
Lower-Body Positive Pressure Treadmill Training for Pediatric Gait Disorders: A Scoping Review




Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source and Literature Source
2.2. Eligibility Criteria
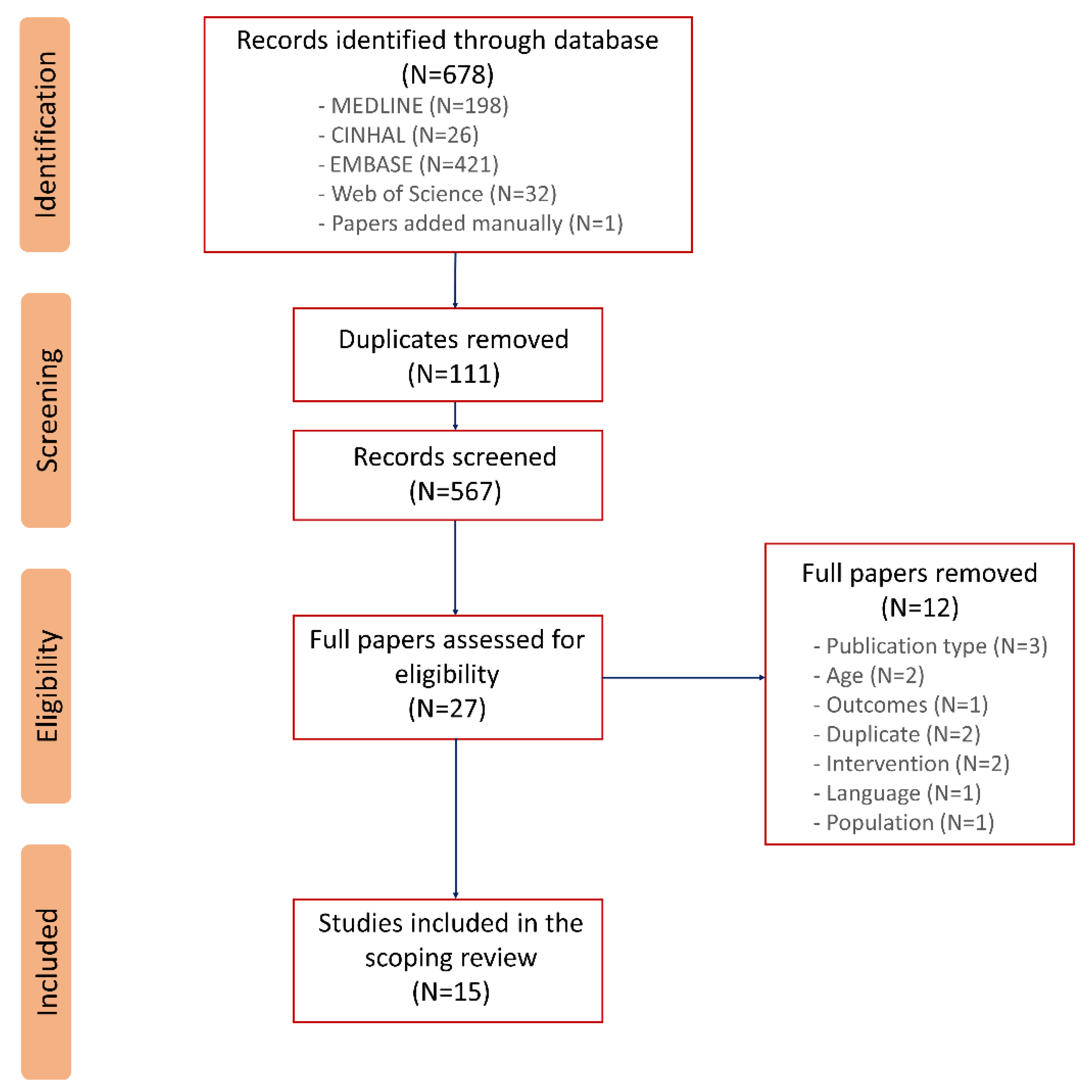
2.3. Study Screening
2.4. Quality Assessment
2.5. Outcome Variables
3. Results
3.1. Design and Quality of the Studies
3.2. Participant Characteristics
3.3. Training Protocols
3.4. Effect of Anti-Gravity Treadmill Training on Muscle Strength, Spasticity and Gross Motor Function
3.5. Effect of Anti-Gravity Treadmill Training on Balance
3.6. Effect of Anti-Gravity Treadmill Training on Gait Parameters

{kind=link}
| Studies | Study Design | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total (/10) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Kurz et al. [16] | Before/After | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 3 (low) |
| Emara [21] | RCT | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 (high) |
| Emara [22] | RCT | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 (high) |
| Birgani et al. [26] | Case study | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 2 (low) |
| El-Shamy [11] | RCT | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 8 (high) |
| Rasooli et al. [27] | Multiple case studies | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 2 (low) |
| Lotfian et al. [23] | Multiple case studies | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 (low) |
| Azizi et al. [28] | RCT | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 3 (low) |
| Azizi et al. [29] | Multiple case studies | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 2 (low) |
| Azizi et al. [30] | Multiple case studies | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 2 (low) |
| Dadashi et al. [31] | Controlled cases study | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 2 (low) |
| Azizi et al. [15] | RCT | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 4 (low) |
| Lotfian et al. [32] | Before/After | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 (low) |
| Aras et al. [25] | RCT | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 (high) |
| Noroozi et al. [24] | NECG | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 (low) |
| Study | Participant Characteristics | Intervention | Outcomes of Interest | ICF Domains | Results | ||
|---|---|---|---|---|---|---|---|
| Experimental Group | Control Group | Anti-Gravity Training | Comparator Training | ||||
| Kruz et al. [27] | 9 children with CP | - | Anti-gravity training (2 participants continued conventional therapy) | - | Isometric muscle strength; spatiotemporal parameters; balance (BESTest) | Body function and activity | A significant improvement in the overall strength of the lower extremity, walking speed, time spent in the double support and BESTest scores after anti-gravity training. |
| (age = 8 to 18 yrs; GMFCS II–V) | |||||||
| Emara et al. [18] | 15 children with hemophilic knee arthritis | 15 children with hemophilic knee arthritis | Anti-gravity training + stretching and strengthening exercise | Stretching and strengthening exercises | Concentric muscle strength (hamstrings and quadriceps); balance | Body function and activity | Peak torque of the quadriceps and peak torque of the hamstring increased in the control and anti-gravity group. Both groups demonstrated a significant increase in balance. Greater improvements were in favor of the anti-gravity group. |
