
Development of Immersive VR Device for Gait Training Rehabilitation with Biofeedback System-Preliminary Study



Abstract
:1. Introduction
2. Methods
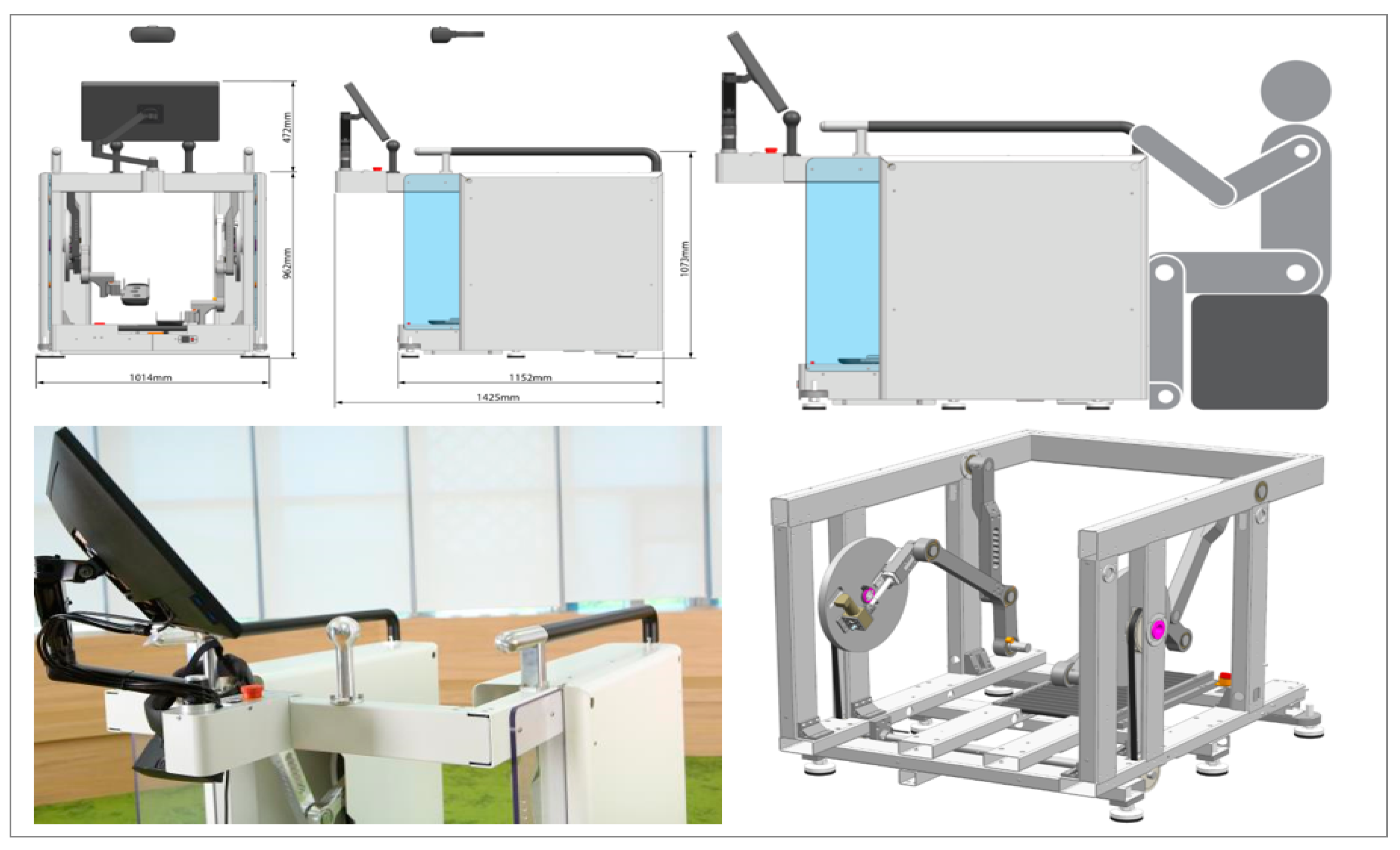
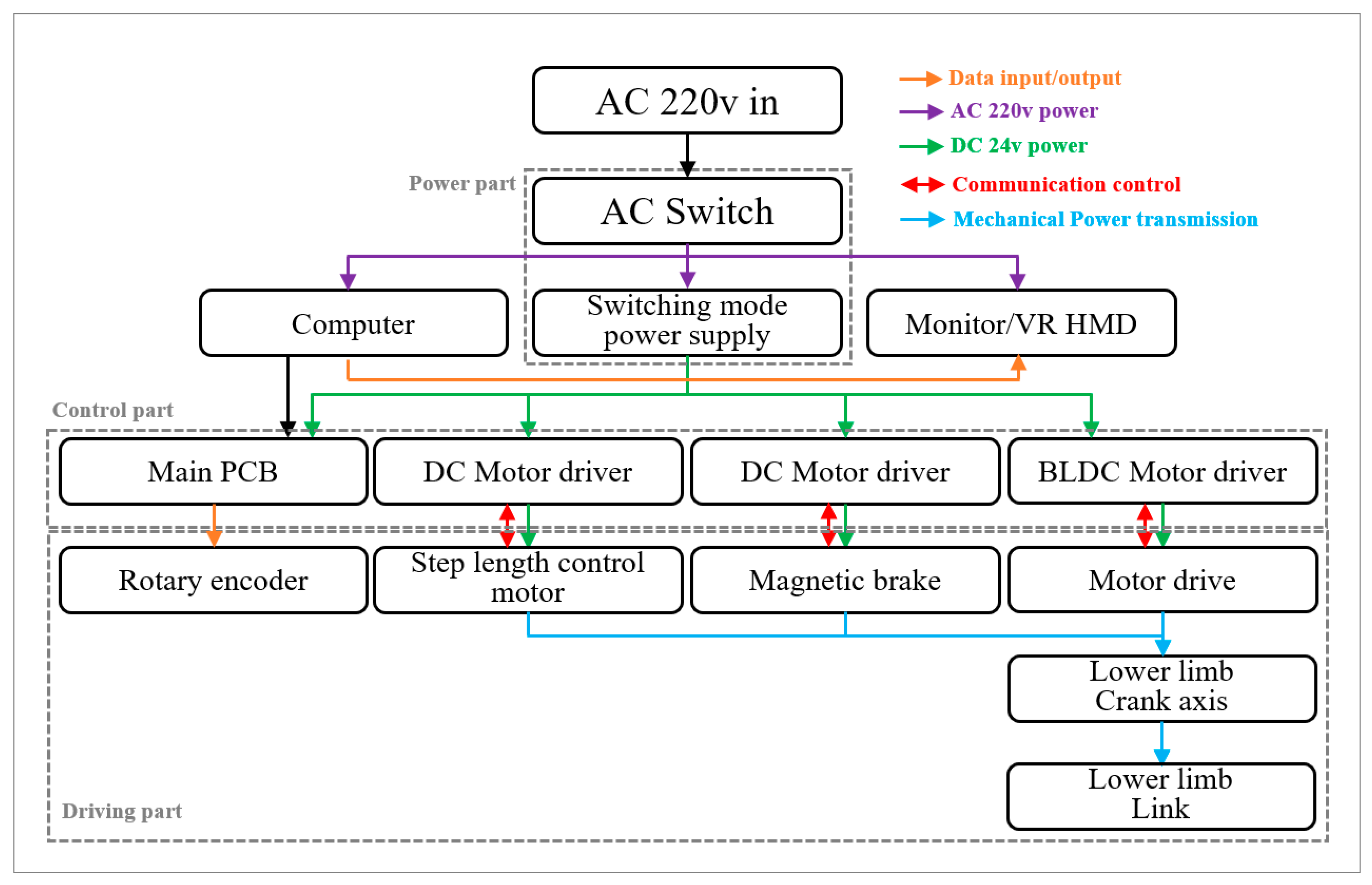
2.1. MGTR Design
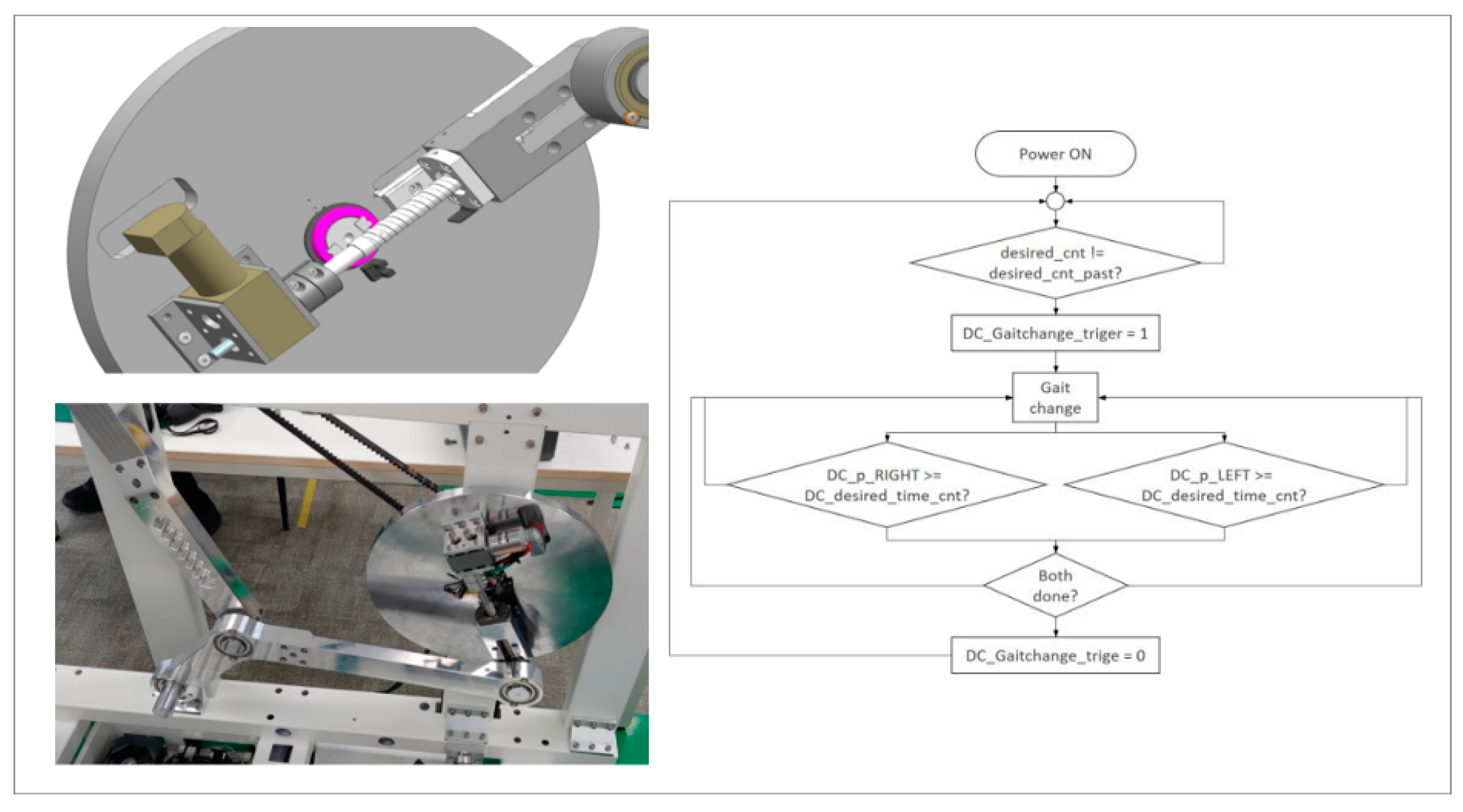
2.2. Mechanism of Gait Functionality
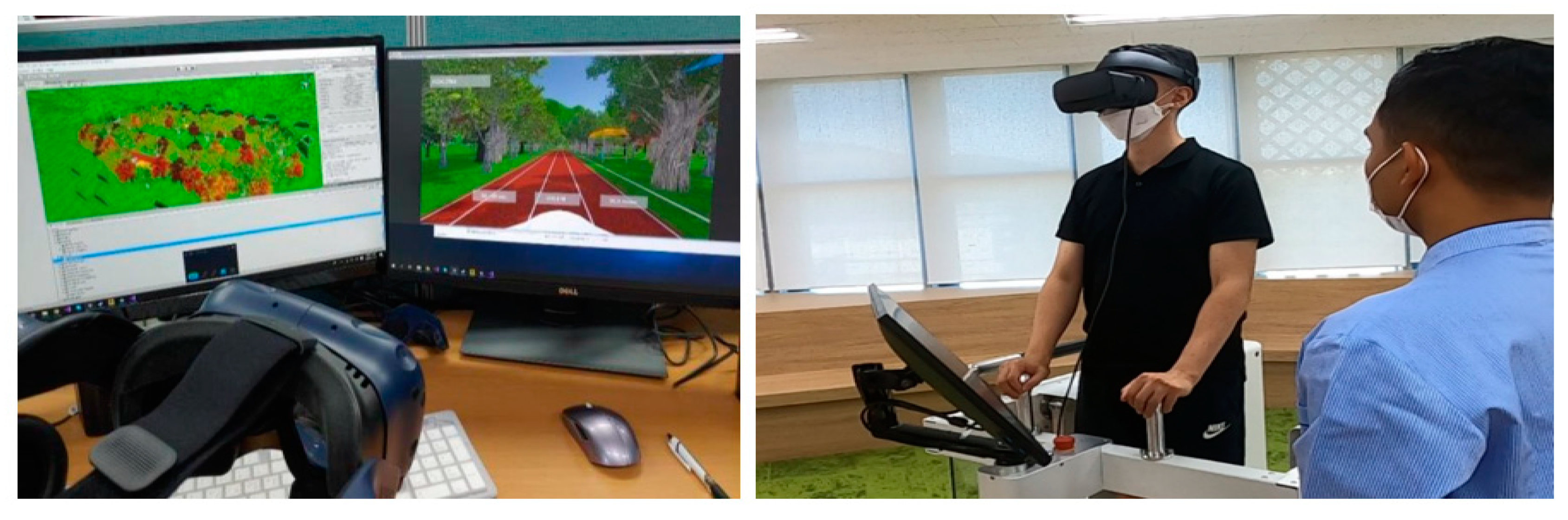
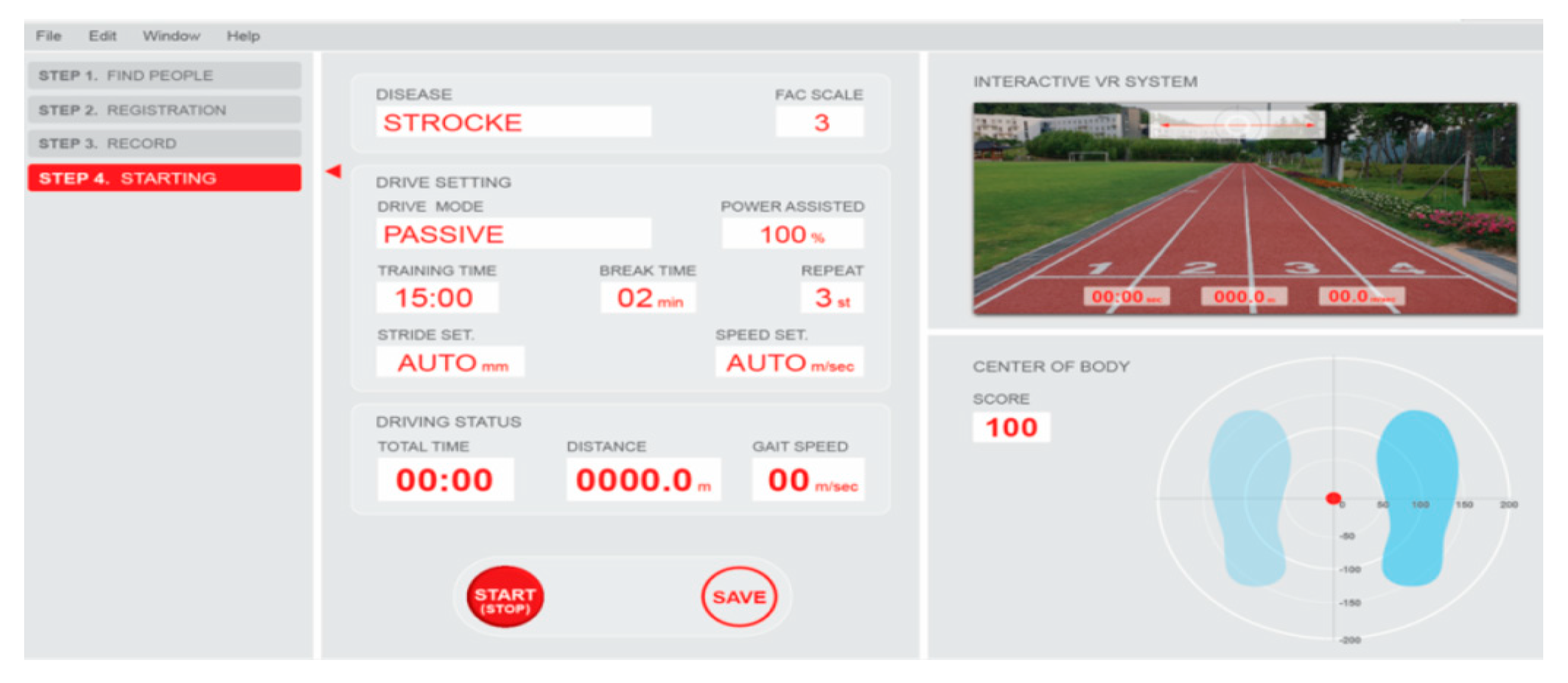
2.3. Application of VR System
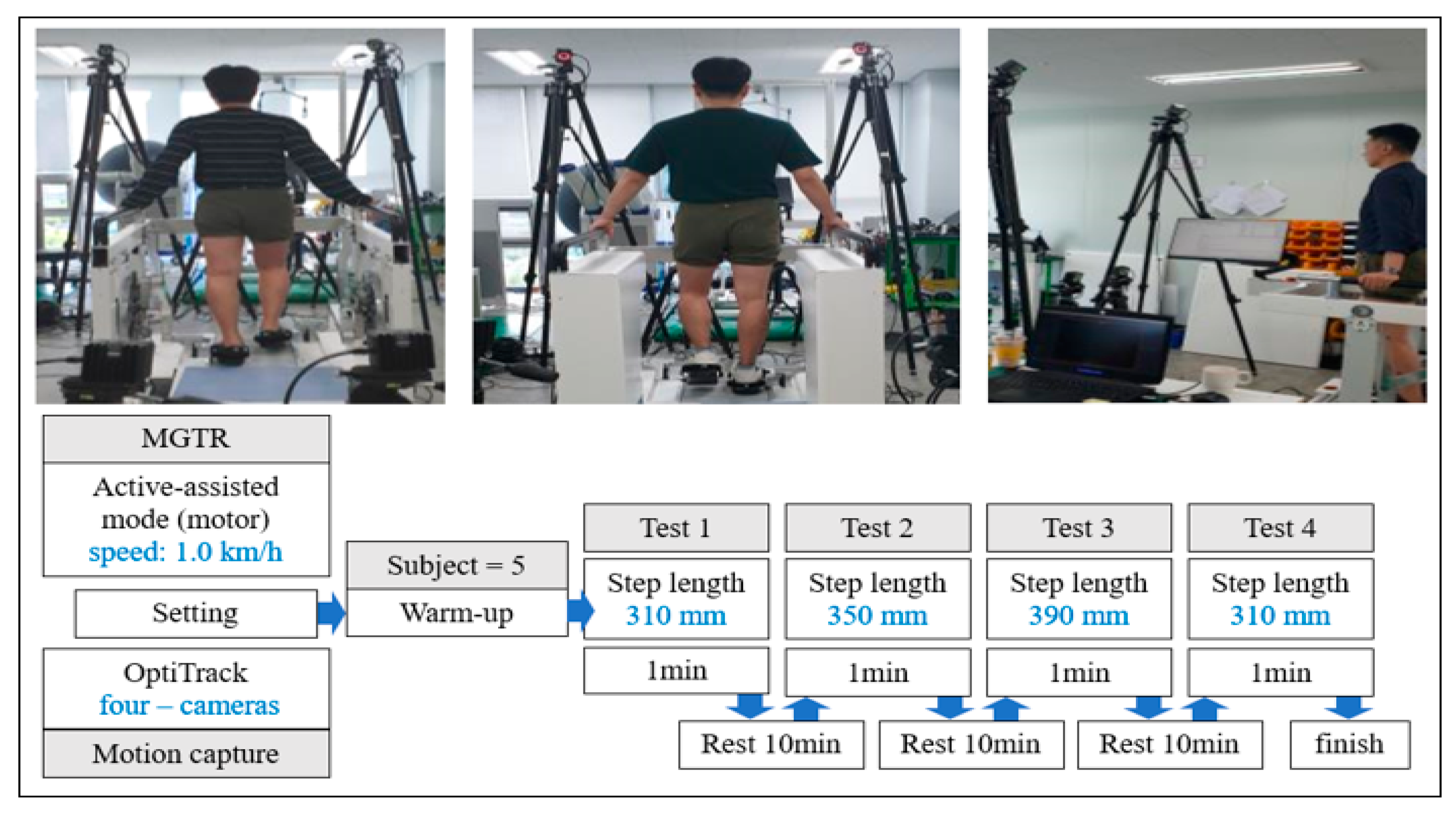
2.4. Training Program
2.5. System Functioning Test
2.6. VR System Test
2.7. Kinematic Evaluation
3. Results
3.1. System Functioning Test
3.2. VR System Test
3.3. Kinematic Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Calabrò, R.S.; Cacciola, A.; Bertè, F.; Manuli, A.; Leo, A.; Bramanti, A.; Naro, A.; Milardi, D.; Bramanti, P. Robotic Gait Rehabilitation and Substitution Devices in Neurological Disorders: Where Are We Now? Neurol. Sci. 2016, 37, 503–514. [Google Scholar] [CrossRef]
- Cho, K.H.; Park, S.J. Effects of Joint Mobilization and Stretching on the Range of Motion for Ankle Joint and Spatiotemporal Gait Variables in Stroke Patients. J. Stroke Cerebrovasc. Dis. 2020, 29, 104933. [Google Scholar] [CrossRef]
- Díaz, I.; Gil, J.J.; Sánchez, E. Lower-Limb Robotic Rehabilitation: Literature Review and Challenges. J. Robot. 2011, 2011, 1–11. [Google Scholar] [CrossRef]
