
Emerging Oncogenic Viruses in Head and Neck Cancers from Romanian Patients

 ,
,  ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Samples
2.2. DNA Extraction
2.3. Detection of Viral DNA
2.4. Statistical Analysis
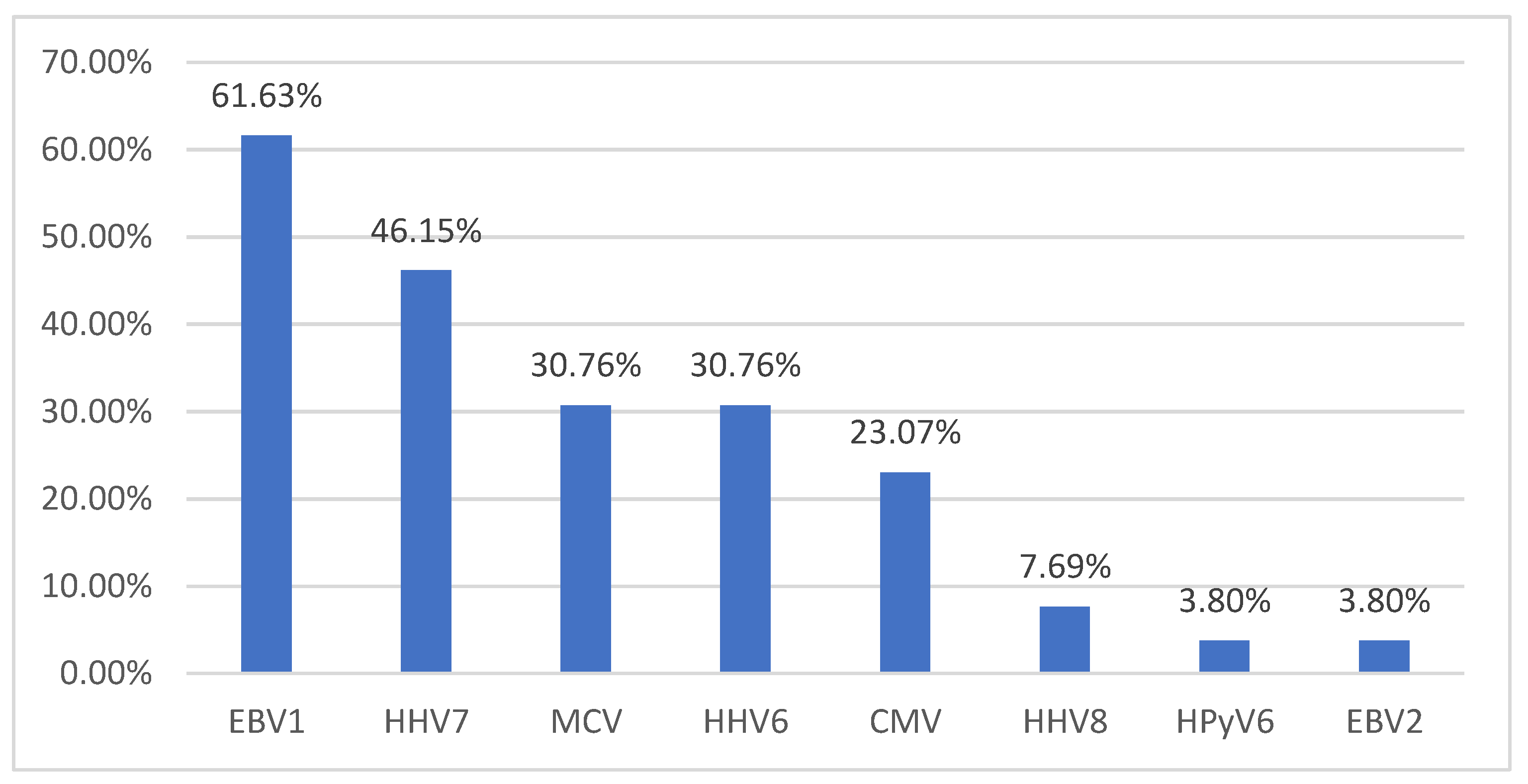
3. Results
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Europe Beating Cancer Plan. Joint Research Center. 2020. Available online: https://ec.europa.eu/info/law/better-regulation/have-your-say/initiatives/12154-Europe%E2%80%99s-Beating-Cancer-Plan_en (accessed on 21 August 2021).