| Age = 8 to 11 yrs | |||||||
| Emara et al. [19] | 15 spastic diplegic CP | 15 spastic diplegic CP | Anti-gravity training + the same exercise program given to control group | Personalized therapeutic exercise program | Dynamic postural control (AP stability and M-L stability; overall stability/index) | Activity | A greater stability index was observed after anti-gravity training compared with the control group. |
| Age = 6 to 8 yrs | |||||||
| Birgani et al. [29] | 1 hemiplegic CP child | - | Anti-gravity training | - | Balance and postural stability based on the COP | Activity | The surface of COP signal decreased after training. |
| El-Shamy [11] | 15 spastic diplegic CP | 15 spastic diplegic CP | Anti-gravity and conventional therapy | Conventional physical therapy program | Gait spatiotemporal parameters, postural stability, fall risk | Activity | Anti-gravity group exhibited greater improvements in terms of spatiotemporal parameters, stability index and fall risk compared to the control group. |
| Age = 8 to 12 yrs; GMFCS I–II | |||||||
| Rasooli et al. [21] | 3 children with spastic hemiplegic CP | 1 child with spastic hemiplegic CP | Anti-gravity training | Over-ground gait training | Postural stability (posturography) | Activity | The results of the posturography evaluations showed a consistent improvement in postural stability in both groups. |
| Age = 6 to 12 yrs; GMFCS I–III | |||||||
| Lotfian et al. [28] | 4 children with CP | - | Anti-gravity training | - | Isometric strength, RFD, AROM, spatiotemporal gait parameters | Body function and activity | Ankle and knee isometric strength and RFD isokinetic strength increased after anti-gravity training. Ankle AROM increased with training. Walking speed and step width and length increased after anti-gravity training. |
| Age = 9 to 13 yrs, GMFCS II–III | |||||||
| Azizi et al. [22] | 3 children with spastic hemiplegic | 1 child with spastic hemiplegic | Anti-gravity training | OT focused on walking capacity | Walking speed (10MWT) and dynamic balance (TUG) | Activity | Walking speed increased by between 26 and 82 % after anti-gravity training, whereas it was limited to 35% for the control subject. The change in TUG was relatively small. |
| Age = 4 to 12 yrs | |||||||
| Azizi et al. [30] | 3 children with CP | - | Anti-gravity training | - | Walking speed (10MWT), dynamic balance (TUG), endurance (6MWT) | Activity | All cases increased their walking speed, decreased the time recorded in TUG and increased the distance during 6MWT after anti-gravity training. |
| Age = 9 to 12 yrs | |||||||
| Azizi et al. [31] | 3 children with CP | - | Anti-gravity training | - | Balance using the BBS and TUG | Activity | The time in TUG decreased by up to 30% and the Berg index increased by up to 30% for all patients after anti-gravity training. |
| Age = 9 to 12 yrs | |||||||
| Dadashi et al. [23] | 2 children with hemiplegic CP | 2 children with hemiplegic CP | Anti-gravity training | OT focused on walking capacity | Dynamic balance (center-of-mass and center-of-pressure displacements) | Activity | Dynamic balance improved after anti-gravity training. The changes were greater after anti-gravity training compared to control training. |
| Age = 4 to 14 yrs | |||||||