- Aprile, I.; Iacovelli, C.; Goffredo, M.; Cruciani, A.; Galli, M.; Simbolotti, C.; Pecchioli, C.; Padua, L.; Galafate, D.; Pournajaf, S.; et al. Efficacy of End-Effector Robot-Assisted Gait Training in Subacute Stroke Patients: Clinical and Gait Outcomes from a Pilot Bi-Centre Study. NeuroRehabilitation 2019, 45, 201–212. [Google Scholar] [CrossRef] [PubMed]
- Molteni, F.; Gasperini, G.; Cannaviello, G.; Guanziroli, E. Exoskeleton and End-Effector Robots for Upper and Lower Limbs Rehabilitation: Narrative Review. PM&R 2018, 9 (Suppl. 2), 174–188. [Google Scholar]
- Shi, D.; Zhang, W.; Zhang, W.; Ding, X. A Review on Lower Limb Rehabilitation Exoskeleton Robots. Chin. J. Mech. Eng. 2019, 32, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Maranesi, E.; Riccardi, G.R.; Di Donna, V.; Di Rosa, M.; Fabbietti, P.; Luzi, R.; Pranno, L.; Lattanzio, F.; Bevilacqua, R. Effectiveness of Intervention Based on End-effector Gait Trainer in Older Patients with Stroke: A Systematic Review. J. Am. Med. Dir. Assoc. 2020, 21, 1036–1044. [Google Scholar] [CrossRef]
- Hobbs, B.; Artemiadis, P. A Review of Robot-Assisted Lower-Limb Stroke Therapy: Unexplored Paths and Future Directions in Gait Rehabilitation. Front. Neurorobot. 2020, 14, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kern, F.; Winter, C.; Gall, D.; Kathner, I.; Pauli, P.; Latoschik, M.E. Immersive Virtual Reality and Gamification Within Procedurally Generated Environments to Increase Motivation During Gait Rehabilitation. In Proceedings of the IEEE Conference on Virtual Reality and 3D User Interfaces (VR), Osaka, Japan, 23–27 March 2019. [Google Scholar]
