
Accuracy of Implant Level Intraoral Scanning and Photogrammetry Impression Techniques in a Complete Arch with Angled and Parallel Implants: An In Vitro Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moreira, A.H.; Rodrigues, N.F.; Pinho, A.C.; Fonseca, J.C.; Vilaça, J.L. Accuracy comparison of implant impression techniques: A systematic review. Clin. Implant Dent. Relat. Res. 2015, 17, e751–e764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joda, T.; Ferrari, M.; Gallucci, G.O.; Wittneben, J.G.; Brägger, U. Digital technology in fixed implant prosthodontics. Periodontology 2000 2016, 73, 178–192. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.; Gandolfi, A.; Luongo, G.; Logozzo, S. Intraoral scanners in dentistry: A review of the current literature. BMC Oral Health 2017, 17, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mizumoto, R.M.; Yilmaz, B. Intraoral scan bodies in implant dentistry. A systematic review. J. Prosthet. Dent. 2018, 120, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Pyo, S.W.; Kim, D.J.; Han, J.S.; Yeo, I.L. Ceramic materials and technologies applied to digital works in implant-supported restorative dentistry. Materials 2020, 13, 1964. [Google Scholar] [CrossRef] [PubMed]
- Papadiochou, S.; Pissiotis, A.L. Marginal adaptation and CAD-CAM technology: A systematic review of restorative material and fabrication techniques. J. Prosthet. Dent. 2018, 119, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Hultin, M.; Svensson, K.G.; Trulsson, M. Clinical advantages of computer-guided implant placement: A systematic review. Clin. Oral Implant. Res. 2012, 6, 124–135. [Google Scholar] [CrossRef] [PubMed]
- Bover-Ramos, F.; Viña-Almunia, J.; Cervera-Ballester, J.; Peñarrocha-Diago, M.; García-Mira, B. Accuracy of implant placement with computer-guided surgery: A systematic review and meta-analysis comparing cadaver, clinical, and in vitro studies. Int. J. Oral Maxillofac. Implant. 2018, 33, 101–115. [Google Scholar] [CrossRef] [PubMed]
- Keul, C.; Güth, J.F. Accuracy of full-arch digital impressions: An in vitro and in vivo comparison. Clin. Oral Investig. 2020, 24, 735–745. [Google Scholar] [CrossRef] [PubMed]
- Aragón, M.L.; Pontes, L.F.; Bichara, L.M.; Flores-Mir, C.; Normando, D. Validity and reliability of intraoral scanners compared to conventional gypsum models measurements: A systematic review. Eur. J. Orthod. 2016, 38, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Giménez, B.; Özcan, M.; Martínez-Rus, F.; Pradíes, G. Accuracy of a digital impression system based on parallel confocal laser technology for implants with consideration of operator experience and implant angulation and depth. Int. J. Oral Maxillofac. Implant. 2014, 29, 853–862. [Google Scholar] [CrossRef] [PubMed]
