
Designing and Analyzing 3D-Printed Personal Steering Controller for Outdoor Electric-Powered Wheelchair Users: A Randomized Controlled Trial on Stroke Patients



Abstract
:Featured Application
Abstract
1. Introduction
2. Methods and Technologies
2.1. Research Design and Procedures
2.2. Participants
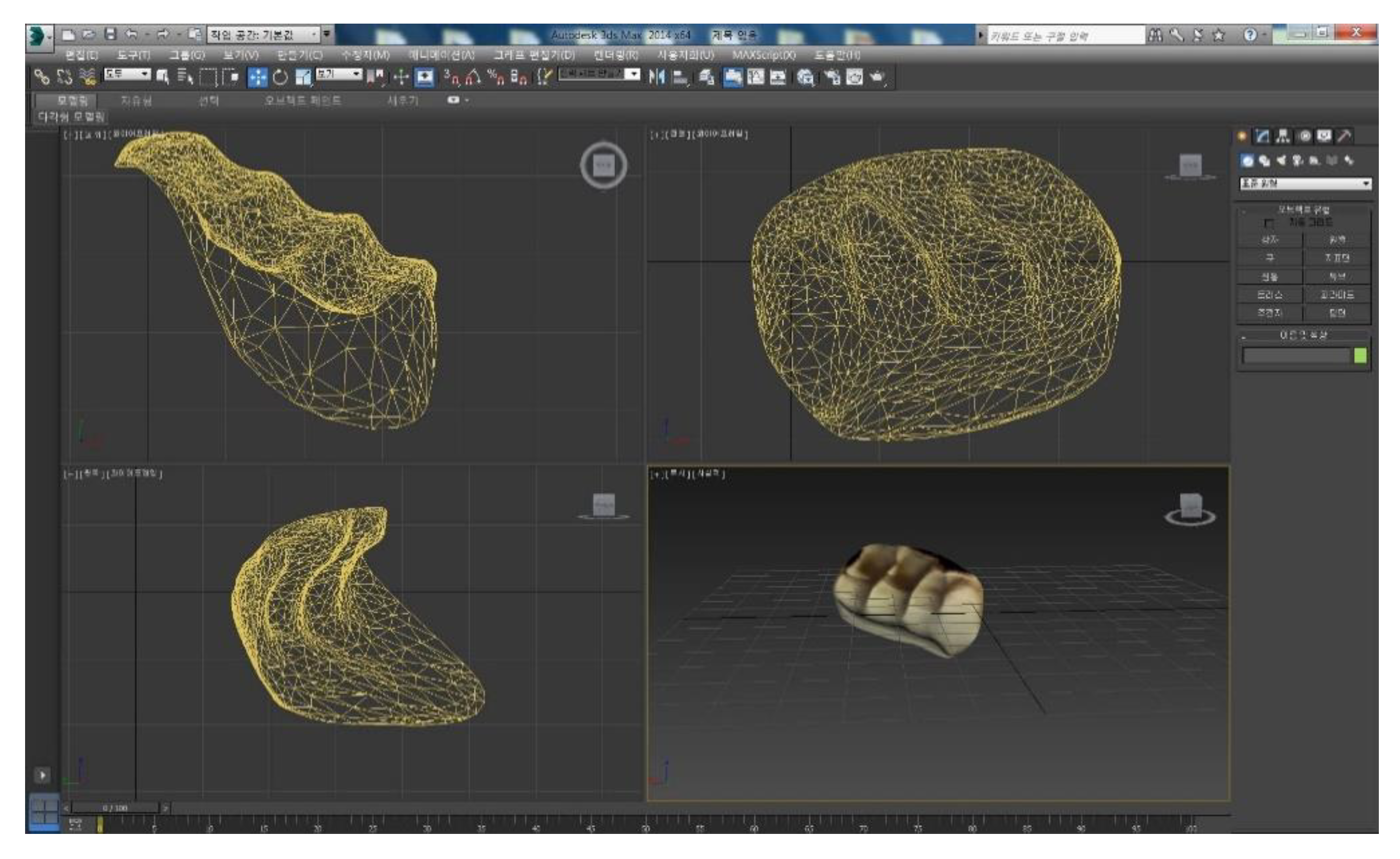
2.3. Designing and 3D-Printing the 3DSC
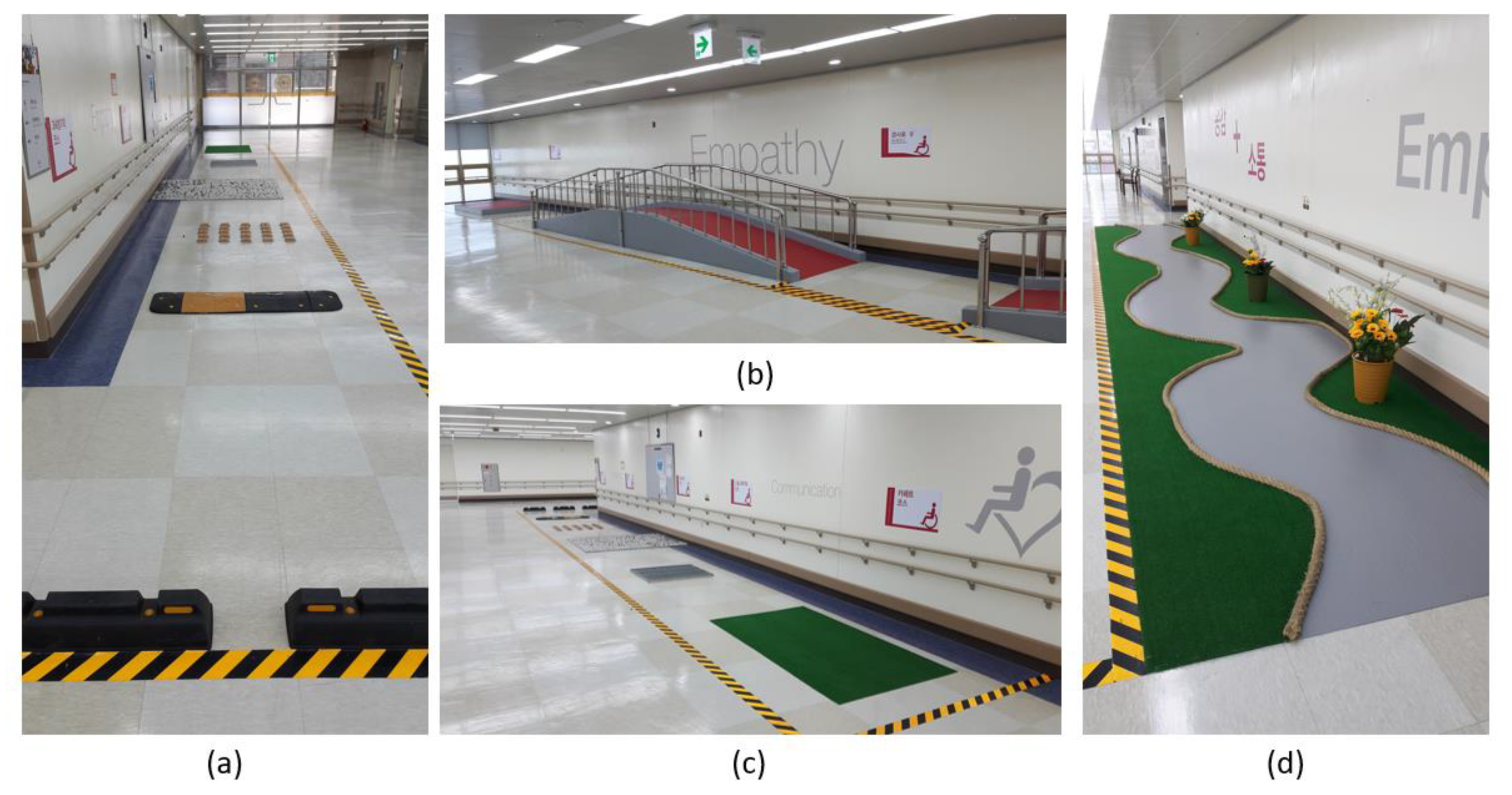
2.4. Driving Test Modules
2.5. Clinical Evaluation Tools
2.5.1. sEMG
2.5.2. WST
2.5.3. Assistive Device Satisfaction Part of the Korean Version of QUEST 2.0
2.6. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cook, A.M.; Polgar, J.M. Cook and Hussey’s Assistive Technologies-E-Book: Principles and Practice; Elsevier Health Sciences: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Choi, B.G. Designing and Manufacturing of Custom-Made Joystick Handles for Improvement in Control Ability of Power Wheelchairs: Using 3D Printing Technology. Master’s Thesis, Daegu University, Qingshan City, Korea, 2015. [Google Scholar]
- Fehr, L.; E Langbein, W.; Skaar, S.B. Adequacy of power wheelchair control interfaces for persons with severe disabilities: A clinical survey. J. Rehabil. Res. Dev. 2000, 37, 353–360. [Google Scholar]
- Rao, R.; Seliktar, R.; Rahman, T. Evaluation of an isometric and a position joystick in a target acquisition task for individuals with cerebral palsy. IEEE Trans. Rehabil. Eng. 2000, 8, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Bigongiari, A.; Souza, F.D.A.E.; Franciulli, P.M.; Neto, S.E.R.; Araújo, R.C.; Mochizuki, L. Anticipatory and compensatory postural adjustments in sitting in children with cerebral palsy. Hum. Mov. Sci. 2011, 30, 648–657. [Google Scholar] [CrossRef] [PubMed]