| Azizi et al. [24] | 9 children with CP | 5 children with CP | Anti-gravity training | OT focused on walking capacity | Walking speed (10MWT), dynamic balance (TUG), endurance (6MWT) | Activity | Improvements in walking speed and endurance, measured by 10MWT and 6MWT, were statistically greater in the anti-gravity group than in the control group. |
| Age = 4 to 15 yrs | |||||||
| Lotfian et al. [25] | 7 children with CP | 4 children with CP | Anti-gravity training | OT focused on walking capacity | Gait spatiotemporal parameters, dynamic balance (COP and COM displacement), clinical measures (10MWT, TUG, 6MWT) | Activity | Walking speed, cadence and single-support time increased by 98%, 10% and 65%, respectively. Clinical measures increased by 26% (10MWT), 18% (TUG) and 20% (6MWT) after anti-gravity training. Dynamic balance improved after anti-gravity training. All the changes were greater after anti-gravity training compared to control training. |
| GMFCS = I–II | |||||||
| Aras et al. [20] | 10 children with CP (one withdrawn) | 10 children with CP in robotic group and 10 children with CP in BWS training group | Anti-gravity training | A group allocated for BWS treadmill training and a group allocated for robotic training | Gait spatiotemporal parameters, walking endurance (6MWT), GMFM-66 | Activity | Walking speed increased in the three groups but did not reach statistical significance. After anti-gravity training, the increase in cadence, stride length, and stride time were statistically significant. The decrease in the double-support phase was statistically significant in the anti-gravity and robotic groups. GFMF-D, GMFM-E and 6MWT increased similarly in all the groups. |
| Age = 6 to 14 yrs; GMFCS II–III | |||||||
| Noroozi et al. [33] | 9 children with hemiplegic CP (1 withdrawn) | 9 children with hemiplegic CP (1 withdrawn) | Anti-gravity training | OT focused on walking capacity | Ankle dorsiflexion spasticity by assessment of reflex stiffness gain and intrinsic stiffness gain | Body function | Intrinsic stiffness gain and reflex stiffness gain parameters decreased substantially following anti-gravity training. The changes were greater than those observed in the control group. |
| Age = 4 to 14 yrs | |||||||
| Study | Training Parameters | Anti-Gravity Treadmill Settings |
|---|---|---|
| Kruz et al. [27] | 30 min per session, 2 times per week for 6 weeks | BWS was set to 40% of body weight and gradually reduced to 10% by the end of the intervention. The speed of the treadmill was initially set at 90% of the child’s over-ground walking speed and gradually increased. |
| Emara et al. [18] | 20 min per session, 3 times per week for 12 weeks | BWS was set at 30% of the child’s body weight. The speed of the tredmill was set at 75% of over-ground speed and zero-degree inclination. |
| Emara et al. [19] | 20 min per session, 3 times per week for 12 weeks | Comfortable treadmill speed was selected for all participants as 75% of their comfortable speed during over-ground walking. The treadmill was set at zero-degree inclination. |
| Birgani et al. [29] | 45 min per session, 3 times per week for 8 weeks. | The training started with a 50% BWS and with a speed of 1.5 km/h. Then, BWS was gradually reduced and the speed was increased based on the subject’s ability. |