- Alikhasi, M.; Siadat, H.; Nasirpour, A.; Hasanzade, M. Three-dimensional accuracy of digital impression versus conventional method: Effect of implant angulation and connection type. Int. J. Dent. 2018, 2018, 3761750. [Google Scholar] [CrossRef] [PubMed]
- Carneiro Pereira, A.L.; Medeiros, V.R.; da Fonte Porto Carreiro, A. Influence of implant position on the accuracy of intraoral scanning in fully edentulous arches: A systematic review. J. Prosthet. Dent. 2020. [Google Scholar] [CrossRef] [PubMed]
- Arcuri, L.; Pozzi, A.; Lio, F.; Rompen, E.; Zechner, W.; Nardi, A. Influence of implant scanbody material, position and operator on the accuracy of digital impression for complete-arch: A randomized in vitro trial. J. Prosthodont. Res. 2020, 64, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Müller, P.; Ender, A.; Joda, T.; Katsoulis, J. Impact of digital intraoral scan strategies on the impression accuracy using the TRIOS Pod scanner. Quintessence Int. 2016, 47, 343–349. [Google Scholar] [PubMed]
- Revilla-León, M.; Jiang, P.; Sadeghpour, M.; Piedra-Cascón, W.; Zandinejad, A.; Özcan, M.; Krishnamurthy, V.R. Intraoral digital scans-Part 1: Influence of ambient scanning light conditions on the accuracy (trueness and precision) of different intraoral scanners. J. Prosthet. Dent. 2020, 124, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Jiang, P.; Sadeghpour, M.; Piedra-Cascón, W.; Zandinejad, A.; Özcan, M.; Krishnamurthy, V.R. Intraoral digital scans: Part 2-influence of ambient scanning light conditions on the mesh quality of different intraoral scanners. J. Prosthet. Dent. 2020, 124, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.Y.; Yee, S.H.X.; Wong, K.M.; Tan, Y.H.; Tan, K.B.C. Comparison of three-dimensional accuracy of digital and conventional implant impressions: Effect of interimplant distance in an edentulous arch. Int. J. Oral Maxillofac. Implant. 2019, 34, 366–380. [Google Scholar] [CrossRef] [PubMed]
