Abstract
Background: In the literature, there are few studies on included mandibular canines and possible therapeutic solutions for arch restoration. The aim of this review was to evaluate how the recovery of included mandibular canines is performed in adolescent patients with mixed or permanent dentition. The clinical case reported is that of successful orthodontic surgical treatment in an 11-year-old mixed-dentition patient with an included mandibular right canine. Methods: A literature search was performed using the PubMed/Medline, Scopus, Web of Science, and Cochrane Library databases with the following Boolean indicators: canine, mandibular, impacted. The inclusion criteria were year of publication between 2017 and 2022, orthodontic canine surgical approach included, age between 9 and 18 years, free full text, and English language. Results: A total of 536 articles was identified through the electronic search, and 11 articles published between 2017 and 2022 were ultimately included in the qualitative analysis. Conclusions: In the majority of cases, combined surgical–orthodontic therapy, as reported in the studies that we reviewed, is successful in correcting the eruption defect, restoring the canine to occlusion and the physiological arch perimeter, and maintaining the health of the periodontal supporting tissues.
1. Introduction
Altered tooth eruption indicates a tooth that fails to achieve the correct position in the arch, and can result in two clinical conditions that can be combined: inclusion, and transmigration. The incidence of included mandibular canines (IMCs) and transmigrated mandibular canines (TMCs) is rare, and is less frequent than that of impacted maxillary canines (IMXCs) [1]. IMCs have a prevalence of 0.05% to 0.4%, while IMXCs have a frequency of inclusion ranging from 1 to 3% [2].
The included tooth may occasionally remain in the same hemiarch or migrate laterally via a phenomenon called transmigration [3]. The mandibular and maxillary canines play a fundamental role in maintaining the arch form and function. Failure of included canines to recover may result in resorption or migration of near roots, loss of natural arch form, or the formation of dentigerous cysts [4].
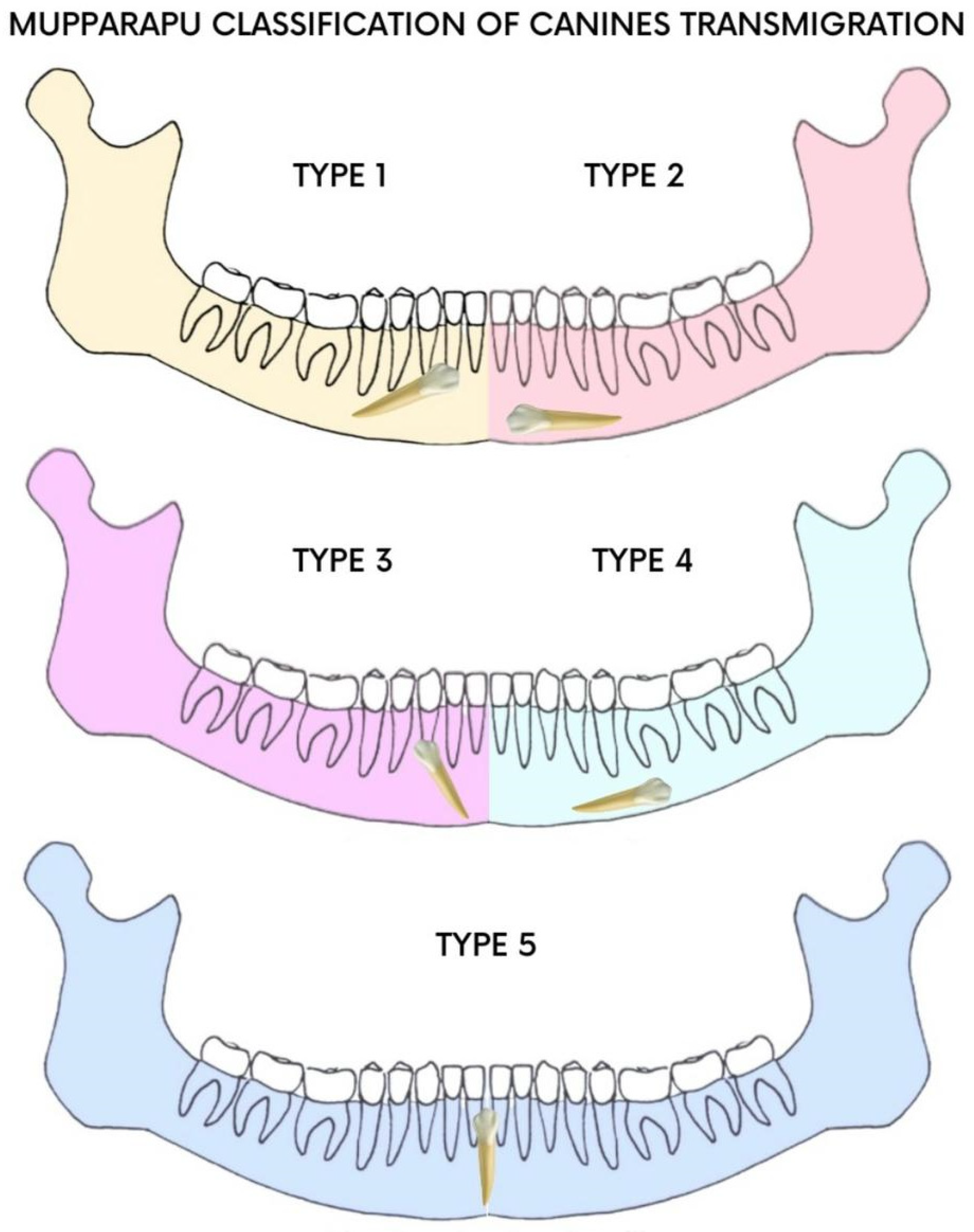
According to Mupparapu’s classification (Figure 1), TMCs are classified into five types [5]; type 1 is the most frequent. Early diagnosis makes it possible to assess the extent of canine transmigration and reduce aesthetic and functional complications [6,7,8,9,10].
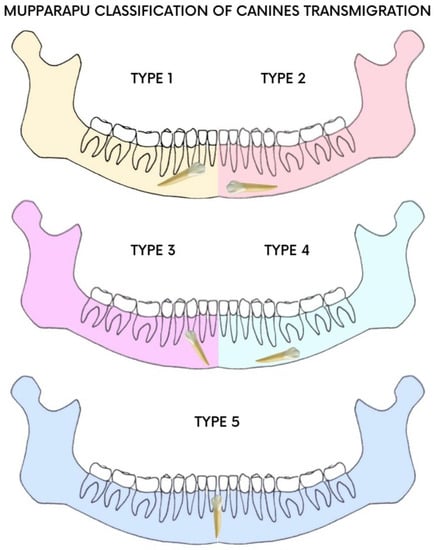
Figure 1.
Mupparapu classification.
There are some hypotheses as to the causes of included mandibular canines, and these include premature loss of deciduous teeth, retention of the deciduous canine, odontomas, crowding, and supernumerary teeth [11,12]. However, the etiology and exact mechanism are still unclear [12]. Consequently, it is difficult to find clinical guidelines derived from valid studies based on large patient samples. The current state of the art provides for various approaches to the problem of included canines. Depending on the age of the patient and the severity of the inclusion, interceptive therapy is provided where possible; guided forced eruption with repositioning in the arch is implemented in cases of medium severity; and in severe cases that cannot be recuperated, avulsion of the element is performed [13]. Early diagnosis and clinical and radiological evaluation can help the dentist to plan the surgical technique and avoid possible complications [14]. Surgical techniques provide for guided eruption with a closed or open technique in the case of buccal positioning of the included tooth [15,16]. Few systematic reviews on this subject can be found in the literature; therefore, it is difficult for clinicians to identify clear guidelines on the topic [17]. The aim of this article is to describe the buccal surgical approach used to engage and return the mandibular canine to the arch, and to review the scientific literature regarding the recurrence of IMCs, the successes described, the periodontal health of the treated tooth, and the techniques adopted.
2. Materials and Methods
2.1. Systematic Literature Review Methodology
2.1.1. Search Strategies
Article screening was performed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [18]. The review protocol was registered with PROSPERO under the unique number CRD42022342607. Details of the protocol can be found at https://www.crd.york.ac.uk/prospero (accessed on 8 July 2022).
The search strategy was conducted with the keywords ((canine) AND (mandibular)) AND (impacted) as illustrated in Table 1.

Table 1.
Search strategies and keywords.
Initial screening was performed using the electronic databases PubMed, Scopus, Web of Science, and Cochrane (June 2022), with the Boolean indicators canine AND mandibular AND impacted. The titles and abstracts of scientific studies were assessed, and an initial screening was performed. Articles were restricted to randomized and non-randomized human clinical trials, prospective and retrospective studies, clinical case reports, and case series, and the full text was assessed for suitability for descriptive analysis.
2.1.2. Inclusion and Exclusion Criteria
The criteria required for inclusion (Table 2) in the qualitative synthesis were limited to studies including patients aged between 9 and 18 years with inclusion and/or transmigration of the mandibular canine, original prospective and retrospective studies on human subjects, studies including a clear description of the materials and techniques applied, and studies with surgical and orthodontic techniques.
Table 2.
Inclusion and exclusion criteria.
The exclusion criteria (Table 2) were studies on patients with genetic syndromes and severe facial malformations, systematic literature reviews and letters to editors, and non-English-language articles.
2.1.3. Article Identification Procedure
The suitability assessment was conducted independently by three reviewers (C.V., G.L., and C.M.). In addition, a manual search was conducted to increase the pool of articles for full-text evaluation. Articles written in English that met the inclusion criteria were taken into account, while duplicates and excluded articles were categorized by stating the reasons for exclusion.
2.1.4. Study Evaluation
The article data were independently evaluated by the reviewers using a special electronic form designed according to the following categories: study model design, patient age, major symptoms, associated neoplasms or neoformations, treatment protocol, surgical technique, postoperative sequelae, tooth position, periodontal evaluation of included canines, number of subjects, and study results.
