
Tilted Implants and Sinus Floor Elevation Techniques Compared in Posterior Edentulous Maxilla: A Retrospective Clinical Study over Four Years of Follow-Up


 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Surgical Procedures
Post-Surgical Protocol
2.3. Prosthetic Protocol
2.4. Follow-Up
- Implant survival rate. The implant survival rate was dependent on the number of implants lost during the follow-up period due to mobility associated with progressive marginal bone loss due to peri-implantitis. Implant loss was classified according to the period: if it occurred within 6 months of fixture placement, it was called early failure; after 6 months, it was called late failure. Early failure was usually intercepted at the reopening stage, when there was a lack of osseointegration of the implant. In the case of late failure, there were signs of peri-implantitis, implant mobility, radiolucent areas around fixtures, mucosal suppuration, and/or pain during the follow-up period.
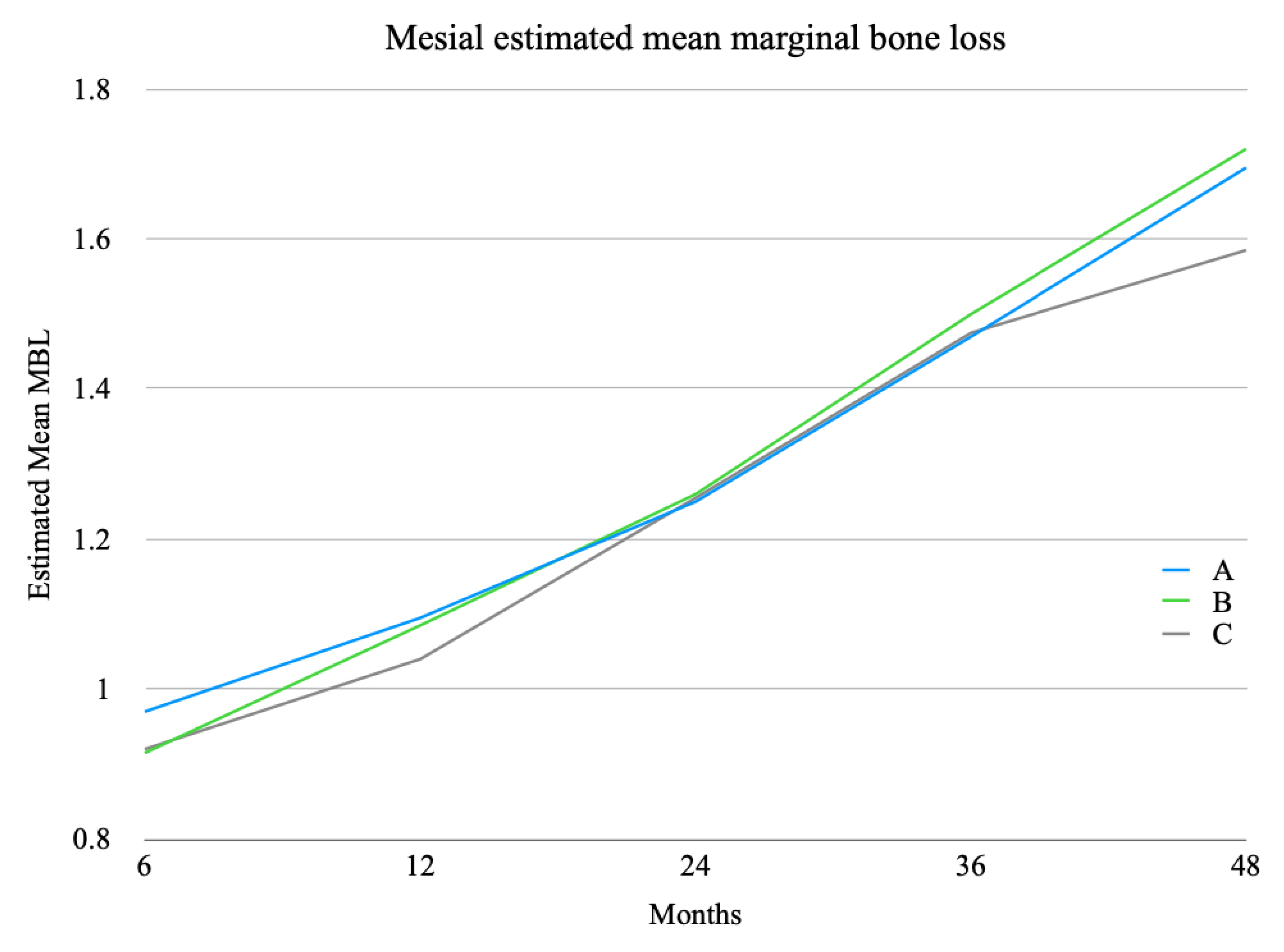
- Marginal bone loss (MBL). The MBL was evaluated via digital phosphor intra-oral radiography performed for each patient using the parallel cone technique at 6, 12, 24, 36, and 48 months. To assess marginal bone trends, measurements were performed only after image calibration. Digora 2.5 software (Soredex, Tuusula, Finland) was used as an analysis platform, making use of the specific measurement tool contained therein. As a first step, calibration (pixels/mm) of the instrument was performed, using the implant diameter of the survey site as the known unit. Next, any changes in the height of the peri-implant marginal bone in relation to the most coronal part of the implant and the point of contact between the implant and marginal ridge were measured. To evaluate bone resorption, a line passing over the shoulder of the implant was considered as a reference point for measurement from which a straight line was drawn parallel to the long axis of the implant to the most coronal point where the bone met the fixture both mesially and distally. The software automatically provided, in relation to the calibration, the distance between the two points measured in millimeters. To reduce human error, this measurement was performed by three operators, and the average of the three measurements was considered. To evaluate the marginal bone level, first the mesial and distal measurements were taken, then the averages of the mesial, of