- Fluegge, T.; Att, W.; Metzger, M.; Nelson, K. A novel method to evaluate precision of optical implant impressions with commercial scan bodies-an experimental approach. J. Prosthodont. 2017, 26, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Andriessen, F.S.; Rijkens, D.R.; van der Meer, W.J.; Wismeijer, D.W. Applicability and accuracy of an intraoral scanner for scanning multiple implants in edentulous mandibles: A pilot study. J. Prosthet. Dent. 2014, 111, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Giménez, B.; Pradíes, G.; Martínez-Rus, F.; Özcan, M. Accuracy of two digital implant impression systems based on confocal microscopy with variations in customized software and clinical parameters. Int. J. Oral Maxillofac. Implant. 2015, 30, 56–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodacre, B.J.; Goodacre, C.J.; Baba, N.Z. Using intraoral scanning to capture complete denture impressions, tooth positions, and centric relation records. Int. J. Prosthodont. 2018, 31, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Rhee, Y.K.; Huh, Y.H.; Cho, L.R.; Park, C.J. Comparison of intraoral scanning and conventional impression techniques using 3-dimensional superimposition. J. Adv. Prosthodont. 2015, 7, 460–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petriceks, A.H.; Peterson, A.S.; Angeles, M.; Brown, W.P.; Srivastava, S. Photogrammetry of human specimens: An innovation in anatomy education. J. Med. Educ. Curric. Dev. 2018, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jemt, T.; Bäck, T.; Petersson, A. Photogrammetry-an alternative to conventional impressions in implant dentistry? A clinical pilot study. Int. J. Prosthodont. 1999, 12, 363–368. [Google Scholar] [PubMed]
- Peñarrocha-Oltra, D.; Agustín-Panadero, R.; Bagán, L.; Giménez, B.; Peñarrocha, M. Impression of multiple implants using photogrammetry: Description of technique and case presentation. Med. Oral Patol. Oral Cir. Bucal 2014, 19, e366. [Google Scholar] [CrossRef] [PubMed]
- Peñarrocha-Diago, M.; Balaguer-Martí, J.C.; Peñarrocha-Oltra, D.; Balaguer-Martínez, J.F.; Peñarrocha-Diago, M.; Agustín-Panadero, R. A combined digital and stereophotogrammetric technique for rehabilitation with immediate loading of complete-arch, implant-supported prostheses: A randomized controlled pilot clinical trial. J. Prosthet. Dent. 2017, 118, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Pradíes, G.; Ferreiroa, A.; Özcan, M.; Giménez, B.; Martínez-Rus, F. Using stereophotogrammetric technology for obtaining intraoral digital impressions of implants. J. Am. Dent. Assoc. 2014, 145, 338–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peñarrocha-Oltra, D.; Agustín-Panadero, R.; Pradíes, G.; Gomar-Vercher, S.; Peñarrocha-Diago, M. Maxillary Full-Arch Immediately Loaded Implant-Supported Fixed Prosthesis Designed and Produced by Photogrammetry and Digital Printing: A Clinical Report. J. Prosthodont. 