
Comparison of Functional Connectivity Analysis Methods in Alzheimer’s Disease


Abstract
:1. Introduction
1.1. Model/Seed Based Methods
1.2. Data Driven Methods
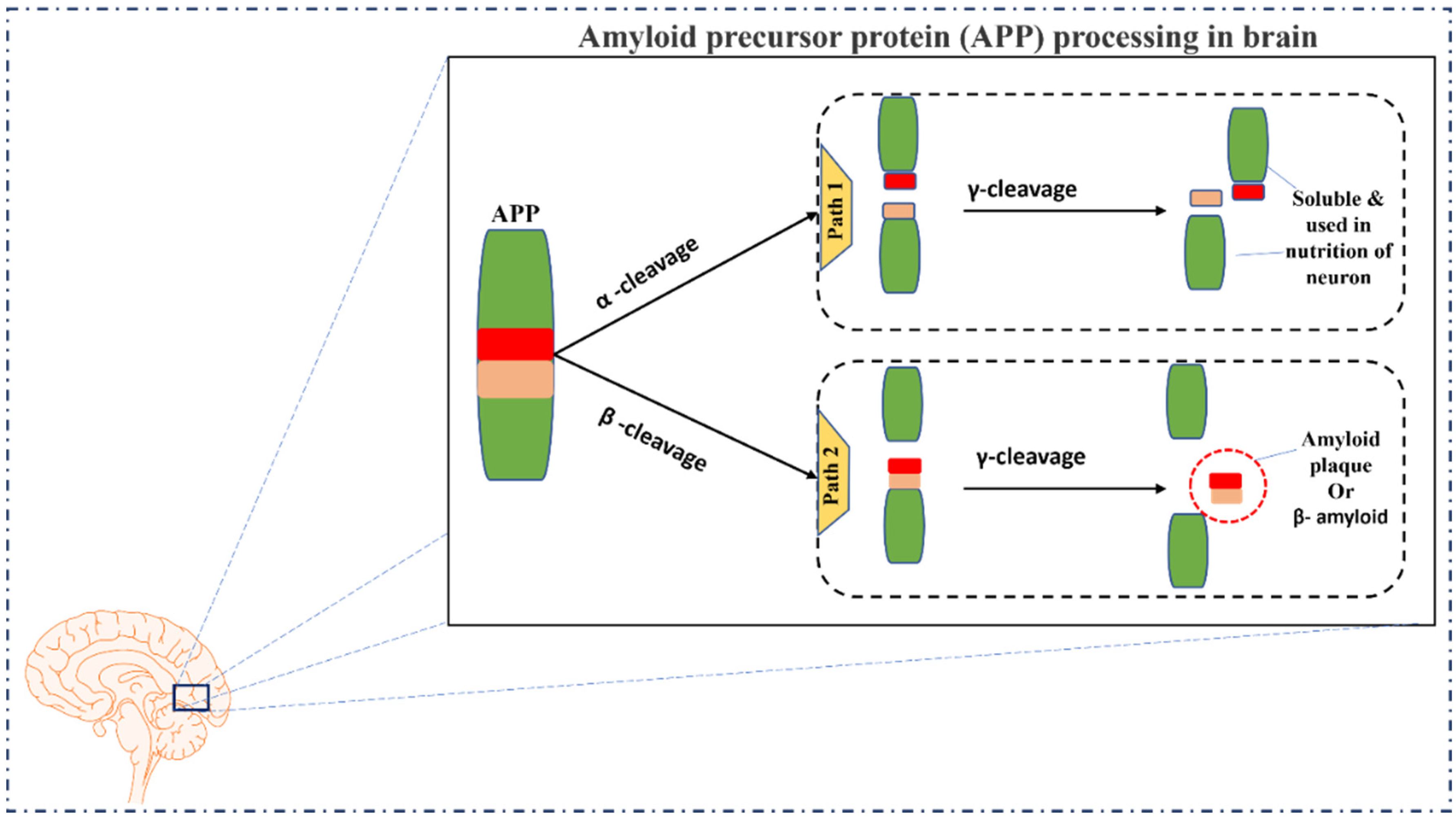
2. The Pathophysiology of Alzheimer’s Disease
3. Functional Connectivity Analysis Methods
3.1. Model/Seed Based Methods
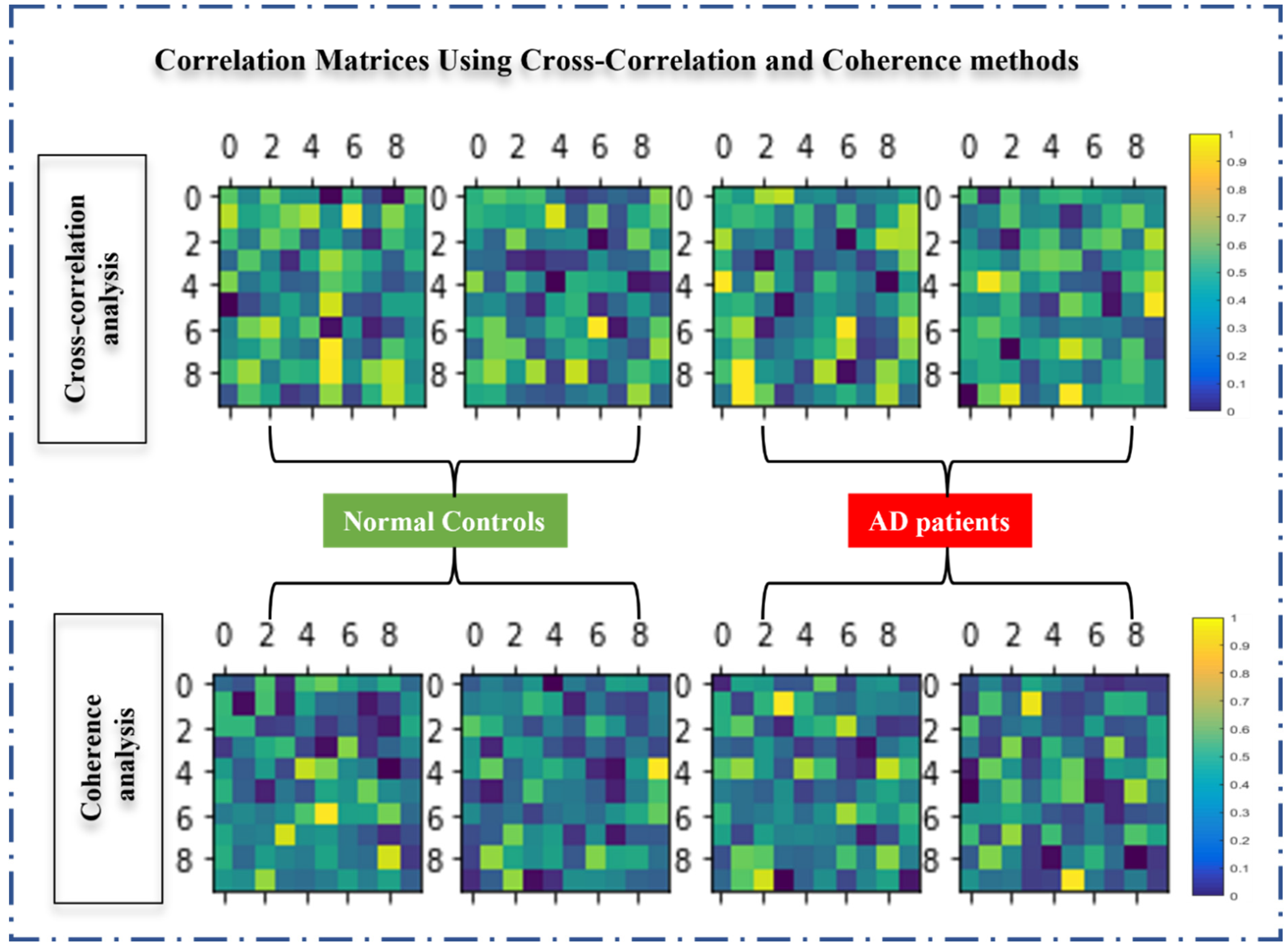
3.1.1. Cross-Correlation Analysis (CCA)
3.1.2. Coherence Analysis (CA)
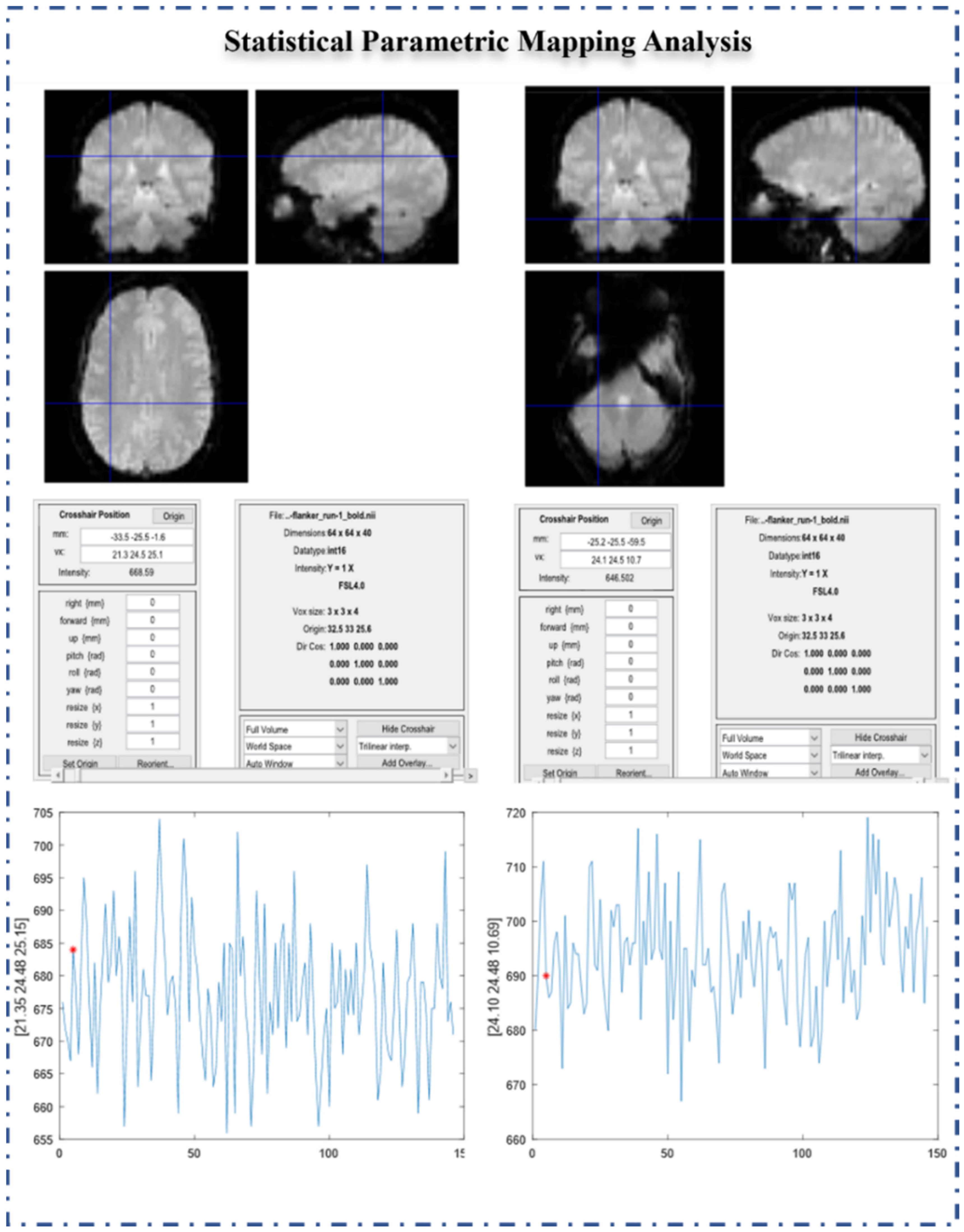
3.1.3. Statistical Parametric Mapping (SPM)
3.2. Data-Driven Methods
3.2.1. Principal Component Analysis (PCA)
3.2.2. Independent Components Analysis (ICA)
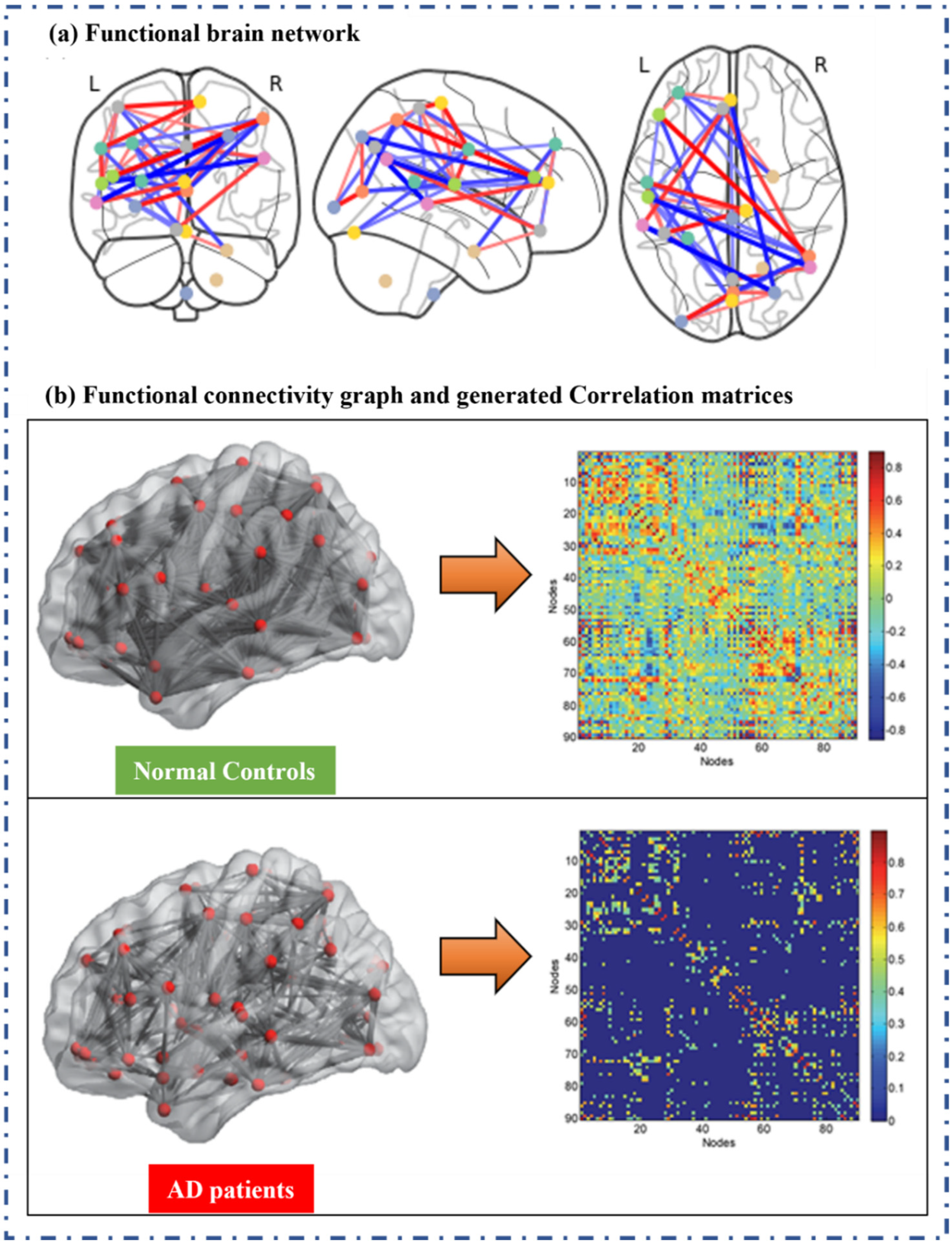
3.2.3. Graph Theory based Method (GT)
3.2.4. Machine Learning-Based Methods
4. Challenges and Limitations
