Version]
- Cakabay, T.; Gokdogan, O.; Bezgin, S.; Kocyigit, M. Maxillofacial Traumas in Farmers Caused by Farm Animals, Agricultural Vehicles, and Materials. J. Craniofacial Surg. 2016, 27, e401–e406. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Lee, K.; Räsänen, K. Agricultural injuries in Korea and errors in systems of safety. Ann. Agric. Environ. Med. 2016, 23, 432–436. [Google Scholar] [CrossRef]
- Abdulkarim, A.; Carroll, P.; Coffey, P.; Sheehan, E. A retrospective review of farm injuries presenting to an Irish hospital emergency department in 2013. Ir. J. Med Sci. 2017, 186, 781–784. [Google Scholar] [CrossRef]
- Berney, M.J.; Horstmann, E.; Cassidy, N. Traumatic spinal injuries on farms: Patients treated in the national spinal unit of Ireland 2005–2015. J. Orthop. 2017, 14, 211–215. [Google Scholar] [CrossRef] [Green Version]
- Kaustell, K.O.; Mattila, T.E.A.; Ahvonen, A.; Rautiainen, R.H. Occupational injuries and diseases in fish farming in Finland 1996–2015. Int. Marit. Health 2019, 70, 47–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheehan, M.; Brent, L.; Deasy, C. Trauma on Farms in the Republic of Ireland. Injury 2020, 51, 2025–2032. [Google Scholar] [CrossRef]
- Kalina, R.M. The profile of Sense of Positive Health and Survival Abilities indices (subjective assessment) as a diagnostic tool used in health-related training. Arch. Budo 2012, 8, 179–190. [Google Scholar] [CrossRef] [Green Version]
- Kalina, R.M.; Kalina, A. Three methods of prophylaxis and therapy of innovative agonology, important from the perspective of personal safety. Arch. Budo Sci. Martial Art Extrem. Sport 2020, 16, 7–15. [Google Scholar]
- Budō. The Martial Ways of Japan; Nippon Budokan Foundation: Tokyo, Japan, 2009. [Google Scholar]
- Pocecco, E.; Ruedl, G.; Stankovic, N.; Sterkowicz, S.; Del Vecchio, F.B.; Gutierez-Garcia, C.; Rousseau, R.; Wolf, M.; Kopp, M.; Miarka, B.; et al. Injuries in judo: A systematic literature review including suggestions for prevention. Br. J. Sports Med. 2013, 47, 1139–1143. [Google Scholar] [CrossRef] [Green Version]
- Kamitani, T.; Nimura, Y.; Nagahiro, S.; Miyazaki, S.; Tomatsu, T. Catastrophic Head and Neck Injuries in Judo Players in Japan from 2003 to 2010. Am. J. Sports Med. 2013, 41, 1915–1921. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Arkkukangas, M.; Bååthe, K.S.; Ekholm, A.; Tonkonogi, M. Health promotion and prevention: The impact of specifically adapted judo-inspired training program on risk factors for falls among adults. Prev. Med. Rep. 2020, 19, 101126. [Google Scholar] [CrossRef]
- Arkkukangas, M.; Bååthe, K.S.; Ekholm, A.; Tonkonogi, M. A 10-week judo-based exercise programme improves physical functions such as balance, strength and falling techniques in working age adults. BMC Public Health 2021, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Dobosz, D.; Barczyński, B.J.; Kalina, A.; Kalina, R.M. The most effective and economic method of reducing death and disability associated with falls. Arch. Budo 2018, 14, 239–246. [Google Scholar]
- Jaskólski, E.; Nowacki, Z. Teoria, Metodyka i Systematyka Miękkiego Padania. Część, i. Teoria Miękkiego Padania; WSWF: Wrocław, Poland, 1972; pp. 83–88. (In Polish) [Google Scholar]
- Mroczkowski, A. Motor safety of a man during a fall. Arch. Budo 2015, 11, 293–303. [Google Scholar]
- Kalina, R.M.; Kruszewski, A.; Jagiełło, W.; Włoch, G. Combat Sports Propaedeutics—Basics of Judo; Wydawnictwo Akademii Wychowania Fizycznego: Warszawa, Poland, 2003. [Google Scholar]
- Kalina, R.M.; Kalina, A. Theoretical and methodological aspects of teaching lower extremity amputees safe falling. Adv. Rehab. 2003, 17, 71–87. [Google Scholar]