2017, 26, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Agustín-Panadero, R.; Peñarrocha-Oltra, D.; Gomar-Vercher, S.; Peñarrocha-Diago, M. Stereophotogrammetry for Recording the Position of Multiple Implants: Technical Description. Int. J. Prosthodont. 2015, 28, 631–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-Monescillo, A.; Sánchez-Turrión, A.; Vellon-Domarco, E.; Salinas-Goodier, C.; Prados-Frutos, J.C. Photogrammetry Impression Technique: A Case History Report. Int. J. Prosthodont. 2016, 29, 71–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-Monescillo, A.; Hernanz-Martín, J.; González-Serrano, C.; González-Serrano, J.; Duarte, S., Jr. All-on-four rehabilitation using photogrammetric impression technique. Quintessence Int. 2019, 50, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Molinero-Mourelle, P.; Lam, W.; Cascos-Sánchez, R.; Azevedo, L.; Gómez-Polo, M. Photogrammetric and intraoral digital impression technique for the rehabilitation of multiple unfavorably positioned dental implants: A clinical report. J. Oral Implantol. 2019, 45, 398–402. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Att, W.; Özcan, M.; Rubenstein, J. Comparison of conventional, photogrammetry, and intraoral scanning accuracy of complete-arch implant impression procedures evaluated with a coordinate measuring machine. J. Prosthet. Dent. 2021, 125, 470–478. [Google Scholar] [CrossRef] [PubMed]
- Sallorenzo, A.; Gómez-Polo, M. Comparative study of the accuracy of an implant intraoral scanner and that of a conventional intraoral scanner for complete-arch fixed dental prostheses. J. Prosthet. Dent. 2021. [Google Scholar] [CrossRef] [PubMed]
- Tohme, H.; Lawand, G.; Chmielewska, M.; Makhzoume, J. Comparison between stereophotogrammetric, digital, and conventional impression techniques in implant-supported fixed complete arch prostheses: An in vitro study. J. Prosthet. Dent. 2021. [Google Scholar] [CrossRef] [PubMed]
- ISO 5725-1. Accuracy (Trueness and Precision) of Measuring Methods and Results. Part-I: General Principles and Definitions; Beuth Verlag GmbH: Berlin, Germany, 1994. [Google Scholar]
- Ender, A.; Mehl, A. Accuracy of complete-arch dental impressions: A new method of measuring trueness and precision. J. Prosthet. Dent. 2013, 109, 121–128. [Google Scholar] [CrossRef] [Green Version]
