
Automated Extraction of Cerebral Infarction Region in Head MR Image Using Pseudo Cerebral Infarction Image by CycleGAN

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
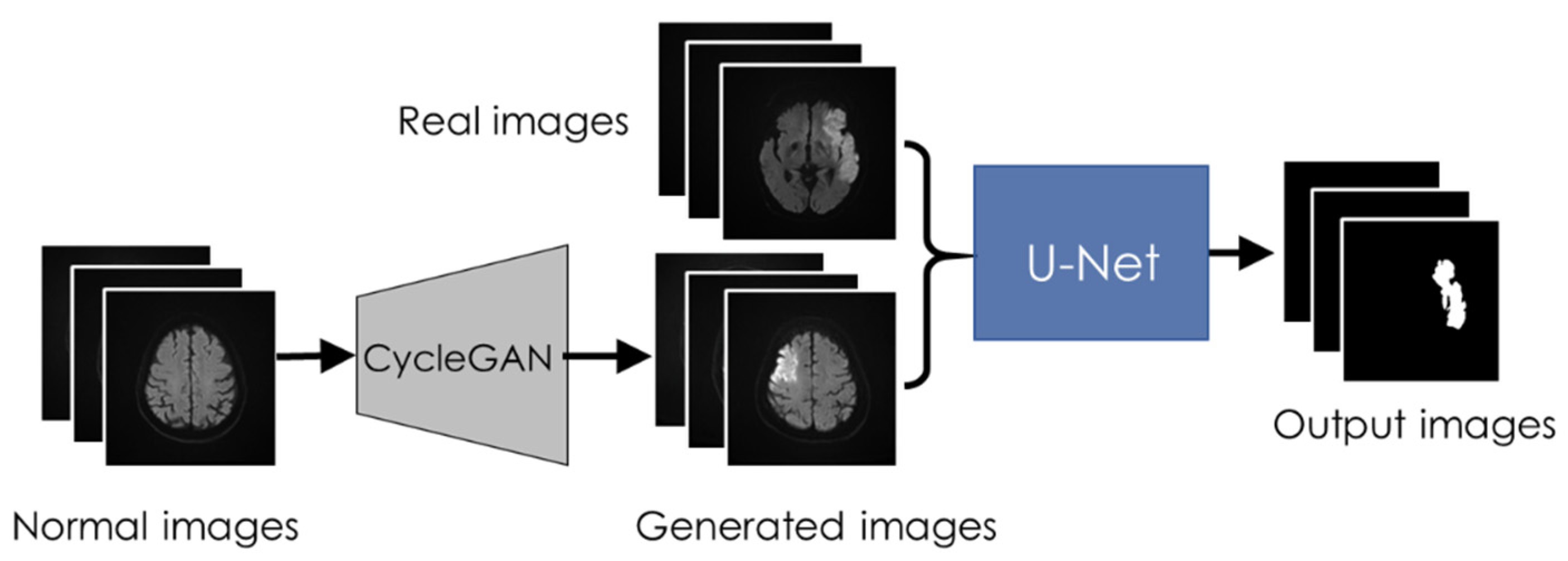
2.1. Outline
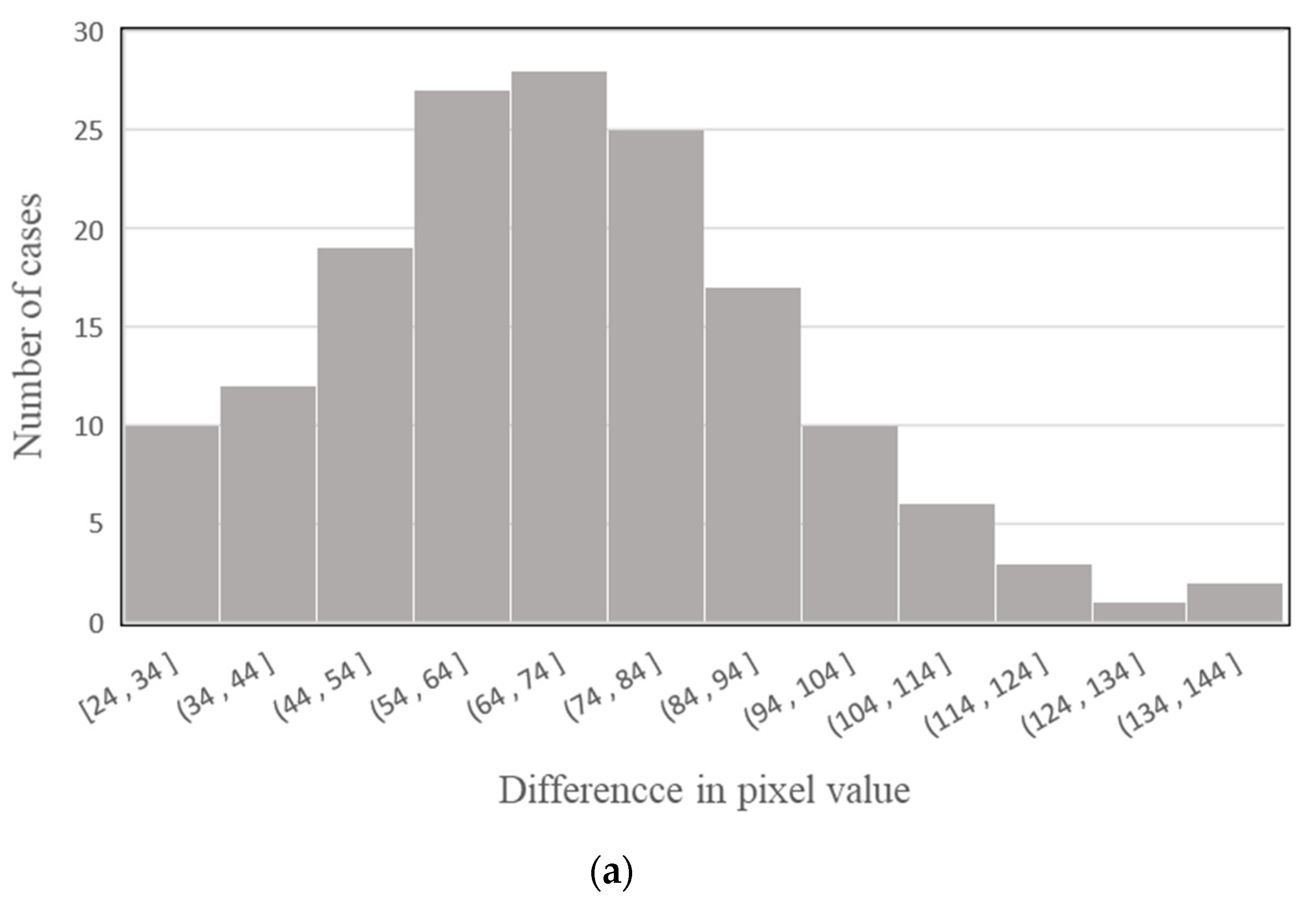
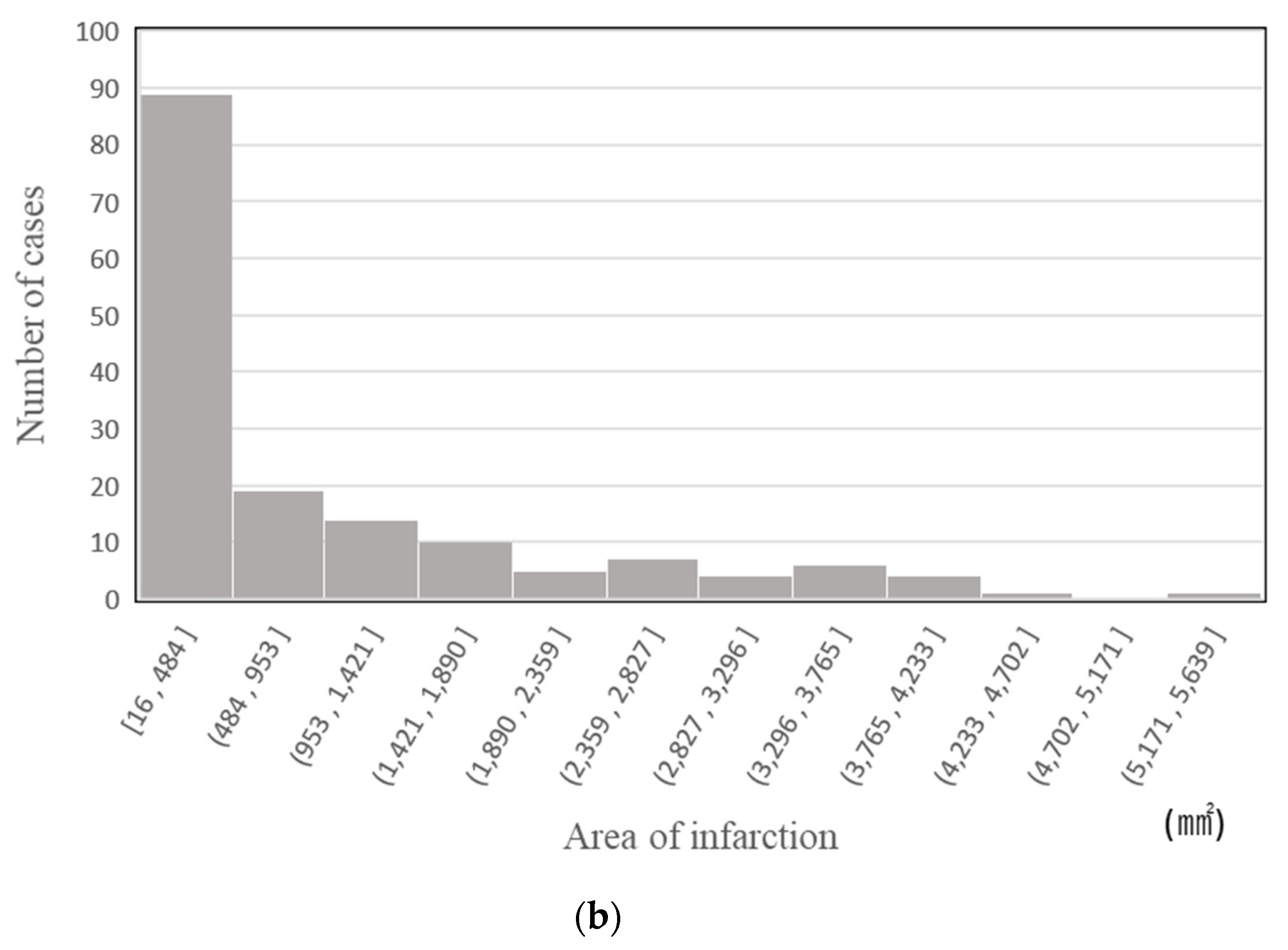
2.2. Image Dataset
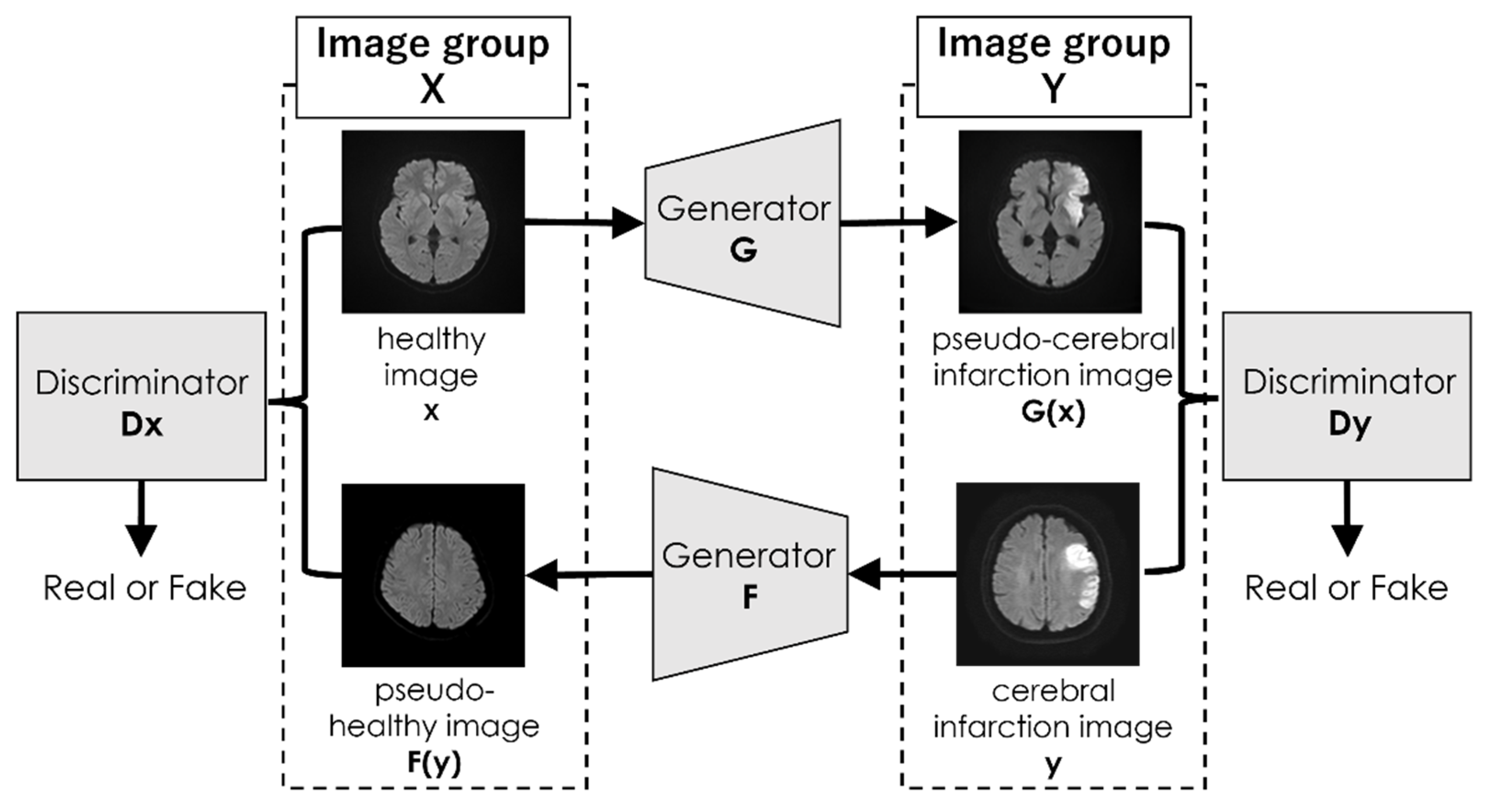
2.3. Generation of Pseudo Abnormal Images by CycleGAN
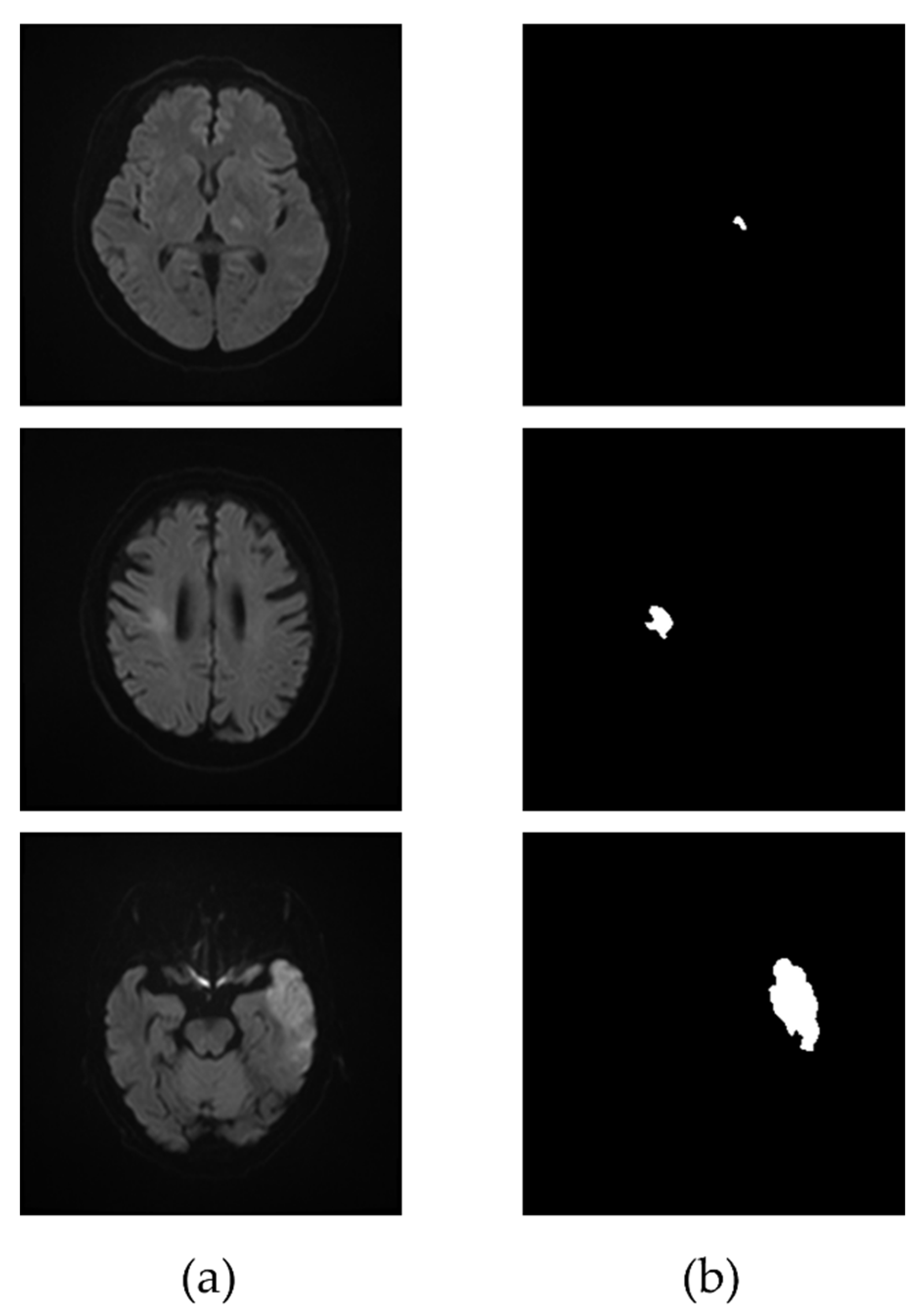
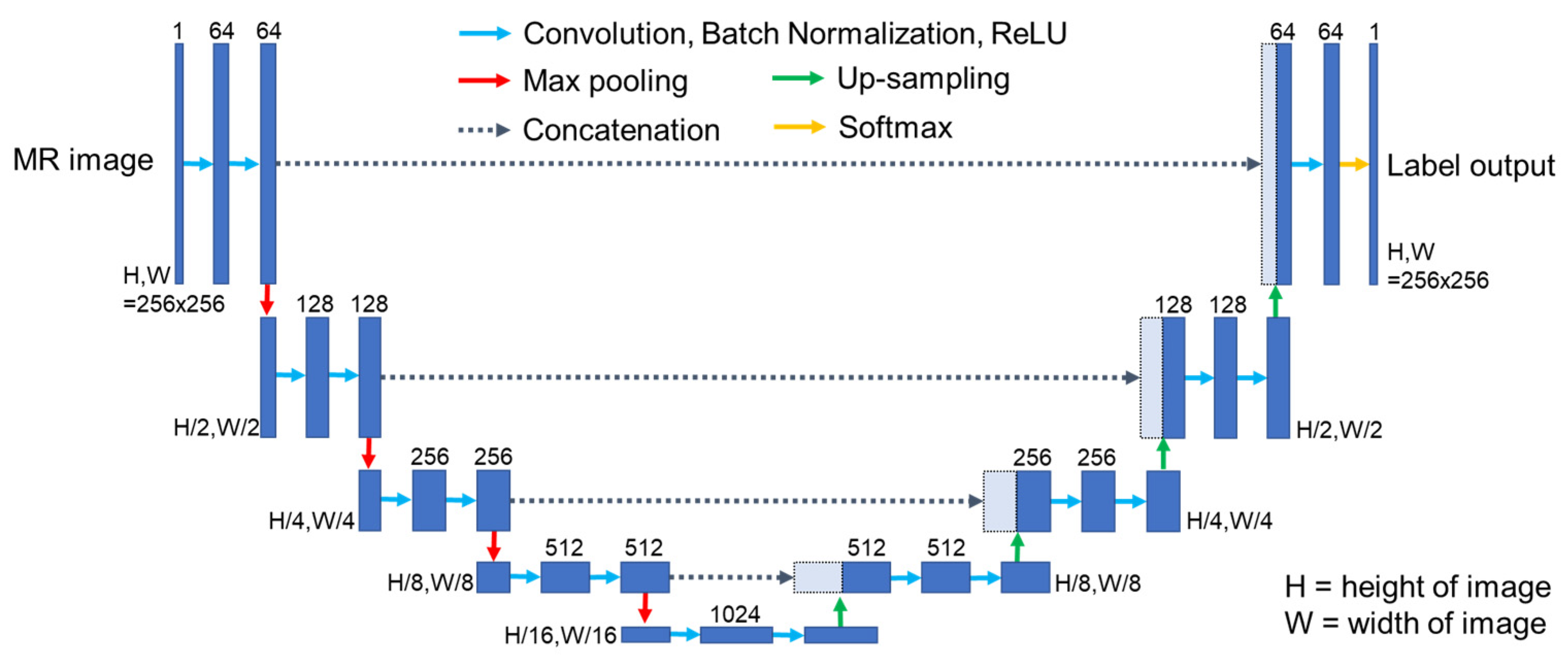
2.4. Extraction of Infarcted Region
2.5. Evaluation Metrics
3. Results
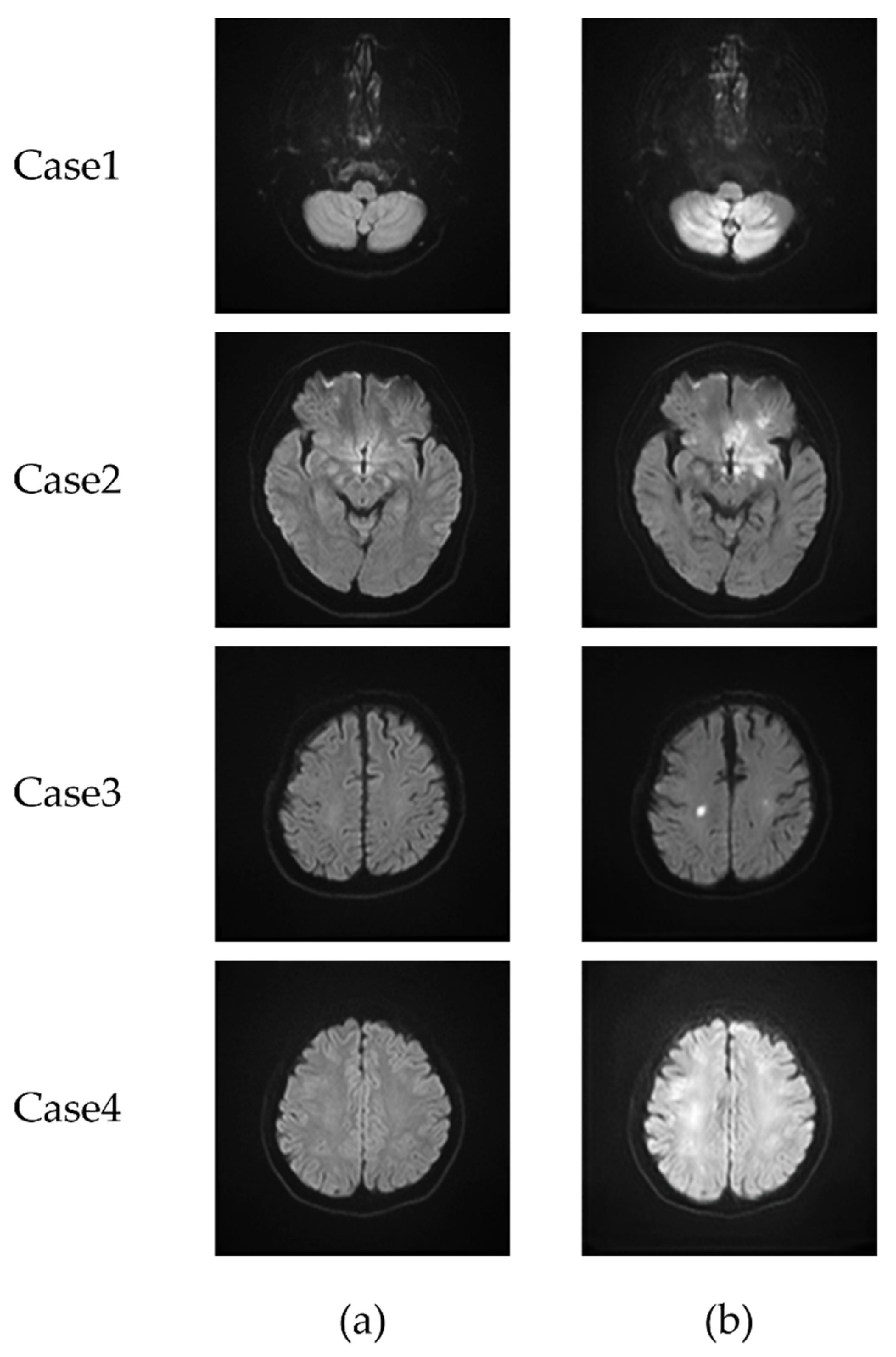
3.1. CycleGAN-Generated Images
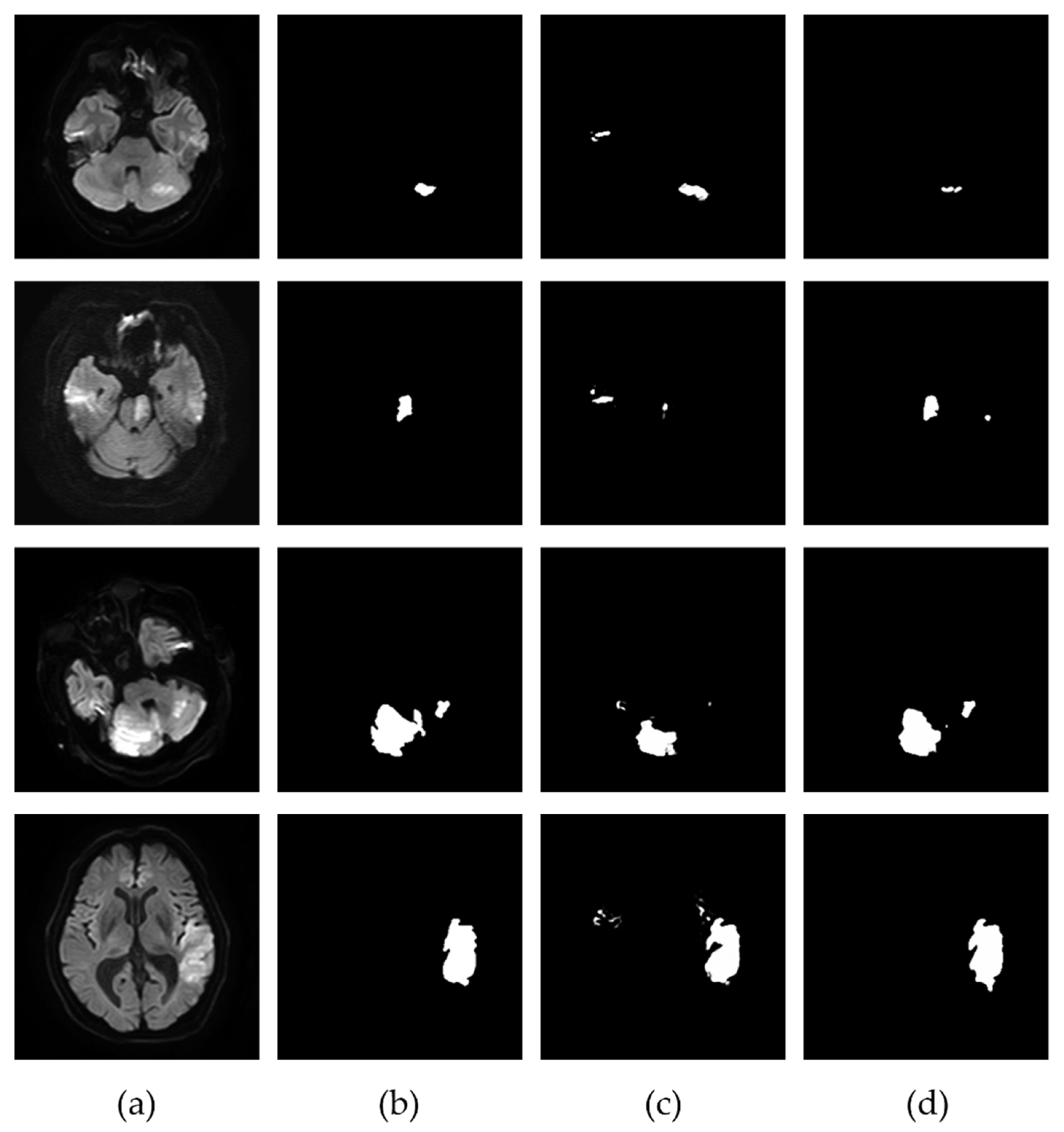
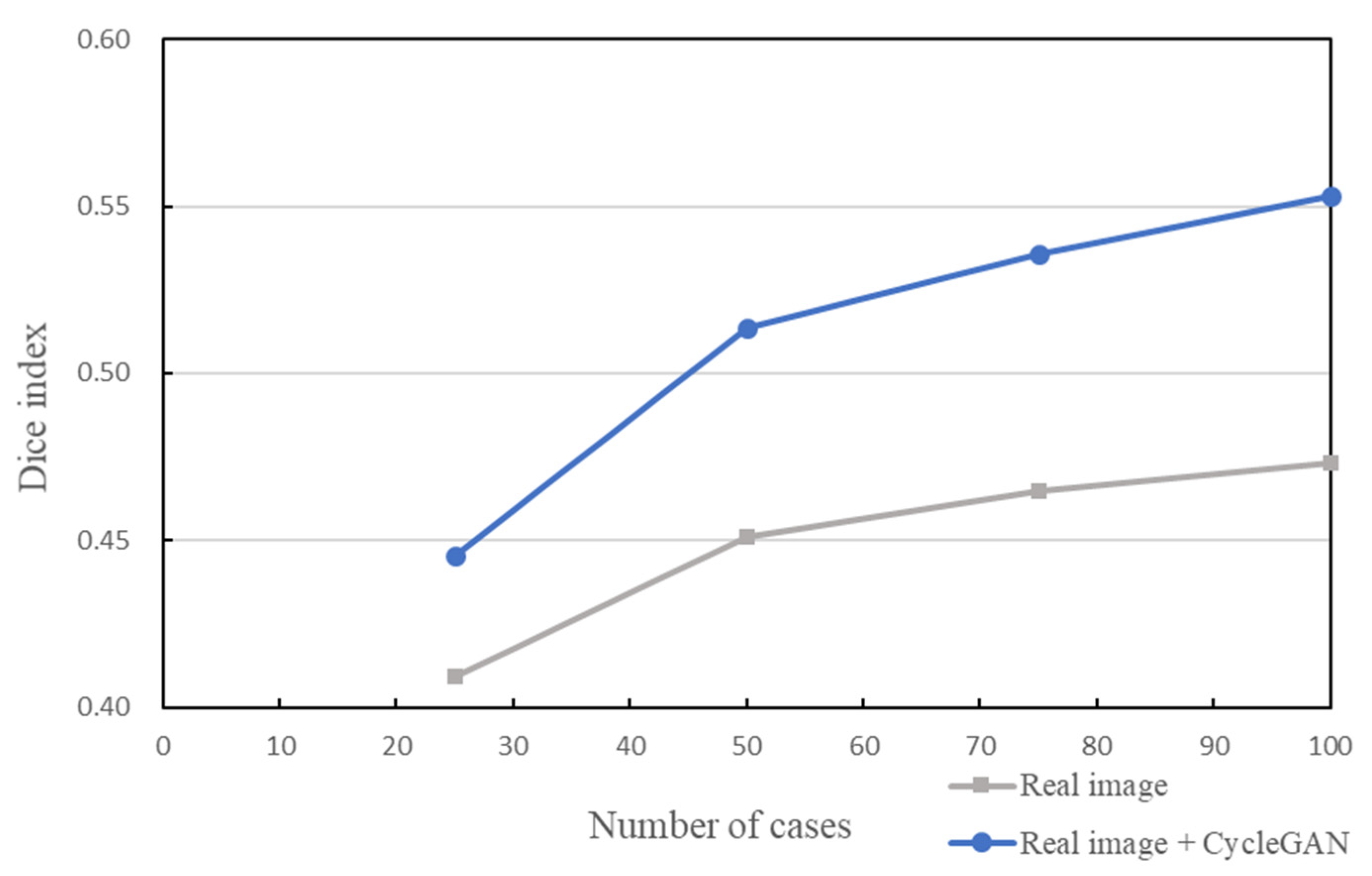
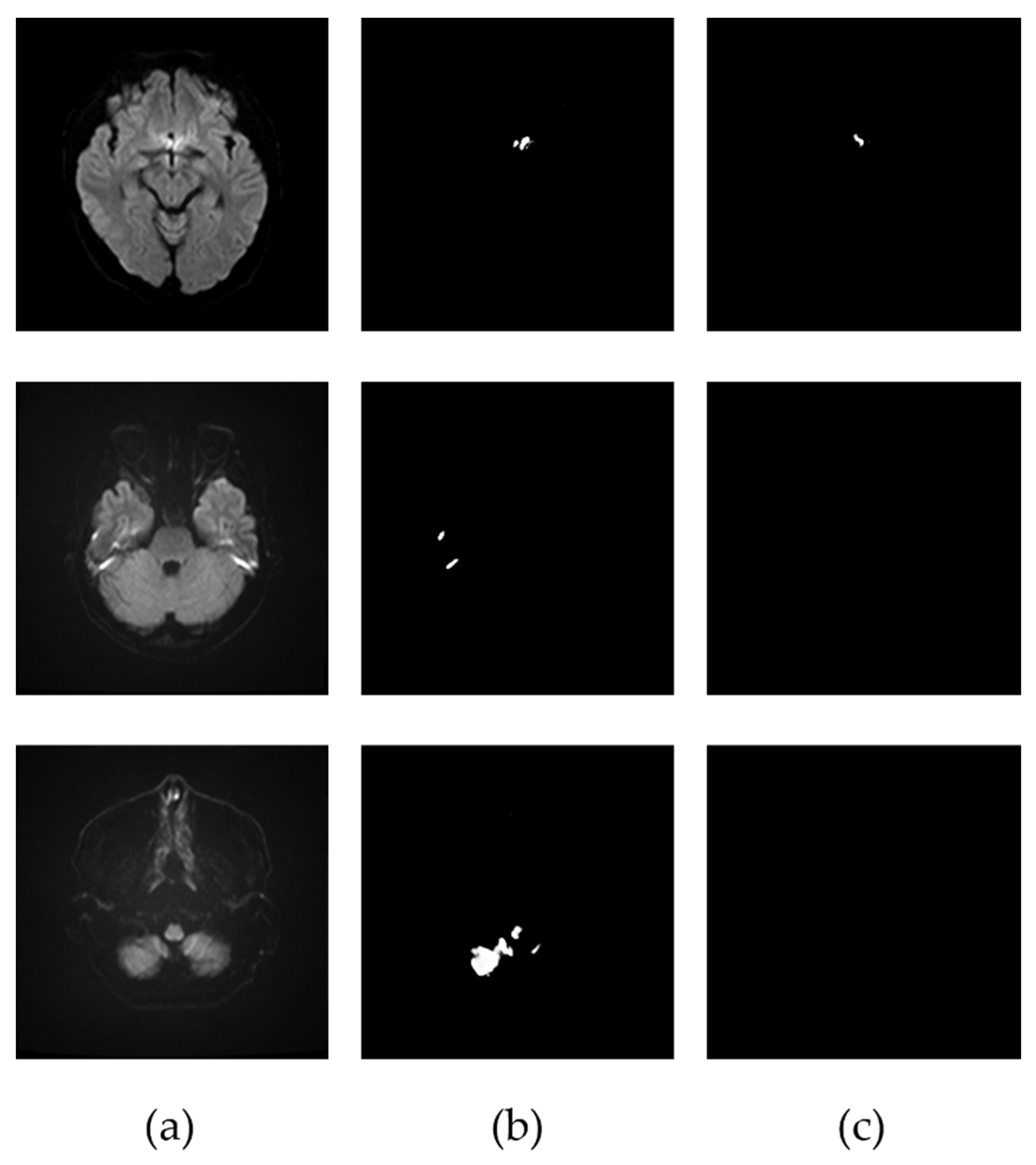
3.2. Extraction of the Infarcted Regions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; de Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. Heart disease and stroke statistics-2016 update a report from the American Heart Association. Circulation 2017, 135, e38–e48. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Lawes, C.M.; Bennett, D.A.; Anderson, C. Stroke epidemiology: A review of population-based studies of incidence, prevalence, and case-fatality in the late 20th century. Lancet Neurol. 2003, 2, 43–53. [Google Scholar] [CrossRef]
