Abstract
Immersive technologies are redefining ways of interacting with 3D objects and their environments. Moreover, efforts in blended learning have presented several advantages of incorporating educational technology into the learning space. The advances in educational technology have in turn helped to widen the choice of different pedagogies for improving learner engagement and levels of understanding. However, there is limited research in anatomy education that has considered the use and adoption of immersive technologies for the musculoskeletal system, despite its immense advantage. This research presents a practical immersive anatomy education system (coined Anat_Hub) developed using the agile scrum and participatory design method at a selected tertiary institution in Cape Town, South Africa, which promotes learner engagement through an asynchronous technological means using augmented reality (AR). The aim of the study was to develop an immersive AR mobile application that will assist learners and educators in studying and teaching the names, attachments, and actions of muscles of the human musculoskeletal system (upper and lower limbs). The Anat_Hub application offers a wide range of useful features for promoting active and self-regulated learning, such as 3D and AR modes, glossary, and quiz features. The application was tested with potential users, and on a variety of mobile device specifications. Very few volunteers have used AR prior to this study (13.2%). On a scale of 1 to 5, the majority of volunteers scored the application a 4 or 5. Overall, results and feedback obtained from users show that the proposed immersive anatomy system could effectively improve learner engagement and retention of anatomy concepts.
1. Introduction
Improving the quality and impact of higher education and training for the development of appropriate skills and capabilities is at the forefront of the National development plan for South Africa’s vision for 2030 [1]. Great advances have been made in blended learning and its implementation in the medical science disciplines to assist students with a range of topics from anatomy to surgery [2]. On the other hand, however, the field of anatomy education is still impeded by various challenges that could negatively impact the desired educational outcomes. These challenges, which are magnified in under-resourced settings, include limited practical hours for learners and qualified instructors, limited access to and high cost of cadavers and artificial models, as well as large amounts of content with complex nomenclature that students are expected to grasp using supplementary resources [3]. Anatomy learning heavily relies on the visualization of structures, and the use of blended learning has the potential to alleviate such challenges and promote the importance of using alternative interventions in traditional teaching and learning [4].
Blended learning involves the combination of different learning methods, new technologies, and activities that combine traditional face-to-face teaching methods with authentic online methodologies [5]. In recent years, the majority of existing literature on how to enhance anatomy learning by means of augmented reality (AR) implementation focused on new curriculum approaches and theoretical frameworks to improve academic performance (e.g., blended learning) [5,6,7,8], the introduction of new teaching tools [9,10,11,12,13], and challenging factors encountered by the anatomy discipline and how to solve them [3,4,7]. The use of immersive technology (virtual reality (VR), AR, and mixed reality (MR)) in blended learning has great potential to effectively address the aforementioned challenges. Benefits include the practical exploration of theory through a combination of multimedia information, where students can visualise and grasp difficult theoretical concepts and naturally interact with multimedia representations of teaching materials in a fun, compelling and engaging manner [14]. However, the use and adoption of immersive technologies in blended anatomy education (particularly for the musculoskeletal system—which is key in supporting locomotion and protecting vital organs) remains relatively understudied, potentially due to the newness of AR technology at higher education institutions on the African continent [15,16]. Hence, this research developed an immersive anatomy learning platform (coined Anat_Hub), which focuses on the musculoskeletal system using AR. The aim of the developed system was to allow users to learn how to isolate various anatomical structures of the upper and lower limbs by offering an engaging platform and features such as AR mode, 3D mode, a glossary, and a quiz. The developed system was then tested with undergraduate anatomy students to prove its relevance and viability.
The remainder of the paper is organised as follows: Section 2 presents the related literature on anatomy education and further establishes the novelty in this research, Section 3 discusses the design methodology and implementation approaches adopted in this study, Section 4 reports on the results, and Section 5 summarises and concludes the paper.
2. Related Research
In recent years, anatomy education has adopted blended learning approaches through combining technology and traditional teaching and learning methods. The benefits that blended learning offers have greatly motivated advances in various pedagogies and educational technologies. For example, it is a combination of the advantages of both face-to-face and online learning, which allows students to contextualise and conceptualise content autonomously. Other benefits include enhanced learner engagement through self-regulated learning, and the potential to increase academic performance [17,18].
A study in 2016 by Green and Whitburn [6] examined the effects of online content with traditional face-to-face lectures (blended learning approach) and found that learning outcomes increased with no loss in student engagement. They further suggested that, with extensive research and planning, institutions should implement innovative strategies such as new online resources to support student diversity and improve student learning outcomes and engagement when learning gross anatomy.
Miles et al. (2017) [8] also highlighted the importance of planning in their proposed model for blended and flipped classroom learning, which is a teaching approach or strategy in which students are encouraged to acquire content via multiple formats and technologies before attending traditional lectures in medical education. The authors indicated that any model aimed at designing and delivering a blended course successfully must involve academics and their teaching teams, the students taking the course, and instructional designers [8].
In 2018, Khalil et al. [5] proposed a four-step blended learning framework for teaching anatomical sciences, consisting of: (i) an analysis and planning phase; (ii) a design and development phase; (iii) an implementation phase; and (iv) an evaluation phase. The implementation of such a framework aims to improve student academic performance, motivation, attitude, and satisfaction, which would provide convenient and flexible learning [5]. Nobles (2019) [19] aimed to provide insight into how blended learning occurs by drawing on the anatomy faculty’s experience in their respective blended learning modules, using a theoretical framework of community of inquiry, cooperative learning, and discovery learning.
It is observed that despite the numerous efforts in blended learning, the use of immersive technology is still at its stage of exploration and development due to its novelty, particularly in the African continent. However, the adoption of educational technologies such as immersive technologies (e.g., AR, VR, and MR) are becoming more popular in anatomy education to assist students with grasping concepts related to anatomy and surgery [2]. Immersive technologies create a unique experience by merging the physical world with a simulated world. However, there are key differences between each experience; for instance, AR casts virtual objects onto the real-world environment, whereas VR replaces the entire “real world” with a virtual one [20]. This research focuses on the use and implementation of AR features rather than VR or MR. It is important to note that the definition for AR has varied over the years. In 1997, Azuma [21] defined AR according to its features or characteristics, “a system that fulfils three basic features: a combination of real and virtual worlds, real time interaction, and accurate 3D registration of virtual and real objects”. Another way to define AR would be according to human perception, as it “allows digital content to be seamlessly overlaid and mixed into our perceptions of the real world” [22]. According to Klopfer (2008) [23], the term AR should not be restricted in terms of its definition, and should apply to any technology that blends real and virtual information in a meaningful way, and users’ interactions and engagement are augmented [24]. Hence, in this paper we define AR similarly to Suárez-Escudero (2020) [25], that is, as a technology that allows the user to integrate virtual objects onto physical objects in the “real world” using cameras, tablets, or mobile phones. Furthermore, our work draws from Kamphuis (2014) [15] in order to define our mobile AR application as markerless AR, which “uses positional data to acquire the user’s location” in order to “augment the virtual content on a precise location on or within the real environment, regardless of whether or not that environment is static”.
There are various studies that discuss the implementation of AR in anatomy learning using mobile devices. For instance, Küçük et al. (2016) [12], who aimed to discover the effects of MagicBook AR, a mobile AR application, on academic performance and cognitive overload of medical students, found that their experimental group (who used mAR) recorded higher achievements and a lower cognitive load. These results can be attributed to MagicBook facilitating abstract information becoming concrete, instant access to content anywhere, students exerting less cognitive effort, and learner satisfaction recorded by the experimental group. Then there are also studies that created and developed their own mobile AR learning systems in order to test user satisfaction, among other reasons. In 2015, Jamali et al. [13] developed a mobile prototype called Human anatomy in Mobile Augmented Reality (HuMAR) within a Waterfall Model in order to assist students and potentially strengthen their learning process of the human skeletal structure. They tested the user experience from both a didactic and technical perspective, and demonstrated that students were satisfied with HuMAR, which could potentially have a positive effect on their learning processes. However, as opposed to the waterfall model, our work used an Agile Scrum approach for development so that we can take advantage of the simultaneous and adaptive workflow scheme that is offered by this approach.
Moro et al. (2017) [4] determined if VR and AR were as effective as tablet-based (TB) applications for learning structural anatomy, and furthermore if they enhanced student learning, engagement, and performance. They recorded the student perceptions of the various learning modes used to study the human skull as well as any side effects. According to their findings, there was a negligible difference in average scores in VR, AR, and TB, suggesting that VR and AR are as valuable as tablet devices; however, VR participants had higher chances of experiencing adverse effects such as headaches, dizziness, or blurred vision.
Kurniawan et al. (2018) [26], developed a mobile AR anatomy marker system to evaluate the usefulness thereof in anatomy learning. They used Floating Euphoria Framework in combination with the SQLite database to capture the marker, which is achieved by taking a picture that is divided into pieces so that the pattern matches the images stored in the database. The application has features that can display the entire body or parts of the human organs interactively. Highschool and medical students tested the application for learning human anatomy. The results revealed that the majority of students indicated that all of the evaluation requirements were met and that they were satisfied with the application to aid in anatomy learning.
Patil (2021) [27] developed a mobile AR application (AR in Anatomy) using the Waterfall approach in order to test its efficacy to promote learning of anatomy concepts and increase interest in the topic. The objectives were to allow students to explore 3D human body parts within the range of the body functions by rotating as well as zooming in and out. Furthermore, labels for small parts were provided. These objectives were successfully met.
Cercenelli et al. (2022) [28] developed and tested an innovative prototype tool, Anatomical Education with Augmented Reality (AEducaAR), for education in human anatomy. A unique attribute of the AEducaAR tool is that it favours a three-dimensional and topographical learning approach whereby a combination of AR technology and a tangible 3D printed anatomical model can be explored and manipulated. The study compared AEducaAR-based learning to standard learning (classical anatomy atlas) of medical students. Both groups performed an objective test and an anonymous questionnaire. The two learning methods did not significantly differ, however, in the questionnaire, the majority of students perceived the technology as useful to gain confidence with future medical technologies. When compared with the use of textbooks in their open-ended comments, students mentioned more advantages with the use of the AEducaAR tool. The results of their research survey clearly indicated the students’ enthusiasm and enjoyment with the tool and their eagerness to recommend it to their colleagues.
In 2013, research indicated that the development, usability, and initial implementation of AR tools in the education sector was still in its infancy, mostly following design-based and case study research methods [29]. Now, seven years later, the adoption of AR has been implemented as an assisting tool in the medical education sector, including anatomy teaching and learning [28], and it seems that student academic performance remains “statistically equivalent” when using either AR or traditional learning methods [4,12,28,30]. However, Moro 2021 [16] suggested that these results can be deemed as a positive outcome proving that technologies such as AR mobile applications can be used together with traditional resources to learn anatomy. Therefore, AR alone cannot replace traditional teaching or learning methods but rather can be used to enhance and supplement it [31].
There are multiple studies that indicate student user satisfaction in terms of the AR application developments and their implementation into anatomy learning [12,13,26,28]. However, though students may be satisfied with the implementation of AR, the adverse effects of such technology should be considered. Adverse effects may include: interfacing between multiple devices, the resistance to using AR applications due to unfamiliarity, time lost due to the implementation phase, the inflexibility of the content in AR systems, students possibly being cognitively overloaded by content encountered, and the novelty of the AR mobile applications wearing off [29].
Furthermore, AR technologies have the ability to enhance student learning processes to grasp complex concepts through the decreasing cognitive load effort required by students [12,13,28]. This can be attributed to student motivation, which tends to be driven by their satisfaction and confidence in their learning resources and tools [32]. Therefore, an opinion validated by Christopoulos (2022) [33] is that students should be given a tool that they are satisfied with that can increase their motivation and in turn can enhance their learning processes, academic performance, and student engagement. Within a South African university context, anatomy teaching and learning standards are still keeping up with the rest of the world, but constantly have to “catch up” with regards to the implementation of Information and Communication Technologies (ICTs) [34,35]. Nevertheless, there have been a few attempts at implementing blended learning with AR technologies into anatomy education in South Africa, and we could only identify two studies that have done so, which are Holmes’(2018) [36] and Khan et al.’s (2019) [10].
Holmes’ study (2018) [36] explored the practicality of an AR application, augmented reality-assisted orthopaedic surgery (ARAOS) technology, to support and enhance orthopaedic wrist replacement surgery through simulation. The experimental study found that compared to conventional fluoroscopic guidance, the AR application is insignificantly less accurate, registers a reduced procedural time, and has a short learning curve. The ARAOS technology shows clinical efficiency and feasibility to use in the operating room while remaining affordable and potentially more intuitive than other forms of navigational assistance.
One of the latest studies on AR in South Africa was conducted by Khan et al. (2019) [10] from the University of Cape Town. Their research focused on learning motivation so as to test undergraduate medical students’ perceptual arousal and attention span with the use of an already existing AR application, Anatomy 4D. Following the ARCS model, results showed that there was a significant increase in the students’ attention and motivation when using the AR mobile application. Another positive aspect, as was desired by the outcome of this research, is the feasibility of mobile AR applications in comparison to the equipment and methods generally used to assist students in grasping content. However, despite these research efforts on the use of AR and or VR in anatomy education, no related studies in South Africa indicated the development of an immersive anatomy mobile application focussing on the musculoskeletal system.
Owing to the lack of research in anatomy education in research, this research aimed to fill the gap and broaden the perspective of teaching and learning processes involving mobile AR technology. This paper is different from previous efforts in South Africa as it investigates our development and possible implementation of a free mobile AR anatomy learning system (Anat_Hub) particularly for the musculoskeletal system. The Anat_Hub learning system was developed and designed for the Department of Medical Bioscience at the University of the Western Cape (UWC), in order to promote active and self-paced learning amongst first-year students registered for anatomy modules. Furthermore, we evaluate the initial user experience of the application in order to establish its viability and areas for future development
Table 1 provides a list of documented research related to the use of blended learning and/or immersive technologies for anatomy education since 2015, and highlights the content and context of anatomy studied, the approaches and technologies applied, and the geographical locations of the studies. The Google Scholar, Researchgate, and Scopus platforms were used to search for and identify relevant articles to include in the table, as these are the most popular and reliable repositories of research articles. The table shows that there is limited research on the use of mobile AR-based technologies for the study of anatomy in general, and even less so in South Africa and the African continent as a whole. This was therefore one of the rationales for the current study.

Table 1.
The recent trend of blended learning with immersive mobile AR technologies in anatomy education.
3. Design Approach and Methodology
Many factors were considered when developing the Anat_Hub tool (an immersive AR mobile application):
First, we considered the cognitive model where emphasis is placed on the mental mechanisms humans use in order to acquire new information or comprehend information [37]. The cognitive model consists of three theories: the social constructivist theory, information processing theory, and metacognitive theory [37]. All of these theories influenced the Anat_Hub application design and development. For example, the application stimulates student interaction with the material (social constructivist theory) and the information within the application is presented in an organized manner in order to help students learn content in an organized way (e.g., displaying first an image showing the upper limb with the location of the muscles, which can then be further broken down to provide finer detail such as its origin) (information processing theory). Finally, the application allows for self-testing with the incorporation of a quiz (metacognitive theory).
Second, the cognitive model theories led us to consider the VARK learning style theory. This theory is directly linked to academic performance and students’ choice or preference for resources when learning content [38]. Therefore, during the development of the application, we aimed to cater to various learning style preferences, including visual, aural, reading or writing, and kinesthetic. The application thus takes into account the following: (i) visual learning preferences in the form of 3D anatomical models, 3D animations, and 2D gifs that are incorporated into the application to enhance visualisation of theoretical concepts; (ii) aural learning preferences in terms of providing students the option of listening and learning content via audio attached to the information panels in the application as well as providing students with additional sound feedback to stimulate their interest; and (iii) reading or writing learning preferences, as it provides students with structured reading materials to the extent of providing labels, information panels, and a glossary (e.g., presented in a textbook format); and (iv) kinesthetic learning preferences as the AR feature within the application would naturally require students to physically move around the model in order to zoom in or out and move toward or away from the 3D model to interact with it in all anatomical views.