| El-Shamy [11] | 20 min per session added to 1 h of conventional therapy, 3 times per week for 12 weeks | The treadmill was set at zero-degree inclination. Comfortable treadmill speed was selected for all participants as 75% of their comfortable speed during over-ground walking. Verbal commands were given to the children to maintain upright posture. |
| Rasooli et al. [21] | 45 min per session, 3 times per week for 8 weeks | Each session, training started with 50–70% of body-weight support and 0.7–1.5 km/h speed, depending on the patient’s condition and tolerance. After warmup, the body-weight support decreased and speed increased gradually based on the therapist’s evaluation of the patient’s tolerance. |
| Lotfian et al. [28] | 45 min per session, 3 times per week for 8 weeks | BWS was set at 50%, and the speed of the treadmill was started at about 1 m/s. After a 3 to 4 min warmup, the experienced trainer began to reduce the BWS and increase the speed, changing them during training based on the patient’s needs. |
| Azizi et al. [21] | 45 min per session, 3 times per week for 8 weeks | No information about anti-gravity treadmill settings. |
| Azizi et al. [30] | 45 min per session, 3 times per week for 8 weeks | The inclination was set at 0°. The speed and BWS of the treadmill were set to their optimum level, at which patients had their best gait pattern. |
| Azizi et al. [31] | 45 min per session, 3 times per week for 8 weeks | The inclination was set at 0°. These parameters were set to the levels at which the patient had the best walking pattern. The primary speed and BWS of each session were dependent on the condition of the patient and were set to 0.7–1.5 km/h and 50–70% of the normal weight, respectively. |
| Dadashi et al. [23] | 45 min per session, 3 times per week for 8 weeks | At first, the BWS was set at 50% of the participant’s weight, and the speed was set at about 1 m/s. As time passed, the speed increased, and the BWS gradually decreased. |
| Azizi et al. [24] | 45 min per session, 3 times per week for 8 weeks | The treadmill was set at zero-degree inclination, the initial speed was set to 0.7 km/h and the body-weight support was selected according to gait patterns. |
| Lotfian et al. [25] | 45 min per session, 3 times per week for 8 weeks | At the beginning of the training session, BWS was reduced by 50%, and the patient was allowe to walk at a low speed to warm up. After 4–5 min, the BWS was gradually decreased, while the speed was increased; the trainer adjusted these two parameters to help the subject maintain a more accurate walking pattern. |
| Aras et al. [20] | 45 min per session, 5 times per week for 4 weeks | BWS was started at 60% and gradually decreased to a level that prevented the collapse of the knee in flexion during the stance phase. The treadmill speed was initiated at the average walking speed according to the child’s walking pattern, weigh and endurance, then increased to the highest level tolerated. |
| Noroozi et al. [33] | 40 min per session, 3 times per week for 8 weeks | No information about anti-gravity treadmill settings. |
4. Discussion
4.1. Participant Characteristics
4.2. Anti-Gravity Training: Protocols and Settings
4.3. Effect of Training on Body Functions
4.4. Effect of Anti-Gravity Training on Activity