5. Concluding Remarks
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sun, J.; Wang, B.; Niu, Y.; Tan, Y.; Fan, C.; Zhang, N.; Xue, J.; Wei, J.; Xiang, J. Complexity analysis of EEG, MEG, and fMRI in mild cognitive impairment and Alzheimer’s disease: A review. Entropy 2020, 22, 239. [Google Scholar] [CrossRef] [PubMed]
- Biswal, B.; Yetkin, F.Z.; Haughton, V.M.; Hyde, J.S. F1000Prime recommendation of: Functional connectivity in the motor cortex of resting human brain using echo-planar MRI. Magn. Reson. Med. 2012, 34, 537–541. [Google Scholar] [CrossRef] [PubMed]
- Chételat, G. Multimodal Neuroimaging in Alzheimer’s Disease: Early Diagnosis, Physiopathological Mechanisms, and Impact of Lifestyle. J. Alzheimer’s Dis. 2018, 64, S199–S211. [Google Scholar] [CrossRef] [PubMed]
- Farahani, F.V.; Karwowski, W. Computational methods for analyzing functional and effective brain network connectivity using fMRI. In Proceedings of the International Conference on Applied Human Factors and Ergonomics, Orlando, FL, USA, 21–25 July 2018; Springer: Cham, Switzerland, 2018; Volume 775, pp. 101–112. [Google Scholar]
- Margulies, D.S.; Kelly, A.M.C.; Uddin, L.Q.; Biswal, B.B.; Castellanos, F.X.; Milham, M.P. Mapping the functional connectivity of anterior cingulate cortex. Neuroimage 2007, 37, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Iraji, A.; Calhoun, V.D.; Wiseman, N.M.; Davoodi-Bojd, E.; Avanaki, M.R.N.; Haacke, E.M.; Kou, Z. The connectivity domain: Analyzing resting state fMRI data using feature-based data-driven and model-based methods. Neuroimage 2016, 134, 494–507. [Google Scholar] [CrossRef] [PubMed]