- Giachetti, L.; Sarti, C.; Cinelli, F.; Russo, D.S. Accuracy of digital impressions in fixed prosthodontics: A systematic review of clinical studies. Int. J. Prosthodont. 2020, 33, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Wenz, H.J.; Hertrampf, K. Accuracy of impressions and casts using different implant impression techniques in a multi-implant system with an internal hex connection. Int. J. Oral Maxillofac. Implant. 2008, 23, 39–47. [Google Scholar]
- Mangano, F.G.; Hauschild, U.; Veronesi, G.; Imburgia, M.; Mangano, C.; Admakin, O. Trueness and precision of 5 intraoral scanners in the impressions of single and multiple implants: A comparative in vitro study. BMC Oral Health 2019, 19, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tantbirojn, D.; Pintado, M.R.; Versluis, A.; Dunn, C.; Delong, R. Quantitative analysis of tooth surface loss associated with gastroesophageal reflux disease: A longitudinal clinical study. J. Am. Dent. Assoc. 2012, 143, 278–285. [Google Scholar] [CrossRef] [PubMed]
- O’Toole, S.; Osnes, C.; Bartlett, D.; Keeling, A. Investigation into the accuracy and measurement methods of sequential 3D dental scan alignment. Dent. Mater. 2019, 35, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Kim, R.J.; Benic, G.I.; Park, J.M. Trueness of digital intraoral impression in reproducing multiple implant position. PLoS ONE 2019, 14, e0222070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iturrate, M.; Eguiraun, H.; Solaberrieta, E. Accuracy of digital impressions for implant-supported complete-arch prosthesis, using an auxiliary geometry part-An in vitro study. Clin. Oral Implant. Res. 2019, 30, 1250–1258. [Google Scholar] [CrossRef] [PubMed]
- Mizumoto, R.M.; Alp, G.; Özcan, M.; Yilmaz, B. The effect of scanning the palate and scan body position on the accuracy of complete-arch implant scans. Clin. Implant Dent. Relat. Res. 2019, 21, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Papaspyridakos, P.; Gallucci, G.O.; Chen, C.J.; Hanssen, S.; Naert, I.; Vandenberghe, B. Digital versus conventional implant impressions for edentulous patients: Accuracy outcomes. Clin. Oral Implant. Res. 2016, 27, 465–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amin, S.; Weber, H.P.; Finkelman, M.; El Rafie, K.; Kudara, Y.; Papaspyridakos, P. Digital vs. conventional full-arch implant impressions: A comparative study. Clin. Oral Implant. Res. 2017, 28, 1360–1367. [Google Scholar] [CrossRef] [PubMed]
- Chai, T.; Draxler, R.R. Root mean square error (RMSE) or mean absolute error (MAE)? e Arguments against avoiding RMSE in the literature. Geosci. Model Dev. 2014, 7, 1247–1250. [Google Scholar] [CrossRef] [Green Version]