- Lutsep, H.L.; Albers, G.W.; Decrespigny, A.; Kamat, G.N.; Marks, M.P.; Moseley, M.E. Clinical utility of diffusion-weighted magnetic resonance imaging in the assessment of ischemic stroke. Ann. Neurol. 1997, 41, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Doi, K. Computer-aided diagnosis in medical imaging: Historical review, current status and future potential. Comput. Med. Imaging Graph. 2007, 31, 198–211. [Google Scholar] [CrossRef] [Green Version]
- Hinton, G.E.; Salakhutdinovr, R.R. Reducing the Dimensionality of Data with Neural Networks. Science 2006, 313, 504–507. [Google Scholar] [CrossRef] [Green Version]
- LeCun, Y.; Bengio, Y.; Geoffrey Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Hesamian, M.H.; Jia, W.; He, X.; Kennedy, P. Deep Learning Techniques for Medical Image Segmentation: Achievements and Challenges. J. Digit. Imaging 2019, 32, 582–596. [Google Scholar] [CrossRef] [Green Version]
- Long, J.; Shelhamer, E.; Darrell, T. Fully convolutional networks for semantic segmentation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 3431–3440. [Google Scholar] [CrossRef] [Green Version]
- Badrinarayanan, V.; Kendall, A.; Cipolla, R. Segnet: A deep convolutional encoder-decoder architecture for image segmentation. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 2481–2495. [Google Scholar] [CrossRef] [PubMed]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. In Proceedings of the Medical Image Computing and Computer-Assisted Intervention–MICCAI 2015, Munich, Germany, 5–9 October 2015; pp. 234–241. [Google Scholar]
- Dong, H.; Yang, G.; Liu, F.; Mo, Y.; Guo, Y. Automatic Brain Tumor Detection and Segmentation Using U-Net Based Fully Convolutional Networks. In Communications in Computer and Information Science; Springer: Cham, Switzerland, 2017; pp. 506–517. [Google Scholar] [CrossRef] [Green Version]
- Seo, H.; Huang, C.; Bassenne, M.; Xiao, R.; Xing, L. Modified U-Net (mU-Net) with Incorporation of Object-Dependent High Level Features for Improved Liver and Liver-Tumor Segmentation in CT Images. IEEE Trans. Med. Imaging 2020, 39, 1316–1325. [Google Scholar] [CrossRef] [Green Version]
- Gaál, G.; Maga, B.; Lukács, A. Attention U-Net Based Adversarial Architectures for Chest X-ray Lung Segmentation. In Proceedings of the Workshop on Applied Deep Generative Networks Co-Located with 24th European Conference on Artificial Intelligence 2020, CEUR Workshop Proceedings 2692, Santiago de Compostela, Spain, 29 August–8 September 2020. [Google Scholar]