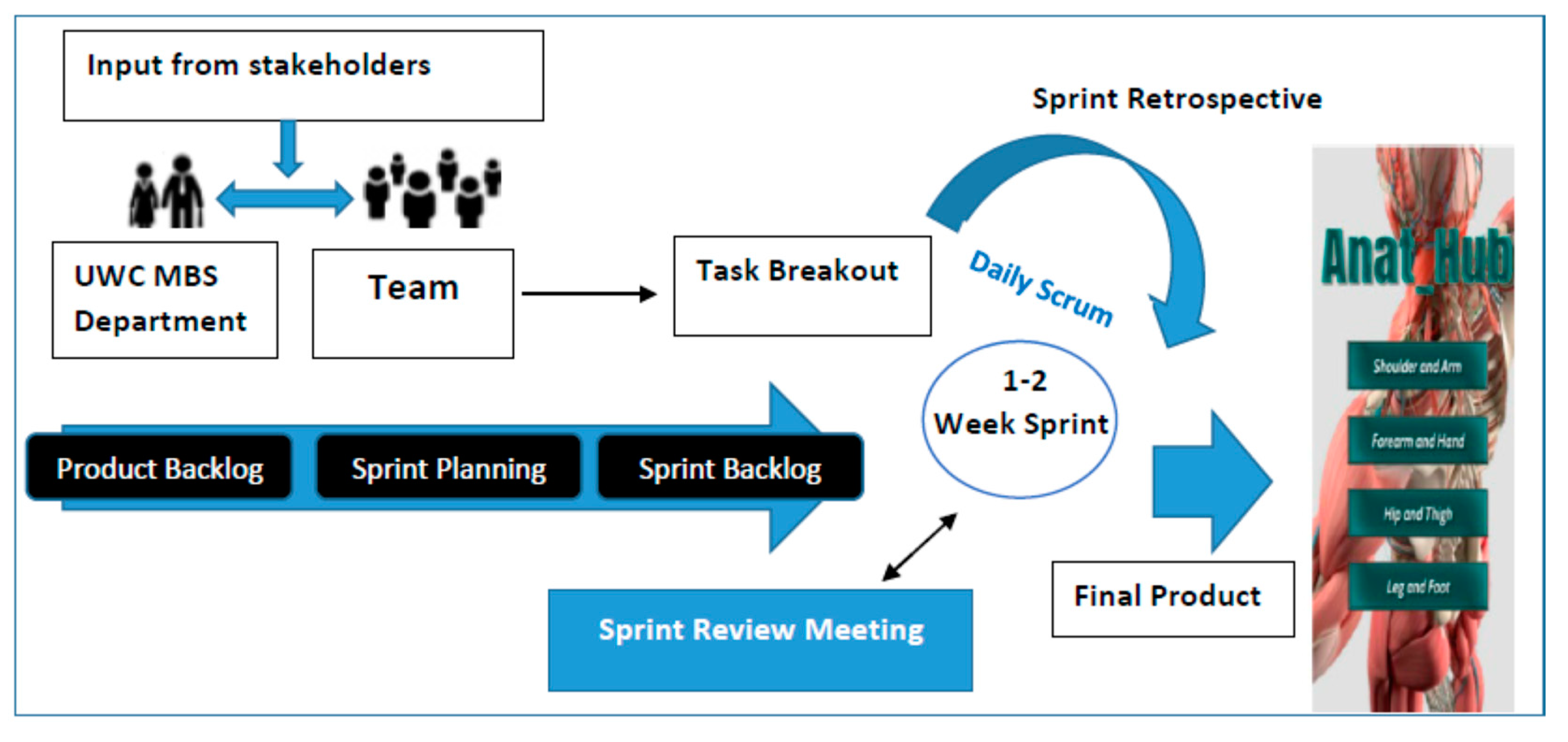
Lastly, the Anat_Hub application was developed using a similar strategy to that of Khalil’s four-step blended learning framework previously mentioned [5], together with the Agile Scrum methodology (consisting of a prioritized backlog of tasks for incremental development) [39]. The first phase of the framework entailed analysis and planning, which, in our case, involved a participatory design approach whereby all stakeholders, such as the development team and clients, had equal input in the application development process [40]. The involvement of the client in all stages of the software development meant that the quality of the final product may well meet the client’s expectations. The second phase involved design and development, whereby we adopted scrum as seen in Figure 1, which consisted of continuous improvements in the quality of the application by using sprints that lasted 1–2 weeks on average. This was executed by daily stand-up meetings where the backlog, progress, and issues were addressed [41,42]. Thus, at the end of each sprint a functional product was deployed and released to the client for testing and feedback. Interestingly, we found the Waterfall methodology adopted by Jamali et al. (2015) [13] and Patil et al. (2021) [27] to be restricting, and therefore chose the Agile Scrum methodology as it does not require a finalized plan to start developing, and therefore building and testing the application can be done as soon as possible [43]. The third phase was the implementation of the application where we gave anatomy students access to the Anat_Hub application. Lastly, the evaluation phase of this project adopted a mixed methods approach in order to investigate the experiences of anatomy students when using the Anat_Hub AR application. This was accomplished through the means of pilot study using a rudimentary user experience and technical evaluation survey.
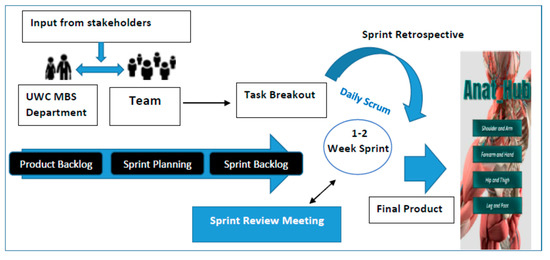
Figure 1.
A simplified breakdown of the adopted agile scrum methodology.
3.1. Data Collection and Requirements Gathering
To ensure that the participatory design approach and agile scrum methodology were correctly followed and implemented, the data collection process was divided into three sections: unit testing (cross-communication between teams); primary testing (meetings were regularly scheduled with clients and supervisors for progress updates and feedback); and secondary testing (requesting feedback from first-year students registered for anatomy modules in the following disciplines: medical bioscience, nursing, sports and exercise science, occupational therapy, physiotherapy, pharmacy, and dentistry). A Google Forms survey was provided to the students to evaluate their perception of the functionality, usability, and experience when using the Anat_Hub application. Informed consent was obtained from the participants, using a Google Form, prior to accessing the survey. The teams, clients, and supervisors provided feedback throughout the application development period to ensure that the relevant 3D models used were presented and configured in an acceptable and realistic manner, while feedback was obtained from the students once the final application was launched. Frequent feedback was necessary to ensure that the aim and specific objectives for the application development process were met.
3.2. Application Design and Development
The design and development process of the application followed a systematic approach from prototyping to user interface design with different sprints, and then the final product.
3.2.1. Prototype
The development process first consisted of planning and prototyping of the application and its contents to ensure that a consensus was reached on what the expected outcomes would be. After gathering initial requirements from stakeholders (clients and supervisors), a prototype was created using Framer and subsequently Unity (see Table 2). A minimum viable product (MVP) was used as a strategy to benchmark the outcomes of the application with the core rudimentary features required, which best represented the purpose of the application. The features for the MVP were acquired from use case scenarios and feedback from the client (UWC Medical Bioscience department).
Table 2.
Functions of the various software and hardware used for the Anat_Hub application development.
3.2.2. User Interface (UI) and Experience Elements (UX)
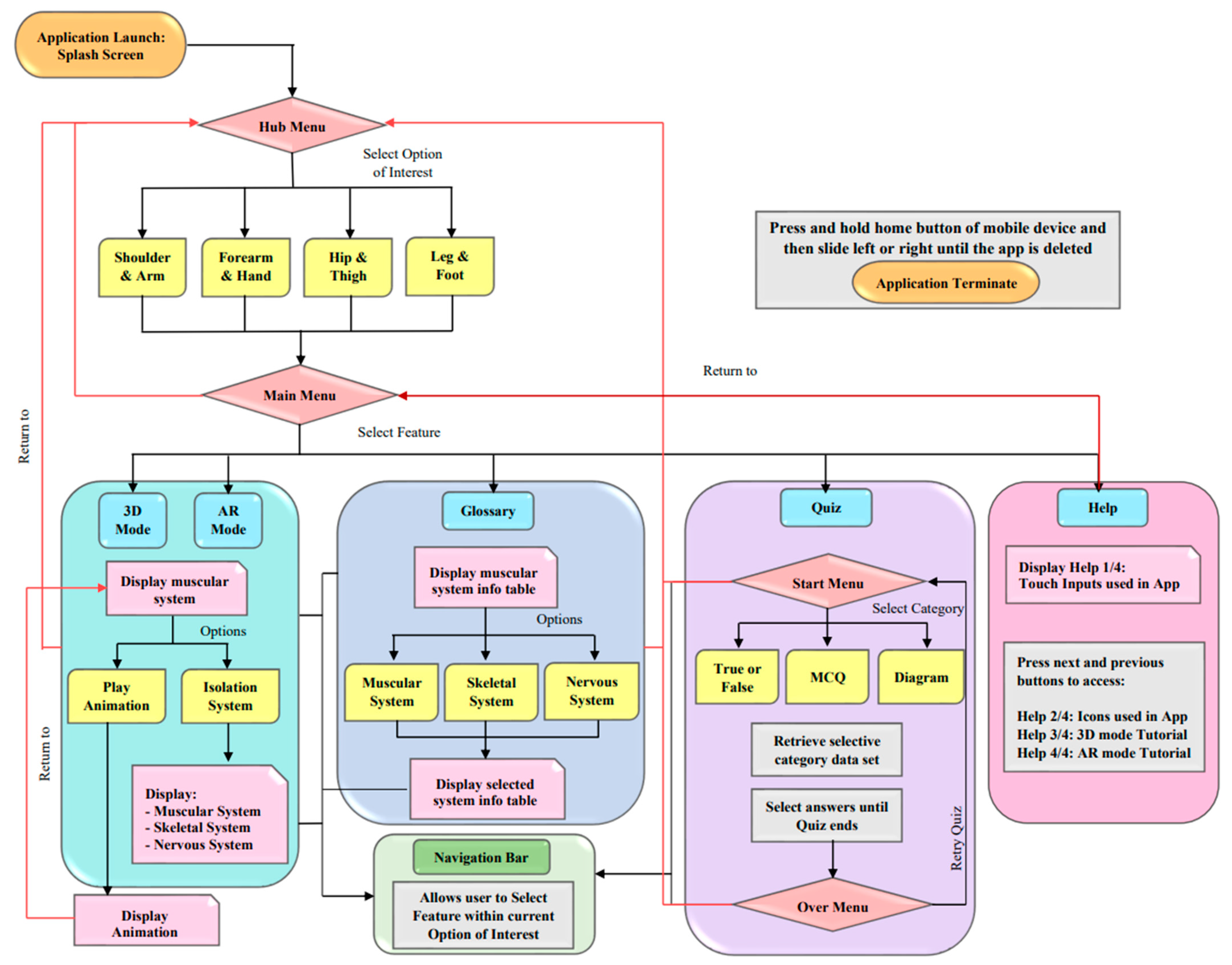
The functionality of the Anat_Hub application user interface (UI) was created using Unity (cross-platform game engine). The application’s touch interactions were kept to three variants: tap to interact with icons or models, double-tap to zoom in and out of models, and swiping up and down to scroll. The application’s flow and structure allow the user to intuitively navigate through the application with simple and comprehensible guidance (Figure 2). The icons and design elements were created using graphics editors: Krita, Photopea and Adobe photoshop. Some 3-D models of the human upper and lower extremities were supplied to be incorporated for users to navigate and interact with. The software, Autodesk 3ds max, was necessary to manipulate, rig, and animate the models with the modifier and motion tools. The sound incorporated into the application was used to enhance user experience and provide users with a feedback response for UI and 3D model interaction. Table 2 provides a detailed summary of various software and hardware required to achieve a functional immersive application.
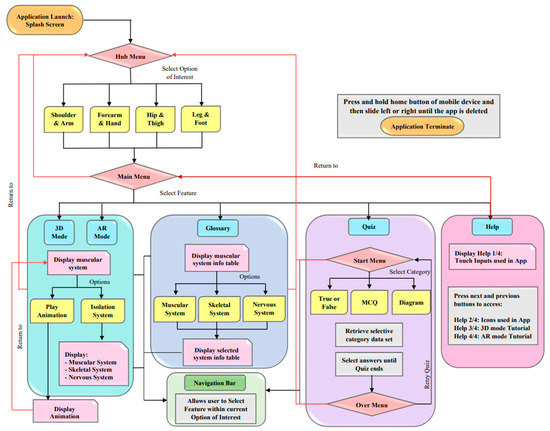
Figure 2.
Flow chart depicting the flow and navigation of the Anat_Hub application.
3.2.3. Deployment Device Specifications
The application was designed, built, and deployed for an android mobile device that supports a minimum API of 26 (Android 8.0 ‘Oreo’) to maximum API level 30 (Android 11), using Vuforia marker-less ground plane detection. The application size is approximately 300 MB and it is internet-independent. During the development period, it was determined that the optimum (suitable) mobile screen aspect ratio is 16:9. However, the application is still functional on other screen aspect ratios.
3.3. Target Audience and Application Output
The Anat_Hub application seeks to assist undergraduate health sciences students at the University of the Western Cape (UWC) to learn and understand the basic musculoskeletal anatomy of the upper and lower extremities, by allowing them to visualize and interact with 3D models in an immersive and non-immersive manner. The MVP and main outcome of the application consist of core features: AR mode, 3D mode, Glossary, and Quiz. The “Clinical Anatomy by Regions” ninth edition by Richard S. Snell was used as a source to add anatomy content to the muscle information panels in the AR and 3D modes, glossary, and quiz. This was done so that we could provide users with information that aligns with the standard anatomy curriculum.
4. Implementation, Results, and Discussions
The research approach and methodology were successfully implemented in order to meet the application and device specifications as set out in Section 3. The product delivered (called Anat_Hub) is an education-based learning tool that incorporates immersive technology to assist students in understanding the musculoskeletal anatomy of the human upper and lower extremities. It was developed to meet the needs and specifications set out by the UWC Medical Bioscience department; however, it could be adapted for anatomy teaching and learning in general.
4.1. Application Navigation and Features
The initial Android package (APK) deployed, the MVP, was based on the framer prototype created to display the navigation and functionality of the Anat_Hub application. This MVP was used as a benchmark for testing and the following improvements (based on feedback) were made to the features within the application.
4.1.1. Interface: UI Navigation (Touch Inputs), Orientation, and Sound
The initial orientation of the application was in landscape; however, the entirety of the application was changed to portrait except for the Glossary feature. This was to allow the 3D models displayed to be viewed in an anatomical position and allow the tables in the glossary feature to be displayed optimally and viewed without strain in landscape. To navigate the application, a simple single tap touch input was used. However, this was later adapted to further improve the navigation to a single tap to only interact with models and UI buttons; double-tap to zoom, swipe up and down to scroll through information; and slide across the screen to rotate the model (later updated with a rotational UI button). To improve navigation between features within the application, a Home button and Navigation Bar is present throughout the application since the development of the initial APK deployed. Near the end of the development period, background sound was added to the Hub, Main, and Quiz Start and Over menus; additionally an application icon and splash screen (containing application name, university, and Unity logo) was incorporated into the application. All of these new elements were added in an effort to improve the user interface and user experience. The UI interface (icons, buttons, colour palette, etc.) of the application was constantly updated to enhance user experience, as presented and discussed in the subsequent sections hereafter.