the distal, and between the two values of a single implant site (MBL, marginal bone level) were calculated, as reported in Section 3. Marginal bone levels detected were divided into two categories according to the implant position, whether mesial (Implant 1/I1) or distal (Implant 2/I2). The first group included only axial implants; the second group also included tilted fixtures, always placed distally and in association with a mesial axial implant (Implant 1/I1). The data thus obtained were then statistically investigated.
- Surgical complications. Surgical complications were divided according to the surgical procedure.
- Prosthetic complications. These included fracture of the provisional prothesis, unscrewing of temporary crowns and/or abutments (Group C), unscrewing of final crowns and/or abutments (Group C), and chipping.
2.5. Statistical Analysis
3. Results
- 1.
- Implant survival rate. In the lateral sinus floor elevation technique (Group A), no implants were lost in the first six months after surgery; two fixtures were lost in the following period. In the transcrestal approach (Group B), one implant was lost in the first six months after surgery, and only one was lost later. Only one tilted implant (Group C) was lost early; no implants were lost in the following period.
- 2.
- Marginal Bone Loss. Statistical analysis was also performed for marginal bone loss, evaluated 6 months after the surgical procedure, 12 months after the surgical procedure, and once a year subsequently. The values obtained were divided into two categories according to the fixture position (Table 5 and Table 6).
- 3.
- Surgical Complications. All recorded complications were related to the lateral sinus floor elevation technique (Group A) or transcrestal sinus floor elevation (Group B). In Group C, there were no intra-operative complications. Three membrane perforations were reported in Group A. The complication was resolved intra-operatively by further detaching the Schneider membrane from the inferior-medial region to reposition the hole under the bone wall. This avoided leakage of the graft material and possible subsequent infection. In the same group, no other complications were reported. In Group B, the only problem encountered was paroxysmal benign positional vertigo (PPBV), associated with the percussive action induced by the surgical mallet. After about one month, the complication resolved itself in all four cases where it was found.
- 4.