- Kalina, R.M. Language and methods of innovative agonology as a guide in interdisciplinary research on in-terpersonal relationships and people with the environment—From micro to macro scale. Arch. Budo 2020, 16, 271–280. [Google Scholar]
- Kalina, R.M.; Barczynski, B.J.; Jagiello, W.; Przezdziecki, B.; Kruszewski, A.; Harasymowicz, J.; Syska, J.; Szamotulska, K. Teaching of safe falling as most effective element of personal injury prevention in people regardless of gender, age and type of body build—The use of advanced information technologies to monitor the effects of education. Arch. Budo 2008, 4, 82–90. [Google Scholar]
- Gąsienica-Walczak, B.; Kalina, A. Susceptibility of body injuries during a fall of people after amputation or with abnormalities of lower limb. In Proceedings of the 1st World Congress on Health and Martial Arts in Interdisciplinary Approach, Czestochowa, Poland, 17–19 September 2015; Kalina, R.M., Ed.; Archives of Budo: Warsaw, Poland, 2015; pp. 193–195. [Google Scholar]
- Gąsienica-Walczak, B.; Barczyński, B.J.; Kalina, R.M. Evidence-based monitoring of the stimuli and effects of prophylaxis and kinesiotherapy based on the exercises of safe falling and avoiding collisions as a condition for optimising the prevention of body injuries in a universal sense—People with eye diseases as an example of an increased risk group. Arch. Budo 2018, 13, 79–95. [Google Scholar]
- Gąsienica-Walczak, B.; Barczyński, B.J.; Kalina, R.M. Fall as an extreme situation for obese people. Arch. Budo Sci. Martial Art Extrem. Sport 2019, 15, 93–104. [Google Scholar]
- Mosler, D. Changes of susceptibility of body injuries during a fall of patients with mental impairment participating for several months in special cognitive-behavioural therapy. In Proceedings of the 1st World Congress on Health and Martial Arts in Interdisciplinary Approach, Czestochowa, Poland, 17–19 September 2015; Kalina, R.M., Ed.; Archives of Budo: Warsaw, Poland, 2015; pp. 196–198. [Google Scholar]
- Jagiełło, W.; Kalina, R.M.; Klimczak, J.; Anaczenko, K.V.; Ashkinazi, S.; Kalina, A. Fun forms of martial arts in positive enhancement of all dimensions of health and survival abilities. In Proceedings of the 1st World Congress on Health and Martial Arts in Interdisciplinary Approach, Czestochowa, Poland, 17–19 September 2015; Kalina, R.M., Ed.; Archives of Budo: Warsaw, Poland, 2015; pp. 32–39. [Google Scholar]
- Kalina, R.M. Non-apparatus safe falls preparations test (N-ASFPT)—Validation procedure. Arch. Budo 2013, 4, 255–265. [Google Scholar]
- Klimczak, J.; Kalina, R.M.; Jagiełło, W. Fun forms of martial arts in diagnosing and reducing aggressiveness—Mental effects of a one-day course for Polish animators of sport. In Proceedings of the 1st World Congress on Health and Martial Arts in Interdisciplinary Approach, Czestochowa, Poland, 17–19 September 2015; Kalina, R.M., Ed.; Archives of Budo: Warsaw, Poland, 2015; pp. 32–39. [Google Scholar]
- Klimczak, J.; Kalina, R.M. Placebo effect—The perspective of diagnosis and therapy of aggressiveness by us-ing fun forms of martial arts during innovative agonology cognitive-behavioural sessions (case study). Arch. Budo 2019, 15, 57–66. [Google Scholar]
- Kalina, R.M. Cognitive and application barriers to the use of “agonology in preventive and therapeutic di-mension”. In Advances in Intelligent Systems and Computing; Salmon, P., Macquet, A.-C., Eds.; Springer: Berlin/Heidelberg, Germany, 2017; Volume 496, pp. 25–35. [Google Scholar]
- Kalina, R.M. Innovative agonology as a synonym for prophylactic and therapeutic agonology—The final impulse. Arch. Budo 2016, 12, 329–344. [Google Scholar]
- Walczak, B.G. Acceptance of the sense of implementing safe fall programs for people with visual impairments or after amputation of limbs—The perspective of modern adapted physical activity. Phys. Educ. Stud. 2019, 23, 288–296. [Google Scholar] [CrossRef] [Green Version]