- Winter, C.; Kern, F.; Gall, D.; Latoschik, M.E.; Pauli, P.; Käthner, I. Immersive Virtual Reality during Gait Rehabilitation Increases Walking Speed and Motivation: A Usability Evaluation with Healthy Participants and Patients with Multiple Sclerosis and Stroke. J. Neuroeng. Rehabil. 2021, 18, 68. [Google Scholar] [CrossRef] [PubMed]
- Laver, K.E.; Lange, B.; George, S.; Deutsch, J.E.; Saposnik, G.; Crotty, M. Virtual Reality for Stroke Rehabilitation. Cochrane Database Syst. Rev. 2017, 11, CD008349. [Google Scholar] [CrossRef] [Green Version]
- Bevilacqua, R.; Maranesi, E.; Riccardi, G.R.; Di Donna, V.; Pelliccioni, P.; Riccardo, L.; Lattanzio, F.; Pelliccioni, G. Non-Immersive Virtual Reality for Rehabilitation of the Older People: A Systematic Review into Efficacy and Effectiveness. J. Clin. Med. 2019, 8, 1882. [Google Scholar] [CrossRef] [Green Version]
- Booth, A.T.C.; Buizer, A.I.; Harlaar, J.; Steenbrink, F.; Van Der Krogt, M.M. Immediate Effects of Immersive Biofeedback on Gait in Children with Cerebral Palsy. Arch. Phys. Med. Rehabil. 2019, 100, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Bevilacqua, R.; Casaccia, S.; Cortellessa, G.; Astell, A.; Lattanzio, F.; Corsonello, A.; D’Ascoli, P.; Paolini, S.; Di Rosa, M.; Rossi, L.; et al. Coaching Through Technology: A Systematic Review into Efficacy and Effectiveness for the Ageing Population. Int. J. Environ. Res. Public Health 2020, 17, 5930. [Google Scholar] [CrossRef]
- Cano Porras, D.; Siemonsma, P.; Inzelberg, R.; Zeilig, G.; Plotnik, M. Advantages of Virtual Reality in the Rehabilitation of Balance and Gait: Systematic Review. Neurology 2018, 90, 1017–1025. [Google Scholar] [CrossRef]