- De Souza, L.H.; Frank, A.O. Clinical features of electric powered indoor/outdoor wheelchair users with spinal cord injuries: A cross-sectional study. Assist. Technol. 2018, 32, 117–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pettersson, I.; Törnquist, K.; Ahlström, G. The effect of an outdoor powered wheelchair on activity and participation in users with stroke. Disabil. Rehabil. Assist. Technol. 2006, 1, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Hurd, W.J.; Morrow, M.M.B.; Kaufman, K.R.; An, K.-N. Wheelchair propulsion demands during outdoor community ambulation. J. Electromyogr. Kinesiol. 2009, 19, 942–947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, C.-Y.; Kim, H.J.; Lim, D. New wearable exoskeleton for gait rehabilitation assistance integrated with mobility system. Int. J. Precis. Eng. Manuf. 2016, 17, 957–964. [Google Scholar] [CrossRef]
- Heo, S.Y. A Study on the Case of Developing Manufacturing Techniques for Orthosis Using 3D Printing Technology: Focusing on Comparative Study with Using the Splint Pan. Disabil. Employ. 2015, 25, 79–103. [Google Scholar]
- Mahajan, H.P.; Spaeth, N.M.; Dicianno, B.E.; Brown, K.; Cooper, R.A. Preliminary evaluation of variable compliance joystick for people with multiple sclerosis. J. Rehabil. Res. Dev. 2014, 51, 951–962. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, V.T.; Sentouh, C.; Pudlo, P.; Popieul, J.-C. Path Following Controller for Electric Power Wheelchair Using Model Predictive Control and Transverse Feedback Linearization. In Proceedings of the 2018 IEEE International Conference on Systems, Man, and Cybernetics (SMC), Miyazaki, Japan, 7–10 October 2018; pp. 4319–4325. [Google Scholar]
- Demers, L.; Weiss-Lambrou, R.; Ska, B. Item Analysis of the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST). Assist. Technol. 2000, 12, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Hwang, W.-J.; Hwang, S.; Chung, Y. Test-retest reliability of the Quebec user evaluation of satisfaction with assistive technology 2.0-Korean version for individuals with spinal cord injury. J. Phys. Ther. Sci. 2015, 27, 1291–1293. [Google Scholar] [CrossRef] [Green Version]