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. 2020. Available online: https://gco.iarc.fr/today (accessed on 21 August 2021).
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2018, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Agency for Research on Cancer. A Review of Human Carcinogens: Biological Agents. IARC Monographs of the Evaluation of Carcinogenic Risks to Humans; IARC: Lyon, France, 2012. [Google Scholar]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Malaria and Some Polyomaviruses (SV40, BK, JC, and Merkel Cell Viruses). IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; IARC: Lyon, France, 2014. [Google Scholar]
- Poluschkin, L.; Rautava, J.; Turunen, A.; Wang, Y.; Hedman, K.; Syrjänen, K.; Grenman, R.; Syrjänen, S. Polyomaviruses detectable in head and neck carcinomas. Oncotarget 2018, 9, 22642–22652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, A.A.; Gheit, T.; Stellin, M.; Lupato, V.; Spinato, G.; Fuson, R.; Menegaldo, A.; Mckay-Chopin, S.; Cin, E.D.; Tirelli, G. Oncogenic DNA viruses found in salivary gland tumors. Oral Oncol. 2017, 75, 106–110. [Google Scholar] [CrossRef] [PubMed]
- Haeggblom, L.; Ursu, R.G.; Mirzaie, L.; Attoff, T.; Gahm, C.; Nordenvall, L.H.; Nasman, A. No evidence for human papillomavirus having a causal role in salivary gland tumors. Diagn. Pathol. 2018, 13, 44. [Google Scholar] [CrossRef] [Green Version]
- Ramqvist, T.; Ursu, R.G.; Haeggblom, L.; Mirzaie, L.; Gahm, C.; Hammarstedt-Nordenvall, L.; Dalianis, T.; Nasman, A. Human polyomaviruses are not frequently present in cancer of the salivary glands. Anticancer. Res. 2018, 38, 2871–2874. [Google Scholar] [CrossRef]
- Tan, R.; Phua, S.K.A.; Soong, Y.L.; Oon, L.L.E.; Chan, K.S.; Lucky, S.S.; Mong, J.; Tan, M.H.; Lim, C.M. Clinical utility of Epstein-Barr virus DNA and other liquid biopsy markers in nasopharyngeal carcinoma. Cancer Commun. 2020, 40, 564–585. [Google Scholar] [CrossRef]
- Carlander, A.F.; Jakobsen, K.K.; Bendtsen, S.K.; Garset-Zamani, M.; Lynggaard, C.D.; Jensen, J.S.; Grønhøj, C.; Buchwald, C. A contemporary systematic review on repartition of HPV-positivity in oropharyngeal cancer worldwide. Viruses 2021, 13, 1326. [Google Scholar] [CrossRef]
- Klufah, F.; Mobaraki, G.; Liu, D.; Alharbi, R.A.; Kurz, A.K.; Speel, E.J.M.; Winnepenninckx, V.; Zur Hausen, A. Emerging role of human polyomaviruses 6 and 7 in Human Cancers. Infect. Agents Cancer 2021, 16, 1–12. [Google Scholar] [CrossRef]
- Zhao, Y.; Amorrortu, R.P.; Fenske, N.A.; Cherpelis, B.; Messina, J.L.; Sondak, V.K.; Giuliano, A.R.; Schell, M.J.; Waterboer, T.; Pawlita, M. Cutaneous viral infections associated with ultraviolet radiation exposure. Int. J. Cancer 2021, 148, 448–458. [Google Scholar] [CrossRef]
- Ursu, R.G.; Ivanov, I.; Popescu, E.; Costan, V.; Stamatin, O.; Ghetu, N.; Palade, D.; MIRTU, C.; Andrese, E.; Danciu, M. Human papilloma virus genotyping in fresh head and neck tumors-our first experience. Med. Surg. J. 2015, 119, 676–680. [Google Scholar]
- Ursu, R.G.; Onofriescu, M.; Luca, A.; Prisecariu, L.J.; Salceanu, S.O.; Nemescu, D.; Iancu, L.S. The need for cervical cancer control in HIV-positive and HIV-negative women from romania by primary prevention and by early detection using clinically validated HPV/DNA tests. PLoS ONE 2015, 10, e0132271. [Google Scholar] [CrossRef]
- Popovici, O.; Ursu, R.G.; Azoicai, D.; Iancu, L.S. HBV genotypes circulation in pregnant women in Romania: A pilot study. Rev. Romana Med. Lab. 2020, 28, 91–98. [Google Scholar] [CrossRef] [Green Version]