- Falls Clinic FMH. Finchley Memorial Day Hospital: Information on falls. For patients and carers; Falls Clinic FMH: London, UK, 2005. [Google Scholar]
- Mosler, D.; Kalina, R.M. Possibilities and limitations of judo (selected martial arts) and innovative agonology in the therapy of people with mental disorders and also in widely understood public health prophylaxis. Arch. Budo 2017, 13, 211–226. [Google Scholar]

{kind=link}
| Year and Author/-s | Material | Study Design | Injured Body Parts (% of Cases) and Types of Injuries (% of Cases) + B:D | Estimated Falls Contribution (% of Causes) and Imortant Remarks (IR) |
|---|---|---|---|---|
| 2000 Xiang et al. [10] | Farmers from 14 villages Country: the People’s Republic of China | The interviewers with help from village leaders conducted face-to-face interviews with eligible individual farmers to collect data | Body parts: extremities (68.5%), multiple body parts (21.4%), trunk (5.8%), head (4.3%). Types of injuries: not specified | Falls were the second leading cause of injuries (26.1%) |
| 2001 Pickett et al. [11] | Data from the Canadian Agricultural Injury Surveillance Program (CAISP) concerning persons experiencing a farm injury requiring hospitalization, April 1991 to March 1995 | Descriptive analyses characterizing farm injuries by persons involved, mechanisms, primary diagnoses, and agents of injury. | Body parts. Machinery related farm injuries (results for particular age groups: 0–14, 15–59 and 60 + respectively): upper limb (29.8%, 34.1%, 27.3%), lower limb (22.2%, 20.3%, 16.7%), head (15%, 5.7%, 4.8%) trunk (8.6%, 11.1%, 18.9%). Non-machinery related farm injuries: upper limb (25.5%, 13.5%, 8.9%), head (22.2%, 11.7%, 9.3%), lower limb (13%, 17.6%, 22.7%), trunk (4%, 12.1%, 16.1%). Type of injuries. Machinery related: (results for particular age groups: 0–14, 15–59 and 60 + respectively): fracture: skull/spine trunk/upper and lower limb (44.1%, 40.7%, 40.7%), open wound: head/neck/trunk/upper and lower limb (22.4%, 26.3%, 22.1%), intracranial injury, excluding those with skull fracture (10.5%, 3.4%, 2.9%), contusion with intact skin surface (5.5%, 4.5%, 6.2%), crushing injury (4.7%, 5.3%, 3.8%), internal injury of chest, pelvis, and abdomen (3.3%, 2.7%, 3.9%), certain traumatic complications and unspecified injuries (3.1%, 4.7%, 5.5%), other (2.7%, 4.2%, 7.1%), superficial injury (1.6%, 0.7%, 0.5%), dislocation (0.8%, 2.3%, 2.1%), burns (0.6%, 1.6%, 0.6%), injury to nerves and spinal cord (0.6%, 0.7%, 0.9%), injury to blood vessels (0.2%, 0.3%, 0.3%), sprains/strains of joints and adjacent muscles (0, 2.8%, 3.4%), missing (0, 0, 0.1%). Non-machinery related: fracture: skull/spine trunk/upper and lower limb (39%, 36.9%, 42.5%), intracranial injury, excluding those with skull fracture (17.2%, 6.9%, 7.1%), other (12.9%, 14.4%, 14.2%), open wound: head/neck/trunk/upper and lower limb (10.8%, 10%, 5.5%), burns (6.4%, 3.9%, 3.6%), contusion with intact skin surface (4.1%, 6.2%, 7.4%), internal injury of chest, pelvis, and abdomen (2.8%, 3.1%, 3.1%), certain traumatic complications and unspecified injuries (2.6%, 4%, 4.1%), superficial injury (1.6%, 0.9%, 0.8%), dislocation (1%, 4.1%, 3.3%), sprains/strains of joints and adjacent muscles (0.9%, 7.9%, 7.6%), crushing injury (0.5%, 1%, 0.4%), injury to nerves and spinal cord (0.2%, 0.5%, 0.2%), injury to blood vessels (0, 0.3%, 0.2%), missing (0, 0.2%, 0.1%). | Fall was third and second leading cause of machinery (fall from machine) and non-machinery related injuries (15.1% and 24.5% respectively). |