4.1.2. Hub Menu
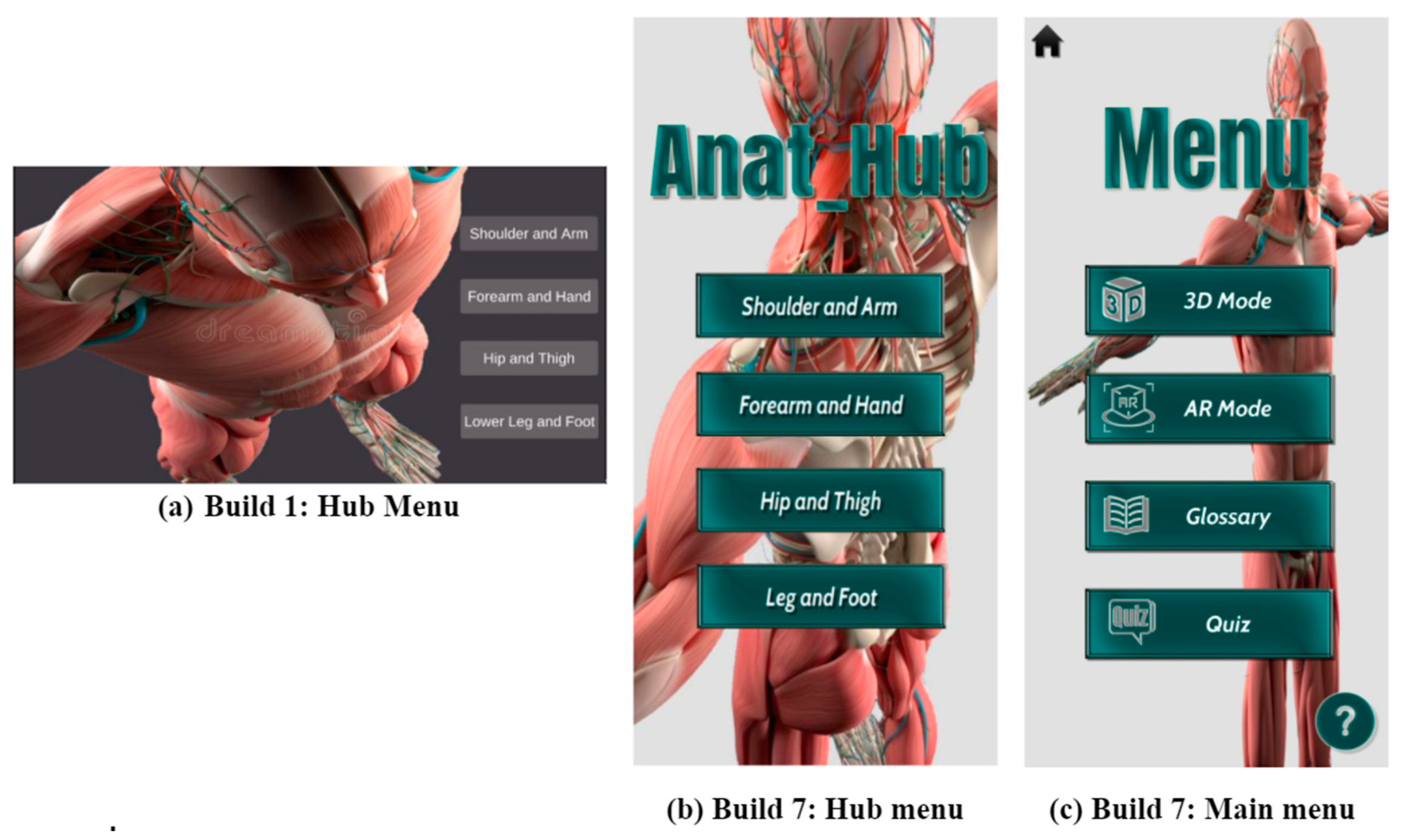
Once the application launches, the user will encounter the Hub menu, which allows them to choose an option of interest from the four possible menu options, which are: (i) shoulder and arm; (ii) forearm and hand; (iii) hip and thigh and (iv) leg and foot to explore (Figure 3a). However, as each option of interest was developed similarly besides its particular models or content, only the “shoulder and arm” option is presented in this paper for the sake of simplicity. The original prototype included four individual applications to be carried out for each option of interest, which were eventually integrated to form a Hub. The application was integrated due to the similarities in navigation and design with the exception of the “realistic” models and its particular content within each option of interest. The Hub Menu was then updated regarding orientation, application name and background (Figure 3b).
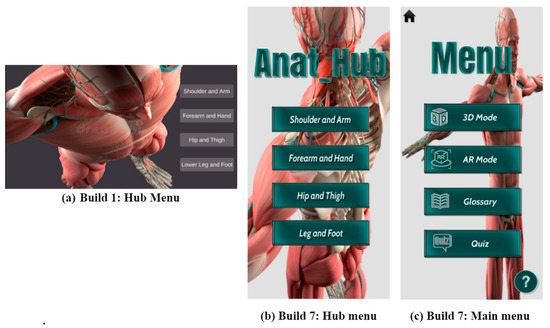
Figure 3.
The changes made to the Hub and Main Menu, including final UI design and placement, during application development.
4.1.3. Main Menu
When the user chooses their option of interest, they would encounter a main menu that was later incorporated into Build 7 upon the client’s request. The main menu allows the user the choice of which features to select among the four key features available (Figure 3c): (i) 3D mode (non-immersive functionality); (ii) AR mode (immersive functionality); (iii) Glossary (containing tables with more detailed information on the muscles, bones, and nerves); and (iv) Quiz (to test user knowledge). The final progression of this menu, including the addition of the application name, Home and Help UI button, is shown in Figure 3.
The main menu allows access to important features such as the following:
- (i)
- 3D mode non-immersive functionality
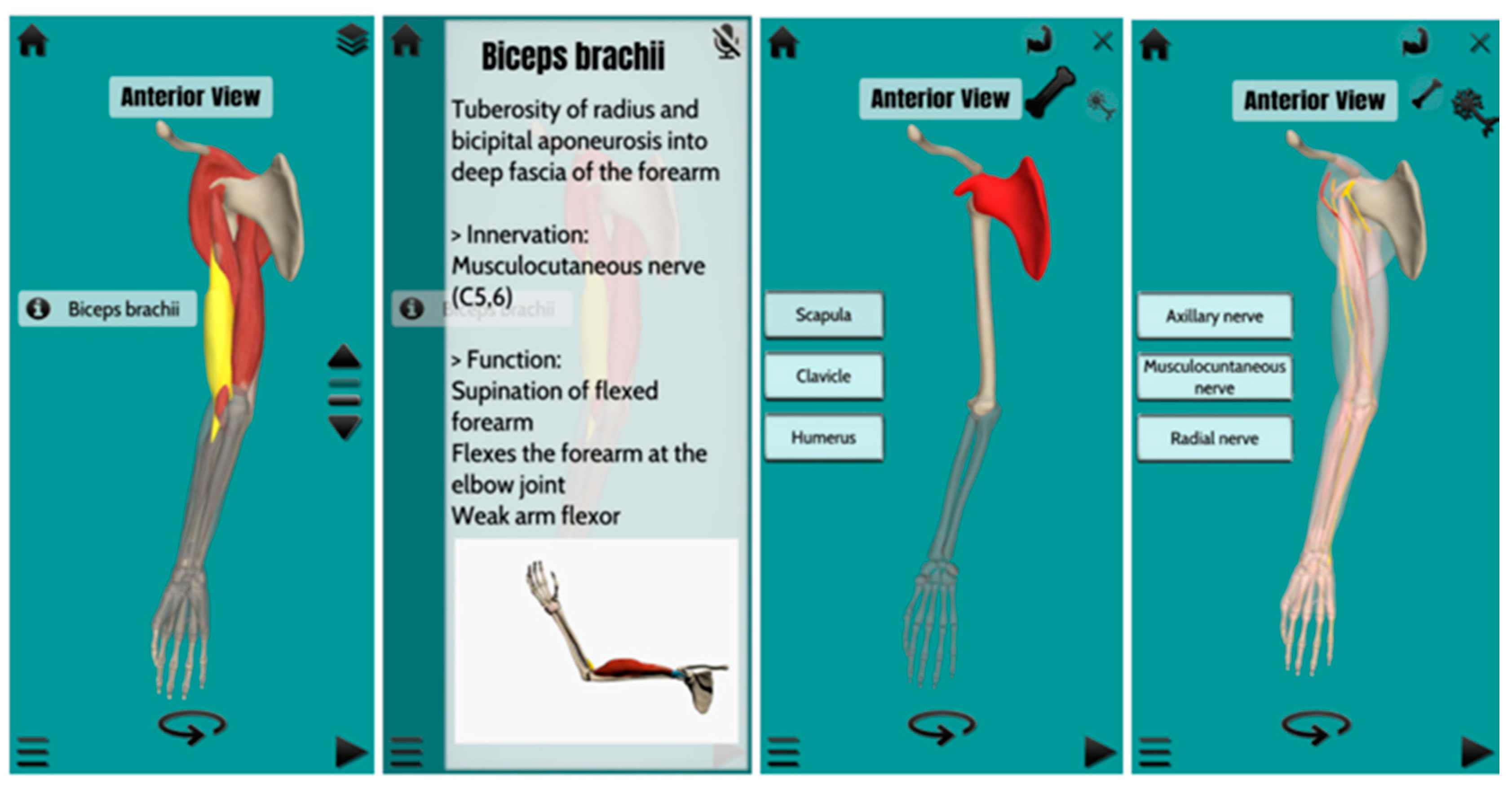
In the 3D mode, using a System Isolation UI button (top-right of mobile screen on Figure 4b and Figure 5), the user can interact with either the muscular, skeletal, or nervous components of the 3D models (Figure 4 and Figure 5). Although the application was developed for students to learn the muscular system, according to the client’s request, it was decided that the addition of skeletal and nervous system elements would make for a more integrated learning of how muscles work in relation to other anatomical structures. In order to obtain a deeper understanding of the musculoskeletal system, the user can further isolate the musculoskeletal system into various muscle layers or compartments within the musculoskeletal system using a Muscle Layer UI toggle (middle-right of mobile screen in Figure 5).
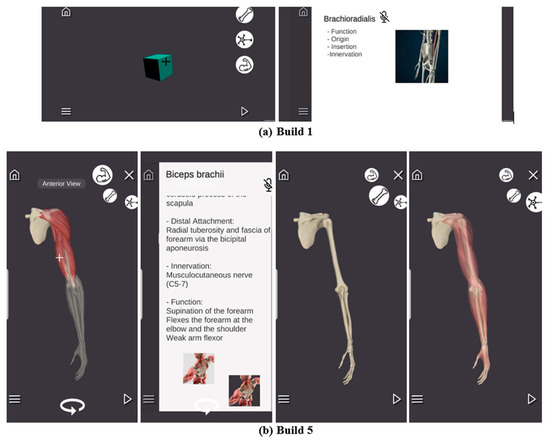
Figure 4.
The changes made to the 3D mode, including final UI design and placement, during application development.
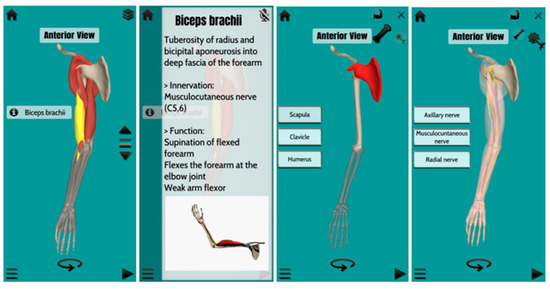
Figure 5.
The changes made to the 3D mode, including final UI design and placement, during application development.
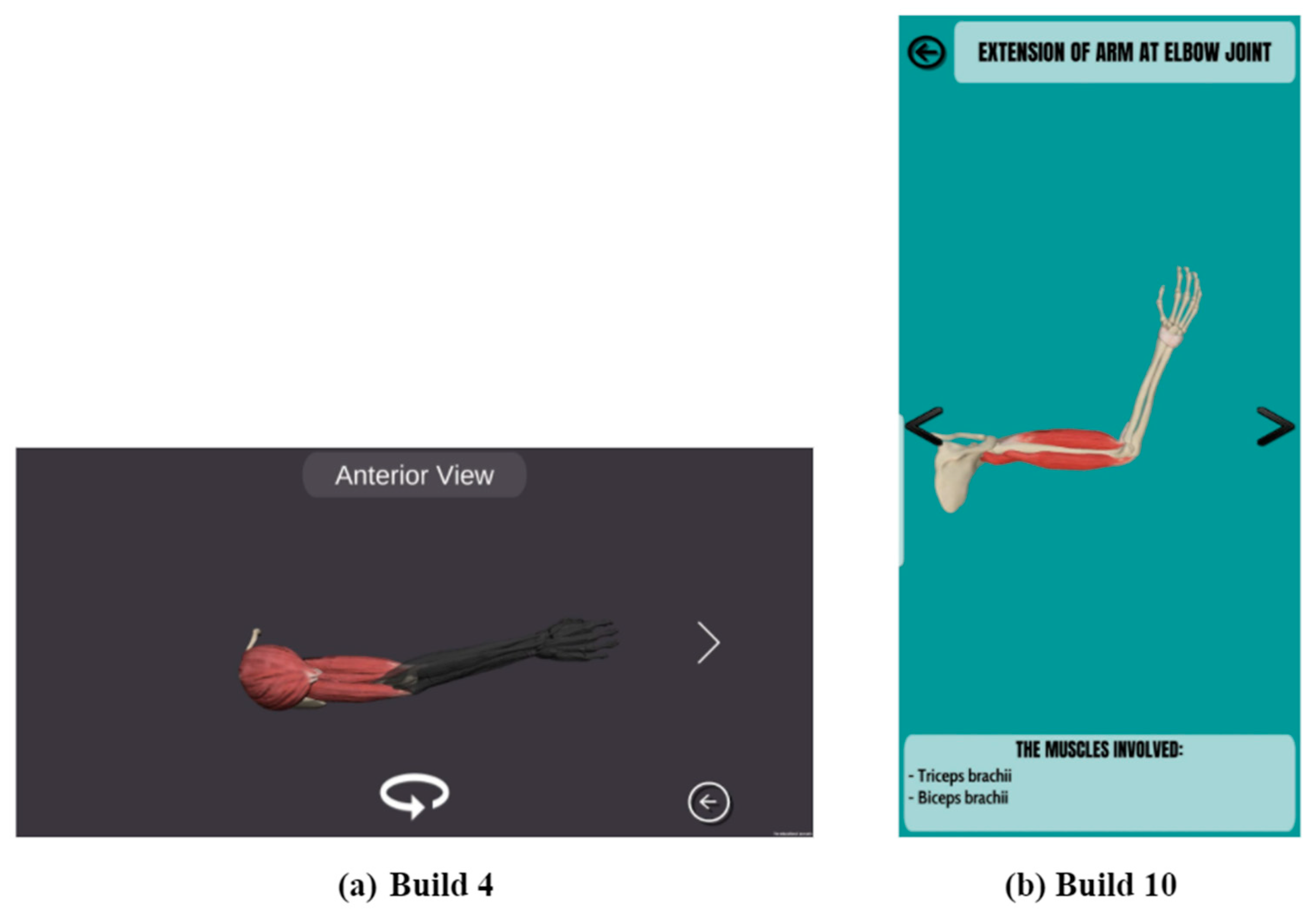
Furthermore, the user can rotate the model using the Rotation UI button (bottom-centre of mobile screen Figure 5), relocated from the Play Animation Figure 6a, to view the different anatomical positions (anterior, posterior, medial, lateral) with tags displayed top-centre of the screen (Figure 4b and Figure 5). Lastly, the 3D mode also contains a Navigation Bar (bottom-left of mobile screen), allowing easier navigation in order to access either the AR mode, 3D mode, Glossary, or Quiz within the option of interest, a Home button (top-left of mobile screen, returns the user to the Hub Menu), and an Animation UI button (bottom-right of mobile screen, which allows access to animations of muscle functionality that the user can observe) (Figure 4).
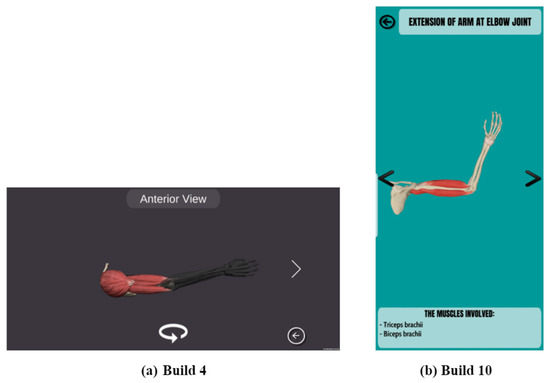
Figure 6.
The changes made to the animation feature, including final UI design and placement, during application development.