- Schmitt, M.; Dondog, B.; Waterboer, T.; Pawlita, M.; Tommasino, M.; Gheit, T. Abundance of multiple high-risk human papillomavirus (HPV) infections found in cervical cells analyzed by use of an ultrasensitive HPV genotyping assay. J. Clin. Microbiol. 2010, 48, 143–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gheit, T.; Billoud, G.; de Koning, M.N.; Gemignani, F.; Forslund, O.; Sylla, B.S.; Vaccarella, S.; Franceschi, S.; Landi, S.; Quint, W.G. Development of a sensitive and specific multiplex PCR method combined with DNA microarray primer extension to detect Betapapillomavirus types. J. Clin. Microbiol. 2007, 45, 2537–2544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gheit, T.; Landi, S.; Gemignani, F.; Snijders, P.J.; Vaccarella, S.; Franceschi, S.; Canzian, F.; Tommasino, M. Development of a sensitive and specific assay combining multiplex PCR and DNA microarray primer extension to detect high-risk mucosal human papillomavirus types. J. Clin. Microbiol. 2006, 44, 2025–2031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmitt, M.; Bravo, I.G.; Snijders, P.J.; Gissmann, L.; Pawlita, M.; Waterboer, T. Bead-based multiplex genotyping of human Papillomaviruses. J. Clin. Microbiol. 2006, 44, 504–512. [Google Scholar] [CrossRef] [Green Version]
- Corbex, M.; Bouzbid, S.; Traverse-Glehen, A.; Aouras, H.; McKay-Chopin, S.; Carreira, C.; Lankar, A.; Tommasino, M.; Gheit, T. Prevalence of papillomaviruses, polyomaviruses, and herpesviruses in triple-negative and inflammatory breast tumors from algeria compared with other types of breast cancer tumors. PLoS ONE 2014, 9, e114559. [Google Scholar] [CrossRef] [Green Version]
- Lee, L.A.; Fang, T.J.; Li, H.Y.; Chuang, H.H.; Kang, C.J.; Chang, K.P.; Liao, C.T.; Chen, T.C.; Huang, C.G.; Yen, T.C. Effects of Epstein-Barr virus infection on the risk and prognosis of primary laryngeal squamous cell carcinoma: A hospital-based case-control study in Taiwan. Cancers 2021, 13, 1741. [Google Scholar] [CrossRef]
- Deng, Z.; Uehara, T.; Maeda, H.; Hasegawa, M.; Matayoshi, S.; Kiyuna, A.; Agena, S.; Pan, X.; Zhang, C.; Yamashita, Y.; et al. Epstein-Barr virus and human papillomavirus infections and genotype distribution in head and neck cancers. PLoS ONE 2014, 9, e113702. [Google Scholar] [CrossRef]
- Niya, M.H.K.; Tameshkel, F.S.; Keyvani, H.; Esghaei, M.; Panahi, M.; Zamani, F.; Tabibzadeh, A. Epstein-Barr virus molecular epidemiology and variants identification in head and neck squamous cell carcinoma. Eur. J. Cancer Prev. 2020, 29, 523–530. [Google Scholar] [CrossRef]
- Zhou, X.; Cao, S.M.; Cai, Y.L.; Zhang, X.; Zhang, S.; Feng, G.F.; Chen, Y.; Feng, Q.S.; Chen, Y.; Chang, E.T.; et al. A comprehensive risk score for effective risk stratification and screening of nasopharyngeal carcinoma. Nat. Commun. 2021, 12, 5189. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, J.S.; Forslund, O.; Andersson, F.C.; Lindstedt, M.; Greiff, L. Intralesional EBV-DNA load as marker of prognosis for nasopharyngeal cancer. Sci. Rep. 2019, 9, 15432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, S.; Kong, T.; Berthelet, E.; Ng, T.; Prisman, E. A Unique Case of Primary EBV-Positive, HPV-Negative Nasopharyngeal Carcinoma Located in the Tonsil. Head Neck Pathol. 2021, 15, 1017–1022. [Google Scholar] [CrossRef] [PubMed]