| 2002 Solomon [12] | Reports submitted under the Reporting of Injuries, Diseases and Dangerous Occurrences Regulations and the Labour Force Survey Country: United Kingdom | Secondary data analysis | No data | Fall from heigh was second leading cause of fatal (15.8%) and fourth leading cause of non-fatal (13.1%) injuries Fall on the same level was third leading cause of non-fatal (15%) |
| 2003 Little et al. [13] | 94 children (under 18) identified with an agricultural-related injury Country: USA, Texas | The study included all farm-related accidents occurring between November 1994 and August 2001 (82 months) involving children 18 years or younger. This consecutive series of patients was accessed from the institutional trauma registry and reviewed retrospectively. | Body parts: Head (50%), upper extremity (35%), lower extremity (29%). Types of injuries: Dislocations/fractures (52%). | Falls were second leading cause of injuries (34% of causes) |
| 2004 McCurdy et al. [14] | Principal farm operators from California Country: USA | Operators participated in computer-assisted telephone interview survey | Body parts: trunk (38.8%), upper extremities (25%), lower extremities (21.3%), head (8.8%), multiple and system(4.4%), neck (1.9%). Types of injuries: sprains/strains (29.4%), open wound (11.8%), fractures (10.6%), contusions and superficial injuries (6.8%), dislocations (2.5%), Traumatic amputations-thumb/fingers (1.9%), foreign body in eye (3.1%). | Falls on the same level (5%), into hole (4.3%), from ladder/scaffold/stairs/steps (2.5%), from one level to the another (1.2%). These types of falls were jointly third leading cause of injuries (13%). |
| 2005 Moshiro et al. [15] | 303 persons reported to have been injured in rural area Country: Tanzania | A two stage cluster sampling method was adopted in selecting the rural sample. In the first stage, using existing AMMP data on mortality and poverty, 6 out of 51 villages were selected to represent different levels of injury. | Body parts: (39%) lower limb, (33%) spinal Types of injuries: fractures | Falls were second leading cause of injuries (27.4% of causes) |
| 2007 Nogalski et al. [16] | Data considering patients with agriculture and forestry related injuries admitted to Emergency Department. Country: Poland | Retrospective data analysis (descriptive and regression analysis) | Body parts: spine (10.8%), lower limbs (9.7%), upper limbs (7.8%), head (5.5%), face/neck (0.8%), thorax/abdomen (0.8%). Type of injuries: no data | Falls were third leading cause of injuries (18.9% of cases) |
| 2007 Solomon et al. [17] | Population of men who were residing in three defined rural areas of England and Wales. Country: United Kingdom | Each man was sent a postal questionnaire. Simple descriptive statistics were used to compare the relative frequency of different types of accidental injury in agricultural workers and other occupations | Body parts: no data Type of injuries: fracture (28.8%), back injury (25.6%), cut needing stitches (22.4%), other (15.3%), other sprain (10.2%), head injury (7.5%), eye injury (6%), burn or scald (2.6%), amputation (2.2%), unknown (1.5%). | Fall from high has the fourth highest frequency rate of accidents (3.4/1000 person-years) among agricultural employees and the highest frequency rate of accidents (5.3/1000 person-years) among self-employed agricultural workers. Slipping, tripping or falling has sixth highest frequency rate of accidents (3.1/1000 person-years) among agricultural employees and sixth highest frequency rate of accidents (2.2/1000 person-years) among self-employed agricultural workers. IR: Both agricultural employees and self-employed agricultural workers are more volnerable to fall from high than fall on the same level. |