- Prosthetic Complications. No prosthetic complications were reported during the follow-up period.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gerken, U.; Esser, F.; Möhlhenrich, S.C.; Bartella, A.K.; Hölzle, F.; Fischer, H.; Raith, S.; Steiner, T. Objective computerised assessment of residual ridge resorption in the human maxilla and maxillary sinus pneumatisation. Clin. Oral Investig. 2020, 24, 3223–3235. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.C.; Kim, S.; Kim, D.H.; Herr, Y.; Chung, J.H.; Shin, S.I. Factors affecting maxillary sinus pneumatization following posterior maxillary tooth extraction. J. Periodontal. Implant Sci. 2021, 51, 285–295. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.W.; Finkelman, M.; Papaspirisdakos, P.; César-Neto, J.B.; Weber, H.P.; de Souza, A.B. Comparative analysis of dimensional alterations following extraction of maxillary molars using three-dimensional images’ superimposition: A CBCT study. Odontology 2021, 109, 514–523. [Google Scholar] [CrossRef] [PubMed]
- Vinci, R.; Teté, G.; Lucchetti, F.R.; Capparé, P.; Gherlone, E.F. Implant survival rate in calvarial bone grafts: A retrospective clinical study with 10 year follow-up. Clin. Implant Dent. Relat. Res. 2019, 21, 662–668. [Google Scholar] [CrossRef] [PubMed]
- Ha, J.; Son, J.H.; Sung, I.Y.; Cho, Y.C.; Choi, J.H. Clinical outcome of implants placed in grafted maxillary sinus via lateral approach: A 10-year follow-up study. J. Dent. Sci. 2020, 15, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Aloy-Prósper, A.; Carramolino-Cuéllar, E.; Peñarrocha-Oltra, D.; Soto-Peñaloza, D.; Peñarrocha-Diago, M. Intraoral onlay block bone grafts versus cortical tenting technique on alveolar ridge augmentations: A systematic review. Med. Oral Patol. Oral Cir. Bucal. 2022, 27, e181–e190. [Google Scholar] [CrossRef]
- Leung, M.; Alghamdi, R.; Guallart, I.F.; Bergamini, M.; Yu, P.Y.; Froum, S.J.; Cho, S.C. Patient-Related Risk Factors for Maxillary Sinus Augmentation Procedures: A Systematic Literature Review. Int. J. Periodont. Restor. Dent. 2021, 41, e121–e128. [Google Scholar] [CrossRef]
- Carosi, P.; Lorenzi, C.; Lio, F.; Laureti, M.; Ferrigno, N.; Arcuri, C. Short implants (≤6 mm) as an alternative treatment option to maxillary sinus lift. Int. J. Oral Maxillofac. Surg. 2021, 50, 1502–1510. [Google Scholar] [CrossRef]
- Asawa, N.; Bulbule, N.; Kakade, D.; Shah, R. Angulated implants: An alternative to bone augmentation and sinus lift procedure: Systematic review. J. Clin. Diagn. Res. 2015, 9, ZE10-3. [Google Scholar] [CrossRef]
- Desai, S.R.; Singh, R.; Karthikeyan, I. 2D FEA of evaluation of micromovements and stresses at bone-implant interface in immediately loaded tapered implants in the posterior maxilla. J. Indian Soc. Periodontol. 2013, 17, 637–643. [Google Scholar] [CrossRef]
- Sumra, N.; Desai, S.; Kulshrestha, R.; Mishra, K.; Singh, R.V.; Gaonkar, P. Analysis of micromovements and peri-implant stresses and strains around ultra-short implants—A three-dimensional finite-element method study. J. Indian Soc. Periodontol. 2021, 25, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Gallucci, G.O.; Avrampou, M.; Taylor, J.C.; Elpers, J.; Thalji, G.; Cooper, L.F. Maxillary Implant-Supported Fixed Prosthesis: A Survey of Reviews and Key Variables for Treatment Planning. Int. J. Oral Maxillofac. Implants 2016, 31, S192–S197. [Google Scholar] [CrossRef] [PubMed]