- Brütsch, K.; Koenig, A.; Zimmerli, L.; Mérillat-Koeneke, S.; Riener, R.; Jäncke, L.; Van Hedel, H.J.; Meyer-Heim, A. Virtual Reality for Enhancement of Robot-Assisted Gait Training in Children with Central Gait Disorders. J. Rehabil. Med. 2011, 43, 493–499. [Google Scholar] [CrossRef] [Green Version]
- Bergmann, J.; Krewer, C.; Bauer, P.; Koenig, A.; Riener, R.; Müller, F. Virtual Reality to Augment Robot-Assisted Gait Training in Non-Ambulatory Patients with a Subacute Stroke: A Pilot Randomized Controlled Trial. Eur. J. Phys. Rehabil. Med. 2018, 54, 397–407. [Google Scholar] [CrossRef]
- Weber, H.; Barr, C.; Gough, C.; Van Den Berg, M. How Commercially Available Virtual Reality-Based Interventions Are Delivered and Reported in Gait, Posture, and Balance Rehabilitation: A Systematic Review. Phys. Ther. 2020, 100, 1805–1815. [Google Scholar] [CrossRef]
- Lünenburger, L.; Colombo, G.; Riener, R. Biofeedback for Robotic Gait Rehabilitation. J. Neuroeng. Rehabil. 2007, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seo, J.W.; Kim, H.S. Biomechanical Analysis in Five Bar Linkage Prototype Machine of Gait Training and Rehabilitation by IMU Sensor and Electromyography. Sensors 2021, 21, 1726. [Google Scholar] [CrossRef] [PubMed]
- Hagita, K.; Matsumoto, S.; Ota, K. Study of Commodity VR for Computational Material Sciences. ACS Omega 2019, 4, 3990–3999. [Google Scholar] [CrossRef] [Green Version]
