Abstract
(1) Background: The achievement of an optimal implant position is still a critical consideration in implantology, especially in the aesthetic area. Dynamic navigation is a computer-aided procedure that allows the surgeon to follow on a screen the three-dimensional position of instruments in real time during implant site preparation. The aim of this proof-of-concept study was to assess the clinical and radiographical performance and accuracy of the surgical workflow during maxillary immediate implant placement assisted by DTX studio Implant software planning and X-Guide Navigation. (2) Methods: Twelve consecutive patients requiring at least one implant in the maxillary aesthetic region were treated. Clinical outcome measures were biological complications and implant or prosthetic success rate. The accuracy was measured by calculating the deviation between the real implant position obtained from the postoperative cone beam computed tomography (CBCT) scan and the planned implant position. (3) Results: The average deviation at the implant shoulder was 0.77 ± 0.25 mm and at the apical point was 1.2 ± 0.61 mm. The depth error was 0.5 ± 0.21 mm. The axis deviation was 2.5 ± 0.41 degrees. No biological complications or implant and prosthetic failures occurred after mean 6-month follow-up. (4) Conclusions: Within the limitations of this study, it seems that the dynamic navigation system for implant placement in the maxillary aesthetic region is accurate for prosthetically driven implant placement.
1. Introduction
Implant-supported fixed prosthesis has become a well-established treatment to rehabilitate partially or fully edentulous patients. Surgical complications (including nerve injuries or hemorrhage), aesthetic deficiencies (buccal plate resorption resulting in dehiscence), and prosthetic complications (difficulties of loading a restoration, the need for utilizing an angled abutment to correct the placement axis), and marginal bone loss can be prevented by achieving a 3D implant placement that follows an ideal prosthetically driven concept, which in return eases the restoration procedure and enhances the aesthetic outcomes. Refs. [1,2] Computer-aided implant surgery (CAIS) has been inducted recently into dental implantology concepts to minimize the deviations from the virtually pre-planned implant placement procedure. Hämmerle et al. stated that [3] static computer-aided implant surgery (sCAIS) systems utilize STL templates supported by soft tissue and hard tissue, and teeth are fused during the drilling and placement of the implant, meanwhile dynamic computer-aided implant surgery (dCAIS) systems perform a live tracking for the implant; they drill using an optimal marker and then relate this information to the 3D pre-operative virtual plan set with CBCT. Such surgical techniques are being widely utilized in major neuro, maxillo-facial, ENT, and orthopedic surgeries and are rapidly becoming popular in implantology [4,5]. The advantages of dynamic navigation are that any implant system can be used, thanks to open-source systems and the reduced time and costs required for the laboratorial and impression-making procedures of static guided systems [6]. Another advantage of dynamic navigation is that the implant is placed with a wide area of visibility and thus remains controllable. Moreover, the planned placement of the implant can be modified intraoperatively during the intervention according to the three-dimensional position [7,8]. A recent systematic review demonstrated that dCAIS systems allow high accuracy during implant placements, accompanied by mean angle of deviation of less than 4° and superior accuracy with respect to freehand placement; the angle of deviations is slightly reduced with respect to the sCAIS system [9]. However, due to the complexity of the surgical procedure, sufficient training of the surgeon and team is required along with a significant procedure learning curve. The aim of this proof-of-concept study is to assess the clinical and radiographical performance and accuracy of the surgical workflow during maxillary immediate implant placement aided by DTX studio Implants planning software and X-Guide Navigations.
2. Materials and Methods
The study was planned as a retrospective clinical proof-of-concept design. Patients of both sexes and with a minimum age of 18 years were consecutively selected between September 2019 and June 2020 at the Department of Oral Surgery of the University of Naples Federico II according to the following inclusion criteria: healthy patients; full mouth bleeding on probing and full mouth plaque index less than 25; patients needing a minimum of 1 immediate implant in the anterior maxilla; a residual bone of a minimum of 10 mm in length and 6 mm in width; patients possessing at minimum of 3 stable teeth in premolar/molar region. Patients demonstrating empirical contraindications to implant surgery, a history of radiation therapy at the head and neck region, alcohol consumption or drug abuse, who were pregnant or nursing, suffering untreated periodontal conditions, or exhibiting uncompliant behavior with a supportive periodontal therapy (SPT) program were excluded. A total of 12 patients (5 males, 7 females; mean age 45.5 ± 6.15; age range 38–55 years-old) were enrolled, and a total of 22 implants were placed in the anterior region of the maxilla. All implant placements were performed using dynamic navigation systems (X-Guide, X-Nav Technologies, Inc., Lansdale, PA, USA), and clinical software (DTX studio) was used for pre-surgical implant planning. Post-surgical CBCT scans were taken for all patients. The differences between the real implant position acquired from the post-surgical CBCT scan and the pre-planned implant position were measured. The study was carried out in accordance with the ethical principles of the World Medical Association Declaration of Helsinki for studies involving human subjects, and the methods adopted conformed with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational studies [10]. A description of the surgical treatment was given, and written informed consent was obtained from each patient.