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cherni, Y.; Laforte, A.P.; Parent, A.; Marois, P.; Begon, M.; Ballaz, L. Lower limb extension is improved in fast walking condition in children who walk in crouch gait. Disabil. Rehabilitation 2019, 41, 3210–3215. [Google Scholar] [CrossRef] [PubMed]
- Duffy, C.M.; Hill, A.E.; Cosgrove, A.P.; Carry, I.S.; Graham, H.K. Energy Consumption in children with spina bifida and cerebral palsy: A comparative study. Dev. Med. Child Neurol. 2008, 38, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.J.; Son, S.M. Comparison of Spatiotemporal Gait Parameters between Children with Normal Development and Children with Diplegic Cerebral Palsy. J. Phys. Ther. Sci. 2014, 26, 1317–1319. [Google Scholar] [CrossRef] [PubMed]
- Pirpiris, M.; Gates, P.E.; McCarthy, J.J.; D’Astous, J.; Tylkowksi, C.; Sanders, J.O.; Dorey, F.J.; Ostendorff, S.; Robles, G.; Caron, C.; et al. Function and well-being in ambulatory children with cerebral palsy. J. Pediatr. Orthop. 2006, 26, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Marino, F.R.; Lessard, D.M.; Saczynski, J.S.; McManus, D.D.; Silverman-Lloyd, L.G.; Benson, C.M.; Blaha, M.J.; Waring, M.E. Gait speed and mood, cognition, and quality of life in older adults with atrial fibrillation. J. Am. Hear. Assoc. 2019, 8, e013212. [Google Scholar] [CrossRef] [PubMed]
- Zwicker, J.G.; Mayson, T.A. Effectiveness of treadmill training in children with motor impairments: An overview of systematic reviews. Pediatr. Phys. Ther. 2010, 22, 361–377. [Google Scholar] [CrossRef]
- Novak, I.; McIntyre, S.; Morgan, C.; Campbell, L.; Dark, L.; Morton, N.; Stumbles, E.; Wilson, S.-A.; Goldsmith, S. A systematic review of interventions for children with cerebral palsy: State of the evidence. Dev. Med. Child Neurol. 2013, 55, 885–910. [Google Scholar] [CrossRef]
- Cutuk, A.; Groppo, E.R.; Quigley, E.J.; White, K.W.; Pedowitz, R.A.; Hargens, A.R. Ambulation in simulated fractional gravity using lower body positive pressure: Cardiovascular safety and gait analyses. J. Appl. Physiol. 2006, 101, 771–777. [Google Scholar] [CrossRef]
- Patil, S.; Steklov, N.; Bugbee, W.D.; Goldberg, T.; Colwell, C.W.; D’Lima, D.D. Anti-gravity treadmills are effective in reducing knee forces. J. Orthop. Res. 2012, 31, 672–679. [Google Scholar] [CrossRef]
- de Heer, H.D.; Kline, J.R.; Charley, B. Anti-Gravity Treadmill Training for Prevention and Rehabilitation of Running Injuries. In Clinical Care of the Runner; Harrast, M.A., Ed.; Elsevier BV: Amsterdam, The Netherlands, 2020; pp. 113–130. [Google Scholar]
- El-Shamy, S. Effects of Antigravity Treadmill training on gait, balance, and fall risk in children with diplegic cerebral palsy. Am. J. Phys. Med. Rehab. 2017, 96, 809–815. [Google Scholar] [CrossRef]
- Draovitch, P.; Maschi, R.A.; Hettler, J. Return to sport following hip injury. Curr. Rev. Musculoskelet. Med. 2012, 5, 9–14. [Google Scholar] [CrossRef]
- Peeler, J.; Ripat, J. The effect of low-load exercise on joint pain, function, and activities of daily living in patients with knee osteoarthritis. Knee 2018, 25, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.D.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. Int. J. Evid. Based Health 2015, 13, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Functioning, Disability and Health: Children and Youth Version: ICF-CY; World Health Organization: Geneva, Switzerland, 2007; Available online: https://apps.who.int/iris/handle/10665/43737 (accessed on 29 November 2021).