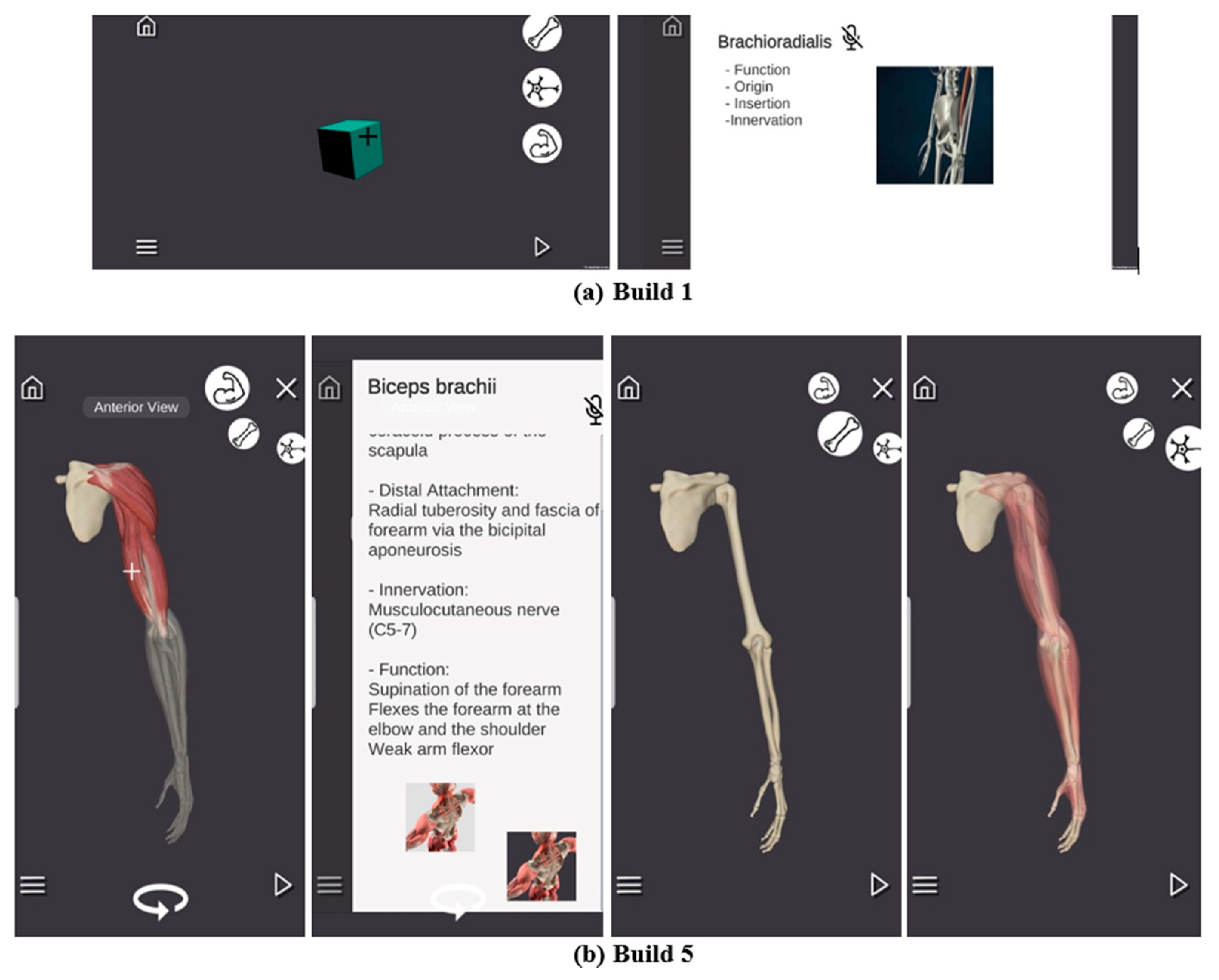
In APK Build 1, basic proxy non-interactive 3D shapes of various colours were used to differentiate and isolate the respective elements (muscular, skeletal, or nervous) as shown in Figure 4a. The proxy shapes were later updated to block-out models and subsequently replaced with “realistic” models by Build 5 (Figure 4a,b). By Build 7, the “realistic” models were edited and imported into all of the systems (skeletal and nervous system non-interactive). Similarly, the basic rotating proxy non-interactive 3D shape in the Play Animation section (accessed via an Animation UI button) was updated to a “realistic” model in Build 4 (Figure 6). The models were presented in this order so as to provide clients with a functional APK build at the end of each week and demonstrate the “direction” in which the application is going. All of the necessary models and information per muscle function were added by Build 9 and updated in Build 10 (Figure 5 and Figure 6).
In Build 1 and 2, a single “+” marker representing a particular muscle selection touch input was interactive (Figure 4a); once tapped, the particular interactive muscle name would appear to allow the user access to an information panel overlay with more information on the muscle origin, insertion, innervation, action, and gifs, as well as voice-over audio with the same content (Figure 4a, e.g., Brachioradialis). Eventually, the “+ then pin” marker was removed, and replaced by Build 8 with a single tap touch input to highlight and interact with the model in an easier manner (Figure 5, e.g., Biceps brachii). However, the information and audio files were only functional by Build 9, and by the 10th build its visual design was improved with the addition of gifs of the muscle function (Figure 4b and Figure 5; e.g., Biceps brachii).
- (ii)
- AR mode immersive functionality
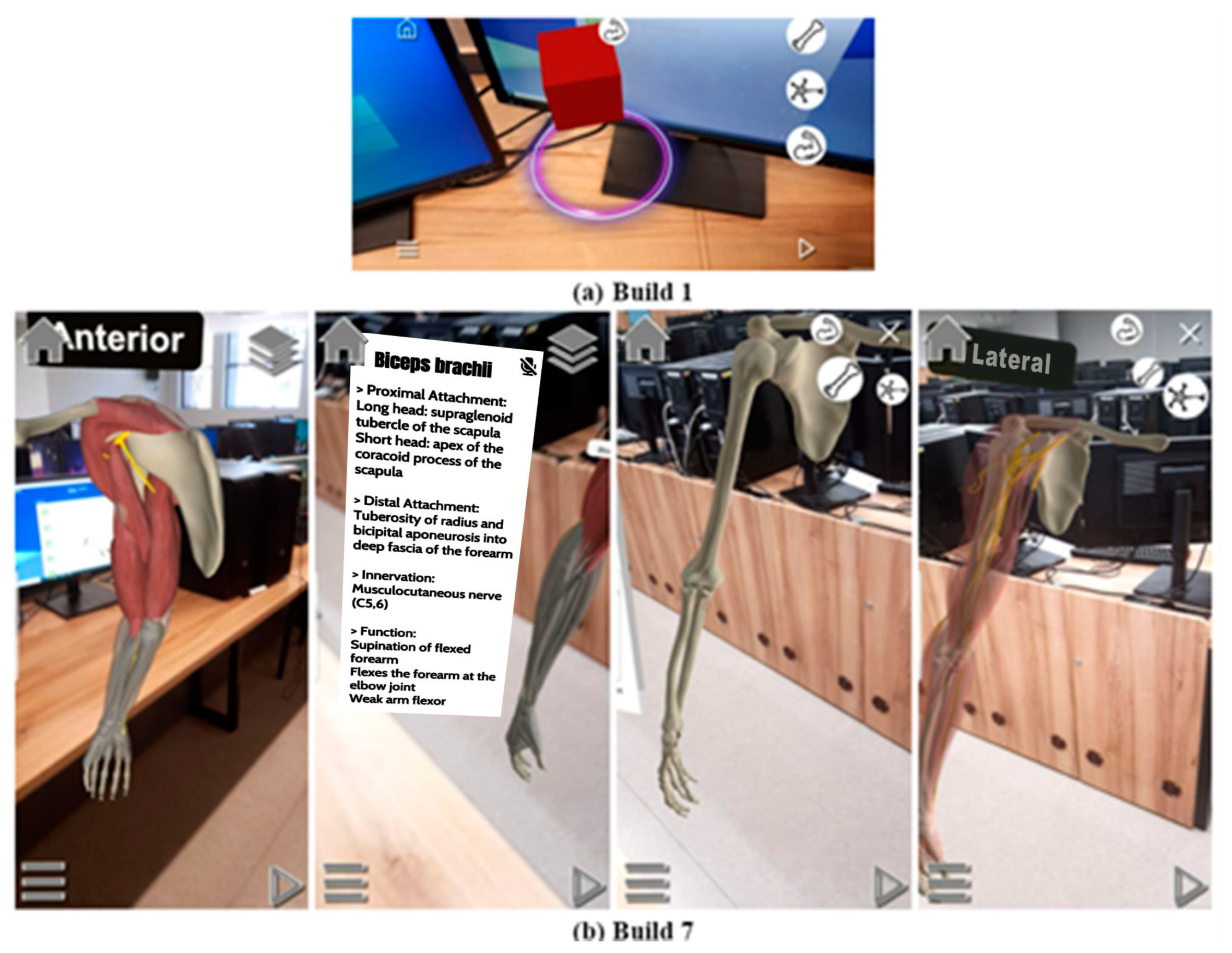
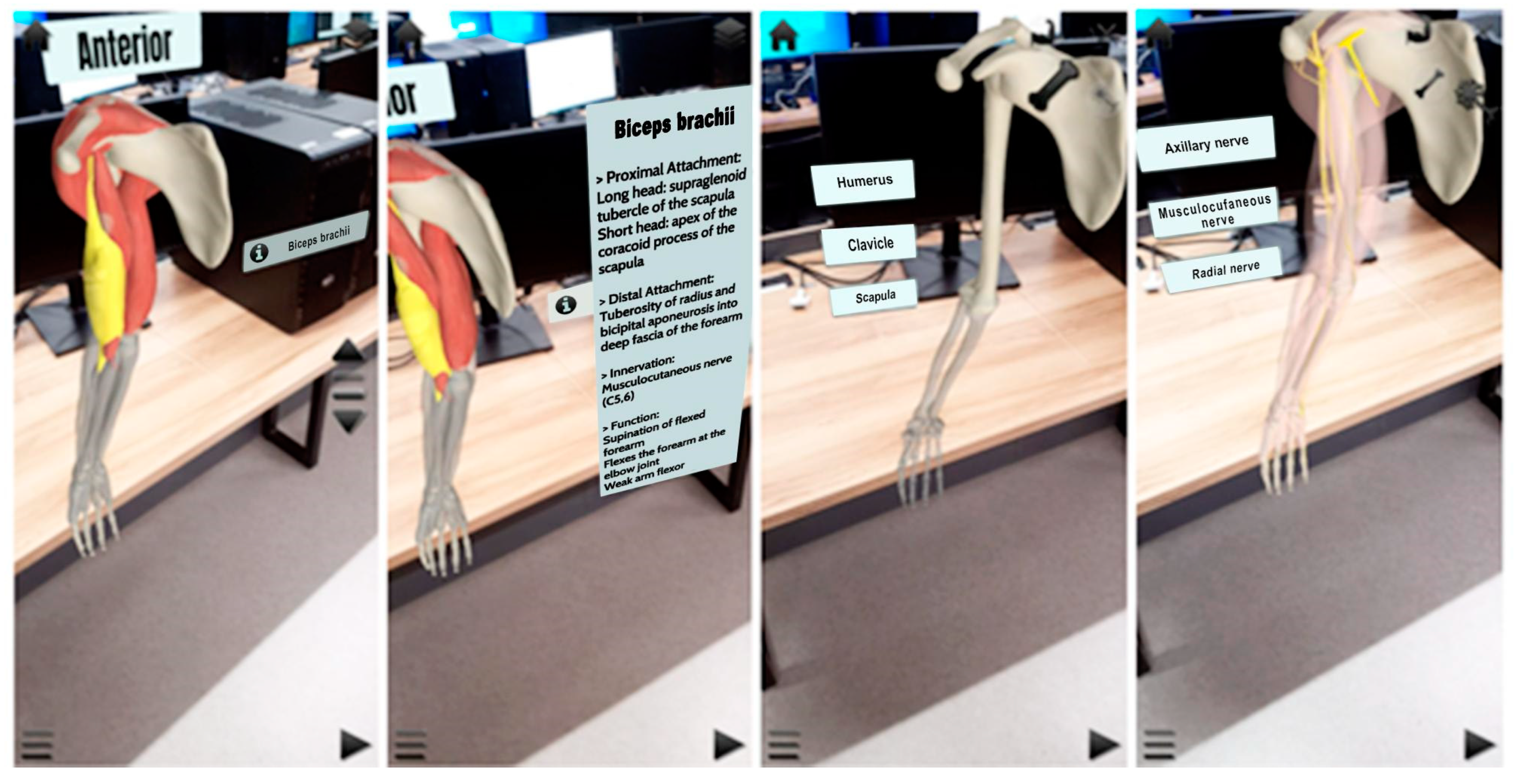
The AR mode is designed similarly to the 3D mode, with the exception of required access to the mobile device camera to detect a flat surface to “spawn life-size” models in the real-world environment. Originally, the AR feature was developed using AR Foundation in conjunction with the ARCore SDK, where the user would encounter the AR mode with the use of their mobile device camera. The camera would detect and utilize a flat surface to produce an interactable “purple ring surface indicator” required to tap on the screen and “spawn life-size” models in the real-world environment (Figure 7a). However, by Build 7 the application made use of Vuforia marker-less ground plane detection as this made it easier to “spawn life-size” models and avoid the instability of the models displayed when using AR Foundation (Figure 7b). The platform change was also easier to operate/navigate in terms of scripting. To add a layer of immersiveness and increase user interest, another difference is the placement of the muscle labels and muscle information panels that were relocated in Build 7 to display next to the model (World UI) as opposed to on the screen overlay (Figure 7b). The final progression of the AR mode can be seen in Figure 8.
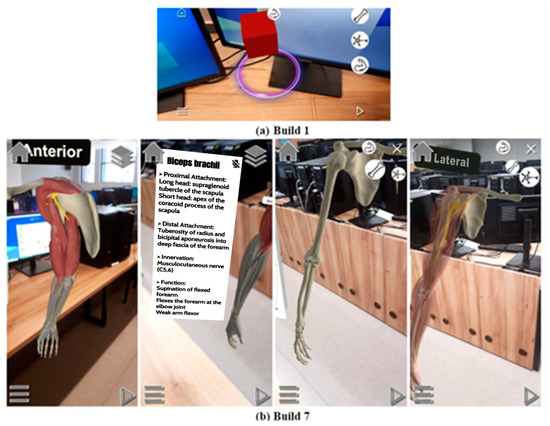
Figure 7.
The changes made to the AR mode, including final UI design and placement, during application development.
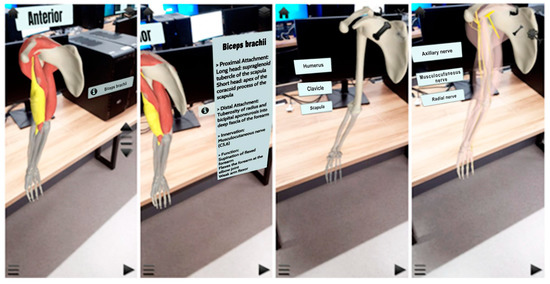
Figure 8.
The changes made to the AR mode, including final UI design and placement, during application development.
- (iii)
- Glossary
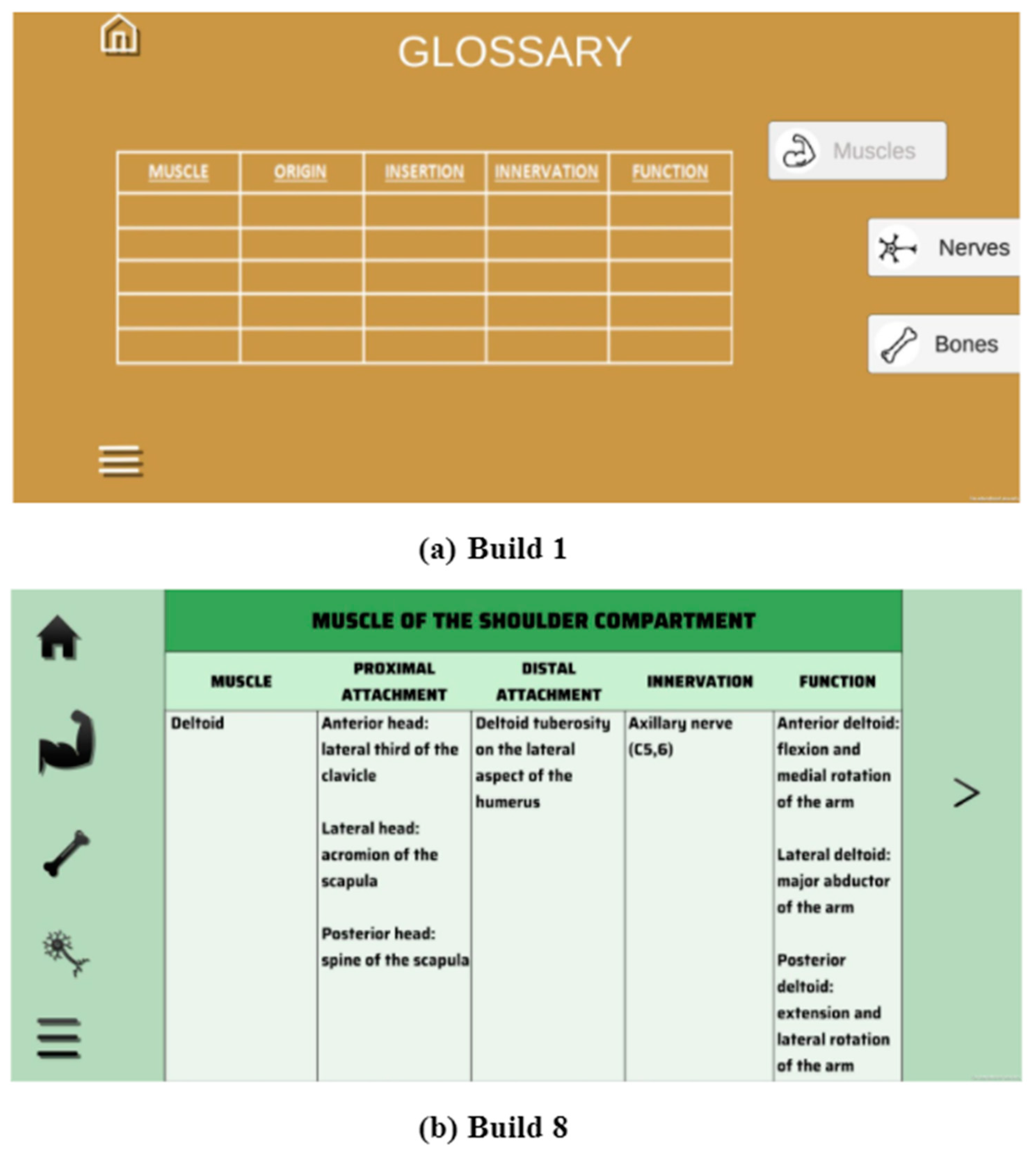
The glossary contains tables with more detailed information on the muscles, bones, and nerves. Initially, two of three system UI buttons were inactive, and only the musculoskeletal system was active with sample images being used to represent the musculoskeletal system table of information (Figure 9a). However, by Build 5 all of the UIs were active with relevant sample images for each system as well as the addition of “next” and “previous” UI buttons. Finally, in Builds 6 to 8, the sample images were replaced with functional interactive (scrollable) Unity tables, a simple table UI, which is an asset from the Unity asset store, so as to display the tables optimally and improve user experience (Figure 9b). The progression of this feature, including the final UI design and placement, can be seen in Figure 9.