2.1. Digital Workflow
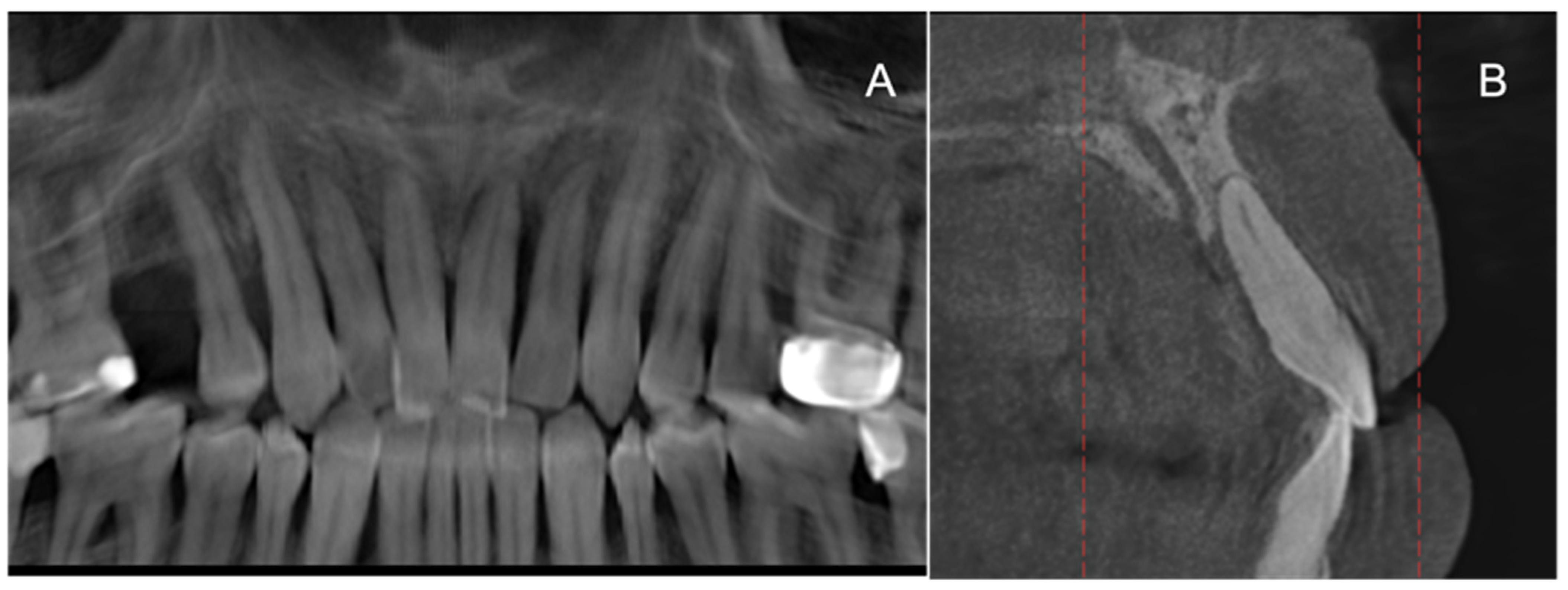
After clinical examination, all patients had a digital assessment, including orthopantomography and CBCT (Figure 1A,B). A high-speed CBCT scan (Kavo OP 3D, Kavo Dental, Biberach an der Riss, Germany) was used with following settings: field of view 140 mm height, 00 mm width, high resolution (voxel sizes 0.25) Kv90, mA10, and exposure time 7 s. Prior to the CBCT scan, a prefabricated thermoplastic device with three radiopaque fiducials (X-Clip, X-Nav Technologies) was placed on the residual teeth of the dental arch involved in the implant surgery. The X-guide Clip was warmed in hot water and positioned in the patient mouth. After 5 s, it was removed and instantly put in cold water. The x-guide clip was worn during the CBCT scan and was set between 8 and 10 mA. The clip device was removed after the CBCT, appropriately disinfected, labeled, and stored. An IOS (3Shape TRIOS®, Copenhagen, Denmark) of each patient was obtained, and the prosthetically driven implant positioning was made by a digital wax-up of the teeth to be replaced. Finally, the 3D CBCT scan and IOS were superimposed, through the matching of resulting DICOM (Digital Imaging and COmmunications in Medicine) and STL (Standard Triangulation Language) data files, respectively, into the DTX software (DTX ImplantStudio, Nobel Biocare AG, Kloten, Switzerland). The approved implant plan, with the implant coordinates and the digital wax-up, was exported an uploaded into the dynamic navigation system (X-Guide, X-Nav Technologies, Inc.).