- Agaimy, A.; Mueller, S.K.; Harrer, T.; Bauer, S.; Thompson, L.D.R. Head and neck Kaposi sarcoma: Clinicopathological analysis of 11 cases. Head Neck Pathol. 2018, 12, 511–516. [Google Scholar] [CrossRef] [PubMed]
- Sikora, A.G.; Shnayder, Y.; Yee, H.; DeLacure, M.D. Oropharyngeal kaposi sarcoma in related persons negative for human immunodeficiency virus. Ann. Otol. Rhinol. Laryngol. 2008, 117, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Soon, G.S.T.; Petersson, F.; Thong, M.K.T.; Tan, C.L. Primary nasopharyngeal Kaposi sarcoma as index diagnosis of AIDS in a previously healthy man. Head Neck Pathol. 2018, 13, 664–667. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, M.; Martins, V.A.O.; Sumita, L.M.; Tozetto-Mendoza, T.R.; Romano, B.B.; Machado, C.M.; Pannuti, C.S.; Brandão, T.B.; Ribeiro, A.C.P.; Corrêa, L.; et al. Oral shedding of human herpesviruses in patients undergoing radiotherapy/chemotherapy treatment for head and neck squamous cell carcinoma. Clin. Oral Investig. 2017, 21, 2291–2301. [Google Scholar] [CrossRef]
- Formánek, M.; Formánková, D.; Hurník, P.; Vrtková, A.; Komínek, P. Epstein-Barr virus may contribute to the pathogenesis of adult-onset recurrent respiratory papillomatosis: A preliminary study. Clin. Otolaryngol. 2021, 46, 373–379. [Google Scholar] [CrossRef]
- Kiprian, D.; Czarkowska-Paczek, B.; Wyczalkowska-Tomasik, A.; Paczek, L. Human cytomegalovirus and Epstein-Barr virus infections increase the risk of death in patients with head and neck cancers receiving radiotherapy or radiochemotherapy. Medicine 2018, 97, e13777. [Google Scholar] [CrossRef]
- Radunovic, M.; Tomanovic, N.; Novakovic, I.; Boricic, I.; Milenkovic, S.; Dimitrijevic, M.; Radojevic-Skodric, S.; Bogdanovic, L.; Basta-Jovanovic, G. Cytomegalovirus induces Interleukin-6 mediated inflammatory response in salivary gland cancer. J. BUON 2016, 21, 1530–1536. [Google Scholar]
- Gangemi, A.C.; Choi, S.H.; Yin, Z.; Feurdean, M. Cytomegalovirus and herpes simplex virus co-infection in an HIV-negative patient: A case report. Cureus 2021, 13, 13214. [Google Scholar] [CrossRef]
- Mulder, F.J.; Klufah, F.; Janssen, F.M.E.; Farshadpour, F.; Willems, S.M.; De Bree, R.; Zur Hausen, A.; Van den Hout, M.F.C.M.; Kremer, B.; Speel, E.M. Presence of human papillomavirus and Epstein-Barr virus, but absence of Merkel cell polyomavirus, in head and neck cancer of non-smokers and non-drinkers. Front. Oncol. 2021, 10, 560434. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, J.P.; Blanco, R.; Osorio, J.C.; Oliva, C.; Diaz, M.J.; Carrillo-Beltrán, D.; Aguayo, R.; Castillo, A.; Tapia, J.C.; Calaf, G.M.; et al. Merkel cell polyomavirus detected in head and neck carcinomas from Chile. Infect. Agent. Cancer 2020, 15, 4–5. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, A.; Xu, M.; Silén, S.; Wang, Y.; Fu, Y.; Sadeghi, M.; Toppinen, M.; Carpén, T.; Hedman, K.; Mäkitie, A.; et al. Newly detected DNA viruses in juvenile nasopharyngeal angiofibroma (JNA) and oral and oropharyngeal squamous cell carcinoma (OSCC/OPSCC). Eur. Arch. Otorhinolaryngol. 2019, 276, 613–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herberhold, S.; Hellmich, M.; Panning, M.; Bartok, E.; Silling, S.; Akgül, B.; Wieland, U. Human polyomavirus and human papillomavirus prevalence and viral load in non-malignant tonsillar tissue and tonsillar carcinoma. Med. Microbiol. Immunol. 2017, 206, 93–103. [Google Scholar] [CrossRef]