- Rajini, N.H.; Bhavani, R. Computer aided detection of ischemic stroke using segmentation and texture features. Measurement 2013, 46, 1865–1874. [Google Scholar] [CrossRef]
- Barros, R.S.; Tolhuisen, M.; Boers, A.M.; Jansen, I.; Ponomareva, E.; Dippel, D.W.J.; Van Der Lugt, A.; Van Oostenbrugge, R.J.; Van Zwam, W.H.; Berkhemer, O.A.; et al. Automatic segmentation of cerebral infarcts in follow-up computed tomography images with convolutional neural networks. J. NeuroInt. Surg. 2019, 12, 848–852. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Bentley, P.; Rueckert, D. Fully automatic acute ischemic lesion segmentation in DWI using convolutional neural networks. NeuroImage Clin. 2017, 15, 633–643. [Google Scholar] [CrossRef] [PubMed]
- Dolz, J.; Ben Ayed, I.; Desrosiers, C. Dense Multi-path U-Net for Ischemic Stroke Lesion Segmentation in Multiple Image Modalities. Lect. Notes Comput. Sci. 2019, 11383, 271–282. [Google Scholar] [CrossRef] [Green Version]
- Karthik, R.; Menaka, R.; Johnson, A.; Anand, S. Neuroimaging and deep learning for brain stroke detection—A review of recent advancements and future prospects. Comput. Methods Programs Biomed. 2020, 197, 105728. [Google Scholar] [CrossRef]
- Paing, M.; Tungjitkusolmun, S.; Bui, T.; Visitsattapongse, S.; Pintavirooj, C. Automated Segmentation of Infarct Lesions in T1-Weighted MRI Scans Using Variational Mode Decomposition and Deep Learning. Sensors 2021, 21, 1952. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Xu, S.; Tan, L.; Wang, H.; Meng, J. Stroke Lesion Detection and Analysis in MRI Images Based on Deep Learning. J. Health Eng. 2021, 2021, 5524769. [Google Scholar] [CrossRef]
- Goodfellow, I.; Pouget-Abadie, J.; Mirza, M.; Xu, B.; Warde-Farley, D.; Ozair, S.; Courville, A.; Bengio, Y. Generative adversarial nets. Adv. Neural. Inf. Process Syst. 2014, 27, 2672–2680. [Google Scholar]
- Radford, A.; Metz, L.; Chintala, S. Unsupervised representation learning with deep convolutional generative adversarial networks. In Proceedings of the 4th International Conference on Learning Representations, ICLR 2016—Conference Track Proceedings, San Juan, PR, USA, 2–4 May 2016. [Google Scholar]