- Kendall, F.P.; McCreary, E.K.; Provance, P.G.; Rodgers, M.M.; Romani, W.A. Muscles: Testing and Testing and Function with Posture and Pain; LWW: Baltimore, MD, USA, 2005; ISBN 978-0-7817-4780-6. [Google Scholar]
- Smith, E.M.; Low, K.; Miller, W.C. Interrater and intrarater reliability of the wheelchair skills test version 4.2 for power wheelchair users. Disabil. Rehabil. 2018, 40, 678–683. [Google Scholar] [CrossRef] [Green Version]
- Jonkers, I.; Nuyens, G.; Seghers, J.; Nuttin, M.; Spaepen, A. Muscular effort in multiple sclerosis patients during powered wheelchair manoeuvres. Clin. Biomech. 2004, 19, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Vitiello, D.; Pochon, L.; Malatesta, D.; Girard, O.; Newman, C.J.; Degache, F. Walking-induced muscle fatigue impairs postural control in adolescents with unilateral spastic cerebral palsy. Res. Dev. Disabil. 2016, 53-54, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Vanlandewijck, Y.C.; Evaggelinou, C.; Daly, D.J.; Verellen, J.; Van Houtte, S.; Aspeslagh, V.; Hendrickx, R.; Piessens, T.; Zwakhoven, B. The relationship between functional potential and field performance in elite female wheelchair basketball players. J. Sports Sci. 2004, 22, 668–675. [Google Scholar] [CrossRef] [PubMed]
- Paulisso, D.C.; Schmeler, M.R.; Schein, R.M.; Allegretti, A.L.C.; Campos, L.C.B.; Costa, J.D.; Fachin-Martins, E.; Cruz, D.M.C. da Functional Mobility Assessment Is Reliable and Correlated with Satisfaction, Independence and Skills. Assist. Technol. 2019, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, M.S.; Chowdhury, Z.I.; Al Mamun, S.; Hussain, A.; Mahmud, M. A Neuro-Fuzzy Control System Based on Feature Extraction of Surface Electromyogram Signal for Solar-Powered Wheelchair. Cogn. Comput. 2016, 8, 946–954. [Google Scholar] [CrossRef] [Green Version]
- Jang, G.; Kim, J.; Lee, S.; Choi, Y. EMG-Based Continuous Control Scheme With Simple Classifier for Electric-Powered Wheelchair. IEEE Trans. Ind. Electron. 2016, 63, 3695–3705. [Google Scholar] [CrossRef]