- Saláková, M.; Košlabová, E.; Vojtěchová, Z.; Tachezy, R.; Šroller, V. Detection of human polyomaviruses MCPyV, HPyV6, and HPyV7 in malignant and non-malignant tonsillar tissues. J. Med. Virol. 2016, 88, 695–702. [Google Scholar] [CrossRef]
- Carpén, T.; Syrjänen, S.; Jouhi, L.; Randen-Brady, R.; Haglund, C.; Mäkitie, A.; Mattila, P.S.; Hagström, J. Epstein-Barr virus (EBV) and polyomaviruses are detectable in oropharyngeal cancer and EBV may have prognostic impact. Cancer Immunol. Immunother. 2020, 69, 1615–1626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bersani, C.; Haeggblom, L.; Ursu, R.G.; Giusca, S.E.; Marklund, L.; Ramqvist, T.; Näsman, A.; Dalianis, T. Overexpression of FGFR3 in HPV-positive tonsillar and base of tongue cancer is correlated to outcome. Anticancer Res. 2018, 38, 4683–4690. [Google Scholar] [CrossRef]
- Ursu, R.G.; Danciu, M.; Spiridon, I.A.; Ridder, R.; Rehm, S.; Maffini, F.; McKay-Chopin, S.; Carreire, C.; Lucas, E.; Costan, V.V.; et al. Role of mucosal high-risk human papillomavirus types in head and neck cancers in Romania. PLoS ONE 2018, 13, e0199663. [Google Scholar] [CrossRef]
- Mena, M.; Frias-Gomez, J.; Taberna, M.; Quirós, B.; Marquez, S.; Clavero, O.; Baena, A.; Lloveras, B.; Alejo, M.; León, X.; et al. Epidemiology of human papillomavirus-related oropharyngeal cancer in a classically low-burden region of southern Europe. Sci. Rep. 2020, 10, 13219. [Google Scholar] [CrossRef] [PubMed]
- Haeggblom, L.; Attoff, T.; Yu, J.; Holzhauser, S.; Vlastos, A.; Mirzae, L.; Ährlund-Richter, A.; Munck-Wikland, E.; Marklund, L.; Hammarstedt-Nordenvall, L.; et al. Changes in incidence and prevalence of human papillomavirus in tonsillar and base of tongue cancer during 2000–2016 in the Stockholm region and Sweden. Head Neck 2019, 41, 1583–1590. [Google Scholar] [CrossRef] [PubMed]
- Anantharaman, D.; Abedi-Ardekani, B.; Beachler, D.C.; Gheit, T.; Olshan, A.F.; Wisniewski, K.; Wunsch-Filho, V.; Toporcov, T.N.; Tajara, E.H.; Levi, J.E.; et al. Geographic heterogeneity in the prevalence of human papillomavirus in head and neck cancer. Int. J. Cancer 2017, 140, 1968–1975. [Google Scholar] [CrossRef] [PubMed]
- Castellsagué, X.; Alemany, L.; Quer, M.; Halec, G.; Quirós, B.; Tous, S.; Clavero, O.; Alòs, L.; Biegner, T.; Szafarowski, T.; et al. International HPV in Head and Neck Cancer Study Group. HPV involvement in head and neck cancers: Comprehensive assessment of biomarkers in 3680 patients. J. Natl. Cancer Inst. 2016, 108, djv403. [Google Scholar] [CrossRef]
- Dang, J.; Bruce, G.A.; Zhang, Q.; Kiviat, N.B. Identification and characterization of novel human papillomaviruses in oral rinse samples from oral cavity and oropharyngeal cancer patients. J. Oral Biosci. 2019, 61, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Galati, L.; Combes, J.D.; Gupta, P.; Sen, R.; Robitaille, A.; Brancaccio, R.N.; Atsou, K.; Cuenin, C.; McKay-Chopin, S.; Tornesello, M.L.; et al. Detection of a large spectrum of viral infections in conjunctival premalignant and malignant lesions. Int. J. Cancer 2020, 147, 2862–2870. [Google Scholar] [CrossRef]
- Zapatka, M.; Borozan, I.; Brewer, D.S.; Iskar, M.; Grundhoff, A.; Alawi, M.; Desai, N.; Sültmann, H.; Moch, H.; Cooper, C.S. The landscape of viral associations in human cancers. Nat. Genet. 2020, 52, 320–330. [Google Scholar] [CrossRef] [Green Version]
- Tabachnick-Cherny, S.; Pulliam, T.; Church, C.; Koelle, D.M.; Nghiem, P. Polyomavirus-driven Merkel cell carcinoma: Prospects for therapeutic vaccine development. Mol. Carcinog. 2020, 59, 807–821. [Google Scholar] [CrossRef]