- Hong, D.G.K.; Oh, J.H. Recent advances in dental implants. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messias, A.; Nicolau, P.; Guerra, F. Different Interventions for Rehabilitation of the Edentulous Maxilla with Implant-Supported Prostheses: An Overview of Systematic Reviews. Int. J. Prosthodont. 2021, 34, S63–S84. [Google Scholar] [CrossRef] [PubMed]
- Khehra, A.; Levin, L. Maxillary sinus augmentation procedures: A narrative clinical review. Quintessence Int. 2020, 51, 578–584. [Google Scholar] [CrossRef]
- Lundgren, S.; Cricchio, G.; Hallman, M.; Jungner, M.; Rasmusson, L.; Sennerby, L. Sinus floor elevation procedures to enable implant placement and integration: Techniques, biological aspects and clinical outcomes. Periodontol. 2000 2017, 73, 103–120. [Google Scholar] [CrossRef]
- Agliardi, E.L.; Tetè, S.; Romeo, D.; Malchiodi, L.; Gherlone, E. Immediate function of partial fixed rehabilitation with axial and tilted implants having intrasinus insertion. J. Craniofac. Surg. 2014, 25, 851–855. [Google Scholar] [CrossRef]
- De Vico, G.; Bonino, M.; Spinelli, D.; Schiavetti, R.; Sannino, G.; Pozzi, A.; Ottria, L. Rationale for tilted implants: FEA considerations and clinical reports. Oral Implantol. 2011, 4, 23–33. [Google Scholar]
- Hsu, Y.T.; Rosen, P.S.; Choksi, K.; Shih, M.C.; Ninneman, S.; Lee, C.T. Complications of sinus floor elevation procedure and management strategies: A systematic review. Clin. Implant. Dent. Relat. Res. 2022. [Google Scholar] [CrossRef]
- Summers, R.B. A new concept in maxillary implant surgery: The osteotome technique. Compendium 1994, 15, 154–156, 158; discussion 162. [Google Scholar]
- Summers, R.B. The osteotome technique: Part 3—Less invasive methods of elevating the sinus floor. Compendium 1994, 15, 698, 700, 702–704; discussion 710. [Google Scholar] [PubMed]
- Andrés-García, R.; Ríos-Santos, J.; Herrero-Climent, M.; Bullón, P.; Fernández-Farhall, J.; Gómez-Menchero, A.; Fernández-Palacín, A.; Ríos-Carrasco, B. Sinus Floor Elevation via an Osteotome Technique without Biomaterials. Int. J. Environ. Res. Public Health 2021, 18, 1103. [Google Scholar] [CrossRef] [PubMed]
- Ulmer, F.C., Jr. Kennedy-Applegate classification of partially edentulous dental arches. NADL J. 1983, 30, 37–40. [Google Scholar] [PubMed]
- Sakkas, A.; Schramm, A.; Winter, K.; Wilde, F. Risk factors for post-operative complications after procedures for autologous bone augmentation from different donor sites. J. Craniomaxillofac. Surg. 2018, 46, 312–322. [Google Scholar] [CrossRef]
- Menini, M.; Signori, A.; Tealdo, T.; Bevilacqua, M.; Pera, F.; Ravera, G.; Pera, P. Tilted implants in the immediate loading rehabilitation of the maxilla: A systematic review. J. Dent. Res. 2012, 91, 821–827. [Google Scholar] [CrossRef]
- Pathan, M.R.; Mehta, S.P.; Sutariya, P.V.; Upadhyay, H.H.; Patel, S.R.; Kantharia, N.D.G. Clinical success between tilted and axial implants in edentulous maxilla: A systematic review and meta-analysis. J. Indian Prosthodont. Soc. 2021, 21, 217–228. [Google Scholar] [CrossRef]