| 2007 Sosnowska and Kostka [18] | Children aged 6–15 Country: Poland | The analysis has been made on the basis of information collected from the Farmers’ Insurance Fund | Body parts and type of injuries: Limbs (76.8%) including: fractures (30.7%), dislocations (26.7%), finger crushes (5.4%), fingers cutting-off (4.0%), wounds and gashes (9.8%); trunk harms (20.5%) including: collar-bone fractures, shoulder-blade fractures, burns, bites by animals, bruises; head injuries (2.7%). | Falls and slips (while lifting or carrying materials, equipment, tools) and falling from high altitudes (stairs/ladder/trailers/tractors/bicycles/carriages/trees, fencing, etc.) were first (47.2%); and second (22.9%) leading causes of injuries respectively. In general, falls were leading cause of injuries (70.1%). |
| 2012 Taattola et al. [19] | Self-employed full-time farmers Country: Finland | Telephone interviews were carried out by the computer-assisted telephone interview unit of the Finnish Institute of Occupational Health | No data | Falling or slipping was one of the most common types of incidents resulting in injuries |
| 2013 Pfortmueller et al. [20] | Out of 390,000, a total of 815 patients were eligible for the study Country: Switzerland | Our retrospective cohort study comprised adult (≥16 years) patients admitted to our emergency department (ED) between 1 January 2000 and 31 December 2011 in relation to an accident in agriculture | Body parts: Upper extremities (45.2%), head/neck (21.5%), lower extremities (18.9%), chest (13.6%), spine (11.2%), esternal (6.6%), abdomen (6%). Type of injuries: no data | Fall were second cause of injuries (30.1%) |
| 2014 Paton et al. [21] | Data from the Canadian Centre for Agricultural Health and Safety’s Saskatchewan Farm Injury Surveillance Database Country: Canada | The basic data was enhanced by a systematic review of the hospital charts. Regional health records personnel verified the information contained in the discharge records and added information about the injury events to standard de-identified abstraction forms. | Body parts: Head and spine including: lumbar spine (55.3%), thoracic (25%), cervical (14.9%), sacrum (2.6%). Type of injuries: head: concussions (36.2%), fractures (33.3%), intracranial injury of unspecified nature (24.9%),intracranial hemorrhages following injury (4.1%), cerebral lacerations and contusions (1.5%); spine: fractures of the vertebral column (87.7%), spinal cord (7.0%), vertebral dislocation without fracture and/or intervertebral disc rupture (5.3%) | Falls (including: falls from heights, animals, machinery and falls on the same level) were the immediate cause of 38.5% and 57% of all head and spine injuries respectively Contribution different types of fall resulting in spine injuries: fall from height (29%) or from animal (13%), fall from machine (12%); fall from same level (3%). |
| 2015 Baksh et al. [22] | Small-scale commercial-oriented vegetable farmers from ten of the most populated agricultural areas Country: Trinidad | Survey was conducted. This study employed a convenience sampling strategy to recruit its participants. The first farmer met was interviewed, followed by every third farmer working in the field at the time of data collection until ten farmers were successfully interviewed. | no data | The 33% of farmers reported experiencing fall while working within the last year. |