- Holzhauser, S.; Wild, N.; Zupancic, M.; Ursu, R.G.; Bersani, C.; Näsman, A.; Kostopoulou, O.N.; Dalianis, T. Targeted therapy with PI3K and FGFR inhibitors on human papillomavirus positive and negative tonsillar and base of tongue cancer lines with and without corresponding mutations. Front. Oncol. 2021, 11, 640490. [Google Scholar] [CrossRef]
- Näsman, A.; Du, J.; Dalianis, T. A global epidemic increase of an HPV-induced tonsil and tongue base cancer—Potential benefit from a pan-gender use of HPV vaccine. J. Intern. Med. 2019, 287, 134–152. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Tumor Samples | Tested Viruses | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| EBV1 | HHV7 | MCV | HHV6 | CMV | HHV8 | HPyV6 | EBV1 | EBV1 | |
| positive samples | 16 | 12 | 8 | 8 | 6 | 2 | 1 | 1 | 1 |
| Positive for 4 Viruses | |||||||||
| hard palate | p = 0.001 | p = 0.001 | p = 0.020 | p = 0.617 | |||||
| inferior lip | p = 0.001 | p = 0.020 | p = 0.192 | p = 0.724 | |||||
| palatine tonsil | p = 0.001 | p = 0.020 | p = 0.020 | p = 0.617 | |||||
| buccal mucosa | p = 0.001 | p = 0.001 | p = 0.020 | p = 0.020 | |||||
| Positive for 3 Viruses | |||||||||
| inferior lip | p = 0.001 | p = 0.003 | p = 0.003 | ||||||
| right half tongue | p = 0.001 | p = 0.001 | p = 0.003 | ||||||
| anterior third hard palate | p = 0.001 | p = 0.003 | p = 0.003 | ||||||
| right temporal | p = 0.001 | p = 0.003 | p = 0.032 | ||||||
| alveolar ridge | p = 0.001 | p = 0.001 | p = 0.003 | p = 0.724 | |||||
| base of tongue | p = 0.001 | p = 0.003 | p = 0.724 | ||||||
| hard palate anterior part | p = 0.001 | p = 0.003 | p = 0.003 | ||||||
| Positive for 2 Viruses | |||||||||
| larynx | p = 0.001 | p = 0.001 | |||||||
| retromolar trigone | p = 0.001 | p = 0.001 | |||||||
| left retromolar trigone | p = 0.001 | p = 0.001 | |||||||
| right retromolar trigone | p = 0.001 | p = 0.001 | |||||||
| base of tongue | p = 0.001 | p = 0.001 | |||||||
| UniqueVirus Presence | |||||||||
| rhinopharyngeal | p = 0.001 | ||||||||
| pharyngeal | p = 0.001 | ||||||||
| buccal mucosa | p = 0.001 | ||||||||
| genian region | p = 0.001 | ||||||||
| uvula | p = 0.001 | ||||||||
| ulcerated superior lip | p = 0.001 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ursu, R.G.; Luchian, I.; Ghetu, N.; Costan, V.V.; Stamatin, O.; Palade, O.D.; Damian, C.; Iancu, L.S.; Porumb-Andrese, E. Emerging Oncogenic Viruses in Head and Neck Cancers from Romanian Patients. Appl. Sci. 2021, 11, 9356. https://doi.org/10.3390/app11199356
Ursu RG, Luchian I, Ghetu N, Costan VV, Stamatin O, Palade OD, Damian C, Iancu LS, Porumb-Andrese E. Emerging Oncogenic Viruses in Head and Neck Cancers from Romanian Patients. Applied Sciences. 2021; 11(19):9356. https://doi.org/10.3390/app11199356
Chicago/Turabian StyleUrsu, Ramona Gabriela, Ionut Luchian, Nicolae Ghetu, Victor Vlad Costan, Ovidiu Stamatin, Octavian Dragos Palade, Costin Damian, Luminita Smaranda Iancu, and Elena Porumb-Andrese. 2021. "Emerging Oncogenic Viruses in Head and Neck Cancers from Romanian Patients" Applied Sciences 11, no. 19: 9356. https://doi.org/10.3390/app11199356
APA StyleUrsu, R. G., Luchian, I., Ghetu, N., Costan, V. V., Stamatin, O., Palade, O. D., Damian, C., Iancu, L. S., & Porumb-Andrese, E. (2021). Emerging Oncogenic Viruses in Head and Neck Cancers from Romanian Patients. Applied Sciences, 11(19), 9356. https://doi.org/10.3390/app11199356