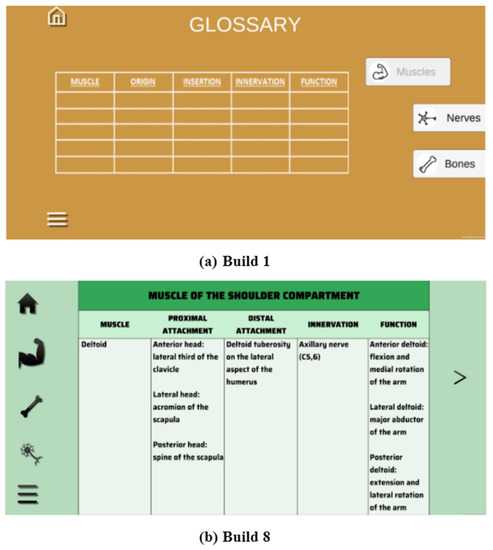
Figure 9.
The changes made to the Glossary feature during application development.
- (iv) Quiz
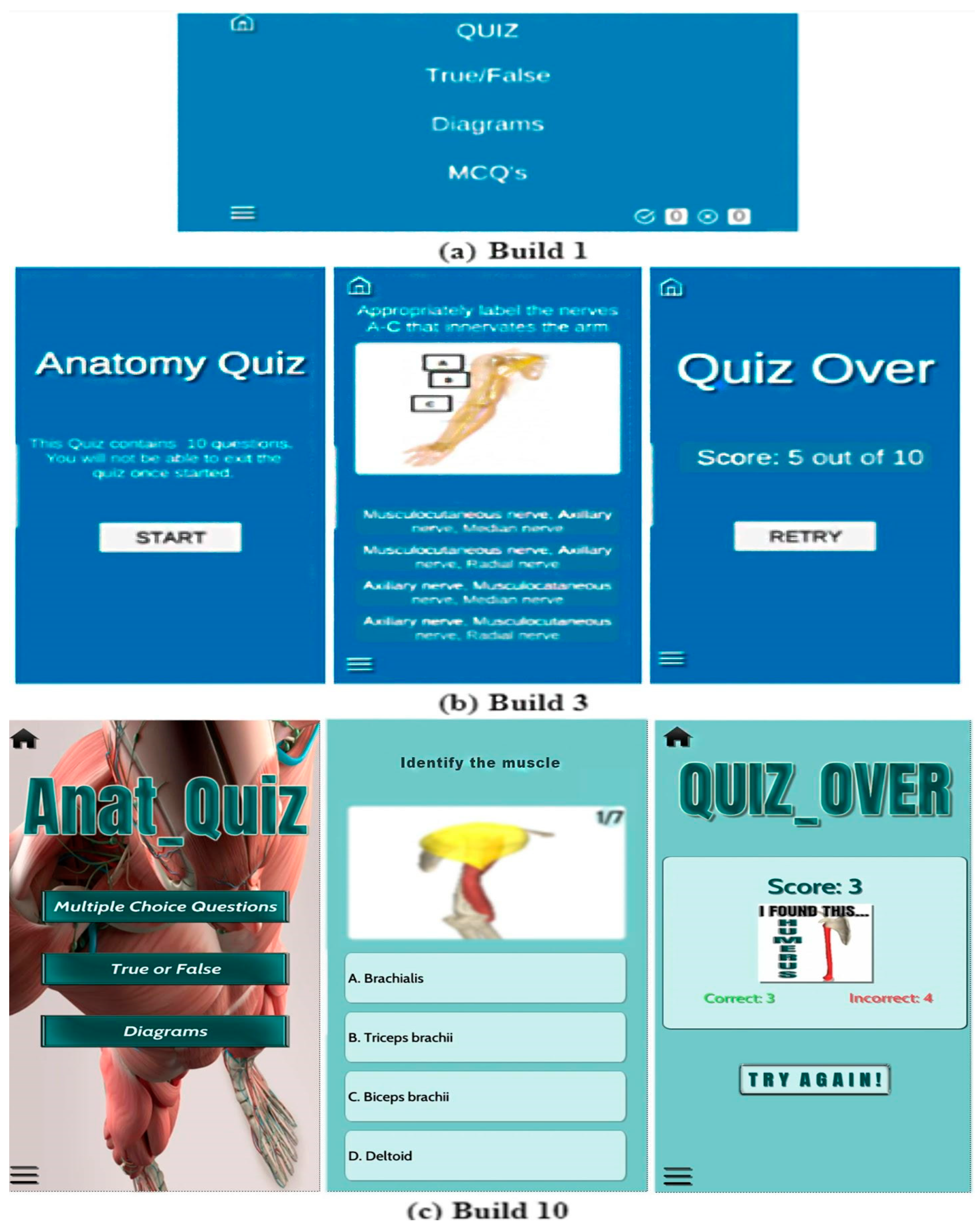
The quiz feature was incorporated to test user knowledge on the content within the application. Initially the quiz was set up to consist of one quiz that contains true or false (T/F), diagrams, and multiple-choice (MCQ) types of questions as well as a simple scoring system (correct and incorrect); see Figure 10a.
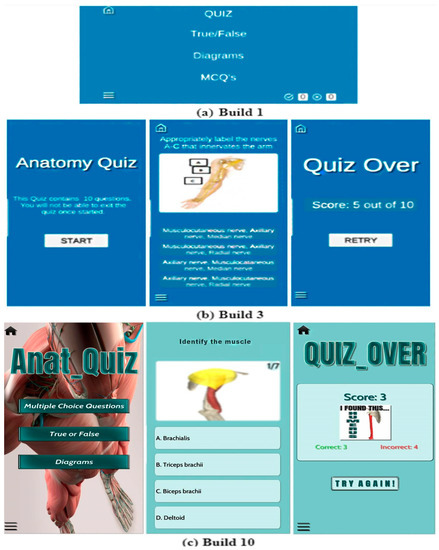
Figure 10.
The changes made to the Quiz feature during application development.
In build 3, a Quiz Start Menu (start UI button) and Quiz Over Menu (retry UI button), as well as a green highlight for correct and red highlight for incorrect answers were incorporated (Figure 10b,c). This was to allow the user a chance to adjust to a test mindset, to choose when to retry the quiz in order to retake the test and improve their retention of the content, and to improve application navigation and enhance user experience. Later, in Builds 8 to 10, the Quiz Start Menu was adapted to allow users to choose a particular category (MCQ, T/F, Diagrams) upon the client’s request to allocate more questions to each question type.
The scoring system underwent various programming and design changes from the original layout design planned (Figure 10a). In Build 3, the incorrect scoring system was removed. It is important to note that a functional scoring system (score and high score) was only achieved in Build 7. However, by Build 9 the high score was removed due to persistent bugs and coding errors. In Build 10, the final changes to the design of the scoring system was made (Figure 10c). Originally, all of the diagrams used in the quiz feature were sourced from Kenhub, however, due to copyright issues these images were replaced with original images (Figure 10c). The progression of this feature, including the colour palette and UI design and placement, is shown in Figure 10.
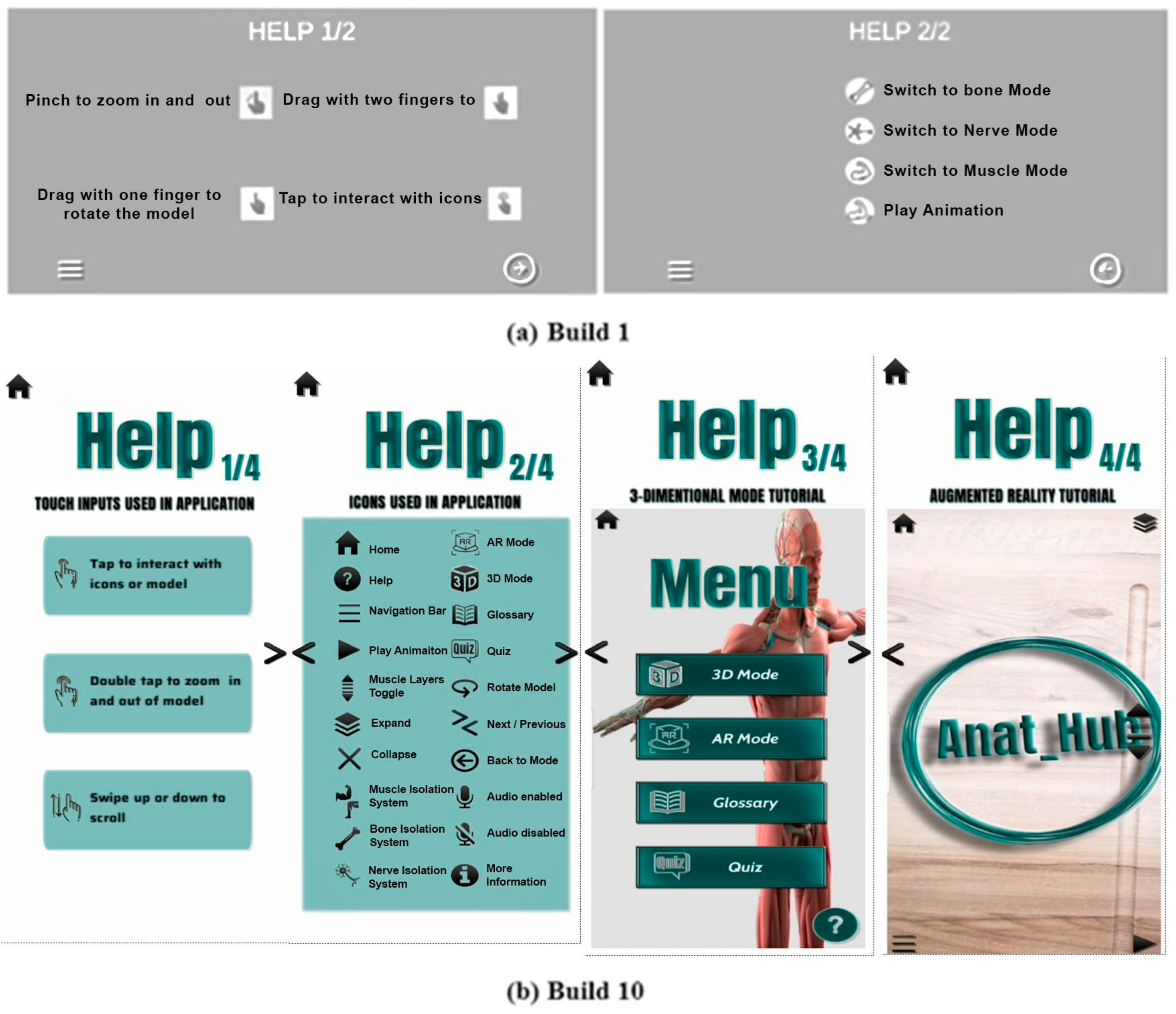
The main menu also allows access to an accessory feature, Help, which provides the user with a detailed explanation of how to navigate the application (Figure 11). Initially this feature was developed to provide explanations of the navigation touch inputs (hand gestures) and UI icons (Figure 11a). However, by Builds 4 and 10, AR and 3D mode video tutorials were added, respectively, in order to assist first-time users on how to navigate these modes (Figure 11b).
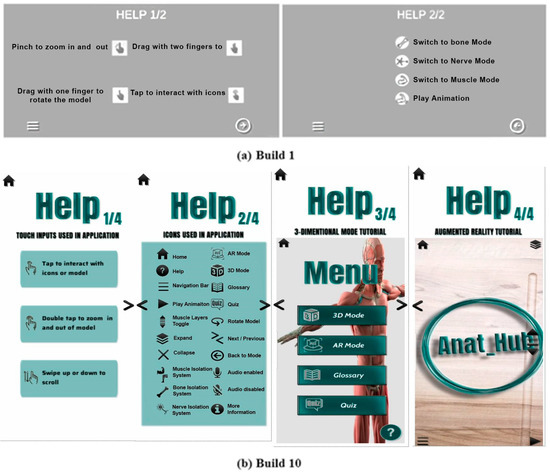
Figure 11.
The changes made to the Help accessory feature, including final UI design and placement, during application development.
4.2. Application Evaluation and Analysis
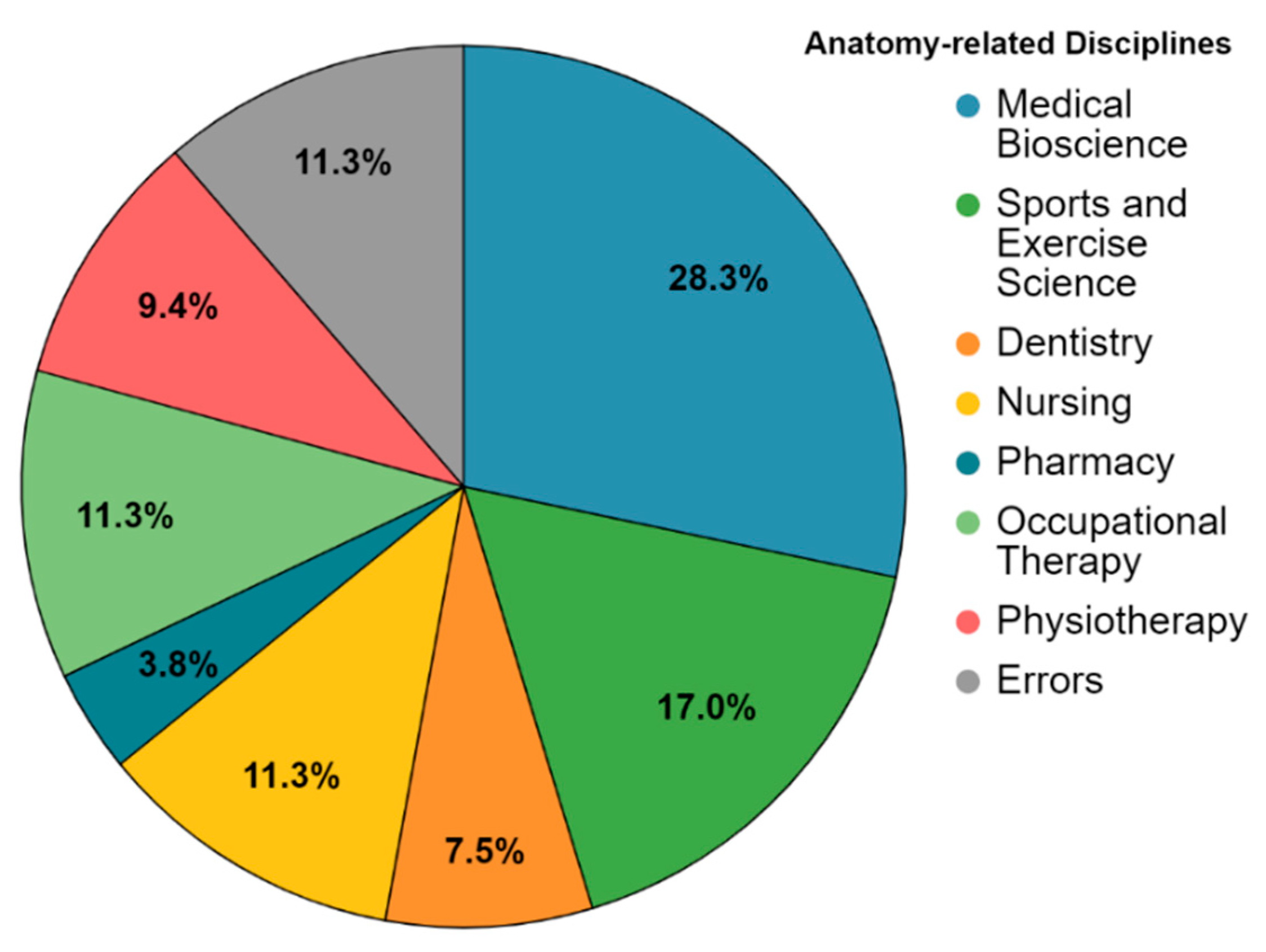
Following completion of the application design and development phase, the pilot study included a rudimentary user experience and technical evaluation survey that was conducted in order to gather data and feedback from first-year undergraduate volunteer students from several anatomy-related disciplines, including medical bioscience, nursing, sports and exercise science, occupational therapy, physiotherapy, pharmacy, and dentistry. These students were enrolled for anatomy modules offered by the Department of Medical Bioscience. The evaluation focused on the initial user experience of the functionality and usability of the Anat_Hub application. A total of 53 responses were captured and analyzed (as per Google form output) in order to understand user perceptions with a view to improving its future usage. The demographic information of the volunteer participants showed a male-to-female ratio of 19:34, respectively, and a higher response rate from students of the Medical Biosciences discipline (28.3%) (Figure 12). Participants with invalid entries for discipline of study were denoted as “error” (approximately 11.3%) (Figure 12), however, any other valid answers to the survey were still taken into account.