- Moon, I.; Lee, M.; Chu, J.; Mun, M. Wearable EMG-Based HCI for Electric-Powered Wheelchair Users with Motor Disabilities. In Proceedings of the Proceedings of the 2005 IEEE International Conference on Robotics and Automation, Barcelona, Spain, 18–22 April 2005; pp. 2649–2654. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Subjects (n = 23) | ||
|---|---|---|---|
| Male (n = 14) n (%) or M ± SD | Female (n = 9) n (%) or M ± SD | ||
| Age | |||
| 40–49 | 5 (35.7) | 4 (44.4) | |
| 50–59 | 7 (50.0) | 4 (44.4) | |
| 60–65 | 2 (14.3) | 1 (11.1) | |
| Brunnstrom Stages | |||
| 4 | 8 (57.1) | 2 (22.2) | |
| 5 | 4 (28.6) | 6 (66.7) | |
| 6 | 2 (14.3) | 1 (11.1) | |
| Paretic Arm | |||
| Left | 3 (21.4) | 1 (11.1) | |
| Right | 9 (64.3) | 8 (88.9) | |
| Both | 2 (14.3) | 0 (0) | |
| Vascular Territories | |||
| ACA | 4 (28.6) | 2 (22.2) | |
| MCA | 9 (64.3) | 5 (55.6) | |
| PCA | 0 (0) | 1 (11.1) | |
| BA | 1 (7.1) | 1 (11.1) | |
| Stroke types | |||
| Hemorrhage | 4 (28.6) | 3 (33.3) | |
| Infarction | 10 (71.4) | 6 (66.7) | |
| MMSE-K | Score | 27.18 ± 1.47 | 26.17 ± 1.13 |
| Target Muscles | 3DSC | CSC | t | p |
|---|---|---|---|---|
| M ± SD | M ± SD | |||
| Male (n = 14) | ||||
| upper trapezius | 12.07 ± 2.96 | 11.14 ± 2.73 | −1.129 | 0.194 |
| deltoid middle part | 4.30 ± 1.34 | 5.12 ± 1.34 | −0.103 | 0.035 * |
| biceps brachii | 2.99 ± 0.73 | 3.74 ± 0.71 | −1.347 | 0.018 * |
| triceps brachii | 0.95 ± 0.31 | 1.21 ± 0.72 | −1.973 | 0.053 * |
| extensor carpi radialis longus | 2.21 ± 0.36 | 2.71 ± 1.19 | −1.703 | 0.019 * |
| Female (n = 9) | ||||
| upper trapezius | 9.21 ± 1.64 | 9.45 ± 2.11 | −0.314 | 0.621 |
| deltoid middle fiber | 3.10 ± 0.31 | 3.89 ± 1.65 | −0.183 | 0.762 |
| biceps brachii | 2.65 ± 0.63 | 2.83 ± 0.71 | −1.505 | 0.218 |
| triceps brachii | 0.89 ± 0.51 | 1.60 ± 1.03 | −2.109 | 0.019 * |
| extensor carpi radialis longus | 1.23 ± 0.34 | 2.95 ± 1.02 | −2.110 | 0.037 * |