- Chen, X.; Duan, Y.; Houthooft, R.; Schulman, J.; Sutskever, I.; Abbeel, P. InfoGAN: Interpretable representation learning by information maximizing generative adversarial nets. Adv. Neural Inf. Process. Syst. 2016, 29, 2180–2188. [Google Scholar]
- Arjovsky, M.; Chintala, S.; Bottou, L. Wasserstein GAN. In Proceedings of the 34th International Conference on Machine Learning, Sydney, Australia, 6–11 August 2017; Volume 70, pp. 214–223. [Google Scholar]
- Zhu, J.-Y.; Park, T.; Isola, P.; Efros, A.A. Unpaired image-to-image translation using cycle-consistent adversarial networks. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 2223–2232. [Google Scholar]
- Hiasa, Y.; Otake, Y.; Takao, M.; Matsuoka, T.; Takashima, K.; Carass, A.; Prince, J.L.; Sugano, N.; Sato, Y. Cross-Modality Image Synthesis from Unpaired Data Using CycleGAN. Adv. Data Min. Appl. 2018, 11037, 31–41. [Google Scholar] [CrossRef]
- Zhou, L.; Schaefferkoetter, J.D.; Tham, I.W.; Huang, G.; Yan, J. Supervised learning with cyclegan for low-dose FDG PET image denoising. Med. Image Anal. 2020, 65, 101770. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar] [CrossRef] [Green Version]
- Isola, P.; Zhu, J.-Y.; Zhou, T.; Efros, A.A. Image-to-Image Translation with Conditional Adversarial Networks. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 5967–5976. [Google Scholar] [CrossRef] [Green Version]