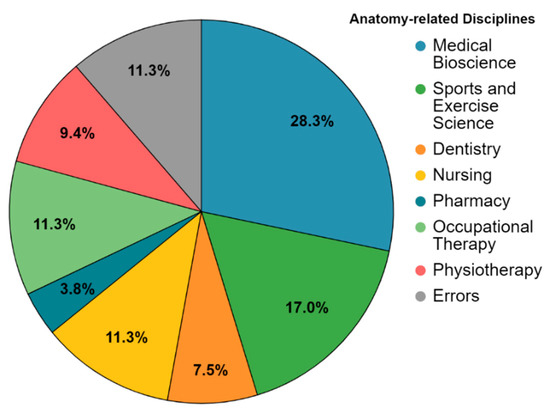
Figure 12.
Distribution of participants from various anatomy-related disciplines; “errors” denotes participants with invalid entries for discipline of study.
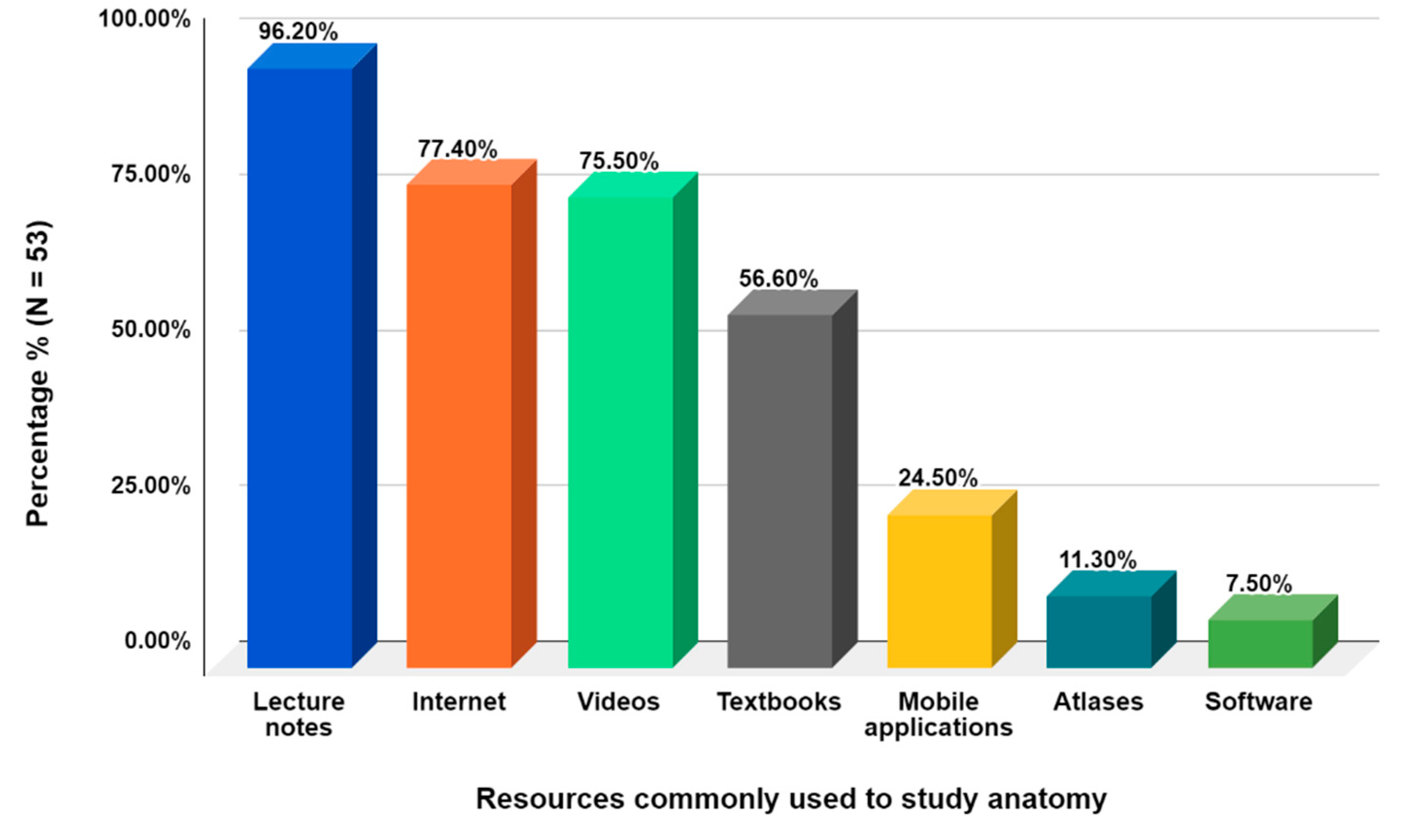
Prior to using the Anat_Hub application, the most commonly used resources to study anatomy by the participants were lecture notes (96.2%), internet sources (77.4%), videos (75.5%), and textbooks (56.6%). Students seemed to make less use of resources such as mobile applications (24.5%), anatomy atlases (11.3%), and e-learning software (7.5%) (Figure 13). In this survey, students were not specifically asked to indicate the type of software they have used.
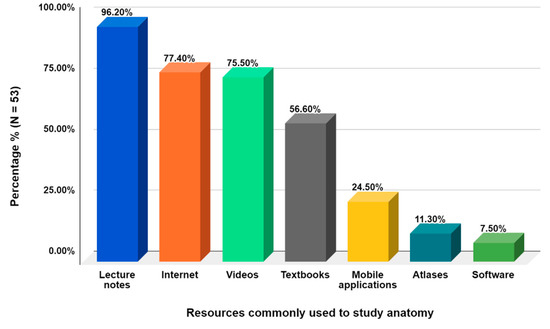
Figure 13.
The resources commonly used by students to study anatomy.
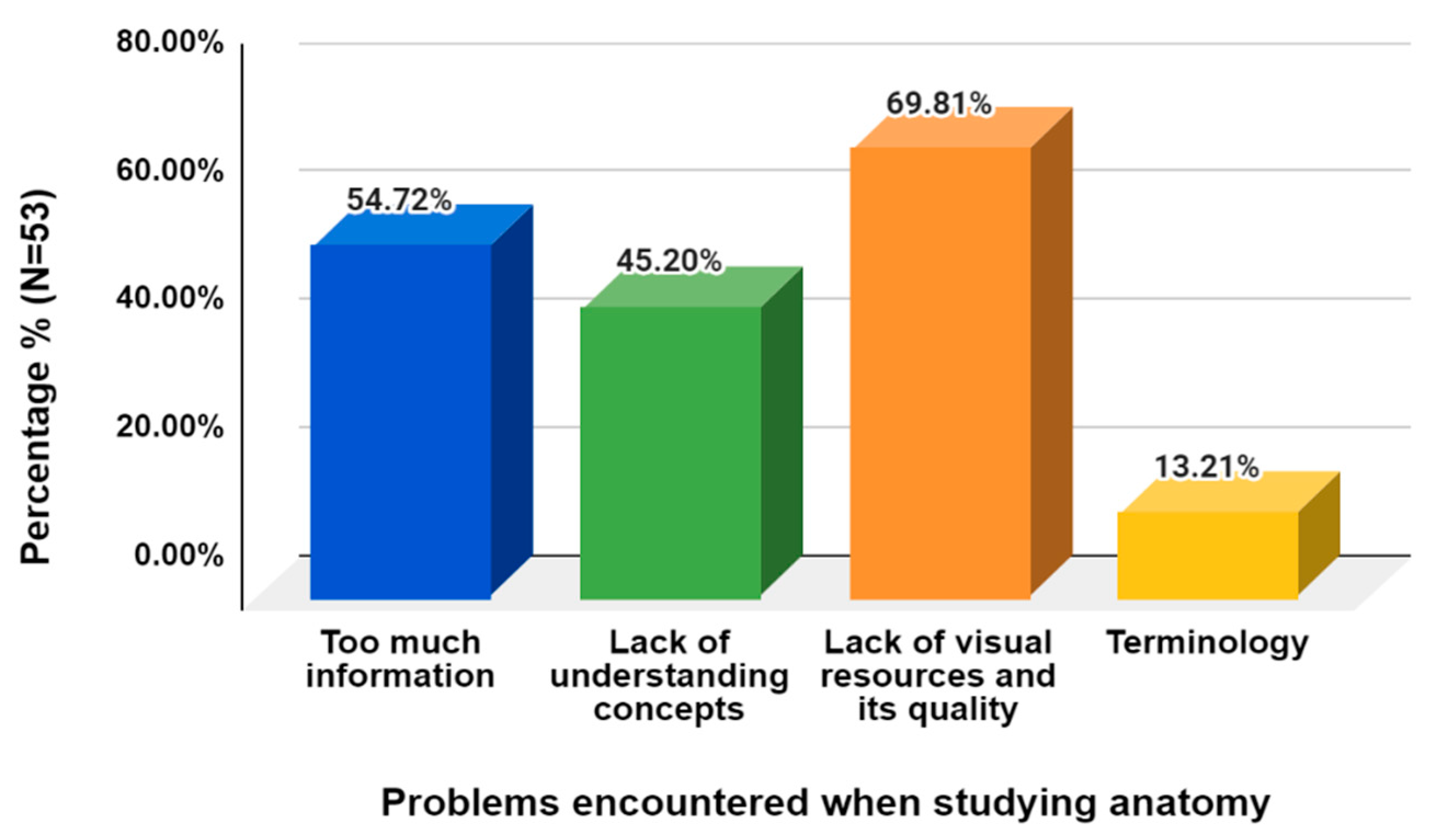
Furthermore, volunteers indicated that the problems encountered when studying anatomy include the lack of visual resources and their quality (69.81%), followed by too much information (54.72%), lack of understanding of concepts (45.20%), and terminology (13.21%) (Figure 14). As these are some of the challenges anatomy students are currently facing, Anat_Hub seeks to alleviate some of these by providing quality 3D visual resources, reducing and organizing information, and providing a text-to-speech component to assist students in grasping and understanding anatomical concepts.
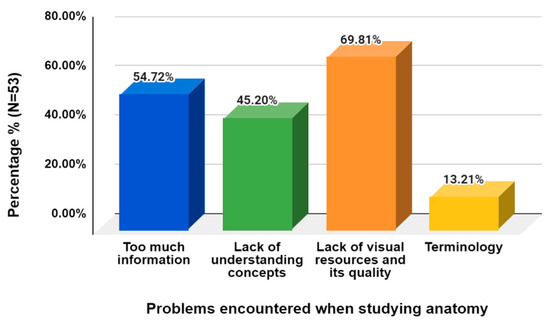
Figure 14.
Problems that participants usually encountered when studying anatomy.
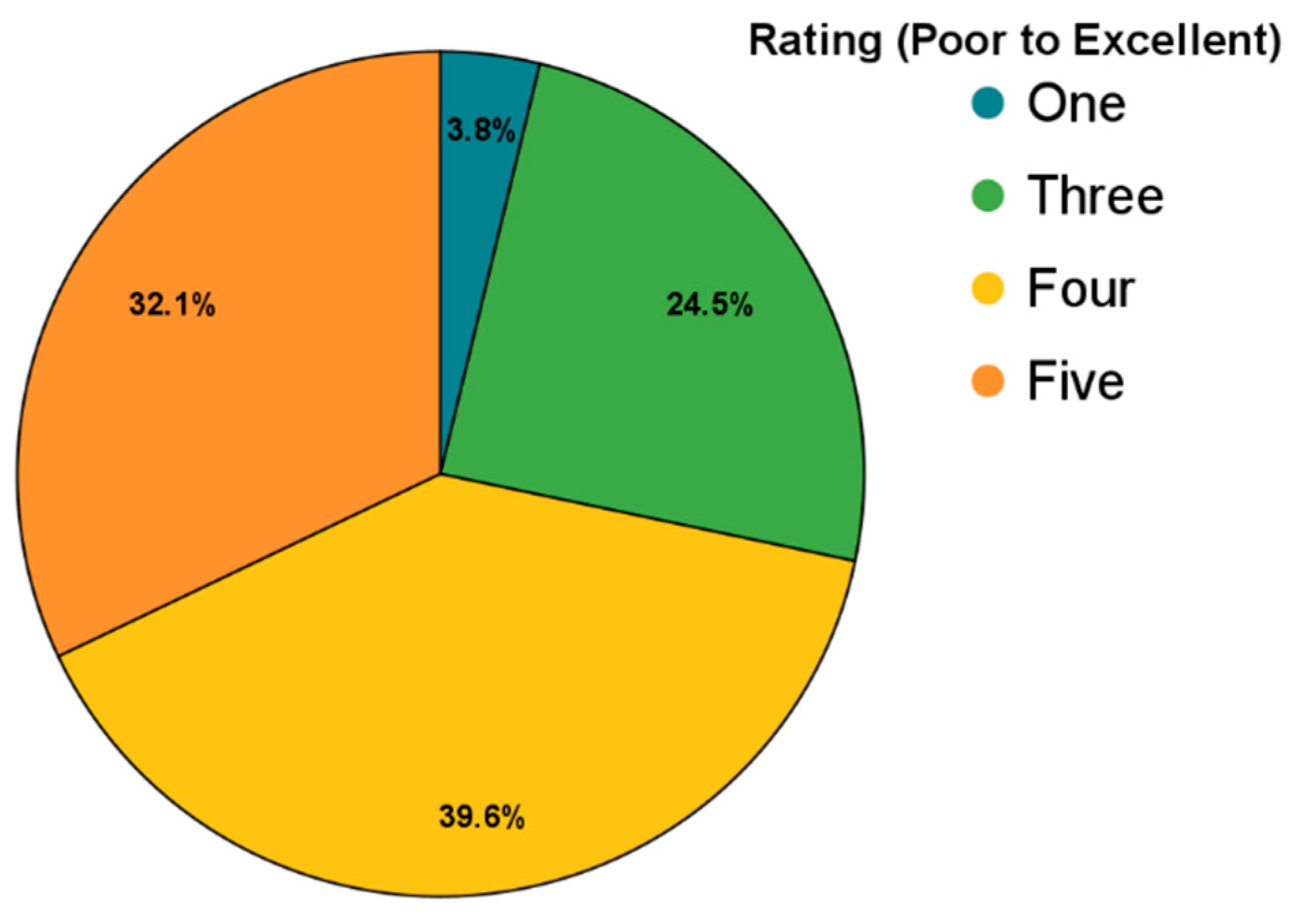
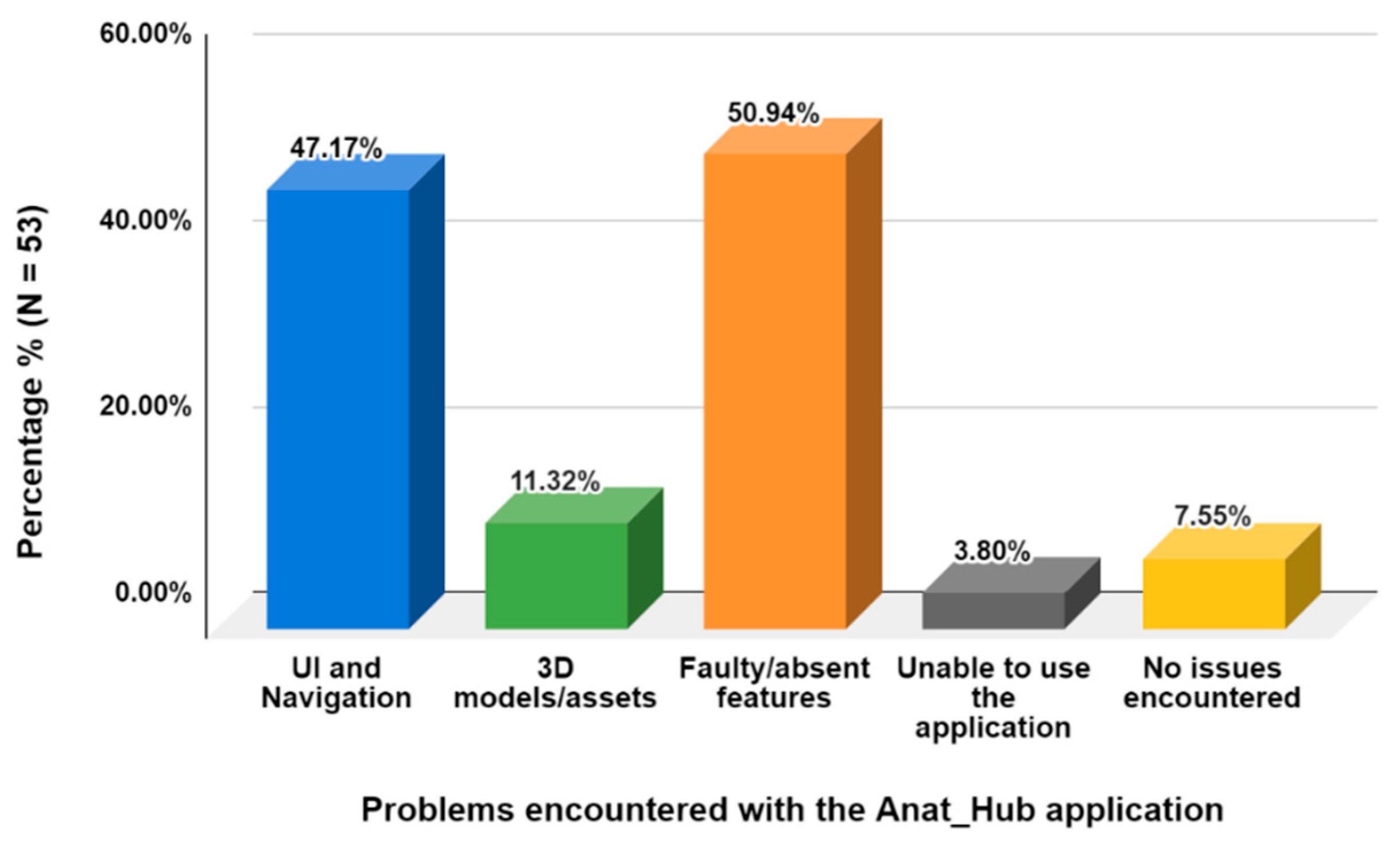
The survey further revealed that all of the volunteers owned a mobile device using either the Android (83%) or iOS (17%) operating system. It is worth noting that although Anat_Hub was specifically designed for Android users, two iOS users were able to provide feedback, implying that they were somehow able to use this application. For future research it would be beneficial to make the application available for all mobile operating systems. Very few volunteers have used AR applications prior to this study (13.2%), and all, except one volunteer, were able to use the Anat_Hub application. When rating Anat_Hub on a scale of 1 to 5, the majority of volunteers scored the application a 4 or 5 (Figure 15). Problems encountered with the application included mainly faulty or missing features (50.94%), UI and navigation (47.17%), and 3D assets (11.32%) (Figure 16). The problems encountered could possibly be ascribed to (but not limited to) the type of mobile device used, and thus devices that did not meet the deployment device specifications (Android API level 26 to 30 with a mobile screen aspect ratio of 16:9). Nevertheless, these problems have been noted for consideration to improve the application. A positive finding was that about two-thirds of the volunteers had a satisfactory initial user experience with the application.