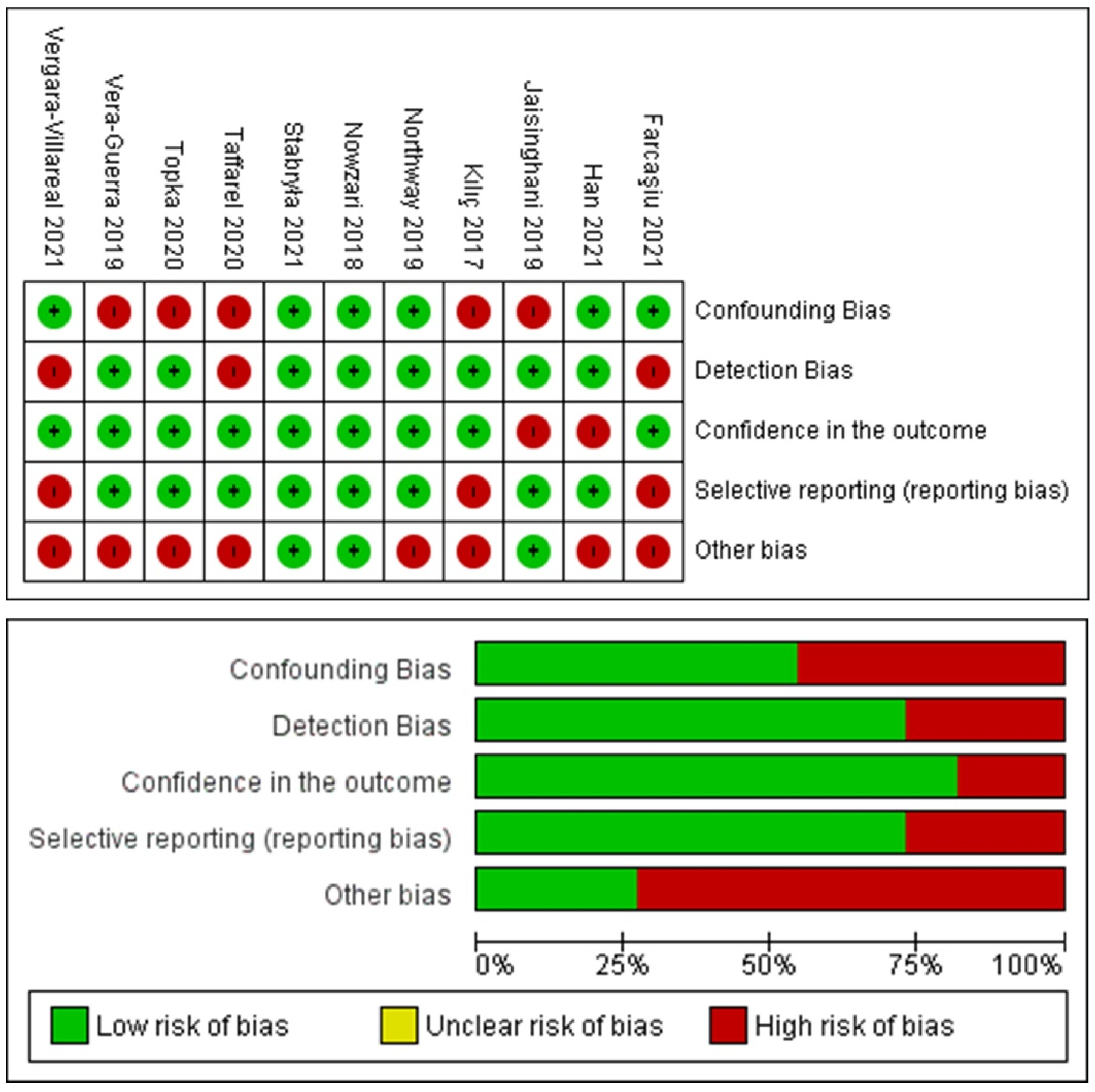
2.1.5. Risk-of-Bias Evaluation
The risk of bias was evaluated in accordance with the OHAT risk-of-bias tool for human and animals studies. The evaluation considered the following criteria: confounding bias, detection bias, confidence in the outcome, reporting bias, and other biases. The risk-of-bias findings were classified as adequate, unclear, or inadequate. The selected studies were categorized as having a low risk of bias with a minimum ratio of 4/5 positive parameters. Otherwise, the studies were classified as high-risk-of-bias articles.
3. Results
3.1. Study Selection and Characteristics
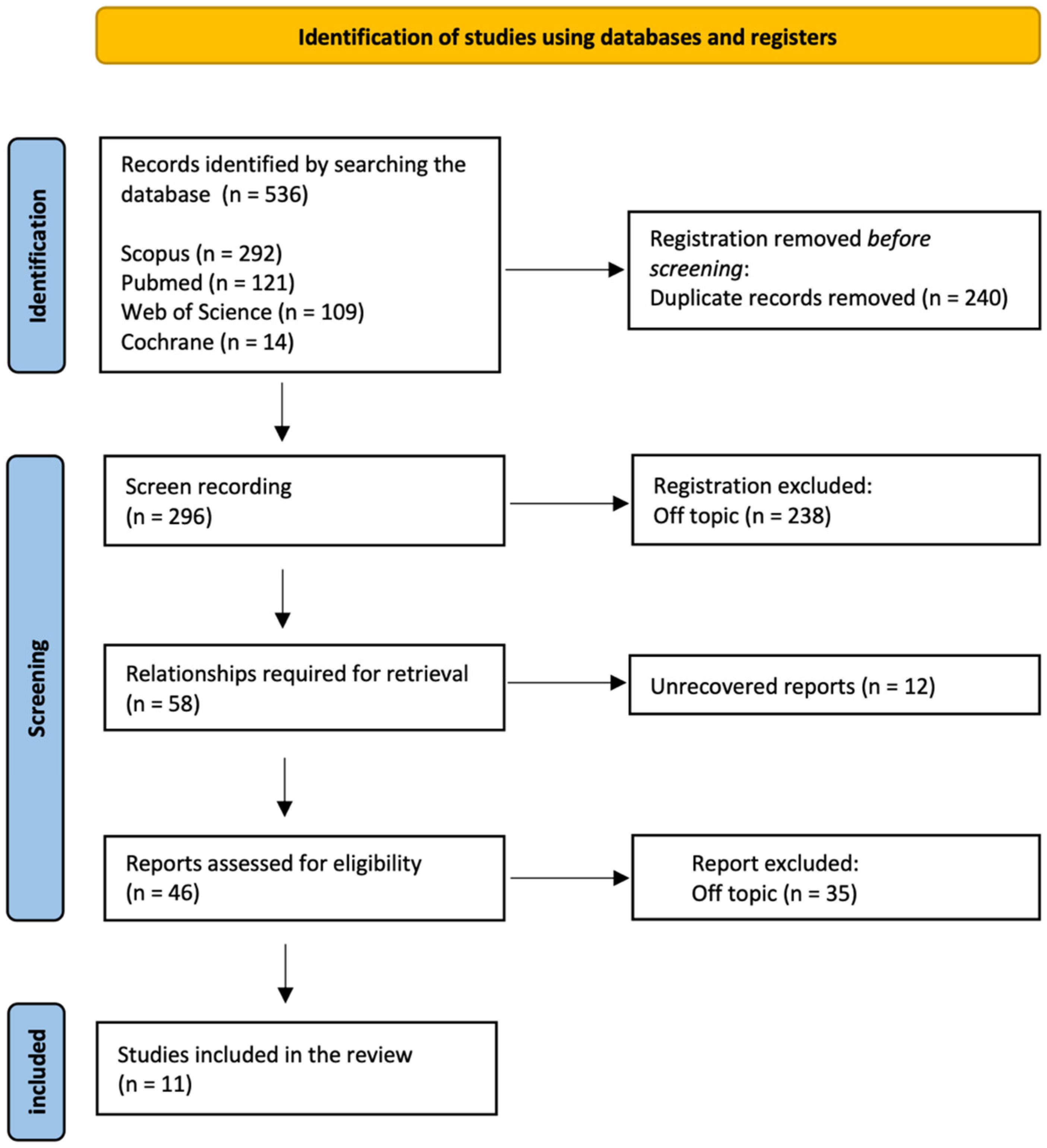
The electronic database and manual search output retrieved a total of 536 manuscripts (Scopus n = 292, PubMed n = 121, Web of Science n = 109, Cochrane n = 14); a total of 240 duplicates was removed. After initial screening, a total of 296 manuscripts was considered. Eligibility assessment was conducted on 46 articles, because 238 articles were off-topic, and the full text of 12 was not available. After reading the full texts, 11 articles were selected for qualitative synthesis. The PRISMA flowchart diagram is illustrated in Figure 2.
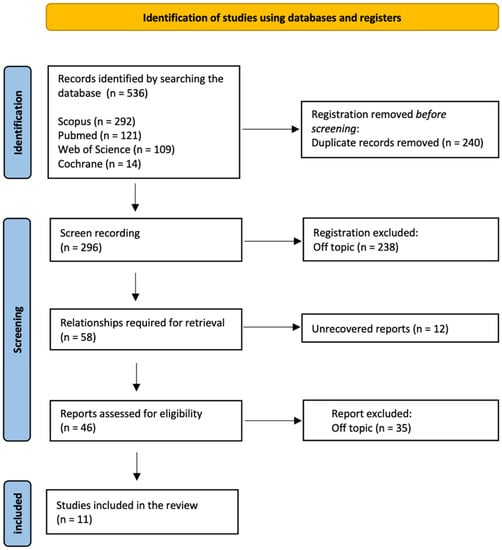
Figure 2.