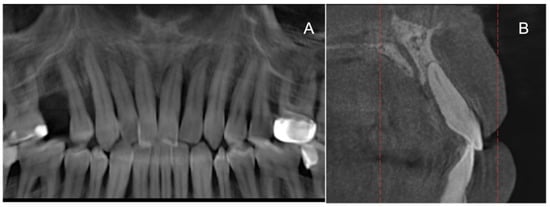
Figure 1.
Preoperative radiographic exams: (A) OPT; (B) CBCT.
2.2. Calibrations
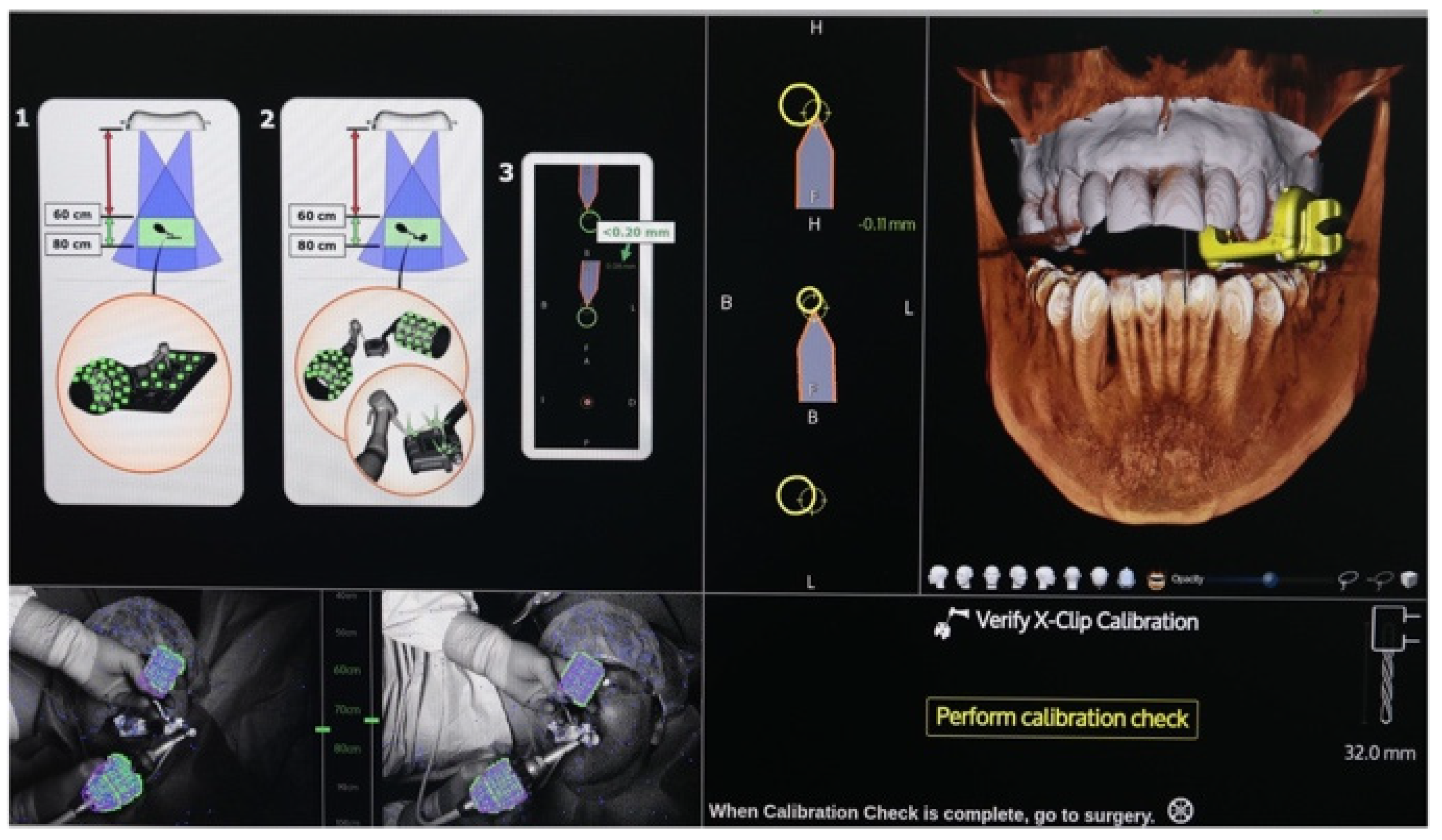
The surgical hand-piece calibration was performed prior to surgery in a sterile environment (Figure 2). The calibration determined the relationships relating the hand-pieces’ geometry and the drilling axis. The hand-pieces and the patients’ tracking arrays were in the sight of an overhead stereo camera to be tracked on the monitor.