- Zhang, R.; Zhao, L.; Lou, W.; Abrigo, J.; Mok, V.C.T.; Chu, W.C.W.; Wang, D.; Shi, L. Automatic Segmentation of Acute Ischemic Stroke From DWI Using 3-D Fully Convolutional DenseNets. IEEE Trans. Med. Imaging 2018, 37, 2149–2160. [Google Scholar] [CrossRef]
- Sandfort, V.; Yan, K.; Pickhardt, P.J.; Summers, R.M. Data augmentation using generative adversarial networks (CycleGAN) to improve generalizability in CT segmentation tasks. Sci. Rep. 2019, 9, 16884. [Google Scholar] [CrossRef] [PubMed]
- Mitra, J.; Bourgeat, P.; Fripp, J.; Ghose, S.; Rose, S.; Salvado, O.; Connelly, A.; Campbell, B.; Palmer, S.; Sharma, G.; et al. Lesion segmentation from multimodal MRI using random forest following ischemic stroke. NeuroImage 2014, 98, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Muda, A.F.; Saad, N.; Bakar, S.; Muda, S.; Abdullah, A. Brain lesion segmentation using fuzzy C-means on diffusion-weighted imaging. ARPN J. Eng. Appl. Sci. 2015, 10, 1138–1144. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| U-Net without CycleGAN | U-Net with CycleGAN | |
|---|---|---|
| Dice index | 0.473 | 0.553 |
| Jaccard index | 0.360 | 0.433 |