- Polizzi, E.; D’Orto, B.; Tomasi, S.; Tetè, G. A micromorphological/microbiological pilot study assessing three methods for the maintenance of the implant patient. Clin. Exp. Dent. Res. 2021, 7, 156–162. [Google Scholar] [CrossRef]
- Cattoni, F.; Tetè, G.; D’orto, B.; Bergamaschi, A.; Polizzi, E.; Gastaldi, G. Comparison of hygiene levels in metal-ceramic and stratified zirconia in prosthetic rehabilitation on teeth and implants: A retrospective clinical study of a three-year follow-up. J. Biol. Regul. Homeost. Agents 2021, 35, 41–49. [Google Scholar] [CrossRef]
- Canullo, L.; Patacchia, O.; Sisti, A.; Heinemann, F. Implant restoration 3 months after one stage sinus lift surgery in severely resorbed maxillae: 2-year results of a multicenter prospective clinical study. Clin. Implant Dent. Relat. Res. 2012, 14, 412–420. [Google Scholar] [CrossRef]
- Schmitt, C.; Karasholi, T.; Lutz, R.; Wiltfang, J.; Neukam, F.-W.; Schlegel, K.A. Long-term changes in graft height after maxillary sinus augmentation, onlay bone grafting, and combination of both techniques: A long-term retrospective cohort study. Clin. Oral Implants Res. 2014, 25, e38–e46. [Google Scholar] [CrossRef]
- Beretta, M.; Poli, P.; Grossi, G.B.; Pieroni, S.; Maiorana, C. Long-term survival rate of implants placed in conjunction with 246 sinus floor elevation procedures: Results of a 15-year retrospective study. J. Dent. 2015, 43, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Al-Moraissi, E.; Alkhutari, A.; Abotaleb, B.; Altairi, N.; Del Fabbro, M. Do osteoconductive bone substitutes result in similar bone regeneration for maxillary sinus augmentation when compared to osteogenic and osteoinductive bone grafts? A systematic review and frequentist network meta-analysis. Int. J. Oral Maxillofac. Surg. 2020, 49, 107–120. [Google Scholar] [CrossRef] [PubMed]
- Stumbras, A.; Krukis, M.M.; Januzis, G.; Juodzbalys, G. Regenerative bone potential after sinus floor elevation using various bone graft materials: A systematic review. Quintessence Int. 2019, 50, 548–558. [Google Scholar] [CrossRef]
- Lie, S.; Claessen, R.; Leung, C.; Merten, H.-A.; Kessler, P. Non-grafted versus grafted sinus lift procedures for implantation in the atrophic maxilla: A systematic review and meta-analysis of randomized controlled trials. Int. J. Oral Maxillofac. Surg. 2022, 51, 122–132. [Google Scholar] [CrossRef] [PubMed]
- Bruschi, G.B.; Crespi, R.; Cappare’, P.; Gherlone, E. Transcrestal sinus floor elevation: A retrospective study of 46 patients up to 16 years. Clin. Implant Dent. Relat. Res. 2012, 14, 759–767. [Google Scholar] [CrossRef] [PubMed]
- Qian, S.; Mo, J.; Si, M.-S.; Qiao, S.; Shi, J.-Y.; Lai, H. Long-term outcomes of osteotome sinus floor elevation with or without bone grafting: The 10-year results of a randomized controlled trial. J. Clin. Periodontol. 2020, 47, 1016–1025. [Google Scholar] [CrossRef]
- Aparicio, C.; Perales, P.; Rangert, B. Tilted implants as an alternative to maxillary sinus grafting: A clinical, radiologic, and periotest study. Clin. Implant Dent. Relat. Res. 2001, 3, 39–49. [Google Scholar] [CrossRef]