| Outcome Assessment | 3DSC | CSC | z | p |
|---|---|---|---|---|
| M ± SD (n = 14) | M ± SD (n = 14) | |||
| Moves controller away and back | 2.00 ± 0.00 | 1.78 ± 0.57 | −1.440 | 0.150 |
| Selects drive modes and speeds | 1.78 ± 0.42 | 2.00 ± 0.00 | −1.800 | 0.072 |
| Operates body positioning options | 1.85 ± 0.36 | 1.85 ± 0.53 | −0.514 | 0.608 |
| Disengages and engages motors | 1.92 ± 0.26 | 1.57 ± 0.75 | −1.516 | 0.130 |
| Rolls forwards (10 m) | 1.85 ± 0.36 | 1.78 ± 0.57 | −0.076 | 0.940 |
| Rolls backwards (2 m) | 1.50 ± 0.51 | 1.85 ± 0.53 | −2.245 | 0.025 * |
| Turns while moving forwards (90°) | 2.00 ± 0.00 | 1.92 ± 0.26 | −1.000 | 0.317 |
| Turns while moving backwards (90°) | 1.85 ± 0.36 | 1.71 ± 0.61 | −0.552 | 0.581 |
| Turns in place (180°) | 2.00 ± 1.85 | 1.85 ± 0.36 | −1.441 | 0.150 |
| Maneuvers sideways (0.5 m) | 1.85 ± 0.36 | 0.85 ± 0.77 | −3.454 | 0.001 * |
| Gets through hinged door | 2.00 ± 0.00 | 1.92 ± 0.26 | −1.000 | 0.317 |
| Reaches high object (1.5 m) | 2.00 ± 0.00 | 1.64 ± 0.74 | −1.797 | 0.072 |
| Rolls 100 m | 1.92 ± 0.26 | 1.64 ± 0.63 | −1.484 | 0.138 |
| Avoids moving obstacles | 1.85 ± 0.36 | 1.55 ± 0.36 | −1.000 | 0.021 * |
| Ascends 5° incline | 2.00 ± 0.00 | 1.85 ± 0.36 | −1.441 | 0.150 |
| Descends 5° incline | 2.00 ± 0.00 | 1.35 ± 0.84 | −2.694 | 0.007 * |
| Ascends 10° incline | 2.00 ± 0.00 | 1.78 ± 0.57 | −1.440 | 0.150 |
| Descends 10° incline | 1.85 ± 0.36 | 1.17 ± 0.61 | −0.552 | 0.581 |
| Rolls across side-slope (5°) | 2.00 ± 0.00 | 1.64 ± 0.63 | −2.117 | 0.034 * |
| Rolls on soft surface (2 m) | 1.87 ± 0.36 | 1.64 ± 0.63 | −0.965 | 0.334 |
| Gets over gap (15 cm) | 1.64 ± 0.49 | 0.57 ± 0.64 | −3.601 | 0.000 * |
| Gets over threshold (2 cm) | 1.92 ± 0.26 | 1.85 ± 0.36 | −0.600 | 0.549 |
| Ascends low curb (5 cm) | 1.71 ± 0.46 | 1.21 ± 0.69 | −1.797 | 0.072 |
| Descends low curb (5 cm) | 2.00 ± 0.00 | 1.83 ± 0.21 | −2.021 | 0.043 * |
| WST total scores | 49.28 ± 2.19 | 42.85 ± 4.31 | −3.935 | 0.000 * |