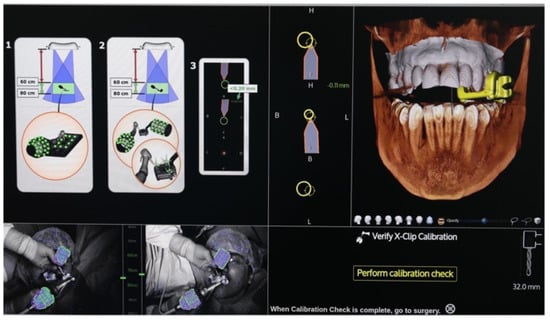
Figure 2.
Calibration.
2.3. Surgical Treatment
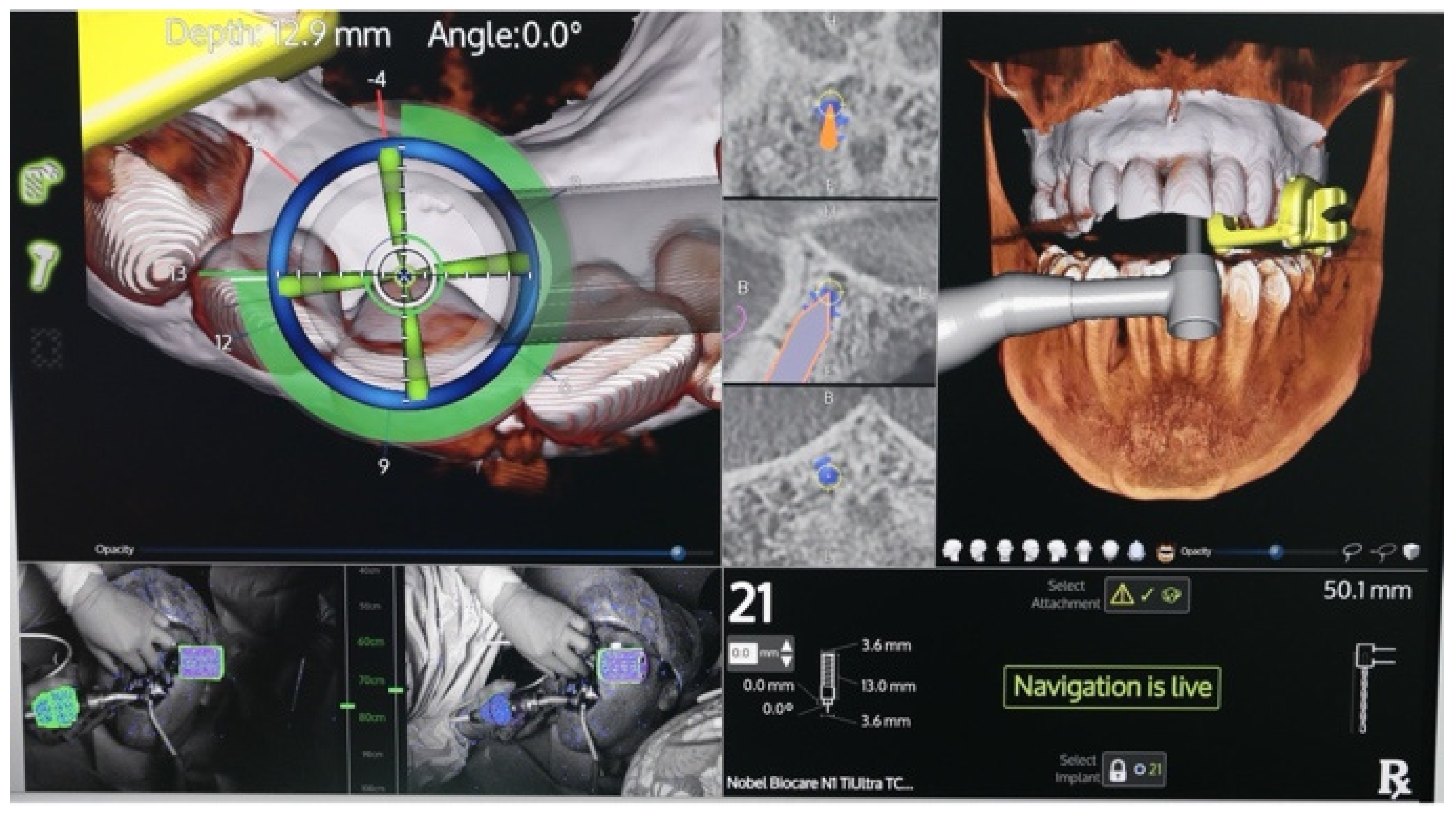
Prior the surgery, patients received periodontal treatment comprising scaling and root planning, if needed. All surgeries were performed by a single expert surgeon. Local anesthesia with 2% mepivacaine 1:100,000 adrenaline was used. The procedure involved the extraction of the anterior teeth, the revision on the sockets, and the placement of the immediate implants (NobelActive, TiUltra®, Nobel Biocare, Kloten, Switzerland) according to the treatment plan. The implant placement was made by using the normal sequence of drills under sterile and cold saline solution (Figure 3). If needed, frenuloplasty was performed. If immediate loading was scheduled, multi-unit abutment screwing and impression making were performed to prepare the temporary PMMA screw-retained prosthetics. Definitive prosthesis was delivered after 6 months. Post-operative instructions included soft diet and enhanced oral hygiene, while preventing the usage of toothbrush and traumas at the surgical sites. Rinsing with a 0.2% chlorexidine mouthwash was instructed to take place twice per day for 14 days. Removal of the sutures was done 2 weeks post-operatively. Antibiotic therapy using amoxicillin and clavulanic acid twice per day for 6 days was prescribed. The patient was enrolled in a SPT program with regular recall visits every six months.
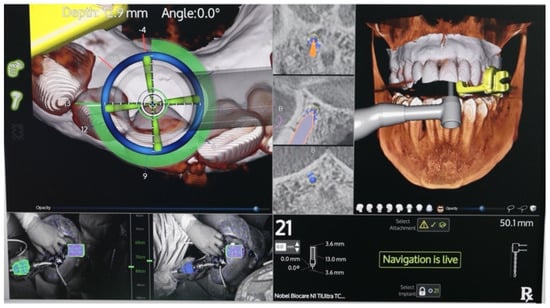
Figure 3.
Implant placement with navigation system.
2.4. Outcome Measures
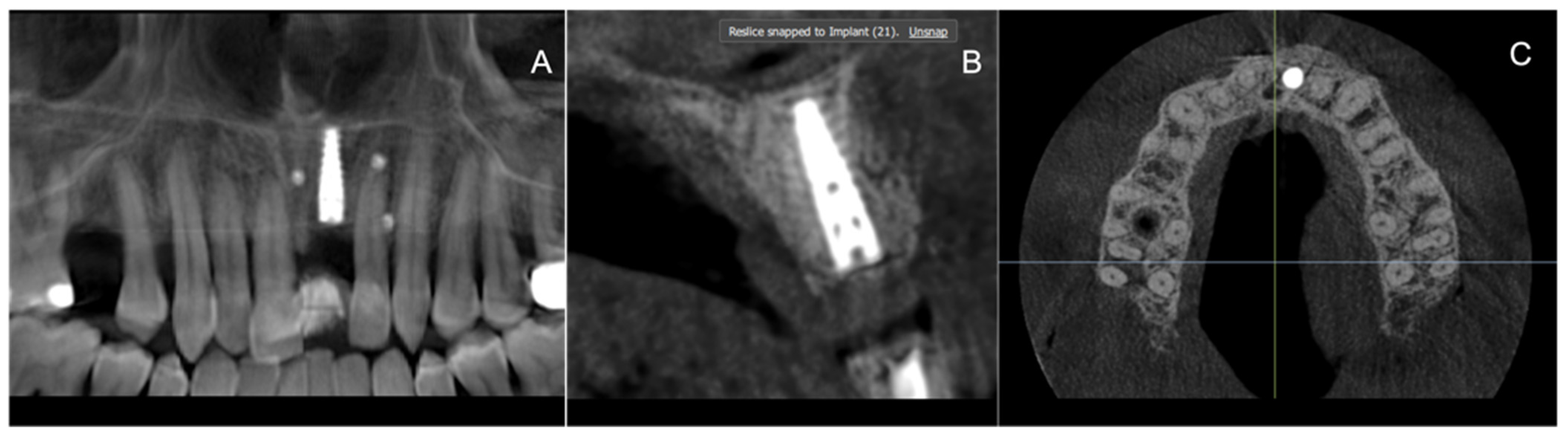
Clinical primary outcomes were biological complications, implant failure (implant mobility and/or removal of stable implant due to marginal bone loss or infection), prosthetic failure (loss of prosthesis secondary to implant loss, prosthesis replacement for any reason), aesthetic outcome, and overall patient satisfaction. The aesthetic outcomes were assessed according to Buser et al. [11]. The secondary outcome was the accuracy of the technique measured as the deviation between the real implant position obtained from the postoperative cone beam computed tomography (CBCT) scan and the planned implant position (Figure 4). It was calculated at the insertion and apical points of the implant. Implant depth error and deviation of angulation degree were also evaluated. Descriptive analysis was performed using mean ± standard deviation. The outcomes were evaluated by one independent blinded investigator.