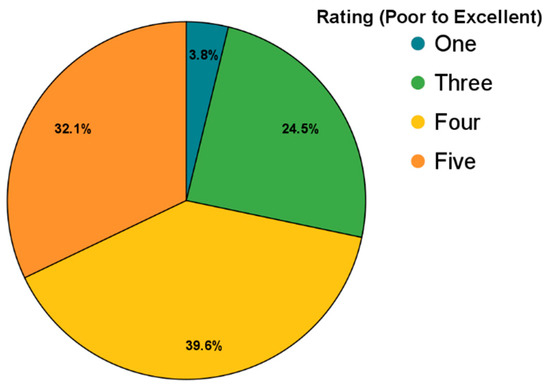
Figure 15.
Rating of the Anat_Hub mobile application on a scale of 1 to 5 (poor to excellent).
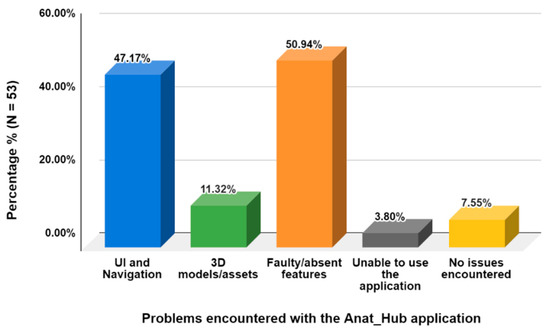
Figure 16.
Problems encountered when using the Anat_Hub mobile application.
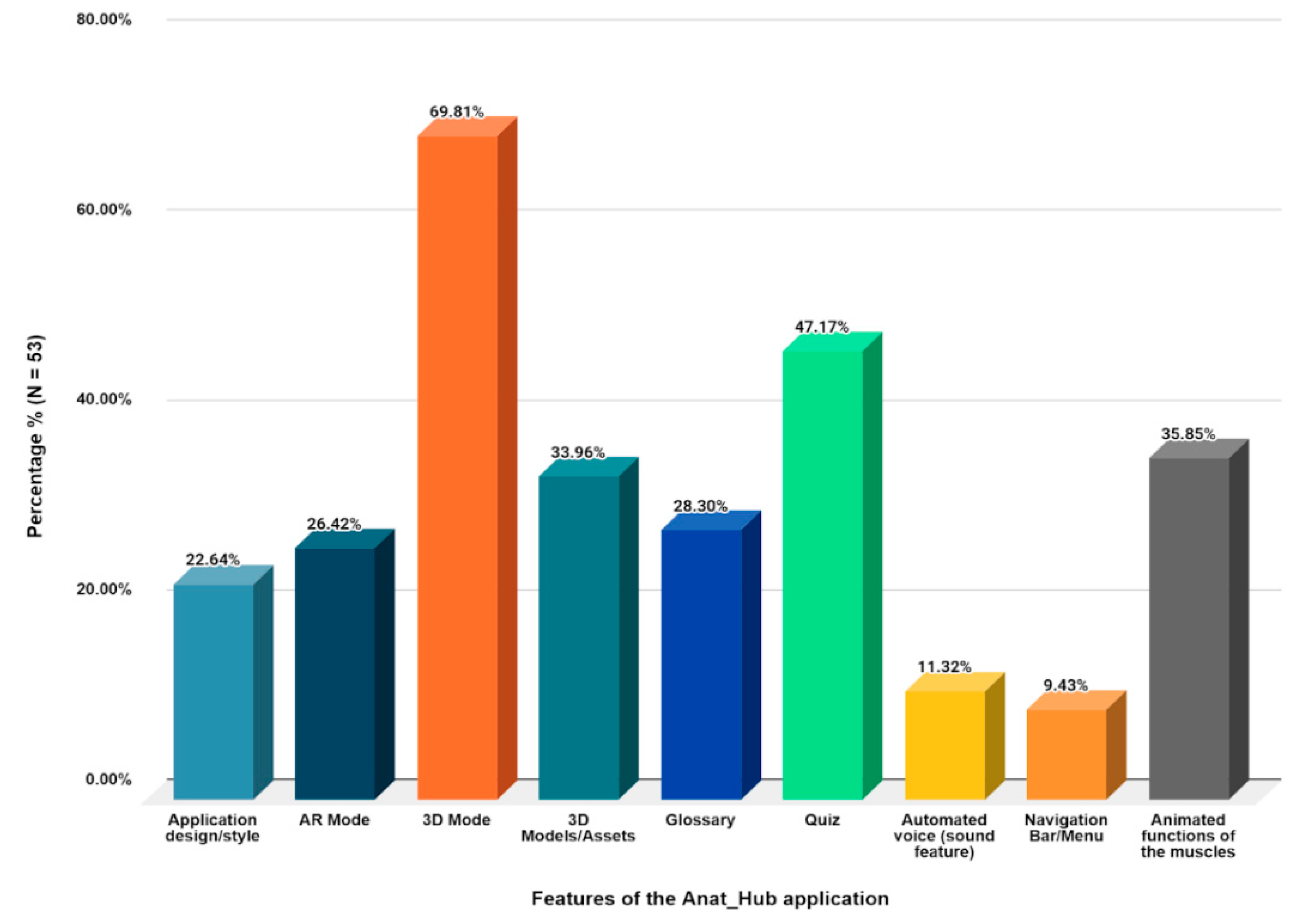
The most-liked feature of the application was the 3D mode (69.8%), while the least-liked were the navigation bar (9.43%) as well as the automated voice (sound feature) (11.23%) (Figure 17). The “robotic nature” of the sound feature is possibly the reason for this response by the volunteers as it could be considered unpleasant to the ear for some students, due to varying accent preferences. This could be rectified in an updated version of the app by incorporating varying accent and language features, where a user could make a choice. Furthermore, we noted that students had difficulty with the AR mode; as previously mentioned, this could be due to the type of mobile device and the deployment device specifications (Android API level 26 to 30) not being met. Another reason could be the inability of the mobile device camera functionality to perform, which would naturally hinder their experience. However, this survey did not ask participants to provide an explanation for their choice.
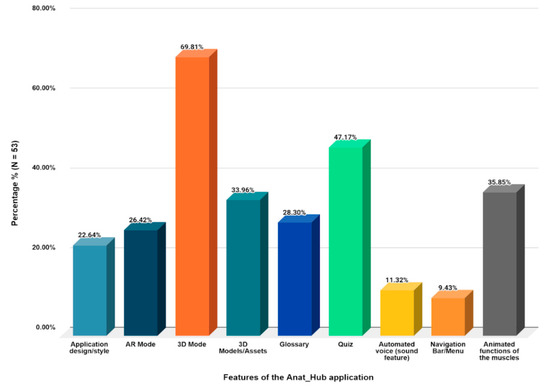
Figure 17.
The most-liked features of the Anat_Hub mobile application.
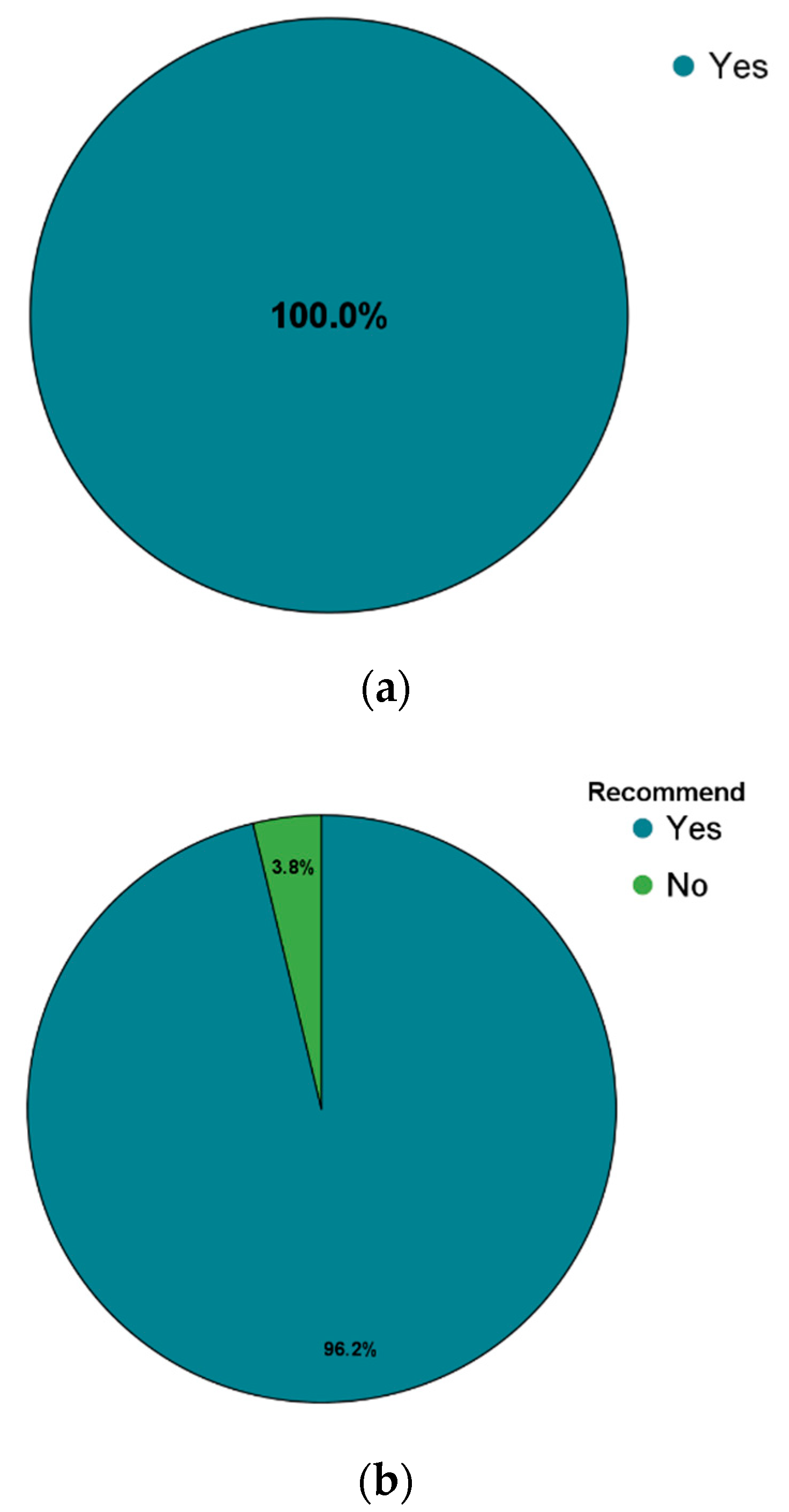
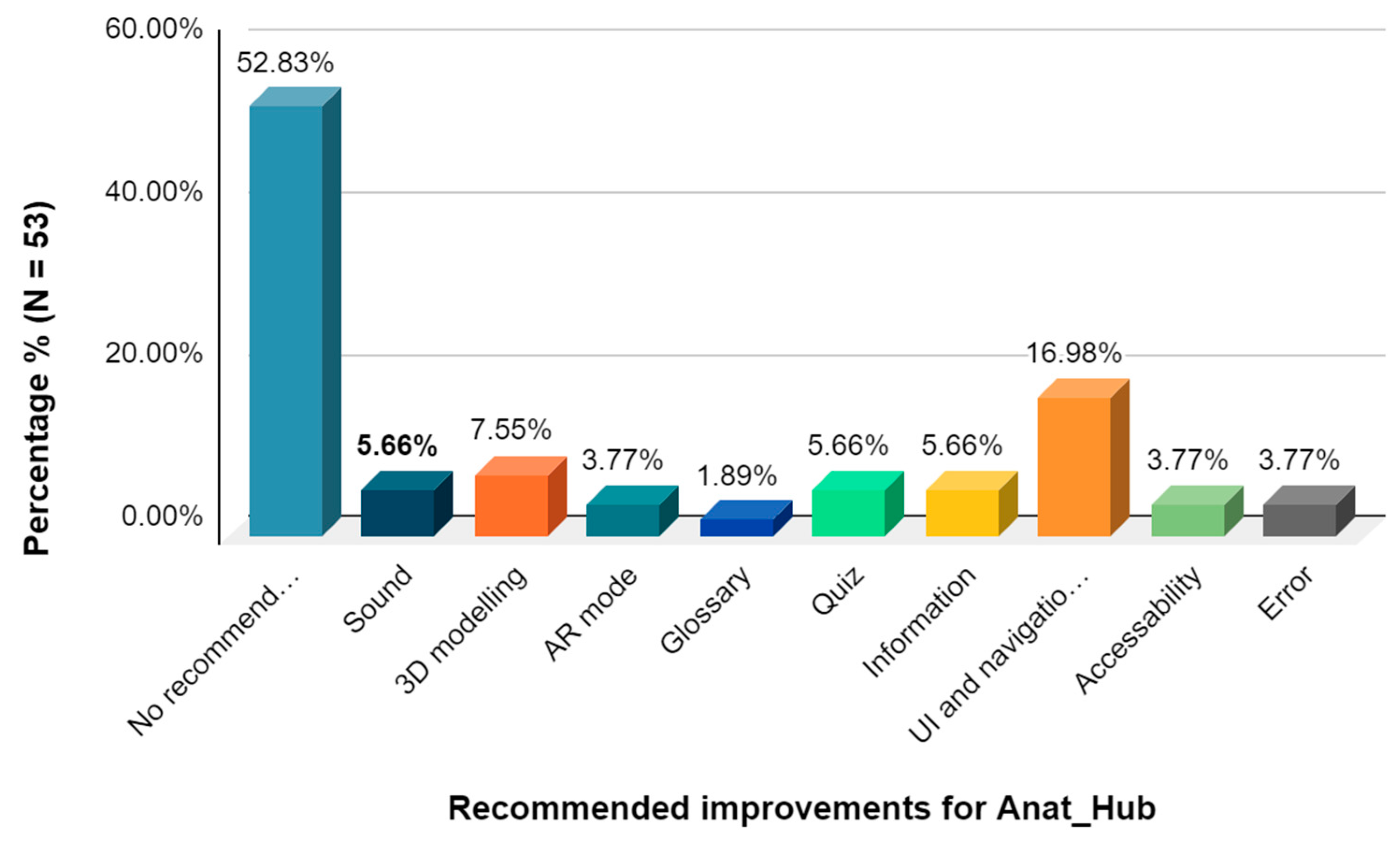
Overall, the application was well received by respondents and all indicated their willingness to make use of the Anat_Hub application to study the musculoskeletal system, while 96.2% said they will recommend the use of this application to others (Figure 18a,b). Finally, participants were asked to provide general recommendations to change or improve features within the Anat_Hub application for future updates and data analyses (Figure 19), and the majority of volunteers did not have any recommendations. This may indicate that the majority of the respondents were satisfied with the application, however, participants were not specifically asked to indicate their level of satisfaction. Therefore, subsequent studies on the improved versions of the app will include a variety of questionnaire items that specifically address this uncertainty as it is recognised that there is always room for improvement, as seen in Figure 19.