- Emara, H. The Role of Antigravity Treadmill in Haemophilic Children Aged 8 to 11 Years with Unilateral Knee Haemarthrosis without Radiological Involvement. Br. J. Med. Med. Res. 2015, 10, 1–10. [Google Scholar] [CrossRef]
- Emara, H.A.M.A.H. Effect of a new physical therapy concept on dynamic balance in children with spastic diplegic cerebral palsy. Egypt. J. Med. Hum. Genet. 2015, 16, 77–83. [Google Scholar] [CrossRef][Green Version]
- Aras, B.; Yaşar, E.; Kesikburun, S.; Türker, D.; Tok, F.; Yılmaz, B. Comparison of the effectiveness of partial body weight-supported treadmill exercises, robotic-assisted treadmill exercises, and anti-gravity treadmill exercises in spastic cerebral palsy. Turk. J. Phys. Med. Rehabil. 2019, 65, 361–370. [Google Scholar] [CrossRef]
- Rasooli, A.H.; Birgani, P.M.; Azizi, S.; Shahrokhi, A.; Mirbagheri, M.M. Therapeutic effects of an anti-gravity locomotor training (AlterG) on postural balance and cerebellum structure in children with Cerebral Palsy. In Proceedings of the 2017 International Conference on Rehabilitation Robotics (ICORR), London, UK, 17–20 July 2017; Volume 2017, pp. 101–105. [Google Scholar] [CrossRef]
- Azizi, S.; Marzbani, H.; Raminfard, S.; Birgani, P.; Rasooli, A.; Mirbagheri, M.M. The impact of an anti-gravity treadmill (AlterG) training on walking capacity and corticospinal tract structure in children with cerebral palsy. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju, Korea, 11–15 July 2017; pp. 1150–1153. [Google Scholar] [CrossRef]
- Dadashi, F.; Kharazi, M.R.; Lotfian, M.; Shahroki, A.; Mirbagheri, A.; Mirbagheri, M.M. The Effects of Lower Body Positive Pressure Treadmill Training on Dynamic Balance of Children with Cerebral Palsy. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; Volume 2018, pp. 2487–2490. [Google Scholar] [CrossRef]
- Azizi, S.; Birgani, P.M.; Irani, A.; Shahrokhi, A.; Nourian, R.; Mirbagheri, M. Impact of anti-gravity locomotion (AlterG) training on structure and function of corticospinal tract and gait in children with cerebral palsy. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; Volume 2019, pp. 126–129. [Google Scholar] [CrossRef]
- Lotfian, M.; Dadashi, F.; Rafieenazari, Z.; Shahroki, A.; Rasteh, M.; Molavi, M.; Mirbagheri, A.; Mirbagheri, M. The Effects of Anti-gravity Treadmill Training on Gait Characteristics in Children with Cerebral Palsy. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; Volume 2019, pp. 5256–5259. [Google Scholar] [CrossRef]
- Noroozi, S.; Mehrabi, R.; Lotfian, M.; Nooshiravan, F.; Shahroki, A.; Irani, A.; Mirbagheri, M.M. Therapeutic Effects of an Anti-Gravity Treadmill (AlterG) Training on Neuromuscular Abnormalities Associated with Spasticity in Children with Cerebral Palsy*. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; Volume 2020, pp. 3856–3859. [Google Scholar] [CrossRef]
- Kurz, M.J.; Corr, B.; Stuberg, W.; Volkman, K.; Smith, N. Evaluation of Lower Body Positive Pressure Supported Treadmill Training for Children with Cerebral Palsy. Pediatr. Phys. Ther. 2011, 23, 232–239. [Google Scholar] [CrossRef]