- Dong-Eui University. Development of a Guideline for Evaluating and Testing Safety and Performance of Robot-Assisted Rehabilitation System; TRKO201600010293; Korea Food & Drug Administration (KFDA): Busan, Korea, 2015. [CrossRef]
- Perry, J.; Burnfield, J.M. Gait Analysis: Normal and Pathological Function, 2nd ed.; Section VI; Slack: Thorofare, NJ, USA, 2010. [Google Scholar]
- Hidler, J.; Wisman, W.; Neckel, N. Kinematic Trajectories While Walking Within the Lokomat Robotic Gait-Orthosis. Clin. Biomech. 2008, 23, 1251–1259. [Google Scholar] [CrossRef] [PubMed]
- Marouvo, J.; Sousa, F.; Fernandes, O.; Castro, M.A.; Paszkiel, S. Gait Kinematics Analysis of Flatfoot Adults. Appl. Sci. 2021, 11, 7077. [Google Scholar] [CrossRef]
- Shi, B.; Chen, X.; Yue, Z.; Yin, S.; Weng, Q.; Zhang, X.; Wang, J.; Wen, W. Wearable Ankle Robots in Post-Stroke Rehabilitation of Gait: A Systematic Review. Front. Neurorobot. 2019, 13, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glowinski, S.; Krzyzynski, T.; Bryndal, A.; Maciejewski, I. A Kinematic Model of a Humanoid Lower Limb Exoskeleton with Hydraulic Actuators. Sensors 2020, 20, 6116. [Google Scholar] [CrossRef] [PubMed]
- De Rooij, I.J.M.; Van De Port, I.G.L.; Meijer, J.-W.G. Effect of Virtual Reality Training on Balance and Gait Ability in Patients with Stroke: Systematic Review and Meta-Analysis. Phys. Ther. 2016, 96, 1905–1918. [Google Scholar] [CrossRef] [PubMed]
- Dao, Q.-T.; Yamamoto, S.-I. Assist-as-Needed Control of a Robotic Orthosis Actuated by Pneumatic Artificial Muscle for Gait Rehabilitation. Appl. Sci. 2018, 8, 499. [Google Scholar] [CrossRef] [Green Version]