- Fortin, T.; Isidori, M.; Bouchet, H. Placement of posterior maxillary implants in partially edentulous patients with severe bone deficiency using CAD/CAM guidance to avoid sinus grafting: A clinical report of procedure. Int. J. Oral Maxillofac. Implants 2009, 24, 96–102. [Google Scholar]
- Pozzi, A.; Sannino, G.; Barlattani, A. Minimally invasive treatment of the atrophic posterior maxilla: A proof-of-concept prospective study with a follow-up of between 36 and 54 months. J. Prosthet. Dent. 2012, 108, 286–297. [Google Scholar] [CrossRef]
- Antonoglou, G.; Stavropoulos, A.; Samara, M.; Ioannidis, A.; Benić, G.; Papageorgiou, S.; Sándor, G. Clinical Performance of Dental Implants Following Sinus Floor Augmentation: A Systematic Review and Meta-Analysis of Clinical Trials with at Least 3 Years of Follow-up. Int. J. Oral Maxillofac. Implants 2018, 33, e45–e65. [Google Scholar] [CrossRef] [Green Version]
- Călin, C.; Petre, A.; Drafta, S. Osteotome-mediated sinus floor elevation: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Implants 2014, 29, 558–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geminiani, A.; Tsigarida, A.; Chochlidakis, K.; Papaspyridakos, P.V.; Feng, C.; Ercoli, C. A meta-analysis of complications during sinus augmentation procedure. Quintessence Int. 2017, 48, 231–240. [Google Scholar] [CrossRef]
- Bacevic, M.; Compeyron, Y.; Lecloux, G.; Rompen, E.; Lambert, F. Intraoperative and postoperative outcomes of sinus floor elevation using the lateral window technique versus the hydrodynamic transalveolar approach: A preliminary randomized controlled trial. Clin. Oral Investig. 2021, 25, 5391–5401. [Google Scholar] [CrossRef] [PubMed]
- Molina, A.; Sanz-Sánchez, I.; Sanz-Martín, I.; Ortiz-Vigón, A.; Sanz, M. Complications in sinus lifting procedures: Classification and management. Periodontol. 2000 2022, 88, 103–115. [Google Scholar] [CrossRef]
- Küçükkurt, S.; Alpaslan, G.; Kurt, A. Biomechanical comparison of sinus floor elevation and alternative treatment methods for dental implant placement. Comput. Methods Biomech. Biomed. Engin. 2017, 20, 284–293. [Google Scholar] [CrossRef]
- Brinkmann, J.C.-B.; García-Gil, I.; Pedregal, P.; Peláez, J.; Prados-Frutos, J.; Suárez, M. Long-Term Clinical Behavior and Complications of Intentionally Tilted Dental Implants Compared with Straight Implants Supporting Fixed Restorations: A Systematic Review and Meta-Analysis. Biology 2021, 10, 509. [Google Scholar] [CrossRef]
- Cappare, P.; Ferrini, F.; Mariani, G.; Nagni, M.; Cattoni, F. Implant rehabilitation of edentulous jaws with predominantly monolithic zirconia compared to metal-acrylic prostheses: A 2-year retrospective clinical study. J. Biol. Regul. Homeost. Agents 2021, 35 (Suppl. S1), 99–112. [Google Scholar] [CrossRef]
- Yücesoy, T.; Göktaş, T. Evaluation of Sinus Pneumatization and Dental Implant Placement in Atrophic Maxillary Premolar and Molar Regions. Int. J. Oral Maxillofac. Implants 2022, 37, 407–415. [Google Scholar] [CrossRef]
- Dagassan-Berndt, D.C.; Clemens, W.; Zitzmann, N.U.; Schulze, R.K. Influence of Three-dimensional Imaging on Implant Treatment Planning: Implant Diameter and Length. J. Contemp. Dent. Pract. 2018, 19, 704–711. [Google Scholar] [CrossRef]