| Outcome Assessment | 3DSC | CSC | z | p |
|---|---|---|---|---|
| M ± SD (n = 9) | M ± SD (n = 9) | |||
| Moves controller away and back | 1.89 ± 0.33 | 1.56 ± 0.73 | −1.156 | 0.248 |
| Selects drive modes and speeds | 1.78 ± 0.44 | 1.78 ± 0.44 | 0.000 | 1.000 |
| Operates body positioning options | 1.89 ± 0.33 | 1.78 ± 0.67 | −0.081 | 0.936 |
| Disengages and engages motors | 1.89 ± 0.33 | 1.56 ± 0.73 | −1.156 | 0.248 |
| Rolls forwards (10 m) | 1.89 ± 0.33 | 1.67 ± 0.71 | −0.680 | 0.496 |
| Rolls backwards (2 m) | 1.67 ± 0.50 | 1.44 ± 0.88 | −0.338 | 0.750 |
| Turns while moving forwards (90°) | 2.00 ± 0.00 | 1.89 ± 0.33 | −1.000 | 0.317 |
| Turns while moving backwards (90°) | 1.78 ± 0.44 | 1.56 ± 0.73 | −0.620 | 0.535 |
| Turns in place (180°) | 1.67 ± 0.71 | 1.67 ± 0.71 | 0.000 | 1.000 |
| Maneuvers sideways (0.5 m) | 1.81 ± 0.14 | 1.02 ± 0.67 | −1.910 | 0.026 * |
| Gets through hinged door | 1.89 ± 0.33 | 1.78 ± 0.44 | −0.615 | 0.539 |
| Reaches high object (1.5 m) | 2.00 ± 0.00 | 1.33 ± 0.87 | −1.837 | 0.029 * |
| Rolls 100 m | 1.78 ± 0.44 | 1.56 ± 0.53 | −0.511 | 0.331 |
| Avoids moving obstacles | 1.78 ± 0.44 | 0.72 ± 0.34 | −3.101 | 0.000 * |
| Ascends 5° incline | 2.35 ± 0.20 | 1.56 ± 0.73 | −1.458 | 0.066 |
| Descends 5° incline | 1.89 ± 0.33 | 1.56 ± 0.53 | −1.102 | 0.125 |
| Ascends 10° incline | 2.00 ± 0.00 | 1.33 ± 0.87 | −1.837 | 0.029 * |
| Descends 10° incline | 1.89 ± 0.33 | 1.56 ± 0.73 | −1.156 | 0.248 |
| Rolls across side-slope (5°) | 2.00 ± 0.00 | 1.56 ± 0.73 | −1.837 | 0.066 |
| Rolls on soft surface (2 m) | 1.89 ± 0.53 | 1.00 ± 0.87 | −1.627 | 0.015 * |
| Gets over gap (15 cm) | 1.67 ± 0.50 | 0.61 ± 0.71 | −2.692 | 0.007 * |
| Gets over threshold (2 cm) | 1.73 ± 0.41 | 1.67 ± 0.50 | −0.511 | 0.609 |
| Ascends low curb (5 cm) | 1.89 ± 0.33 | 1.21 ± 0.43 | −1.627 | 0.039 * |
| Descends low curb (5 cm) | 1.67 ± 0.50 | 1.22 ± 0.67 | −1.491 | 0.136 |
| WST total scores | 48.17 ± 0.44 | 41.11 ± 0.78 | −1.910 | 0.047 * |