- Pereira, L.M.S.; Sordi, M.B.; Magini, R.S.; Calazans Duarte, A.R.; Souza, J.C.M. Abutment misfit in implant-supported prostheses manufactured by casting technique: An integrative review. Eur. J. Dent. 2017, 11, 553–558. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
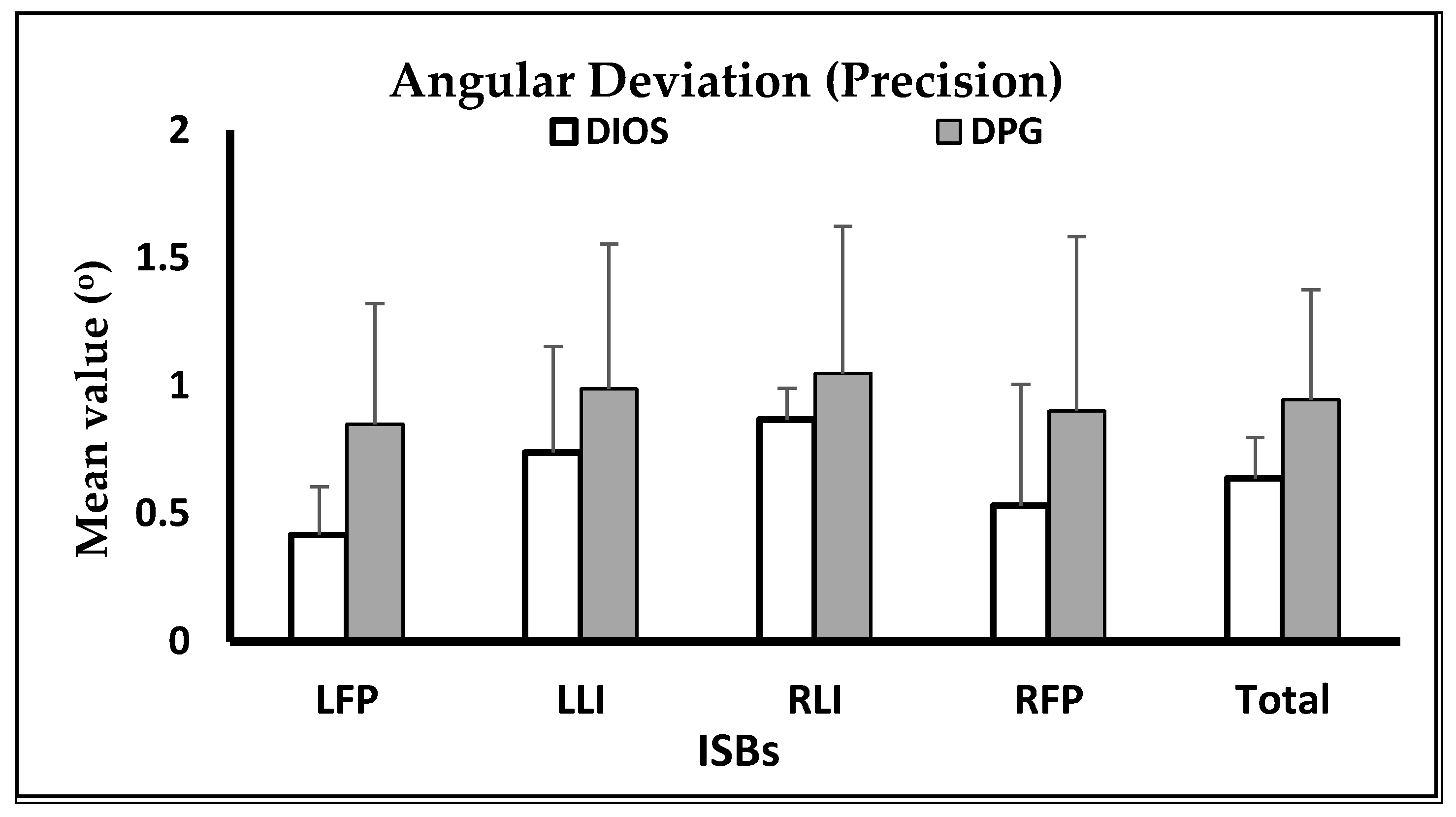
| Angular Deviation for Trueness (Mean ± SD) in Degrees (°) | |||
|---|---|---|---|
| ISBs | DIOS (n = 15) | DPG (n = 15) | p Value |
| LFP | 1.682 ± 0.205 b | 0.586 ± 0.088 a | <0.001 |
| LLI | 1.907 ± 0.234 c | 0.346 ± 0.038 a | <0.001 |
| RLI | 1.496 ± 0.142 | 1.293 ± 0.068 | 0.398 |
| RFP | 1.890 ± 0.293 b | 0.672 ± 0.081 a | <0.001 |
| Global | 1.744 ± 0.175 b | 0.724 ± 0.064 a | <0.001 |
| p value | <0.001 | <0.001 | |
| RLI < LFP < LLI = RFP | LLI < LFP < RFP < RLI | ||
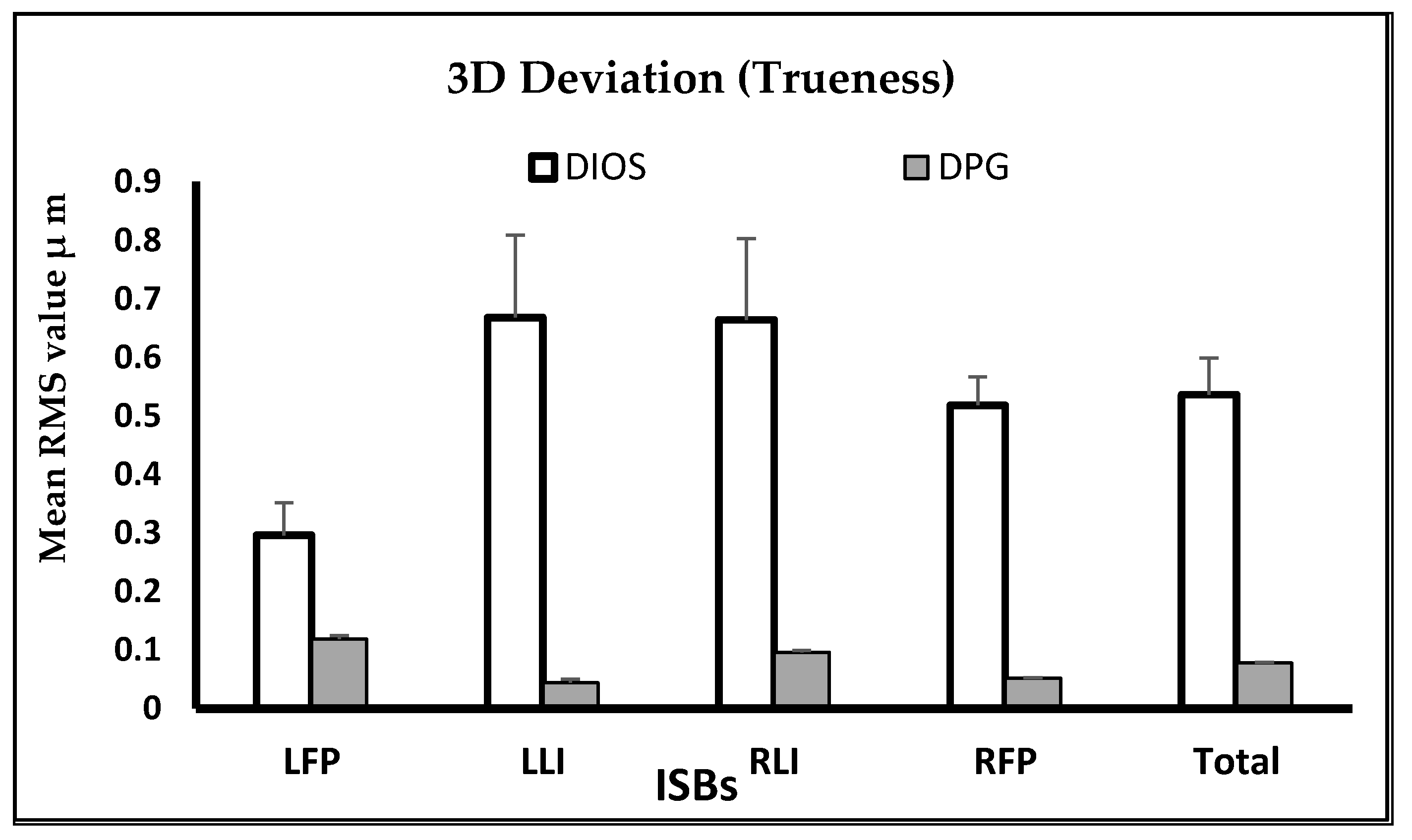
| RMS 3D ISBs Deviation for Precision (Mean ± SD) | |||
|---|---|---|---|
| ISBs | DIOS (n = 15) | DPG (n = 15) | p Value |
| LFP | 0.042 ± 0.020 a | 0.019 ± 0.015 a | <0.001 |
| LLI | 0.042 ± 0.016 a | 0.020 ± 0.021 a | <0.001 |
| RLI | 0.032 ± 0.007 a | 0.009 ± 0.007 a | <0.001 |
| RFP | 0.043 ± 0.012 b | 0.010 ± 0.014 a | <0.001 |
| Global | 0.039 ± 0.009 b | 0.014 ± 0.013 a | <0.001 |
| p value | 0.615 | 0.666 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tohme, H.; Lawand, G.; Eid, R.; Ahmed, K.E.; Salameh, Z.; Makzoume, J. Accuracy of Implant Level Intraoral Scanning and Photogrammetry Impression Techniques in a Complete Arch with Angled and Parallel Implants: An In Vitro Study. Appl. Sci. 2021, 11, 9859. https://doi.org/10.3390/app11219859
Tohme H, Lawand G, Eid R, Ahmed KE, Salameh Z, Makzoume J. Accuracy of Implant Level Intraoral Scanning and Photogrammetry Impression Techniques in a Complete Arch with Angled and Parallel Implants: An In Vitro Study. Applied Sciences. 2021; 11(21):9859. https://doi.org/10.3390/app11219859
Chicago/Turabian StyleTohme, Hani, Ghida Lawand, Rita Eid, Khaled E. Ahmed, Ziad Salameh, and Joseph Makzoume. 2021. "Accuracy of Implant Level Intraoral Scanning and Photogrammetry Impression Techniques in a Complete Arch with Angled and Parallel Implants: An In Vitro Study" Applied Sciences 11, no. 21: 9859. https://doi.org/10.3390/app11219859
APA StyleTohme, H., Lawand, G., Eid, R., Ahmed, K. E., Salameh, Z., & Makzoume, J. (2021). Accuracy of Implant Level Intraoral Scanning and Photogrammetry Impression Techniques in a Complete Arch with Angled and Parallel Implants: An In Vitro Study. Applied Sciences, 11(21), 9859. https://doi.org/10.3390/app11219859