- Fortes, J.H.; de Oliveira-Santos, C.; Matsumoto, W.; da Motta, R.J.G.; Tirapelli, C. Influence of 2D vs 3D imaging and professional experience on dental implant treatment planning. Clin. Oral Investig. 2019, 23, 929–936. [Google Scholar] [CrossRef]
- Dagassan-Berndt, D.C.; Zitzmann, N.U.; Walter, C.; Schulze, R. Implant treatment planning regarding augmentation procedures: Panoramic radiographs vs. cone beam computed tomography images. Clin. Oral Implants Res. 2016, 27, 1010–1016. [Google Scholar] [CrossRef] [PubMed]
- Chmielewski, K.; Ryncarz, W.; Yüksel, O.; Goncalves, P.; Baek, K.-W.; Cok, S.; Dard, M. Image analysis of immediate full-arch prosthetic rehabilitations guided by a digital workflow: Assessment of the discrepancy between planning and execution. Int. J. Implant Dent. 2019, 5, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, D.; Sax, C.; Sancho-Puchades, M.; Hämmerle, C.H.; Jung, R.E. Accuracy of computer-assisted, template-guided implant placement compared with conventional implant placement by hand-An in vitro study. Clin. Oral Implants Res. 2021, 32, 1052–1060. [Google Scholar] [CrossRef]
- Marei, H.F.; Abdel-Hady, A.; Al-Khalifa, K.; Al Mahalawy, H. Influence of surgeon experience on the accuracy of implant placement via a partially computer-guided surgical protocol. Int. J. Oral Maxillofac. Implants 2019, 34, 1177–1183. [Google Scholar] [CrossRef]
- Han, X.-Y.; Xu, X.-M.; Ju, Y.-Q.; Tian, Z.-J. Analysis of implant placement accuracy using freehand in 68 consecutive patients with 97 implants. Shanghai Kou Qiang Yi Xue 2020, 29, 440–444. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
| Group A (Sinus Floor Augmentation via Lateral Approach) | Group B (Transcrestal Sinus Floor Elevation) | Group C (One Tilted and One Axial Implants) | |
|---|---|---|---|
| Residual bone height | Less than 5 mm, inadequate bone volume in the retrocanine area for tilted implant placement at least 10 mm long, impossibility of combining a tilted implant with an axial one and absence of any contraindication to sinus augmentation [15,16,17,18,19] | Minimum of 5 mm [20,21,22] | Less than 7 mm, adequate bone volume in the retrocanine area for tilted implant placement at least 10 mm long, possibility of combining a tilted implant with an axial one and contraindication to sinus augmentation [18,19,20,21,22] |
| Dental Implant Details | |||||
|---|---|---|---|---|---|
| Length 9 mm | Length 11 mm | Length 13 mm | Length 15 mm | ||
| Group A (sinus floor augmentation via lateral approach) n = 48 | diameter 3.3 mm | 6 | 7 | 0 | 0 |
| diameter 3.8 mm | 29 | 6 | 0 | 0 | |
| Group B (transcrestal sinus floor elevation) n = 46 | diameter 3.3 mm | 2 | 3 | 1 | 0 |
| diameter 3.8 mm | 16 | 21 | 3 | 0 | |
| Group C (one tilted and one axial implant) n = 50 | diameter 3.3 mm | 0 | 0 | 4 | 4 |
| diameter 3.8 mm | 0 | 2 | 29 | 11 | |
| Implants Placed | Early Failure | Late Failure | Implant Survival Rate | |
|---|---|---|---|---|
| Group A | 48 | 0 | 2 | 95.83% |
| Group B | 46 | 1 | 1 | 95.65% |
| Group C | 50 | 1 | 0 | 98% |
| Dependent Variable: Prop_lost Dental Implants | |||||
|---|---|---|---|---|---|