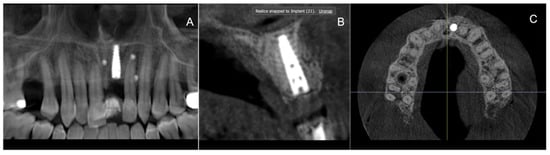
Figure 4.
Post-operative radiographic images: (A) opt; (B) sagittal section of CBCT; (C) axial section of CBCT.
3. Results
The main baseline patient and intervention characteristics are presented in Table 1. In five patients, two implants were placed at the level of lateral incisors to rehabilitate the four incisors. In nine cases, the immediate placement and immediate loading were made. The healing was uneventful for all patients; no complications and no implant or prosthetic failures occurred in a mean of 6 months’ follow-up. The average deviation at the implant insertion was 0.77 ± 0.25 mm, and at the apical point it was 1.2 ± 0.61 mm. The axis deviation was 2.5 ± 0.41 degrees. The depth error was 0.5 ± 0.21 mm. A summary of results is reported in Table 2. All patients confirmed that they were highly satisfied with both the function and esthetic of their implant-supported prostheses.

Table 1.
Patient and intervention characteristics.
Table 2.
Summary of results.
4. Discussion
The aim of this study was to assess the clinical and radiographical performance and accuracy of the surgical workflow during maxillary immediate implant placement assisted by DTX studio Implant software planning and X-Guide Navigation. The navigation systems have been used primarily in implant dentistry [12,13] but recently have been used in endodontics for guided access cavity preparation in calcified root canals or for removing fiber posts from root canal–treated teeth with greater accuracy than free-hand methods [14,15]. The accuracy can be defined as the degree to which the result of a measurement, calculation, or specification conforms to the correct value or standard. In the present study, the accuracy was measured mainly as angle deviation. This was justified in the prosthetic importance of these parameters. Our results show that the axis deviation was 2.5 ± 0.41 degrees. This value is less than the values of averaged 4.1 degrees for clinical studies and 3.7 degrees for in vitro studies reported in a recent systematic review, showing in addition that the accuracy of dynamic navigation is comparable to that of static navigation [16]. D’ahese and collaborators found that guided implant surgery using desktop 3D printed mucosa-supported guides has a clinically acceptable level of accuracy [17]. The dynamic navigation