- Lotfian, M.; Kharazi, M.R.; Mirbagheri, A.; Dadashi, F.; Nourian, R.; Mirbagheri, M.M. Therapeutic effects of an anti-gravity treadmill (AlterG) training on gait and lower limbs kinematics and kinetics in children with cerebral palsy. In Proceedings of the 2017 International Conference on Rehabilitation Robotics (ICORR), London, UK, 17–20 July 2017; Volume 2017, pp. 170–174. [Google Scholar] [CrossRef]
- Birgani, P.M.; Ashtiyani, M.; Rasooli, A.; Shahrokhnia, M.; Shahrokhi, A.; Mirbagheri, M. Can an anti-gravity treadmill improve stability of children with cerebral palsy? In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; Volume 2016, pp. 5465–5468. [Google Scholar] [CrossRef]
- Azizi, S.; Birgani, P.M.; Marzbani, H.; Nourian, R.; Kohanpour, M.; Mirbagheri, M.M. Assessment of neuroplasticity of corticospinal tract induced by antigravity treadmill (AlterG) in cerebral palsy children. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; Volume 2018, pp. 2495–2498. [Google Scholar] [CrossRef]
- Azizi, S.; Rasooli, A.H.; Soleimani, M.; Irani, A.; Shahrokhi, A.; Mirbagheri, M.M. The impact of AlterG training on balance and structure of vestibulospinal tract in cerebral palsy children. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–22 July 2018; pp. 2499–2502. [Google Scholar] [CrossRef]
- E Hanna, S.; Bartlett, D.J.; Rivard, L.M.; Russell, D.J. Reference Curves for the Gross Motor Function Measure: Percentiles for Clinical Description and Tracking Over Time Among Children with Cerebral Palsy. Phys. Ther. 2008, 88, 596–607. [Google Scholar] [CrossRef]
- Fowler, E.G.; Kolobe, T.H.; Damiano, D.L.; E Thorpe, D.; Morgan, D.W.; Brunstrom, J.E.; Coster, W.J.; Henderson, R.C.; Pitetti, K.H.; Rimmer, J.H.; et al. Stevenson, Section on Pediatrics Research Summit Participants, Section on Pediatrics Research Committee Task Force, Promotion of physical fitness and prevention of secondary conditions for children with cerebral palsy: Section on pediatrics research summit proceedings. Phys. Ther. 2007, 87, 1495–1510. [Google Scholar] [CrossRef]
- Kleim, J.A.; Jonest, T. Principles of Experience-Dependent Neural Plasticity: Implications for Rehabilitation after Brain Damage. J. Speech Lang. Heart Res. 2008, 51, S225–S239. [Google Scholar] [CrossRef]
- Verschuren, O.; Peterson, M.D.; Balemans, A.C.; Hurvitz, E.A. Exercise and physical activity recommendations for people with cerebral palsy. Dev. Med. Child Neurol. 2016, 58, 798–808. [Google Scholar] [CrossRef] [PubMed]
- Van Kammen, K.; Boonstra, A.; Reinders-Messelink, H.; Otter, R.D. The Combined Effects of Body Weight Support and Gait Speed on Gait Related Muscle Activity: A Comparison between Walking in the Lokomat Exoskeleton and Regular Treadmill Walking. PLoS ONE 2014, 9, e107323. [Google Scholar] [CrossRef]
- Cherni, Y.; Hajizadeh, M.; Maso, F.D.; Turpin, N.A. Effects of body weight support and guidance force settings on muscle synergy during Lokomat walking. Eur. J. Appl. Physiol. 2021, 121, 2967–2980. [Google Scholar] [CrossRef]