- Mirelman, A.; Patritti, B.L.; Bonato, P.; Deutsch, J.E. Effects of Virtual Reality Training on Gait Biomechanics of Individuals Post-Stroke. Gait Posture 2010, 31, 433–437. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Right Leg | Left Leg | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Set Step Length (mm) | 310 | 350 | 390 | 430 | 310 | 350 | 390 | 430 | |
| Hip angle (deg) | Max (flexion) | 30.08 | 32.58 | 33.73 | 36.01 | 27.58 a,b | 29.91 | 31.94 b | 32.00 a |
| ±5.95 | ±3.95 | ±3.05 | ±4.81 | ±3.21 | ±2.31 | ±1.25 | ±2.36 | ||
| Min (extension) | 1.10 | 0.12 | 1.07 | 0.51 | 0.18 | 0.10 | −0.50 | −1.04 | |
| ±5.40 | ±1.39 | ±1.83 | ±4.08 | ±3.84 | ±1.22 | ±1.82 | ±2.05 | ||
| RoM | 28.99 a | 32.46 | 32.66 | 35.49 a | 27.40 b,c | 29.81 | 32.44 c | 33.03 b | |
| ±3.07 | ±3.14 | ±1.94 | ±3.64 | ±1.16 | ±2.25 | ±1.90 | ±2.12 | ||
| Knee angle (deg) | Max (flexion) | 44.76 | 49.02 | 52.57 | 56.48 | 44.01 a,b | 47.14 c | 51.57 b | 54.74 a,c |
| ±7.78 | ±7.10 | ±7.00 | ±5.94 | ±1.62 | ±2.81 | ±3.47 | ±3.59 | ||
| Min (extension) | 3.05 | 3.49 | 2.57 | 3.13 | 1.27 | 1.44 | −0.33 | 0.86 | |
| ±1.72 | ±1.28 | ±1.96 | ±0.54 | ±0.96 | ±1.86 | ±3.42 | ±0.68 | ||
| RoM | 41.71 a | 45.53 | 50.01 | 53.35 a | 42.73 b,c | 45.71 d | 51.90 c | 53.88 b,d | |
| ±6.62 | ±6.96 | ±5.74 | ±5.83 | ±1.19 | ±1.79 | ±6.67 | ±3.63 | ||
| Ankle angle (deg) | Max (dorsi) | 29.79 | 26.87 | 27.83 | 32.33 | 29.04 | 27.67 | 28.49 | 32.16 |
| ±5.43 | ±4.77 | ±5.55 | ±4.22 | ±3.02 | ±6.59 | ±7.13 | ±6.95 | ||