system allows the surgeon to place the dental implant based on the ideal position to achieve the best outcome, ideally as prosthetic-driven. This is even more true when the placement of the implants relates to the esthetic region of the maxilla [18,19,20]. The rehabilitation of the esthetic region represents a challenge for the clinicians because of patients’ exacting esthetic demands and difficult pre-existing anatomy. The main esthetic objectives of implant therapy from a surgical point of view are the achievement of a harmonious gingival margin without abrupt changes in tissue height, maintaining intact papillae, and obtaining or preserving a convex contour of the alveolar crest. Incorrect inclination of the implants in this region can have serious consequences on the esthetic outcomes and on the success in a long term. An inadequate vestibular thickness around the dental implants may be associated with peri-implant bone loss and mucosal recession [21]. With regard to this matter, dynamic navigation was also shown to be effective to guide bone and soft tissue sculpturing [22]. Moreover, the accuracy may depend on the experience of the surgeon. Pettersson and collaborators compared the accuracy with guided implant surgery from five different surgeons. A statistically significant difference between the virtually planned and placed implant positions was observed for three of the four outcome variables (the apex, hexagon, and depth). A statistically significant difference was also noted among all surgeons regarding the positions of the apex, depth, and angle [23]. However, it should be noted that the guided surgery, rather than accelerating the treatment and helping the inexpert surgeon, is a complex technique for the planification and execution, with a margin of error that, beyond the results of our study, is related to a completion of the learning curve and to the exploitation of the integrated systems. Another drawback is the increased cost of the equipment and the license needed to plan each case. The main limitation of this study is the lack of the control group, related to the fact that, to the best of our knowledge, this is the first study that evaluated the accuracy of dynamic navigation in the immediate placement of implants in the esthetic region. Other limitations are related to absence of sample size calculations due to the design of the study, with a small sample and short follow-up (6 months).