PRISMA flowchart diagram of the inclusion process.
The review selection included a total of 19 cases of IMC. Seven articles described unilateral cases (TMC or IMC) [17,18,19,20,21,22,23] and four described bilateral cases (TMC and IMC) [24,25,26,27]. The mean age of the patients ranged from 11 to 18 years. The cases reported in the 11 articles concerned asymptomatic patients without dentigerous cysts. An orthodontic surgical approach was performed in all cases. Postoperative sequelae were often associated with mild healing symptoms. Gingival recession caused by bracket malposition on 4.3 was described in only one case [23]. Table 3 describes the studies’ characteristics.
Table 3.
Descriptive summary of item selection.
3.2. Risk-of-Bias Assessment Findings
The analysis is presented in Figure 3 for a total of 11 included articles. A total of three articles showed a low risk of bias considering the heterogeneity of the model designs and methodologies. No randomized/blinded clinical trials were detected for further qualitative assessment and meta-analysis statistical evaluation.
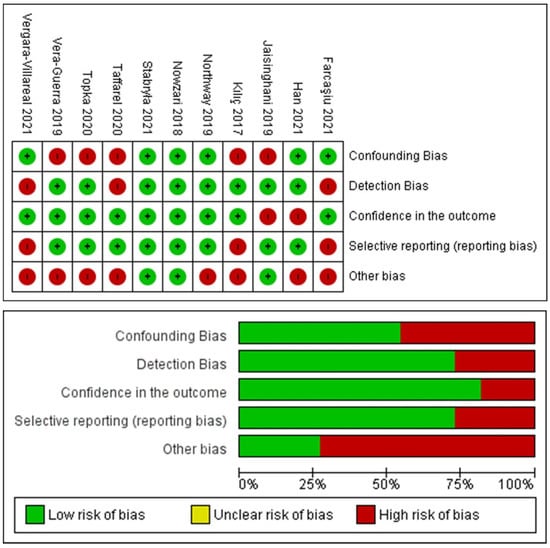
Figure 3.
Graphs of the risk-of-bias assessment of the included studies.
4. Case Report
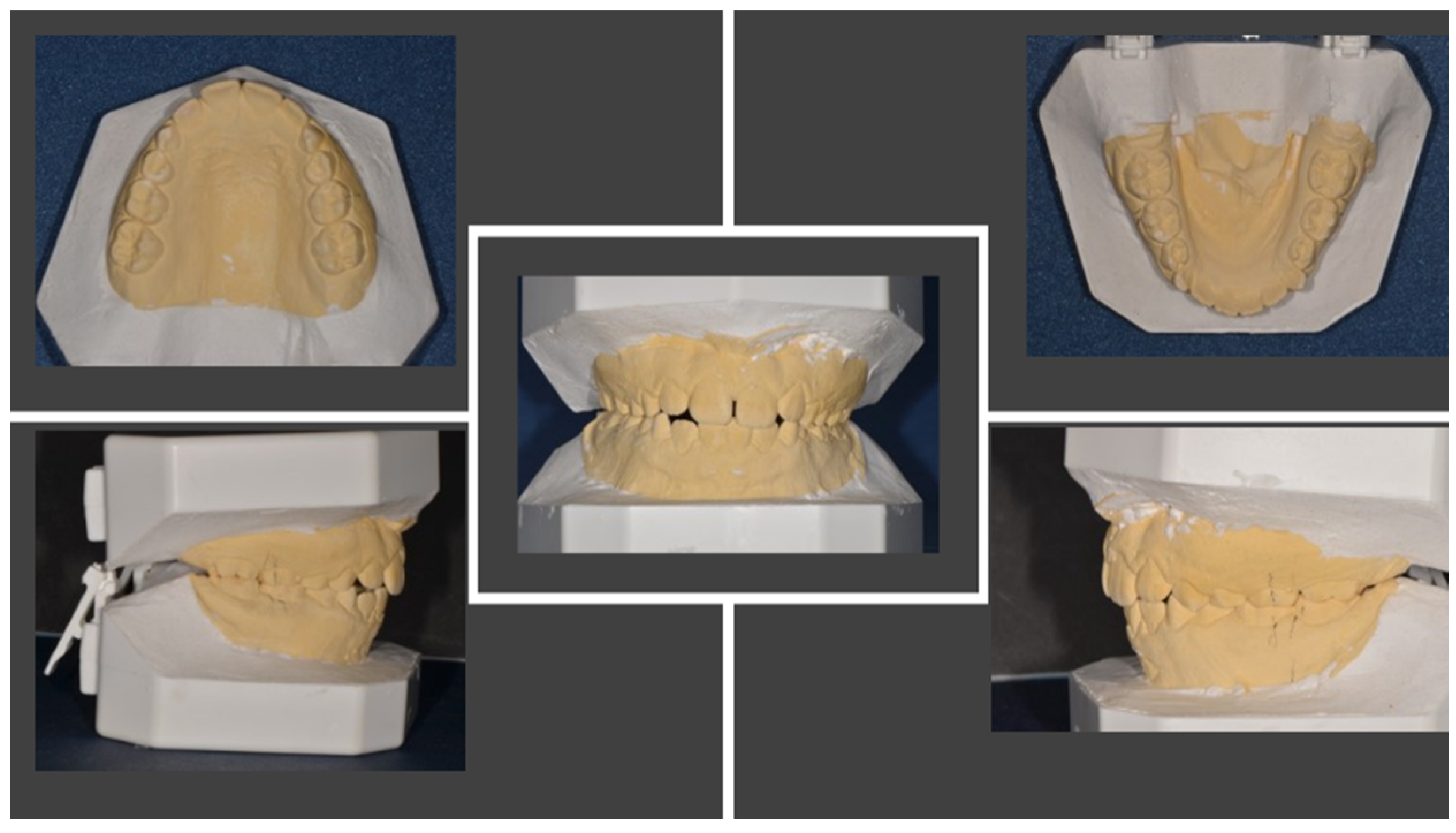
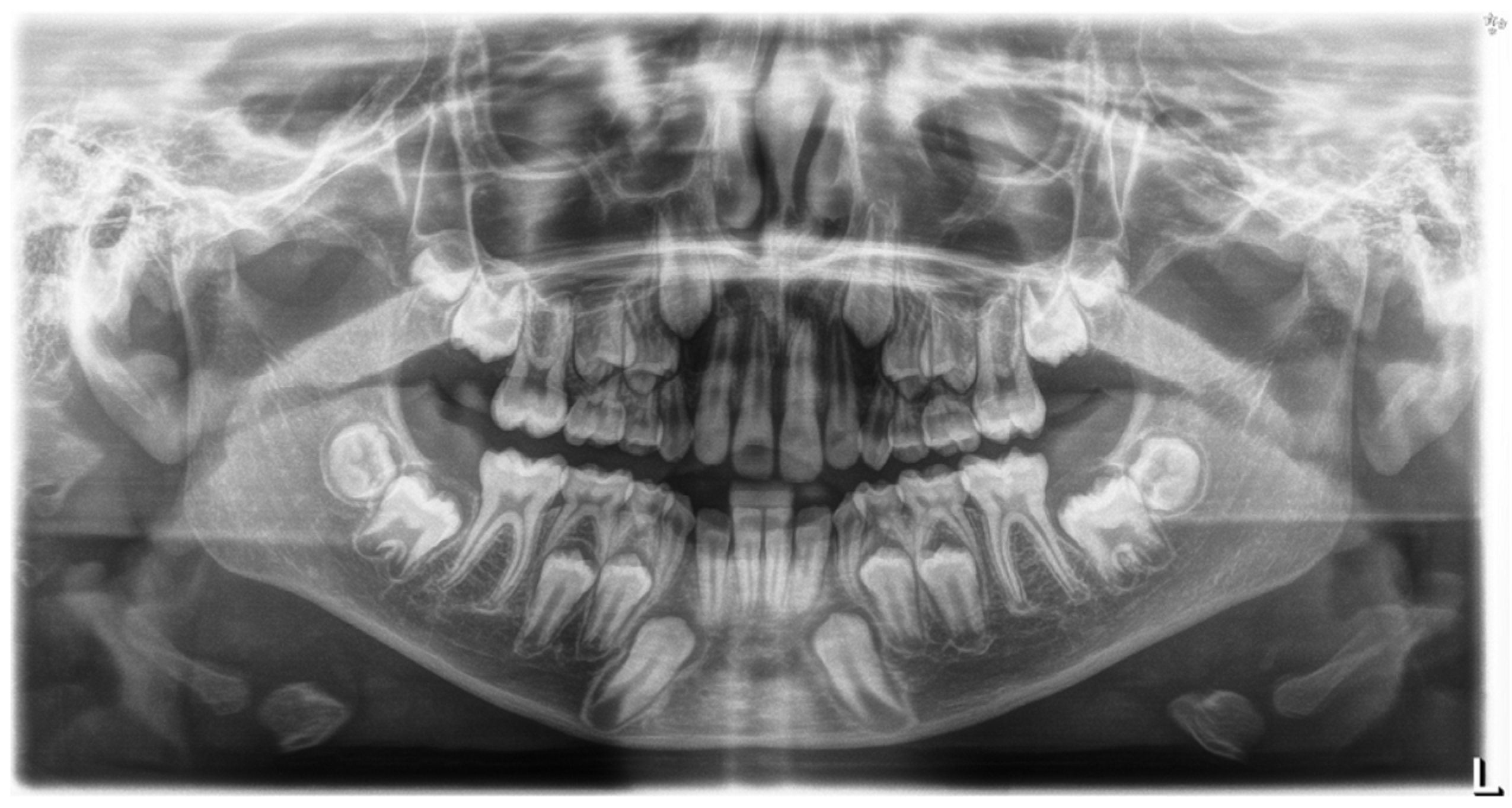
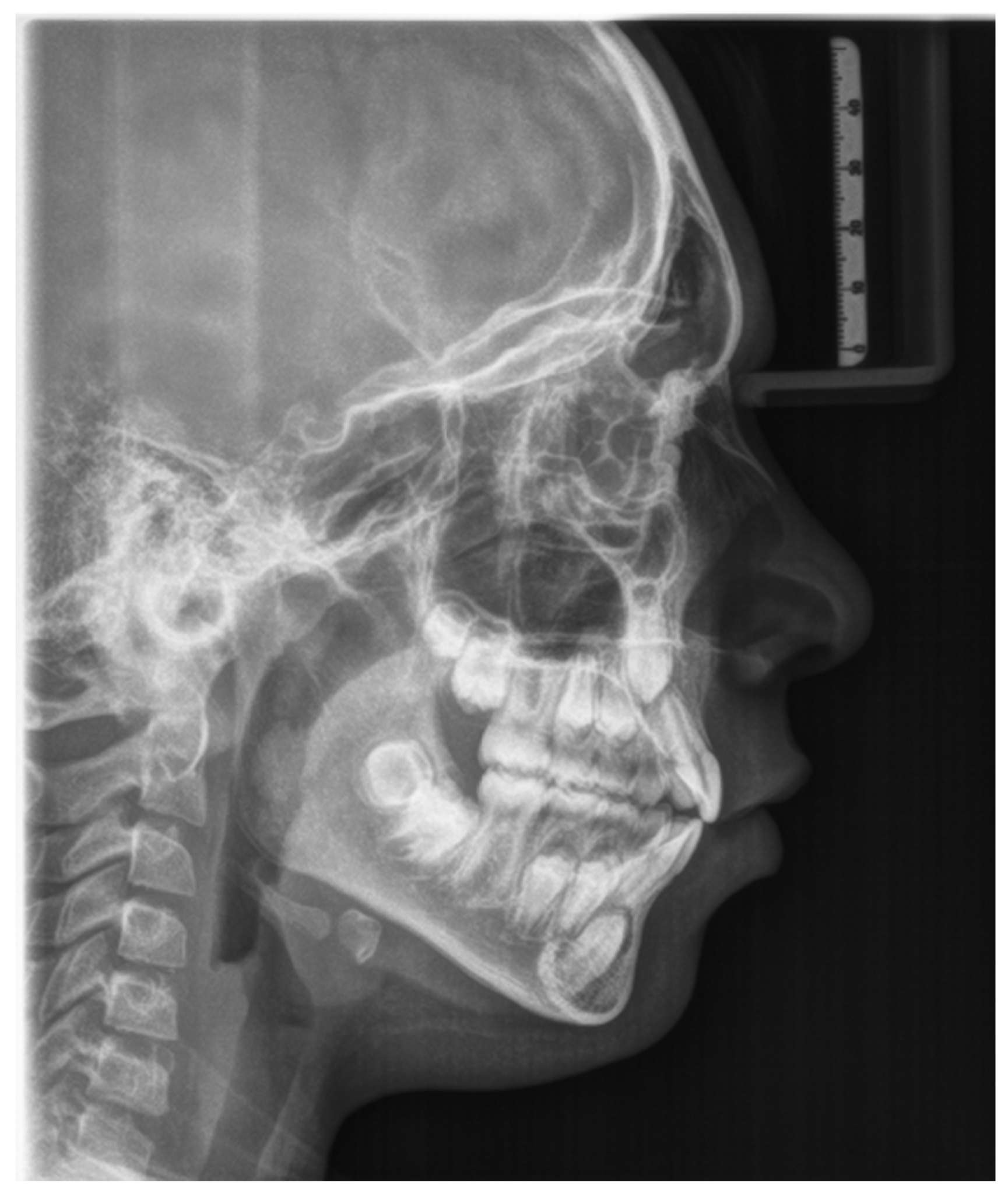
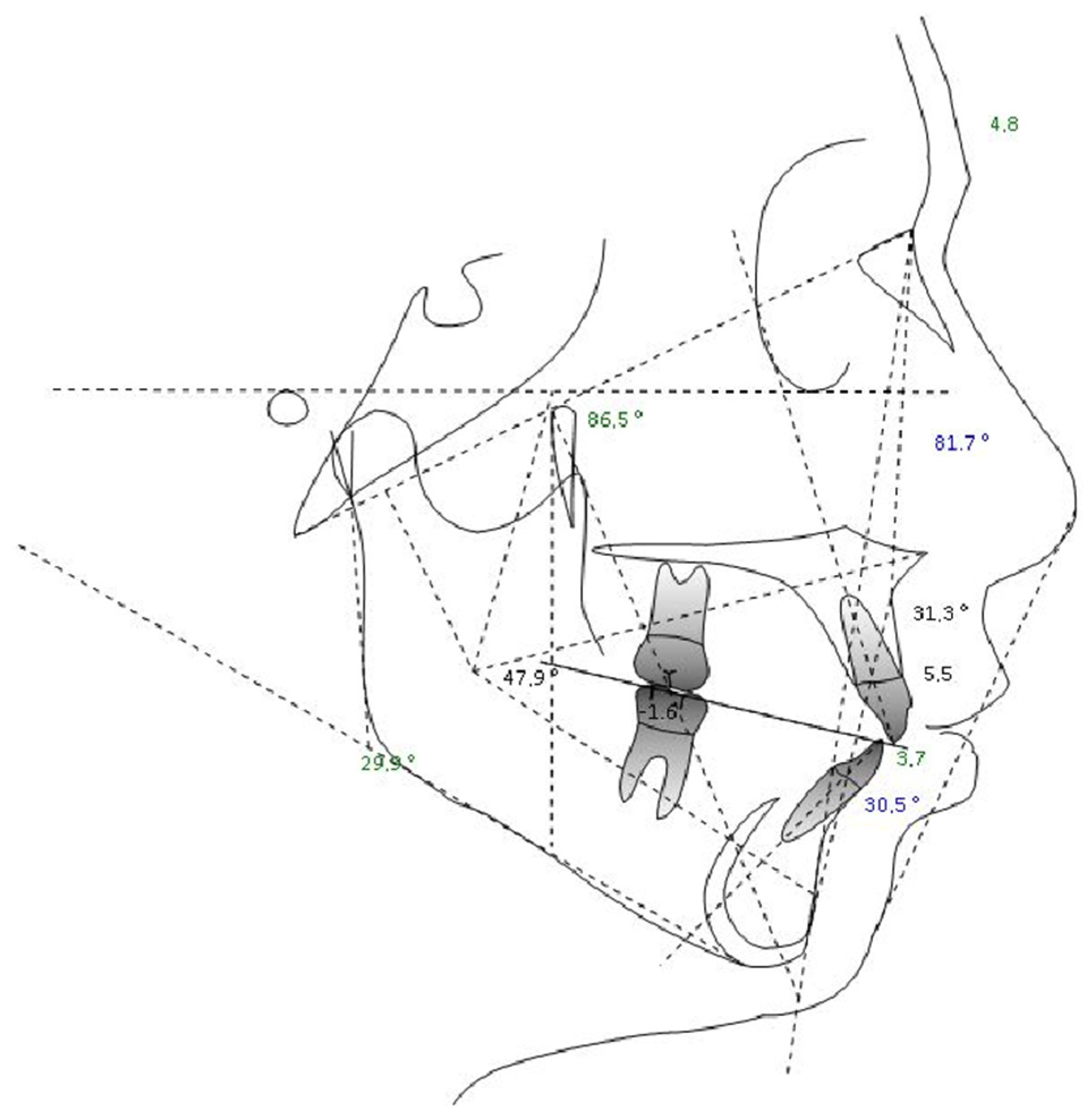
The patient was an 11.5-year-old child undergoing orthodontic treatment. He presented with mixed dentition, Angle Class I dental relationship of the permanent dentition with a 1 mm overjet, centered midlines, and slight crowding in both arches. All clinical documentation—consisting of impressions and study models (Figure 4), Rx OPT (Figure 5), lateral cranial Rx (Figure 6), and cephalometric analysis (Figure 7, Table 4)—was collected for case evaluation and subsequent treatment.
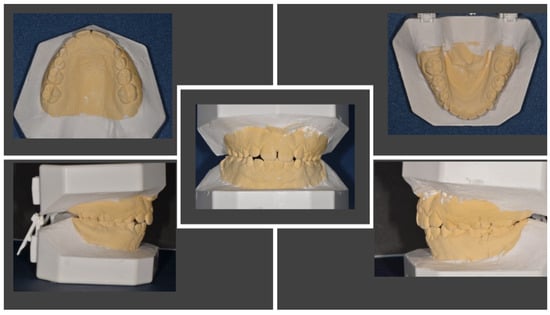
Figure 4.
Study models before orthodontic therapy.
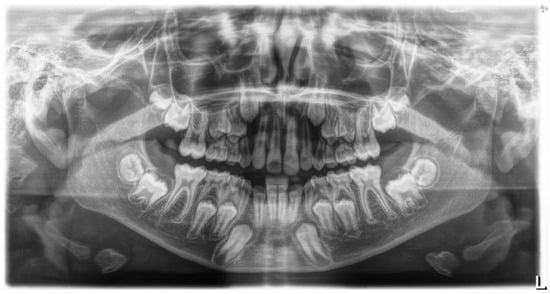
Figure 5.
Rx OPT before orthodontic treatment.