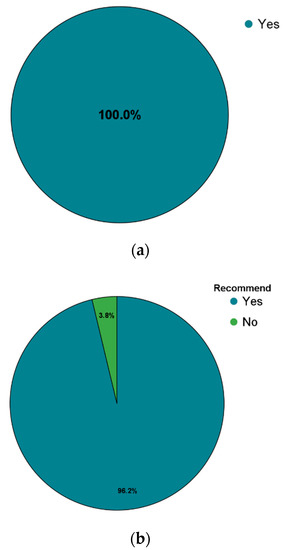
Figure 18.
(a) Responses related to the willingness to make use of the Anat_Hub mobile application for study purposes; and (b) willingness to recommend the Anat_Hub mobile application to others.
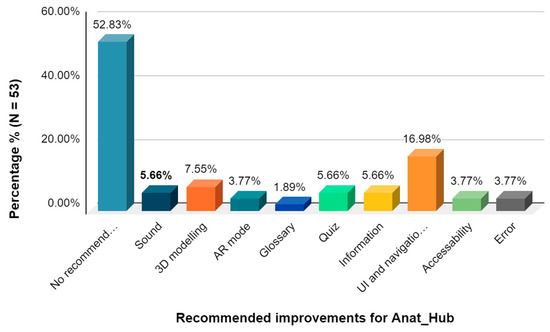
Figure 19.
General recommendations for improving the Anat_Hub mobile application.
The main focus of this rudimentary survey was to determine initial user experience, regarding how the application can be improved, and whether or not students are willing to use and recommend the Anat_Hub application. While retention may not have been explicitly mentioned in the survey, it is believed that this learning technology could promote retention in the learning space in addition to learner engagement. This is further highlighted by the problems faced by students when learning anatomy and how this application could address them, which is supported by the students’ readiness to accept the proposed AR (Anat_Hub) mobile application as a study tool. Future research pertaining to this application, using validated questionnaires and collecting data on engagement, is underway. Currently, research on preferred learning styles and strategies in anatomy education among South African students remains understudied or outdated, and further investigation into this topic may accentuate the need to implement immersive technology (blended learning) as a learning tool.
5. Summary and Conclusions
The teaching of anatomical structures has been impeded by various challenges and limitations, such as high cost of cadavers and limited qualified instructors, to mention a few. On the other hand, the advances in instructional technologies have provided various opportunities for creating innovative learning environments and new pedagogies in delivering educational resources. Specifically, there is evidence that immersive blended learning creates affordances for asynchronous online technology, improved learner engagement and meaningful learning spaces within blended anatomy courses.
While there is increased interest in using AR as learning tools, the amount of available primary research studies on their integration into educational settings, particularly the musculoskeletal system, is still relatively insignificant due to the novelty of this technology. This research developed an immersive anatomy AR application called Anat_Hub (Anatomy Hub), which was developed at a selected tertiary institution in Cape Town, South Africa, to assist in teaching and learning the names, attachments, actions, and innervation of the human musculoskeletal system. The hub displays a range of important features as a learning tool, particularly for medical bioscience undergraduate students, to simplify complex theoretical content in anatomy and promote self-regulated learning. The application was tested by undergraduate health sciences students, who were mostly using the technology for the first time, and on a range of mobile device specifications. The feedback obtained confirms its viability for improved learner engagement and quality anatomy education, while specifying areas for improvement and future research.
It can be concluded that the development of the application was successful and achieved the main aim and objectives. To reiterate, the results of this pilot study suggest that the Anat_Hub AR mobile application may be a valid learning tool that can create affordance for asynchronous learning. The positive indication by volunteers to use and recommend the application further validates its potential. It is also recommended that further improvements to the application are carried out and validated evaluation questionnaires with more detailed analysis are used. The idea offered in this research is one of its kind in Africa and can extend beyond the anatomy education domain. Notably, the review of the literature suggests that more research needs to be done in Africa in order to fully exploit the potential of this technology. Future studies can explore mixed reality for educational purposes, which combines the advantages of both augmented and virtual reality to further accelerate learner retention in anatomy education.
Author Contributions
Conceptualization, R.C.M.K., O.E.I. and O.E.; methodology, O.E.I., D.L.d.L.S., R.C.M.K. and O.E.; validation, R.C.M.K., O.E., O.E.I. and M.S.; visualization and software—shoulder and arm, A.B., T.G. and B.A.; visualization and software—leg and foot, K.J.F., C.C.C. and N.M.; visualization and software—forearm and hand, N.Y., A.L. and L.D.; visualization and software—hip and thigh, K.A.F., L.M. and S.G.; investigation, O.E.I., A.B., K.A.F. and R.C.M.K.; writing—original draft preparation, O.E.I., A.B., K.A.F. and R.C.M.K.; writing—review and editing, K.A.F., A.B., O.E.I., R.C.M.K. and O.E.; supervision, O.E.I., R.C.M.K., O.E., D.L.d.L.S. and M.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
The authors gratefully appreciate resources made available by the University of the Western Cape.
Conflicts of Interest
The authors declare no conflict of interest.
References
- South African Government. National Development Plan 2030. Available online: https://www.gov.za/issues/national-development-plan-2030 (accessed on 20 January 2022).
- Sattar, M.U.; Palaniappan, S.; Lokman, A.; Hassan, A.; Shah, N.; Riaz, Z. Effects of virtual reality training on medical students’ learning motivation and competency. Pak. J. Med. Sci. 2019, 35, 852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopes, I.D.S.L.; Teixeira, B.D.A.C.B.; Cortez, P.O.B.C.; da Silva, G.R.; de Sousa Neto, A.I.; de Sousa Leal, N.M. Use of human cadavers in teaching of human anatomy in Brazilian medical faculties. Acta Sci. Biol. Sci. 2017, 39, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Moro, C.; Štromberga, Z.; Raikos, A.; Stirling, A. The effectiveness of virtual and augmented reality in health sciences and medical anatomy. Anat. Sci. Educ. 2017, 10, 549–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalil, M.K.; Abdel Meguid, E.M.; Elkhider, I.A. Teaching of anatomical sciences: A blended learning approach. Clin. Anat. 2018, 31, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Green, R.A.; Whitburn, L.Y. Impact of introduction of blended learning in gross anatomy. Anat. Sci. Educ. 2016, 9, 422–430. [Google Scholar] [CrossRef] [PubMed]
- Johnson, E.O.; Charchanti, A.V.; Troupis, T.G. Modernization of an anatomy class: From conceptualization to implementation. A case for integrated multimodal–multidisciplinary teaching. Anat. Sci. Educ. 2012, 5, 354–366. [Google Scholar] [CrossRef]
- Miles, C.A.; Lee, A.C.; Foggett, K.A.; Nair, B.K. Reinventing medical teaching and learning for the 21st century: Blended and flipped strategies. Arch. Med. Health Sci. 2017, 5, 97. [Google Scholar] [CrossRef]
- Ma, M.; Fallavollita, P.; Seelbach, I.; Von Der Heide, A.M.; Euler, E.; Waschke, J.; Navab, N. Personalized augmented reality for anatomy education. Clin. Anat. 2016, 29, 446–453. [Google Scholar] [CrossRef]
- Khan, T.; Johnstone, K.; Ophoff, J. The impact of an augmented reality application on learning motivation of students. Adv. Hum.-Comput. Interact. 2019, 2019, 7208494. [Google Scholar] [CrossRef] [Green Version]
- Ferrer-Torregrosa, J.; Torralba, J.; Jimenez, M.A.; García, S.; Barcia, J.M. ARBOOK: Development and assessment of a tool based on augmented reality for anatomy. J. Sci. Educ. Technol. 2015, 24, 119–124. [Google Scholar] [CrossRef]
- Küçük, S.; Kapakin, S.; Göktaş, Y. Learning anatomy via mobile augmented reality: Effects on achievement and cognitive load. Anat. Sci. Educ. 2016, 9, 411–421. [Google Scholar] [CrossRef] [PubMed]
- Jamali, S.S.; Shiratuddin, M.F.; Wong, K.W.; Oskam, C.L. Utilising mobile-augmented reality for learning human anatomy. Procedia-Soc. Behav. Sci. 2015, 197, 659–668. [Google Scholar] [CrossRef] [Green Version]
- Liarokapis, F.; Anderson, E.F. Using augmented reality as a medium to assist teaching in higher education. In Proceedings of the Eurographics Conference: Eurographics 2010—Education Papers, Norrköping, Sweden, 3–7 May 2010. [Google Scholar] [CrossRef]
- Kamphuis, C.; Barsom, E.; Schijven, M.; Christoph, N. Augmented reality in medical education? Perspect. Med. Educ. 2014, 3, 300–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moro, C.; Birt, J.; Stromberga, Z.; Phelps, C.; Clark, J.; Glasziou, P.; Scott, A.M. Virtual and augmented reality enhancements to medical and science student physiology and anatomy test performance: A systematic review and meta-analysis. Anat. Sci. Educ. 2021, 14, 368–376. [Google Scholar] [CrossRef]
- Ocak, M.A.; Topal, A.D. Blended learning in anatomy education: A study investigating medical students’ perceptions. Eurasia J. Math. Sci. Technol. Educ. 2015, 11, 647–683. [Google Scholar] [CrossRef]
- Ngan, O.M.; Tang, T.L.; Chan, A.K.; Chen, D.M.; Tang, M.K. Blended learning in anatomy teaching for non-medical students. Health Prof. Educ. 2018, 4, 149–158. [Google Scholar] [CrossRef]
- Nobles, M.S. Innovative Instruction: Learning in Blended Human Anatomy Education. Ph.D. Thesis, Pepperdine University, Malibu, CA, USA, 2019. Available online: https://digitalcommons.pepperdine.edu/etd/1040 (accessed on 1 February 2022).
- Hutahaean, H.D.; Rahman, S.M.A.; Mendoza, M.D. Development of interactive learning media in computer network using augmented reality technology. J. Phys. Conf. Ser. 2022, 2193, 012072. [Google Scholar] [CrossRef]
- Azuma, R.T. A survey of augmented reality. Presence-Teleoperators Virtual Environ. 1997, 6, 355–385. [Google Scholar] [CrossRef]
- Yuen, S.; Yaoyuneyong, G.; Johnson, E. Augmented reality: An overview and five directions for AR in education. J. Educ. Technol. Dev. Exch. (JETDE) 2011, 4, 119–140. Available online: https://aquila.usm.edu/jetde/vol4/iss1/11/ (accessed on 2 September 2020). [CrossRef]
- Klopfer, E. Augmented Learning: Research and Design of Mobile Educational Games; MIT Press: Cambridge, MA, USA, 2008. [Google Scholar]
- Dunleavy, M.; Dede, C.; Mitchell, R. Affordances and limitations of immersive participatory augmented reality simulations for teaching and learning. J. Sci. Educ. Technol. 2009, 18, 7–22. [Google Scholar] [CrossRef]
- Suárez-Escudero, J.C.; Posada-Jurado, M.C.; Bedoya-Muñoz, L.J.; Urbina-Sánchez, A.J.; Ferreira-Morales, J.L.; Bohórquez-Gutiérrez, C.A. Teaching and learning anatomy. Pedagogical methods, history, the present and tendencies. Acta Med. Colomb. 2020, 45, 48–55. [Google Scholar]
- Kurniawan, M.H.; Suharjito Suharjito, D.; Witjaksono, G. Human anatomy learning systems using augmented reality on mobile application. Procedia Comput. Sci. 2018, 135, 80–88. [Google Scholar] [CrossRef]
- Patil, S.; Rao, A.; Pardeshi, N.; Gavhane, M.; Waghole, D. Augmented Reality in Anatomy; IJERT: Gandhinagar, India, 2021. [Google Scholar]
- Cercenelli, L.; De Stefano, A.; Billi, A.M.; Ruggeri, A.; Marcelli, E.; Marchetti, C.; Manzoli, L.; Ratti, S.; Badiali, G. AEducaAR, anatomical education in augmented reality: A pilot experience of an innovative educational tool combining AR technology and 3D printing. Int. J. Environ. Res. Public Health 2022, 19, 1024. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Lee, S.; Chang, H.; Liang, J. Current status, opportunities and challenges of augmented reality in education. Comput. Educ. 2013, 62, 41–49. Available online: https://www.sciencedirect.com/science/article/pii/S0360131512002527?casa_token=LCwtXVtgLdIAA AAA:Sg6AMP3F1r6hehOi5iNADTGLO3Nc_ROc97hM2HBe7lSKjH6ofZOsHLLuESOJO_1Nni2wb5 z44g (accessed on 10 April 2022). [CrossRef]
- Iwanaga, J.; Loukas, M.; Dumont, A.; Tubbs, S. A review of anatomy education during and after the COVID-19 pandemic: Revisiting traditional and modern methods to achieve future innovation. Clin. Anat. 2021, 34, 108–114. Available online: https://onlinelibrary.wiley.com/doi/epdf/10.1002/ca.23655 (accessed on 6 September 2020). [CrossRef]
- Estai, M.; Bunt, S. Best teaching practices in anatomy education: A critical review. Ann. Anat.-Anat. Anz. 2016, 208, 151–157. Available online: https://www.sciencedirect.com/science/article/pii/S0940960216300322?casa_token=5I6lmNIXvYcAA AAA:2KLiEhVWJKSNBTAwlN81F4taT7Wt6ol2_XHDXpOYKbJBGnp4MFmYqGLJJJBmYXSKR2L5trfoA (accessed on 10 April 2022). [CrossRef]
- Keller, J.M. What is motivational design? In Motivational Design for Learning and Performance; Springer: Boston, MA, USA, 2010. [Google Scholar] [CrossRef]
- Christopoulos, A.; Pellas, N.; Kurczaba, J.; Macredie, R. The effects of augmented reality-supported instruction in tertiary-level medical education. Br. J. Educ. Technol. 2022, 53, 307–325. [Google Scholar] [CrossRef]
- Kramer, B.; Pather, N.; Ihunwo, A.O. Anatomy: Spotlight on Africa. Anat. Sci. Educ. 2008, 1, 111–118. [Google Scholar] [CrossRef]
- Atuahene, F. Re-thinking the missing mission of higher education: An anatomy of the research challenge of African universities. J. Asian Afr. Stud. 2011, 46, 321–341. [Google Scholar] [CrossRef]
- Holmes, G. Augmented Reality Assisted Orthopaedic Surgery. Master’s Thesis, Stellenbosch University, Cape Town, South Africa, 2018. [Google Scholar]
- Terrell, M. Anatomy of learning: Instructional design principles for the anatomical sciences. Anat. Rec. B New Anat. 2006, 289, 252–260. [Google Scholar] [CrossRef]
- Mitchell, B.S. Learning styles in anatomy teaching and learning. In Teaching Anatomy; Lap, K.C., Wojciech, P., Eds.; Springer: Cham, Switzerland, 2015; pp. 23–30. [Google Scholar]
- Fowler, M.; Highsmith, J. The Agile manifesto. Softw. Dev. Mag. 2001, 9, 29–30. [Google Scholar]
- Ehn, P. Work-Oriented Design of Computer Artifacts; Arbetslivscentrum: Stockholm, Sweden, 1988; Available online: https://www.diva-portal.org/smash/get/diva2:580037/FULLTEXT02.pdf (accessed on 10 April 2022).
- Rigby, D.K.; Sutherland, J.; Takeuchi, H. Embracing Agile. Harv. Bus. Rev. 2016, 94, 40–50. [Google Scholar]
- Friess, E. “Filling to capacity”: An exploratory study of project management language in agile scrum teams. Tech. Commun. 2018, 65, 169–180. [Google Scholar]
- Schuh, P. Integrating Agile Development in the Real World; Charles River Media, Inc.: Newton, MA, USA, 2004; ISBN 10-1584503645. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).