5. Conclusions
Within the limitations of this study, the placement of the dental implants under the navigation system for immediate implant placement can be considered an accurate and predictable procedure and can be considered a valid support for surgeons to optimize implantology, especially in the esthetic regions. However, it requires expert clinical and surgical competences and a long learning curve. Further studies are needed to confirm our results and the predictability of the system.
Author Contributions
Conceptualization, G.S. and G.M.; methodology, R.G.; software, E.B.; validation, G.S. and G.M. formal analysis, M.C.; investigation, E.B.; resources, E.B.; data curation, M.C.; writing—original draft preparation, R.G.; writing—review and editing, G.M.; visualization, G.S.; supervision, G.S.; project administration, G.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent was obtained from the patient(s) to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to patient privacy.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| CBCT | Cone Beam Computed Tomography |
| DICOM | Digital Imaging and COmmunications in Medicine |
| STL | Standard Triangulation Language |
References
- Sammartino, G.; Prados-Frutos, J.C.; Riccitiello, F.; Felice, P.; Cerone, V.; Gasparro, R.; Wang, H.-L. The Relevance of the Use of Radiographic Planning in Order to Avoid Complications in Mandibular Implantology: A Retrospective Study. BioMed Res. Int. 2016, 2016, 8175284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sbordone, C.; Toti, P.; Brevi, B.; Martuscelli, R.; Sbordone, L.; Di Spirito, F. Computed tomography-aided descriptive analysis of maxillary and mandibular atrophies. J. Stomatol. Oral. Maxillofac. Surg. 2019, 120, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Hämmerle, C.H.F.; Stone, P.; Jung, R.; Kapos, T.; Brodala, N. Consensus statements and recommended clinical procedures regarding computer-assisted implant dentistry. Int. J. Oral Maxillofac. Implant. 2009, 24, 126–131. [Google Scholar]
- Pellegrino, G.; Lizio, G.; Basile, F.; Stefanelli, L.V.; Marchetti, C.; Felice, P. Dynamic Navigation for Zygomatic Implants: A Case Report about a Protocol with Intraoral Anchored Reference Tool and an Up-To-Date Review of the Available Protocols. Methods Protoc. 2020, 3, 75. [Google Scholar] [CrossRef]
- Pellegrino, G.; Mangano, C.; Mangano, R.; Ferri, A.; Taraschi, V.; Marchetti, C. Augmented reality for dental implantology: A pilot clinical report of two cases. BMC Oral Health 2019, 19, 158. [Google Scholar] [CrossRef]
- D’haese, J.; Ackhurst, J.; Wismeijer, D.; De Bruyn, H.; Tahmaseb, A. Current state of the art of computer-guided implant surgery. Periodontol 2000 2017, 73, 121–133. [Google Scholar] [CrossRef]
- Tahmaseb, A.; Wu, V.; Wismeijer, D.; Coucke, W.; Evans, C. The accuracy of static computer-aided implant surgery: A systematic review and meta-analysis. Clin. Oral. Implant. Res. 2018, 29 (Suppl. 16), 416–435. [Google Scholar] [CrossRef] [Green Version]
- Stefanelli, L.V.; Mandelaris, G.A.; Franchina, A.; Pranno, N.; Pagliarulo, M.; Cera, F.; Maltese, F.; Angelis, F.; Carlo, S.D. Accuracy of Dynamic Navigation System Workflow for Implant Supported Full Arch Prosthesis: A Case Series. Int. J. Environ. Res. Public Health 2020, 17, 5038. [Google Scholar] [CrossRef]