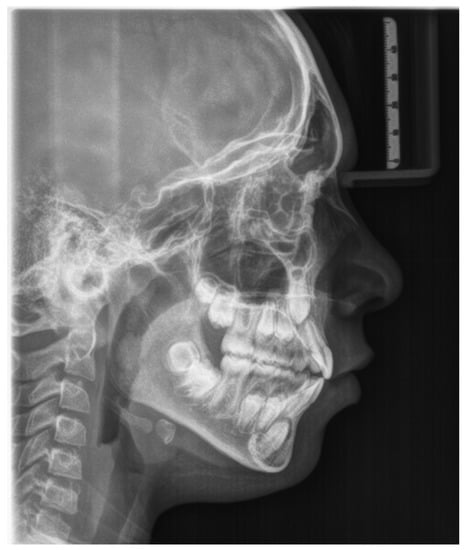
Figure 6.
Lateral cranial radiograph.
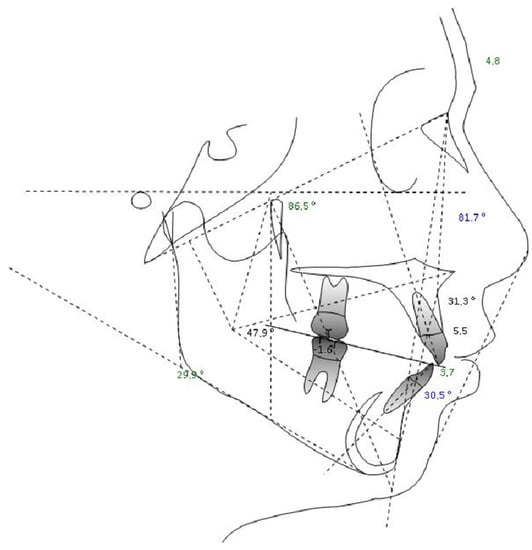
Figure 7.
Cephalometric analysis.
Table 4.
Cephalometric analysis results.
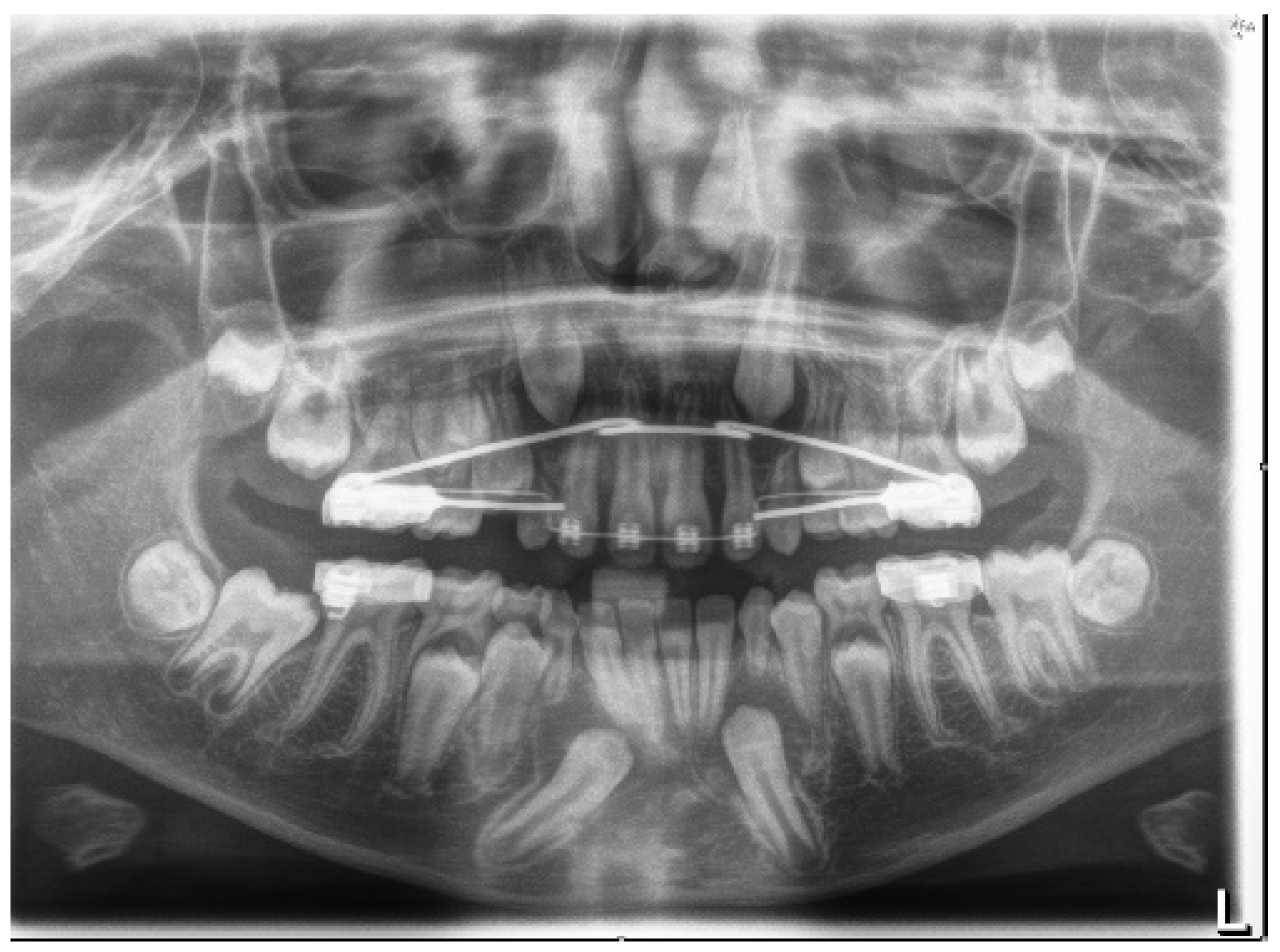
After one year of interceptive therapy, a control Rx OPT was performed to assess the status of the tooth permutation (Figure 8).

Figure 8.
Rx OPT with inclusion of element 4.3.
The Rx OPT showed the intraosseous inclusion with mesio angulation of the 4.3 element.
IMC was assessed according to Mupparapu’s classification [5], which describes five types of transmigrated mandibular canine (Figure 1). The clinical case described in this article concerns type number 1.
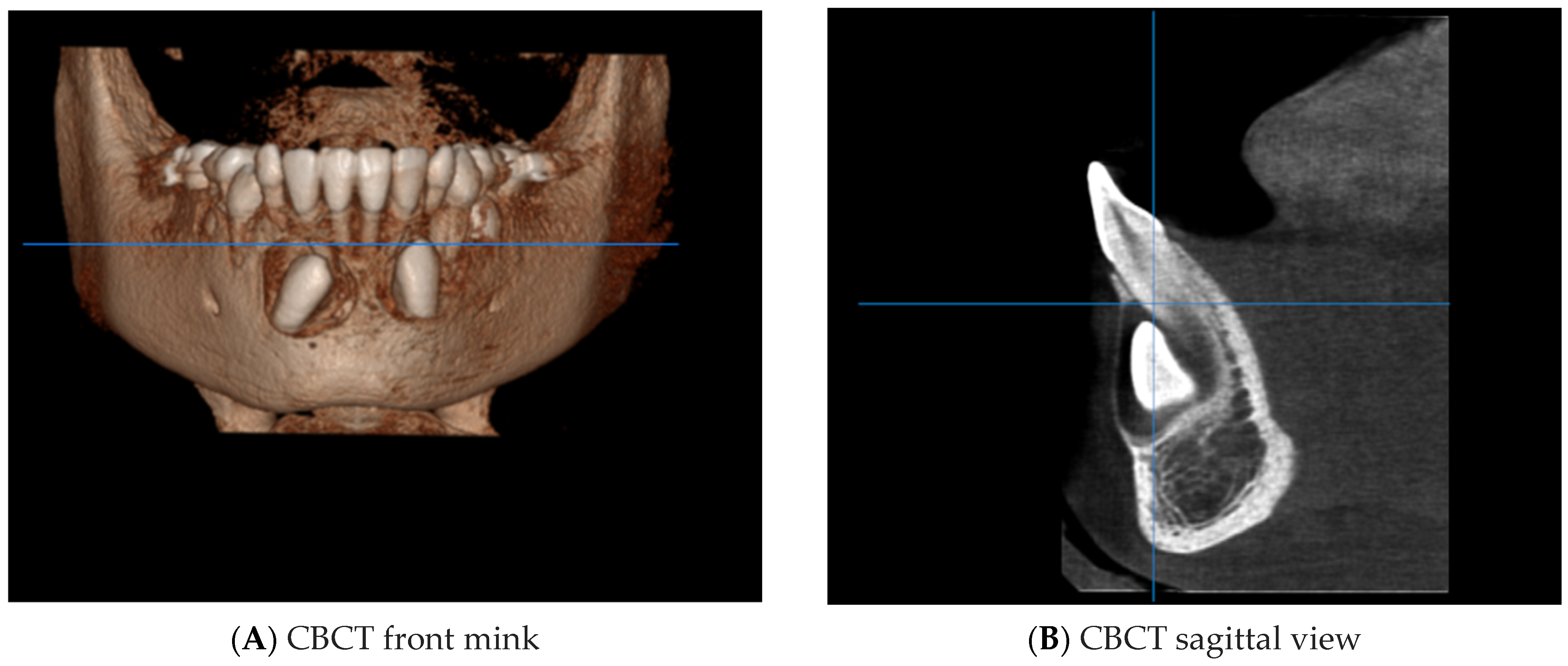
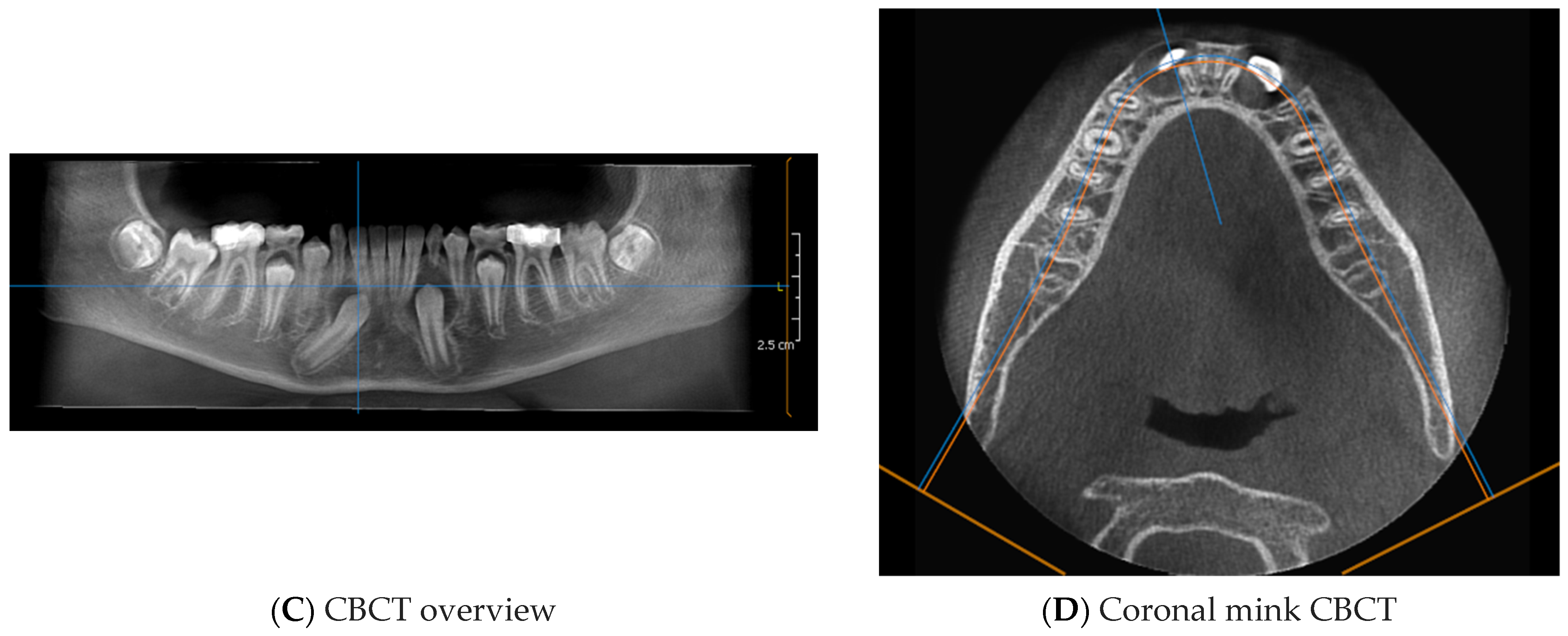
CBCT was performed to assess the position of the IMC in relation to the surrounding anatomical structures (Figure 9).