| Sensitivity | 0.940 | 0.920 |
| False positives per case | 3.750 | 1.234 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshida, M.; Teramoto, A.; Kudo, K.; Matsumoto, S.; Saito, K.; Fujita, H. Automated Extraction of Cerebral Infarction Region in Head MR Image Using Pseudo Cerebral Infarction Image by CycleGAN. Appl. Sci. 2022, 12, 489. https://doi.org/10.3390/app12010489
Yoshida M, Teramoto A, Kudo K, Matsumoto S, Saito K, Fujita H. Automated Extraction of Cerebral Infarction Region in Head MR Image Using Pseudo Cerebral Infarction Image by CycleGAN. Applied Sciences. 2022; 12(1):489. https://doi.org/10.3390/app12010489
Chicago/Turabian StyleYoshida, Mizuki, Atsushi Teramoto, Kohei Kudo, Shoji Matsumoto, Kuniaki Saito, and Hiroshi Fujita. 2022. "Automated Extraction of Cerebral Infarction Region in Head MR Image Using Pseudo Cerebral Infarction Image by CycleGAN" Applied Sciences 12, no. 1: 489. https://doi.org/10.3390/app12010489
APA StyleYoshida, M., Teramoto, A., Kudo, K., Matsumoto, S., Saito, K., & Fujita, H. (2022). Automated Extraction of Cerebral Infarction Region in Head MR Image Using Pseudo Cerebral Infarction Image by CycleGAN. Applied Sciences, 12(1), 489. https://doi.org/10.3390/app12010489