- Jorba-García, A.; González-Barnadas, A.; Camps-Font, O.; Figueiredo, R.; Valmaseda-Castellón, E. Accuracy assessment of dynamic computer–aided implant placement: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 2479–2494. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Buser, D.; Martin, W.; Belser, U.C. Optimizing esthetics for implant restorations in the anterior maxilla: Anatomic and surgical considerations. Int. J. Oral. Maxillofac Implant. 2004, 19, 43–61. [Google Scholar]
- Emery, R.W.; Merritt, S.A.; Lank, K.; Gibbs, J.D. Accuracy of Dynamic Navigation for Dental Implant Placement-Model-Based Evaluation. J. Oral Implant. 2016, 42, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Block, M.S.; Emery, R.W.; Lank, K.; Ryan, J. Implant Placement Accuracy Using Dynamic Navigation. Int. J. Oral Maxillofac. Implant 2017, 32, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Schnutenhaus, S.; Edelmann, C.; Knipper, A.; Luthardt, R.G. Accuracy of Dynamic Computer-Assisted Implant Placement: A Systematic Review and Meta-Analysis of Clinical and In Vitro Studies. J. Clin. Med. 2021, 10, 704. [Google Scholar] [CrossRef]
- Dianat, O.; Nosrat, A.; Mostoufi, B.; Price, J.B.; Gupta, S.; Martinho, F.C. Accuracy and efficiency of guided root-end resection using a dynamic navigation system: A human cadaver study. Int. Endodontic. J. 2021, 54, 793–801. [Google Scholar] [CrossRef]
- Janabi, A.; Tordik, P.A.; Griffin, I.L.; Mostoufi, B.; Price, J.B.; Chand, P.; Martinho, F.C. Accuracy and Efficiency of 3-dimensional Dynamic Navigation System for Removal of Fiber Post from Root Canal-Treated Teeth. J. Endod. 2021, 47, 1453–1460. [Google Scholar] [CrossRef]
- D’haese, R.; Vrombaut, T.; Hommez, G.; De Bruyn, H.; Vandeweghe, S. Accuracy of Guided Implant Surgery in the Edentulous Jaw Using Desktop 3D-Printed Mucosal Supported Guides. J. Clin. Med. 2021, 10, 391. [Google Scholar] [CrossRef]
- Checchi, V.; Gasparro, R.; Pistilli, R.; Canullo, L.; Felice, P. Clinical Classification of Bone Augmentation Procedure Failures in the Atrophic Anterior Maxillae: Esthetic Consequences and Treatment Options. BioMed Res. Int. 2019, 2019, 4386709. [Google Scholar] [CrossRef]
- Ramaglia, L.; Di Spirito, F.; Sirignano, M.; La Rocca, M.; Esposito, U.; Sbordone, L. A 5-year longitudinal cohort study on crown to implant ratio effect on marginal bone level in single implants. Clin. Implant. Dent. Relat. Res. 2019, 21, 916–922. [Google Scholar] [CrossRef]
- Di Spirito, F.; Toti, P.; Brevi, B.; Martuscelli, R.; Sbordone, L.; Sbordone, C. Computed tomography evaluation of jaw atrophies before and after surgical bone augmentation. Int. J. Clin. Dent. 2019, 12, 259–270. [Google Scholar]
- Simonpieri, A.; Gasparro, R.; Pantaleo, G.; Mignogna, J.; Riccitiello, F.; Sammartino, G. Four-year post-loading results of full-arch rehabilitation with immediate placement and immediate loading implants: A retrospective controlled study. Quintessence Int. 2017, 48, 315–324. [Google Scholar] [PubMed]
- Pozzi, A.; Hansson, L.; Carosi, P.; Arcuri, L. Dynamic navigation guided surgery and prosthetics for immediate loading of complete-arch restoration. J. Esthet. Restor. Dent. 2021, 33, 224–236. [Google Scholar] [CrossRef] [PubMed]
- Pettersson, A.; Kero, T.; Söderberg, R.; Näsström, K. Accuracy of virtually planned and CAD/CAM-guided implant surgery on plastic models. J. Prosthet. Dent. 2014, 112, 1472–1478. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).