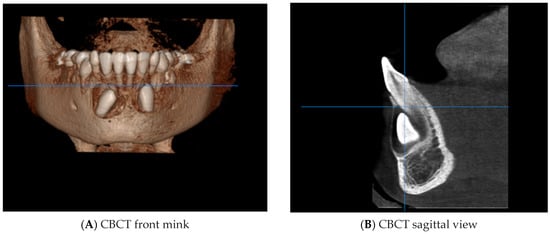
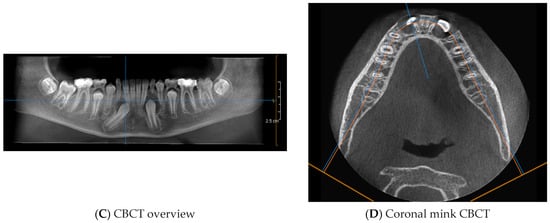
Figure 9.
CBCT of the IMC ((A) + (B) + (C) + (D)).
The CBCT showed part of the crown of the IMC (4.3) in contact with the root apices of the right lower incisors. (4.1 and 4.2).
All of this diagnostic information allowed us to choose between the following treatment options:
- -
- Interceptive treatment, including the extraction of a primary canine or the opening of an orthodontic space with fixed appliances [29];
- -
- Orthodontic extrusion of 4.3 [26];
- -
- Transalveolar transplantation of 4.3 [30];
- -
- Avulsion of 4.3 [31].
The positional factors that influenced the decision to surgically remove or surgically expose the IMC were considered. These included the following:
- Canine angle to the midline;
- Horizontal position of the canine root apex;
- Vertical height of the canine crown;
- Canine overlap of adjacent tooth;
- Buccal–lingual position of the canine.
After explaining the clinical situation and the possible therapeutic solutions to the parents and the young patient, it was decided, after obtaining the informed consent of the parents, to recover the included element (4.3) through a combined orthodontic–surgical approach. The treatment involved three phases, which are described below.
4.1. Phase 1: Initial Orthodontic Treatment
The first phase of the treatment involved orthodontic therapy aimed at preparing the anchorage teeth by aligning and levelling the arches. Once the maximum thickness of the wires was reached, the decision was made to surgically anchor the IMC.
4.2. Phase 2: Surgical Technique
After local anesthetic infiltration, an intrasulcular incision was made from 4.3 to 4.1, and then a vertical release incision (mesial to 4.1) was made to facilitate elevation and visibility of the flap. A full-thickness flap was elevated. Avulsion of the corresponding deciduous element was performed. The apical cortex of the alveolus was removed to reach the crown of the IMC. A bone tunnel was created through which the ligature was passed so that traction would be directed towards the center of the ridge (tunnel technique) [15].
Using an adhesion technique, an orthodontic bracket was bonded to 4.3 and connected to a metal ligature. The metal ligature was inserted along the previously created tunnel. The adhesion was finally tested by applying forced traction (of approximately 150 g). After thorough washing of the surgical field, the mucoperiosteal flap was finally repositioned and sutured.
4.3. Orthodontic Traction
Orthodontic traction was achieved through the use of a metal ligature directly on the multiple brackets in the presence of a rigid full-thickness steel wire. The traction force was approximately 50–60 g, with activation of the wire every 15–20 days.
4.4. Phase 3: Final Orthodontic Treatment
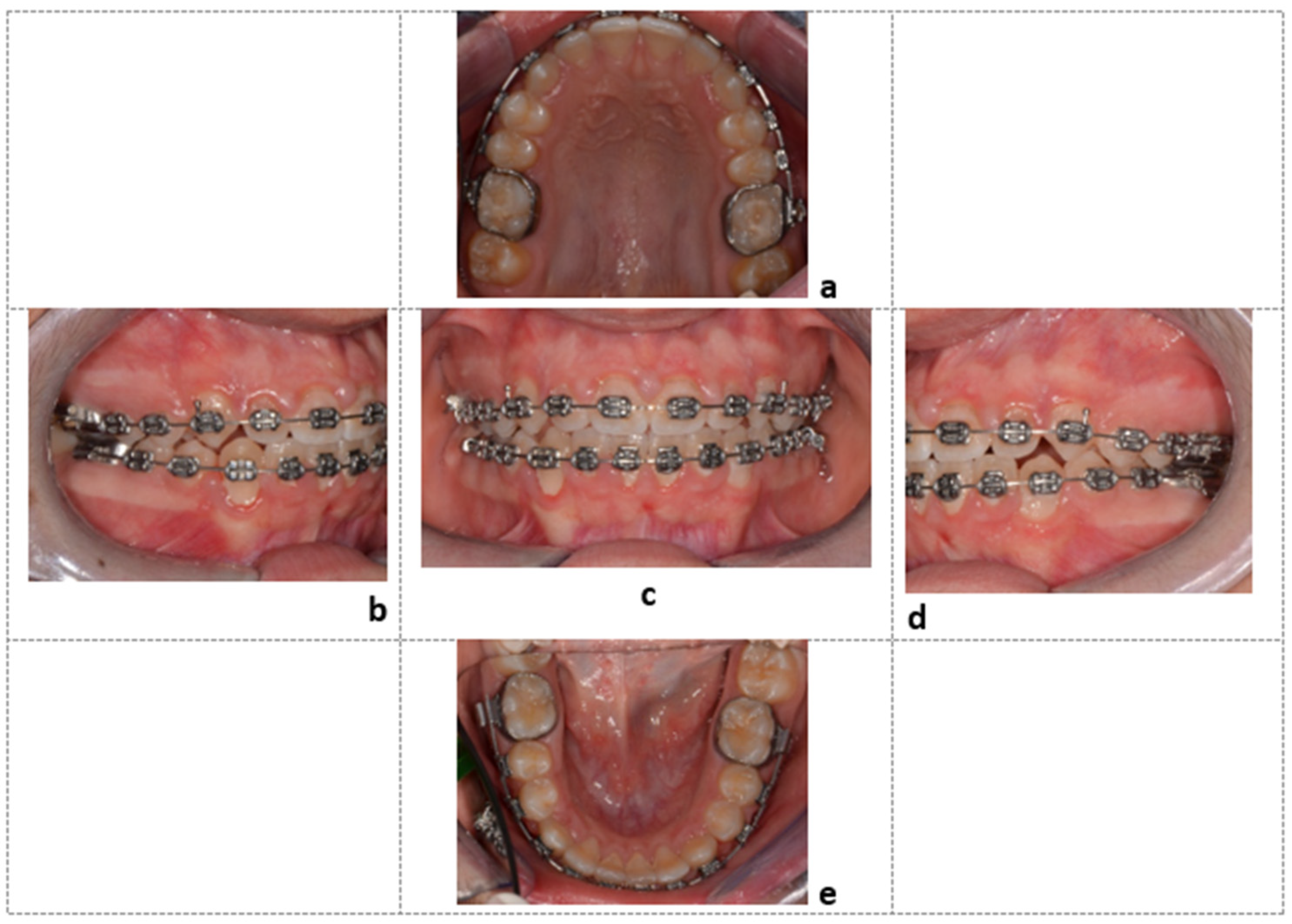
After the recovery of the element included in the arch was achieved, orthodontic therapy continued with the final steps to finalize the case (Figure 10).