| Source | Type III Sum of Squares | Df | Mean Square | F | Sig. |
| Corrected Model | 0.036 a | 2 | 0.018 | 0.539 | 0.586 |
| Intercept | 0.363 | 1 | 0.363 | 10.775 | 0.002 |
| Group | 0.036 | 2 | 0.018 | 0.539 | 0.586 |
| Error | 1.920 | 57 | 0.034 | ||
| Total | 2.319 | 60 | |||
| Corrected Total | 1.956 | 59 | |||
| Descriptive Statistics | ||||
|---|---|---|---|---|
| Group | Mean | Std. Deviation | N | |
| I1_MBL 6 months (mm) | A | 0.970 | 0.1455 | 20 |
| B | 0.915 | 0.1387 | 20 | |
| C | 0.920 | 0.1508 | 20 | |
| Total | 0.935 | 0.1448 | 60 | |
| I1_MBL 12 months (mm) | A | 1.095 | 0.1356 | 20 |
| B | 1.085 | 0.1663 | 20 | |
| C | 1.040 | 0.1847 | 20 | |
| Total | 1.073 | 0.1625 | 60 | |
| I1_MBL 24 months (mm) | A | 1.250 | 0.1235 | 20 |
| B | 1.260 | 0.1729 | 20 | |
| C | 1.255 | 0.1572 | 20 | |
| Total | 1.255 | 0.1501 | 60 | |
| I1_MBL 36 months (mm) | A | 1.470 | 0.0801 | 20 |
| B | 1.500 | 0.1338 | 20 | |
| C | 1.475 | 0.0786 | 20 | |
| Total | 1.482 | 0.1000 | 60 | |
| I1_MBL 48 months (mm) | A | 1.695 | 0.1986 | 20 |
| B | 1.720 | 0.2238 | 20 | |
| C | 1.585 | 0.0933 | 20 | |
| Total | 1.667 | 0.1875 | 60 | |
| Descriptive Statistics | ||||
|---|---|---|---|---|
| Group | Mean | Std. Deviation | N | |
| I2_MBL 6 months (mm) | A | 0.918 | 0.1131 | 17 |
| B | 0.888 | 0.1310 | 16 | |
| C | 0.936 | 0.1447 | 14 | |
| Total | 0.913 | 0.1279 | 47 | |
| I2_MBL 12 months (mm) | A | 1.094 | 0.1249 | 17 |
| B | 1.088 | 0.1708 | 16 | |
| C | 1.100 | 0.1177 | 14 | |
| Total | 1.094 | 0.1374 | 47 | |
| I2_MBL 24 months (mm) | A | 1.306 | 0.1345 | 17 |
| B | 1.238 | 0.1258 | 16 | |
| C | 1.236 | 0.1336 | 14 | |
| Total | 1.262 | 0.1328 | 47 | |
| I2_MBL 36 months (mm) | A | 1.488 | 0.0781 | 17 |
| B | 1.481 | 0.1109 | 16 | |
| C | 1.450 | 0.1092 | 14 | |
| Total | 1.474 | 0.0988 | 47 | |
| I2_MBL 48 months (mm) | A | 1.588 | 0.0857 | 17 |
| B | 1.681 | 0.1328 | 16 | |
| C | 1.600 | 0.1569 | 14 | |
| Total | 1.623 | 0.1306 | 47 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gherlone, E.F.; D’Orto, B.; Nagni, M.; Capparè, P.; Vinci, R. Tilted Implants and Sinus Floor Elevation Techniques Compared in Posterior Edentulous Maxilla: A Retrospective Clinical Study over Four Years of Follow-Up. Appl. Sci. 2022, 12, 6729. https://doi.org/10.3390/app12136729
Gherlone EF, D’Orto B, Nagni M, Capparè P, Vinci R. Tilted Implants and Sinus Floor Elevation Techniques Compared in Posterior Edentulous Maxilla: A Retrospective Clinical Study over Four Years of Follow-Up. Applied Sciences. 2022; 12(13):6729. https://doi.org/10.3390/app12136729
Chicago/Turabian StyleGherlone, Enrico Felice, Bianca D’Orto, Matteo Nagni, Paolo Capparè, and Raffaele Vinci. 2022. "Tilted Implants and Sinus Floor Elevation Techniques Compared in Posterior Edentulous Maxilla: A Retrospective Clinical Study over Four Years of Follow-Up" Applied Sciences 12, no. 13: 6729. https://doi.org/10.3390/app12136729
APA StyleGherlone, E. F., D’Orto, B., Nagni, M., Capparè, P., & Vinci, R. (2022). Tilted Implants and Sinus Floor Elevation Techniques Compared in Posterior Edentulous Maxilla: A Retrospective Clinical Study over Four Years of Follow-Up. Applied Sciences, 12(13), 6729. https://doi.org/10.3390/app12136729