| Subcategories | 3DSC | CSC | t | p |
|---|---|---|---|---|
| M ± SD (n = 23) | M ± SD (n = 23) | |||
| Male (n = 14) | ||||
| dimension | 2.50 ± 0.53 | 2.70 ± 0.87 | −1.00 | 0.317 |
| weight | 2.90 ± 0.88 | 3.40 ± 0.70 | −2.24 | 0.025 * |
| adjustments | 2.80 ± 0.79 | 2.00 ± 0.82 | −2.27 | 0.023 * |
| safety | 3.20 ± 0.78 | 1.70 ± 0.67 | −2.71 | 0.007 * |
| durability | 3.30 ± 0.82 | 2.60 ± 1.43 | −1.33 | 0.185 |
| easy to use | 3.90 ± 0.88 | 1.90 ± 0.81 | −2.62 | 0.009 * |
| comfortable | 3.80 ± 0.92 | 2.30 ± 0.67 | −2.60 | 0.008 * |
| effectiveness | 3.50 ± 0.85 | 2.40 ± 0.70 | −2.21 | 0.027 * |
| Female (n = 9) | ||||
| dimension | 2.91 ± 0.88 | 2.70 ± 0.87 | −2.62 | 0.009 * |
| weight | 1.90 ± 0.82 | 1.70 ± 0.63 | −1.79 | 0.196 |
| adjustments | 3.90 ± 0.75 | 2.10 ± 0.81 | −2.14 | 0.002 * |
| safety | 3.90 ± 0.82 | 2.70 ± 0.87 | −2.50 | 0.009 * |
| durability | 3.20 ± 0.78 | 2.60 ± 1.43 | −1.71 | 0.097 |
| easy to use | 3.70 ± 0.98 | 2.10 ± 0.81 | −2.18 | 0.017 * |
| comfortable | 3.80 ± 0.59 | 2.10 ± 0.61 | −2.97 | 0.003 * |
| effectiveness | 2.90 ± 0.51 | 2.11 ± 0.78 | −2.02 | 0.018 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heo, S.; Choi, W. Designing and Analyzing 3D-Printed Personal Steering Controller for Outdoor Electric-Powered Wheelchair Users: A Randomized Controlled Trial on Stroke Patients. Appl. Sci. 2021, 11, 2743. https://doi.org/10.3390/app11062743
Heo S, Choi W. Designing and Analyzing 3D-Printed Personal Steering Controller for Outdoor Electric-Powered Wheelchair Users: A Randomized Controlled Trial on Stroke Patients. Applied Sciences. 2021; 11(6):2743. https://doi.org/10.3390/app11062743
Chicago/Turabian StyleHeo, Seoyoon, and Wansuk Choi. 2021. "Designing and Analyzing 3D-Printed Personal Steering Controller for Outdoor Electric-Powered Wheelchair Users: A Randomized Controlled Trial on Stroke Patients" Applied Sciences 11, no. 6: 2743. https://doi.org/10.3390/app11062743