| Min (plantar) | −5.64 | −7.92 | −8.85 | −7.25 | −4.87 | −5.32 | −5.82 | −4.95 | |
| ±3.45 | ±4.45 | ±6.96 | ±5.63 | ±6.35 | ±4.77 | ±6.29 | ±5.37 | ||
| RoM | 35.43 | 34.79 | 36.68 | 39.58 | 33.91 | 32.99 | 34.31 | 37.11 | |
| ±7.88 | ±6.18 | ±9.39 | ±8.29 | ±5.62 | ±3.66 | ±2.89 | ±2.39 | ||
| Measured step length (mm) | 310.80 | 352.00 | 392.80 | 433.40 | 311.20 | 353.60 | 395.40 | 435.80 | |
| ±0.45 | ±1.22 | ±0.45 | ±1.14 | ±0.45 | ±2.19 | ±2.19 | ±1.10 | ||
| Right Leg | Left Leg | |||||||
|---|---|---|---|---|---|---|---|---|
| Set Step Length (mm) | 310 | 350 | 390 | 430 | 310 | 350 | 390 | 430 |
| Swing ratio (%) | 68.08 | 68.00 | 66.47 | 70.45 | 70.17 | 68.71 | 67.67 | 71.46 |
| ±9.09 | ±8.13 | ±4.17 | ±5.04 | ±7.34 | ±8.17 | ±2.72 | ±4.80 | |
| Stance ratio (%) | 31.92 | 31.00 | 33.53 | 29.55 | 29.83 | 31.29 | 32.33 | 28.54 |
| ±9.09 | ±7.72 | ±4.17 | ±5.04 | ±7.34 | ±8.17 | ±2.72 | ±4.80 | |
| Swing time (s) | 1.13 | 1.22 | 1.26 | 1.35 | 1.14 | 1.20 | 1.28 | 1.38 |
| ±0.28 | ±0.22 | ±0.21 | ±0.21 | ±0.24 | ±0.06 | ±0.16 | ±0.11 | |
| Stance time (s) | 0.51 | 0.54 | 0.63 | 0.56 | 0.48 | 0.56 | 0.61 | 0.56 |
| ±0.09 | ±0.10 | ±0.03 | ±0.06 | ±0.11 | ±0.17 | ±0.07 | ±0.14 | |
| Step duration (s) | 1.64 | 1.76 | 1.89 | 1.91 | 1.62 | 1.76 | 1.89 | 1.94 |
| ±0.21 | ±0.17 | ±0.21 | ±0.22 | ±0.21 | ±0.17 | ±0.21 | ±0.22 | |
| Max. Heel height (m) | 0.23 a,b,c | 0.25 a,d | 0.27 b,e | 0.29 c,d,e | 0.23 f,g,h | 0.26 f,i | 0.27 g,j | 0.30 h,i,j |
| ±0.01 | ±0.01 | ±0.01 | ±0.01 | ±0.01 | ±0.01 | ±0.01 | ±0.01 | |