- Werner, C.; Lindquist, A.R.; Bardeleben, A.; Hesse, S. The Influence of Treadmill Inclination on the Gait of Ambulatory Hemiparetic Subjects. Neurorehabilit. Neural Repair 2007, 21, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Liang, Y.; Kang, X.; Shao, M.; Siemelink, L.; Zhang, Y. Gait Characteristics of Children with Spastic Cerebral Palsy during Inclined Treadmill Walking under a Virtual Reality Environment. Appl. Bionics Biomech. 2019, 2019. [Google Scholar] [CrossRef] [PubMed]
- Willerslev-Olsen, M.; Petersen, T.H.; Farmer, S.; Nielsen, J.B. Gait training facilitates central drive to ankle dorsiflexors in children with cerebral palsy. Brain 2015, 138, 589–603. [Google Scholar] [CrossRef] [PubMed]
- Warken, B.; Graser, J.V.; Ulrich, T.; Borggraefe, I.; Heinen, F.; Meyer-Heim, A.; van Hedel, H.J.A.; Schroeder, A.S.; Aurich, T. Practical Recommendations for Robot-Assisted Treadmill Therapy (Lokomat) in Children with Cerebral Palsy: Indications, Goal Setting, and Clinical Implementation within the WHO-ICF Framework. Neuropediatrics 2015, 46, 248–260. [Google Scholar] [CrossRef]
- Ross, S.A.; Engsberg, J.R. Relationships between spasticity, strength, gait, and the GMFM-66 in persons with spastic diplegia cerebral palsy. Arch. Phys. Med. Rehab. 2007, 88, 1114–1120. [Google Scholar] [CrossRef]
- Bar-On, L.; Molenaers, G.; Aertbeliën, E.; Monari, D.; Feys, H.; Desloovere, K. The relation between spasticity and muscle behavior during the swing phase of gait in children with cerebral palsy. Res. Dev. Disabil. 2014, 35, 3354–3364. [Google Scholar] [CrossRef]
- Dallmeijer, A.J.; Rameckers, E.A.; Houdijk, H.; de Groot, S.; Scholtes, V.A.; Becher, J.G. Isometric muscle strength and mobility capacity in children with cerebral palsy. Disabil. Rehab. 2017, 39, 135–142. [Google Scholar] [CrossRef]
- Ferland, C.; Lepage, C.; Moffet, H.; Maltais, D.B. Relationships Between Lower Limb Muscle Strength and Locomotor Capacity in Children and Adolescents with Cerebral Palsy Who Walk Independently. Phys. Occup. Ther. Pediatr. 2011, 32, 320–332. [Google Scholar] [CrossRef] [PubMed]
- Wallard, L.; Dietrich, G.; Kerlirzin, Y.; Bredin, J. Balance control in gait children with cerebral palsy. Gait Posture 2014, 40, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.; Ball, J. Energetics of walking in cerebral palsy. Orthop. Clin. N. Am. 1978, 9, 374–377. [Google Scholar]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cherni, Y.; Gagné-Pelletier, L.; Bouyer, L.; Mercier, C. Lower-Body Positive Pressure Treadmill Training for Pediatric Gait Disorders: A Scoping Review. Appl. Sci. 2022, 12, 323. https://doi.org/10.3390/app12010323
Cherni Y, Gagné-Pelletier L, Bouyer L, Mercier C. Lower-Body Positive Pressure Treadmill Training for Pediatric Gait Disorders: A Scoping Review. Applied Sciences. 2022; 12(1):323. https://doi.org/10.3390/app12010323
Chicago/Turabian StyleCherni, Yosra, Léandre Gagné-Pelletier, Laurent Bouyer, and Catherine Mercier. 2022. "Lower-Body Positive Pressure Treadmill Training for Pediatric Gait Disorders: A Scoping Review" Applied Sciences 12, no. 1: 323. https://doi.org/10.3390/app12010323
APA StyleCherni, Y., Gagné-Pelletier, L., Bouyer, L., & Mercier, C. (2022). Lower-Body Positive Pressure Treadmill Training for Pediatric Gait Disorders: A Scoping Review. Applied Sciences, 12(1), 323. https://doi.org/10.3390/app12010323