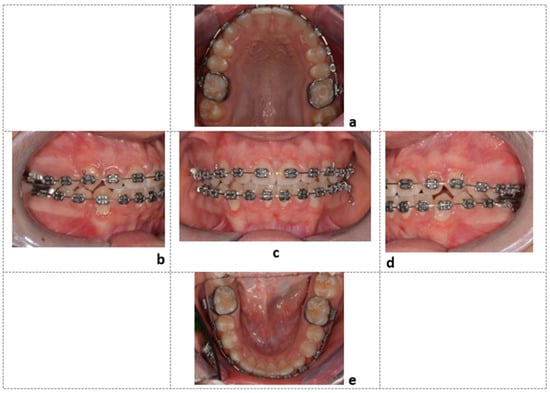
Figure 10.
Final intraoral photos of the patient: Element 4.3, recovered in the center of the dental arch, observed from the upper occlusal view (a), right lateral view (b), frontal view (c), left lateral view (d), and lower occlusal view (e).
5. Discussion
The treatment of IMCs requires a multidisciplinary approach [27]. Just as spontaneous eruption occurs harmoniously and leads to tooth alignment in the presence of healthy periodontal tissues, the combined surgical–orthodontic treatment of an included element should simulate physiological eruption [28]. Therefore, the aim of orthodontic therapy is to guide the eruption of the tooth towards the center of the ridge, while surgical treatment should ensure that the dental and periodontal structures are respected to avoid damage at the end of therapy [19].
Regarding the treatment of IMCs and TMCs, several treatment options can be considered, including orthodontic traction, self-grafting, and surgical removal of the IMC. The strategy of surgically removing IMCs is the quickest and easiest. Although more difficult and complicated, orthodontic traction is the most effective strategy to restore ideal occlusion. Orthodontic mini-screws can be used as temporary anchorage devices to prevent the negative effects of anchorage loss [28]. From a therapeutic point of view, radiological diagnosis in late mixed dentition remains an important tool to detect incidents of mandibular canine inclusion. The clinical case presentation describes the surgical technique of IMC exposure and repositioning in the arch using a combined surgical–orthodontic treatment. Guided eruption techniques have several benefits in dentistry. They can be used for several purposes, such as for tissue regeneration in either lingual [32] or conventional mechanics for impacted teeth [33]. There are two guided eruption techniques towards the center of the alveolar ridge: closed [34] and open [35,36]. In the first technique, an orthodontic bracket is attached to the tooth surface after a full-thickness flap is lifted, and the tooth and bracket are then entirely covered with tissue; meanwhile, the latter (open) method consists of apical repositioning of the full-thickness flap, leaving the element open [36,37,38]. The closed guided eruption technique was adopted in the clinical case described [20]. In the open guided eruption technique, an operculum is made on the IMC and an orthodontic traction is placed on it [20]. In both techniques, the principles of conservative surgery, adhesive technique, and controlled orthodontic traction are applied. In the cases selected in this review, one case with gingival recession was found [28]. In all cases there was periodontal success of the treated IMCs [19,20,21,22,23,24,25,26,27,39].
The reported clinical case was managed using the closed orthodontic eruption technique [15]. A mucoperiosteal flap was prepared with preservation of the interdental papillae, elevated to full thickness to allow minimal exposure of the included tooth for bracket adhesion. The minimal removal of cortical bone and pericoronal tissue, as well as the application of light forces during traction [40], also seems to explain the favorable periodontal outcome.
Some authors state that surgical exposure of the enamel–cement line predisposes patients to a greater risk of gingival recession and bone loss [41]. Finally, repositioning the flap in its original position maintains the entire portion of keratinized tissue, and reduces discomfort during healing [42].
Since the element in the bone inclusion was associated with the presence of the corresponding deciduous element in the arch, the “tunnel” technique was applied, as originally described by Crescini et al. in 1994 [15].
The extraction of the deciduous element creates a natural bone tunnel, and traction through this tunnel simulates a physiological eruption. The tooth is orthodontically pulled towards the center of the ridge, allowing the preservation of keratinized gingival tissue and subsequent periodontal health [34].
6. Conclusions
Although inclusion and transmigration of mandibular canines is a rare clinical condition, it is necessary to shed light on the most predictable treatment options to enable clinicians to carry out effective treatment protocols. According to the articles examined in our review, combined surgical–orthodontic treatment results in clinical success in the majority of cases, in terms of correcting the eruption defect, bringing the canine back into occlusion and into the physiological arch perimeter, and the health of the periodontal supporting tissue. To enable arch alignment of the tooth element while preserving periodontal integrity, the surgical–orthodontic traction must simulate the physiological eruption of the included tooth. All of the articles reviewed describe successful treatments for arch alignment, but periodontal success was not achieved in some of the cases described, due to bone ridge resorption, gingival recession, or root resorption; these are the main complications of surgical–orthodontic traction of the included elements, but the small percentage of cases in which they occurred allows this protocol to be defined as effective and predictable. More research is needed to understand the treatment outcomes of complex clinical cases, such as ankylosed elements.
Author Contributions
Conceptualization, A.D.I., V.C., F.P., F.I., A.M.I., D.D.V., G.D. and B.R.; methodology, A.N., I.F., M.C., G.L., F.V., S.C. (Sabino Ceci), G.M., A.P. (Andrea Palermo), A.M., C.L. and B.R.; software, A.P. (Assunta Patano), F.L., B.R. and G.D.; validation, F.I., A.P. (Assunta Patano), B.R., D.D.V., G.D., A.D.I., A.M.I. and A.S.; formal analysis, V.C., F.L., B.R., D.D.V. and A.D.I.; investigation, A.M.C., G.D., A.D.I., F.L., A.M.I., B.R., A.S. and F.I.; resources, A.M.I., G.D., B.R., A.D.I., F.I. and G.M.; data curation, G.D., I.F., F.L., A.N., B.R., A.M., F.V., M.C., S.C. (Stefania Costa), V.C., G.L., F.P., F.I. and D.D.V.; writing—original draft preparation, A.D.I., A.M.I., G.D., V.C., B.R., A.S. and F.I.; writing—review and editing, V.C., B.R., F.I., D.D.V., G.M. and G.D.; visualization, F.I., B.R. and A.S.; supervision, B.R., D.D.V., F.I., A.D.I. and A.S.; project administration, F.I., G.D., D.D.V. and B.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This clinical study was based at the University of Bari (Italy), in full compliance with ethical principles, including the Declaration of Helsinki of the World Medical Association, and the additional requirements of Italian law. In addition, the University of Bari, Italy, classified the study as exempt from ethical review, as it carries only negligible risks and involves the use of existing data that contain only non-identifiable data on humans. The patient in the case report signed a written informed consent form.
Informed Consent Statement
Informed consent was obtained from the subject involved in the study. Written informed consent was obtained from the patient to publish this document.
Data Availability Statement
All experimental data supporting the results of this study are available from the corresponding author upon request.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| IMC | Included mandibular canine |
| TMC | Transmigrated mandibular canine |
| IMXC | Included maxillary canine |
| OPT | Orthopantomography |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| CBCT | Cone-beam computed tomography |
| 4.3 | Lower mandibular canine |
| 4.1 | Lower-right central incisor |
| 4.2 | Lower-right lateral incisor |
References
- Cavuoti, S.; Matarese, G.; Isola, G.; Abdolreza, J.; Femiano, F.; Perillo, L. Combined Orthodontic-Surgical Management of a Transmigrated Mandibular Canine. Angle Orthod. 2015, 86, 681–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alhammadi, M.; Asiri, H.; Almashraqi, A. Incidence, Severity and Orthodontic Treatment Difficulty Index of Impacted Canines in Saudi Population. J. Clin. Exp. Dent. 2018, 10, e327–e334. [Google Scholar] [CrossRef] [PubMed]
- Gündüz, K.; Çelenk, P. The Incidence of Impacted Transmigrant Canines: A Retrospective Study. Oral Radiol. 2010, 26, 77–81. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Pede, C.D.; et al. The Efficacy of a New AMCOP® Elastodontic Protocol for Orthodontic Interceptive Treatment: A Case Series and Literature Overview. Int. J. Environ. Res. Public Health 2022, 19, 988. [Google Scholar] [CrossRef] [PubMed]
- Mupparapu, M. Patterns of Intra-Osseous Transmigration and Ectopic Eruption of Mandibular Canines: Review of Literature and Report of Nine Additional Cases. Dentomaxillofacial Radiol. 2002, 31, 355–360. [Google Scholar] [CrossRef]