| Min. Angle | Max. Angle | RoM | ||
|---|---|---|---|---|
| Hip | Ground walking | −14.56 ± 7.50 | 54.40 ± 12.59 | 68.97 ± 14.65 |
| Passive | 24.02 ± 3.16 | 43.32 ± 5.74 | 19.31 ± 3.11 | |
| Motor active | 0.70 ± 3.31 | 33.10 ± 4.73 | 32.40 ± 3.64 | |
| Knee | Ground walking | 13.85 ± 6.66 | 93.81 ± 14.31 | 79.96 ± 19.25 |
| Passive | 60.17 ± 3.41 | 102.78 ± 6.90 | 42.61 ± 4.25 | |
| Motor active | 3.06 ± 1.40 | 50.71 ± 7.80 | 47.65 ± 7.35 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seo, J.-W.; Kim, D.-H.; Jung, J.; Kim, J.-J.; Kim, H.-S. Development of Immersive VR Device for Gait Training Rehabilitation with Biofeedback System-Preliminary Study. Appl. Sci. 2021, 11, 10394. https://doi.org/10.3390/app112110394
Seo J-W, Kim D-H, Jung J, Kim J-J, Kim H-S. Development of Immersive VR Device for Gait Training Rehabilitation with Biofeedback System-Preliminary Study. Applied Sciences. 2021; 11(21):10394. https://doi.org/10.3390/app112110394
Chicago/Turabian StyleSeo, Jeong-Woo, Dae-Hyeok Kim, Jeeyoun Jung, Jung-Joon Kim, and Hyeong-Sic Kim. 2021. "Development of Immersive VR Device for Gait Training Rehabilitation with Biofeedback System-Preliminary Study" Applied Sciences 11, no. 21: 10394. https://doi.org/10.3390/app112110394
APA StyleSeo, J.-W., Kim, D.-H., Jung, J., Kim, J.-J., & Kim, H.-S. (2021). Development of Immersive VR Device for Gait Training Rehabilitation with Biofeedback System-Preliminary Study. Applied Sciences, 11(21), 10394. https://doi.org/10.3390/app112110394