| 2015 Missikpode et al. [23] | 2005 63 persons 2006 86 persons 2007 94 persons 2008 147 persons 2009 174 persons 2010 149 persons 2011 159 persons 2012 176 persons 2013 176 persons Country: USA, Iowa | Using Iowa Trauma Registry data collected by the Iowa Department of Public Health, we examined trends in non-fatal agricultural injuries reported by acute care hospitals accredited as Level I, II, and III Trauma Care Facilities from 2005 to 2013. | Type of injuries and body parts: 2005 fracture (43.3%), head injury (20%), dislocation/sprain (No data) 2006 fracture (41.8%), head injury (8.8%), dislocation/sprain (No data) 2007 fracture (29.2%), head injury (18.0%), dislocation/sprain (6.7%) 2008 fracture (39.0%), head injury (13.0%), dislocation/sprain (5.5%) 2009 fracture (40.5%), head injury (12.4%), dislocation/sprain (7.2%) 2010 fracture (47.6%), head injury (9.0%), dislocation/sprain (4.1%) 2011 fracture (41.4%), head injury (14.7%), dislocation/sprain (5.7%) 2012 fracture (44.3%), head injury (18.0%), dislocation/sprain (3.6%) 2013 fracture (47.4%), head injury (11.0%), dislocation/sprain (8.1%) | 2005 Fall were second cause of injuries (24.6%) 2006 Fall were second cause of injuries (18.3%) 2007 Fall were second cause of injuries (20.5%) 2008 Fall were second cause of injuries (21.4%) 2009 Fall were second cause of injuries (24.1%) 2010 Fall were second cause of injuries (18.5%) 2011 Fall were first cause of injuries (24.4%) 2012 Fall were first cause of injuries (20.5%) 2013 Fall were second cause of injuries (15.9%) |
| 2015 Momose and Suenaga [24] | Information concerning farmers’ compensation injury claims Country: Japan | Secondary data analysis: agricultural injuries were identified using the International Classification of External Causes of Injury). The Statistical Analysis | Body parts Men (results for populations 20–64 and 65–89 respectively): hand/wrist (25.3% and 21.5%), lower extremity (19.1% and 17.3%), ankle/toe (11.2% and 10.4%), shoulder/chest (10.4% and 15.1%), head/face (9.4% and 10.1%), lumbar region (7.8% and 10.7%), upper extremity (9.9% and 9%), others (6.8% and 5.9%) Women (results for populations 20–64 and 65–89 respectively): hand/wrist (26.5% and 20.3%), lower extremity (21.2% and 24.4%), upper extremity (12.2% and 12.7%), ankle/toe (12.2% and 8.6%), head/face (11.1% and 4.9%), shoulder/chest (8.5% and 10.3%), lumbar region (4.2% and 14.2%), others (4.2% and 4.5%) Types of injuries: Men (results for populations 20–64 and 65–89 respectively): others (28.7% and 23%), fracture (23.5% and 28.1%), cut wound (17% and 12.6%), bruises (11.8% and 14.5%), contusions (11% and 15.9%), sprain (8.1% and 5.8%), women (results for populations 20–64 and 65–89 respectively): others (24.3% and 16.6%), fracture (32.8% and 44.8%), bruises (12.2% and 14.2%), cut wound (11.1% and 8.2%), contusions (11.6% and 9.7%), sprain (7.9% and 6.6%) | Given nonfatal agricultural injuries, related to machinery fall/slip caused (population age: 20–64): 6.1% (men) and 5.9% (women) of injuries; fall from the machine: 7.6% (men) and 5.9% (women). Population age 65–89: fall/slip—10.4% (men) and 22% (woman); fall from the machine 6.8% (men) and 7.3% (woman). IR: Population aged 65–89 is more vulnurable to fall/slip and fall from the machine (only women) than population aged 20–64. |
| 2016 Cakabay et al. [25] | Data considering the farmers who have come to emergency service unit as a result of maxillofacial trauma between 2010 and 2012. Country: Turkey | Demographic findings, trauma etiologies, seasonal variables of trauma, and maxillofacial fracture area distribution have been analyzed | Body parts: head Type of injuries: Skull and frontal bone, nasoethmoid complex, nasal fractures, orbital floor, mandibula fracture, zygoma fractures, maxilla fracture. | Falling from haystacks and falling from motorized and nonmotorized agricultural vehicles and tools have fourth (9.59%) and fifth (7.53%) position in ranking of 6 (predermined) etiological categories. IR: In general (both types are combined) fall has second position (17.12%). |
| 2016 Kim H et al. [26] | 277 injury cases were identified, of which 68 were contacted Country: Korea | Subjects for this study were chosen from the injury insurance claim database of the Mutual Aid Insurance of the Nation Agricultural Cooperation Federation (NACF) of Korea | No data | Fall were first cause of injuries (27.9%) |