- Majumdar, S.K.; Hossain, M.A.; De, N.; Chadda, D.; Bachhar, M.K.; Mishra, S. Effect of Diagnosis by Two-Dimensional Radiography Versus CBCT on Surgical Aspects of Transmigrated Impacted Mandibular Canines. J. Maxillofac. Oral Surg. 2020, 19, 461–467. [Google Scholar] [CrossRef]
- Laudadio, C.; Inchingolo, A.D.; Malcangi, G.; Limongelli, L.; Marinelli, G.; Coloccia, G.; Montenegro, V.; Patano, A.; Inchingolo, F.; Bordea, I.R.; et al. Management of Anterior Open-Bite in the Deciduous, Mixed and Permanent Dentition Stage: A Descriptive Review. J. Biol. Regul. Homeost. Agents 2021, 35, 271–281. [Google Scholar] [CrossRef]
- Montenegro, V.; Inchingolo, A.D.; Malcangi, G.; Limongelli, L.; Marinelli, G.; Coloccia, G.; Laudadio, C.; Patano, A.; Inchingolo, F.; Bordea, I.R.; et al. Compliance of Children with Removable Functional Appliance with Microchip Integrated during Covid-19 Pandemic: A Systematic Review. J. Biol. Regul. Homeost. Agents 2021, 35, 365–377. [Google Scholar] [CrossRef]
- Cirulli, N.; Ballini, A.; Cantore, S.; Farronato, D.; Inchingolo, F.; Dipalma, G.; Gatto, M.R.; Alessandri Bonetti, G. Mixed Dentition Space Analysis of a Southern Italian Population: New Regression Equations for Unerupted Teeth. J. Biol. Regul. Homeost. Agents 2015, 29, 515–520. [Google Scholar]
- Inchingolo, A.D.; Ceci, S.; Patano, A.; Inchingolo, A.M.; Montenegro, V.; Di Pede, C.; Malcangi, G.; Marinelli, G.; Coloccia, G.; Garibaldi, M.; et al. Elastodontic Therapy of Hyperdivergent Class II Patients Using AMCOP® Devices: A Retrospective Study. Appl. Sci. 2022, 12, 3259. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Palmieri, G.; et al. Genetic Pattern, Orthodontic and Surgical Management of Multiple Supplementary Impacted Teeth in a Rare, Cleidocranial Dysplasia Patient: A Case Report. Medicina 2021, 57, 1350. [Google Scholar] [CrossRef] [PubMed]
- Bertl, M.H.; Frey, C.; Bertl, K.; Giannis, K.; Gahleitner, A.; Strbac, G.D. Impacted and Transmigrated Mandibular Canines: An Analysis of 3D Radiographic Imaging Data. Clin. Oral Investig. 2018, 22, 2389–2399. [Google Scholar] [CrossRef] [PubMed]
- Azeem, M.; Afzal, A.; Ahmed, Z.; Ali, M.M.; Haq, A.U.; Hamid, W.U. Investigation of Transmigrated Mandibular Canines. Dent. Press J. Orthod. 2019, 24, 65. [Google Scholar] [CrossRef] [PubMed]
- Cakir Karabas, H.; Ozcan, I.; Erturk, A.F.; Guray, B.; Unsal, G.; Senel, S.N. Cone-Beam Computed Tomography Evaluation of Impacted and Transmigrated Mandibular Canines: A Retrospective Study. Oral Radiol. 2021, 37, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Crescini, A.; Baccetti, T.; Rotundo, R.; Mancini, E.A.; Prato, G.P. Tunnel Technique for the Treatment of Impacted Mandibular Canines. Int. J. Periodontics Restor. Dent. 2009, 29, 213–218. [Google Scholar]
- Plaza, S.P. Orthodontic Traction of a Transmigrated Mandibular Canine Using Mini-Implant: A Case Report and Review. J. Orthod. 2016, 43, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Dalessandri, D.; Parrini, S.; Rubiano, R.; Gallone, D.; Migliorati, M. Impacted and Transmigrant Mandibular Canines Incidence, Aetiology, and Treatment: A Systematic Review. Eur. J. Orthod. 2017, 39, 161–169. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- Kılıç, N.; Oktay, H. Orthodontic Intervention to Impacted and Transposed Lower Canines. Case Rep. Dent. 2017, 2017, 4105713. [Google Scholar] [CrossRef] [Green Version]
- Northway, W. Orthodontic Management of a Dental Anomaly Pattern (DAP) Including Mandibular Canine Transmigration: A Case Report: A Challenging Treatment but Worth It! Angle Orthod. 2019, 89, 149–162. [Google Scholar] [CrossRef] [Green Version]
- Vera-Guerra, J.A.; Herrera-Atoche, J.R.; Colomé-Ruiz, G.E. Orthodontic Treatment of Bilateral Impacted Mandibular Canines and a Mupparapu Type 2 Transmigration. Case Rep. Dent. 2019, 2019, 7638959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farcaşiu, C.; Dinescu, M.I.; Tărlungeanu, D.I.; Bataiosu, M.; Daguci, C.; Daguci, L.; Dina, M.N.; Andrei, O.-C. A Rare Case of Transmigrated Mandibular Canine and Combined Orthodontic–Surgical Management. Rom. J. Morphol. Embryol. 2022, 62, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Vergara-Villareal, P.; Del Castillo, K.; Ramírez-Ossa, D.; Barbosa-Liz, D. An Innovative Therapeutic Alternative for Correcting the Direction of Eruption of a Lower Mandibular Cuspid: A Mixed Dentition Case Report. Int. J. Orthod. Rehabil. 2021, 12, 79. [Google Scholar] [CrossRef]
- Stabryła, J.; Plakwicz, P.; Kukuła, K.; Zadurska, M.; Czochrowska, E.M. Comparisons of Different Treatment Methods and Their Outcomes for Impacted Maxillary and Mandibular Canines: A Retrospective Study. J. Am. Dent. Assoc. 2021, 152, 919–926. [Google Scholar] [CrossRef]
- Nowzari, H.; Rodriguez, A.E. Impacted Teeth: Closed Flap Surgery. J. Esthet. Restor. Dent. 2019, 31, 233–239. [Google Scholar] [CrossRef]
- Topka, A.; Racka-Pilszak, B.; Wojtaszek-Słomińska, A.; Orzelska-Blomberg, M. Surgical-Orthodontic Treatment of Impacted Permanent Canines in the Mandible: Two Case Reports. Jstoma 2020, 72, 282–290. [Google Scholar] [CrossRef]
- Taffarel, I.A.; Taffarel, I.P.; Gasparello, G.G.; Pithon, M.M.; Tanaka, O.M. Transmigrated Mandibular Canine Guided into Its Normal Position. J. Clin. Diagn. Res. 2020, 14, ZD01–ZD04. [Google Scholar] [CrossRef]
- Jaisinghani, A.P.; Pradhan, T.; Keluskar, K.M.; Takane, V. Treatment of a Transmigrated and an Impacted Mandibular Canine along with Missing Maxillary Central Incisor: A Case Report. Orthod. Waves 2019, 78, 84–92. [Google Scholar] [CrossRef]
- Hamdan, H.A.; Grünheid, T.; Larson, B.E. Effect of Orthodontic Treatment with Preadjusted Edgewise Appliances on the Buccolingual Inclination of Mandibular Canines: A CBCT Study. Orthod. Craniofac. Res. 2015, 18, 156–164. [Google Scholar] [CrossRef]
- Krasny, M.; Krasny, K.; Wojtowicz, A. En Bloc Autotransplantation of Retained Canine in the Mandible: A Case Presentation. Int. J. Periodontics Restor. Dent. 2020, 40, 403–407. [Google Scholar] [CrossRef]
- Aras, M.; Halicioglu, K.; Yavuz, M.; Caglaroglu, M. Evaluation of Surgical-Orthodontic Treatments on Impacted Mandibular Canines. Med. Oral 2011, e925–e928. [Google Scholar] [CrossRef] [Green Version]
- Paolone, M.G.; Kaitsas, R.; Paolone, G.; Kaitsas, V. Lingual Orthodontics and Forced Eruption: A Means for Osseous and Tissue Regeneration. Prog. Orthod. 2008, 9, 46–57. [Google Scholar] [PubMed]
- Kaitsas, R.; Paolone, M.G.; Paolone, G. Guided Orthodontic Regeneration: A Tool to Enhance Conventional Regenerative Techniques in Implant Surgery. Int. Orthod. 2015, 13, 539–554. [Google Scholar] [CrossRef] [PubMed]
- Crescini, A.; Nieri, M.; Buti, J.; Baccetti, T.; Mauro, S.; Pini Prato, G.P. Short- and Long-Term Periodontal Evaluation of Impacted Canines Treated with a Closed Surgical? Orthodontic Approach. J. Clin. Periodontol. 2007, 34, 232–242. [Google Scholar] [CrossRef] [PubMed]
- Chaushu, S.; Becker, A.; Zeltser, R.; Branski, S.; Vasker, N.; Chaushu, G. Patients Perception of Recovery after Exposure of Impacted Teeth: A Comparison of Closed- versus Open-Eruption Techniques. J. Oral Maxillofac. Surg. 2005, 63, 323–329. [Google Scholar] [CrossRef]
- Malcangi, G.; Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Garibaldi, M.; Inchingolo, A.M.; Piras, F.; Cardarelli, F.; Settanni, V.; et al. Impacted Central Incisors in the Upper Jaw in an Adolescent Patient: Orthodontic-Surgical Treatment—A Case Report. Appl. Sci. 2022, 12, 2657. [Google Scholar] [CrossRef]
- Özer, M.; Şener, I.; Bayram, M. Bilaterally Impacted Maxillary Central Incisors: Surgical Exposure and Orthodontic Treatment: A Case Report. J. Contemp. Dent. Pract. 2006, 7, 98–105. [Google Scholar] [CrossRef] [Green Version]
- Chaushu, S.; Zilberman, Y.; Becker, A. Maxillary Incisor Impaction and Its Relationship to Canine Displacement. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 144–150, discussion 150. [Google Scholar] [CrossRef]
- Han, L.; Mei, L.; Zhang, C.; Wu, T.; Wang, C. Correction of Class II Division 2 with Crowding and Bilateral Fully Transposed Impacted Mandibular Canines. Australas. Orthod. J. 2022, 38, 29–40. [Google Scholar] [CrossRef]
- Bishara, S.E.; Ortho, D. Impacted Maxitlary Canines: A Review. Am. J. Orthod. Dentofac. Orthop. 1992, 13, 159–171. [Google Scholar] [CrossRef]
- Boyd, R.L. Clinical Assessment of Injuries in Orthodontic Movement of Impacted Teeth. II. Surgical Recommendations. Am. J. Orthod. 1984, 86, 407–418. [Google Scholar] [CrossRef]
- Vermette, M.E.; Kokich, V.G.; Kennedy, D.B. Uncovering Labially Impacted Teeth: Apically Positioned Flap and Closed-Eruption Techniques. Angle Orthod. 1995, 65, 23–32, discussion 33. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).