| 2017 Abdulkarim et al. [27] | 144 agricultural-related injuries Country: Ireland | Every presentation to the Accident and Emergency Department at the Midlands Regional Hospital from the 1.01.2013 to 31.12.2013 was assessed retrospectively to determine if an injury had been sustained in an agricultural environment | Body parts: upper limb, lowe limb, trunk, spine Type of injuries: fractures, dislocation | Falls more than 3 feet were third leading cause of injuries (10% of causes) |
| 2017 Berney et l. [28] | 31 patients who suffered traumatic spinal injuries on farms Country: Ireland | Retrospective study. Patients who suffered traumatic spinal injuries on farms and underwent treatment were identified using the Hospital In-Patient Enquiry (HIPE) system. | Body parts: spinal cord injuries Type of injuries: Concerning spinal injuries alone, 81% suffered fractures at a single level and 6 patients (19%) had non-contiguous spinal injuries including one patient with injuries at 3 sites in the spine | Fall were fourth leading cause of injuries (16% of cases) |
| 2019 Kaustell et al. [29] | Data concerning injuries and occupational diseases to people working on Finnish fish farms acquired from the Finnish Workers’ Compensation Centre Country: Finland | Secondary data analysis | Body parts: Hand/finger (24.9%), leg from hip to ankle (19.2%), arm from shoulder to wrist (16.2%), back/spine (9.5%), eye (8.2%), head excluding eyes (6.7%), foot and toes (5.6%), other, e.g., internal organ injury (4.1%), neck and body excluding back (3.6%), multiple body parts (2.1%) Type of injuries: Dislocations, sprains and strains (35%) wounds and superficial injuries (29.4%), concussion and internal injuries (17.6%), bone fractures (9.0%), other (e.g., poisoning, suffocation) (4.3%), not known (2%), burns, scalds and frostbites (1.8%), traumatic amputations (0.8%) | Slipping, stumbling, and falling were the leading cause of injuries (36.5% of them) IR: Given contact modes of injuries, horizontal or vertical impact (the victim is in motion) and struck by/collision with object in motion caused 36.8% and 10.4% of injuries, respectively. |
| 2020 Sheehan et al. [30] | 430 patients where the incident location was farm Country: Ireland | Data were gathered from the National Office of Clinical Audit Major Trauma Audit (MTA) 2014 to 2016. Patients were included and excluded based on Trauma Audit and Research Network(TARN) inclusion criteria. | Body parts: The most common body area injured was limbs, followed by chest, spine and head injuries Type of injuries: fractures, dislocation | Falls less than 2 m were second leading cause of injuries (26.7% of causes) Falls more than 2 m were third leading cause of injuries (25.6% of causes) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blach, W.; Dobosz, D.; Gasienica-Walczak, B.; Grants, J.; Litwiniuk, A. Falls Are the Leading Cause of Injuries among Farmers—Limitations of Practicing Judo in Preventing These Incidents. Appl. Sci. 2021, 11, 7324. https://doi.org/10.3390/app11167324
Blach W, Dobosz D, Gasienica-Walczak B, Grants J, Litwiniuk A. Falls Are the Leading Cause of Injuries among Farmers—Limitations of Practicing Judo in Preventing These Incidents. Applied Sciences. 2021; 11(16):7324. https://doi.org/10.3390/app11167324
Chicago/Turabian StyleBlach, Wieslaw, Dawid Dobosz, Bartlomiej Gasienica-Walczak, Juris Grants, and Artur Litwiniuk. 2021. "Falls Are the Leading Cause of Injuries among Farmers—Limitations of Practicing Judo in Preventing These Incidents" Applied Sciences 11, no. 16: 7324. https://doi.org/10.3390/app11167324