- Fox, M.D.; Raichle, M.E. Spontaneous fluctuations in brain activity observed with functional magnetic resonance imaging. Nat. Rev. Neurosci. 2007, 8, 700–711. [Google Scholar] [CrossRef]
- Wu, J.T.; Wu, H.Z.; Yan, C.G.; Chen, W.X.; Zhang, H.Y.; He, Y.; Yang, H.S. Aging-related changes in the default mode network and its anti-correlated networks: A resting-state fMRI study. Neurosci. Lett. 2011, 504, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Jiang, T.; Liang, M.; Wang, L.; Tian, L.; Zhang, X.; Li, K.; Liu, Z. Discriminative analysis of early alzheimer’s disease based on two intrinsically anti-correlated networks with resting-state fMRI. Lect. Notes Comput. Sci. (Incl. Subser. Lect. Notes Artif. Intell. Lect. Notes Bioinform.) 2006, 4191 LNCS, 340–347. [Google Scholar] [CrossRef]
- Allen, G.; Barnard, H.; McColl, R.; Hester, A.L.; Fields, J.A.; Weiner, M.F.; Ringe, W.K.; Lipton, A.M.; Brooker, M.; McDonald, E.; et al. Reduced hippocampal functional connectivity in Alzheimer disease. Arch. Neurol. 2007, 64, 1482–1487. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Guo, L.; Nie, J.; Li, G.; Liu, T. Review of methods for functional brain connectivity detection using fMRI. Comput. Med. Imaging Graph. 2009, 33, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Beckmann, C.F.; DeLuca, M.; Devlin, J.T.; Smith, S.M. Investigations into resting-state connectivity using independent component analysis. Philos. Trans. R. Soc. B Biol. Sci. 2005, 360, 1001–1013. [Google Scholar] [CrossRef] [PubMed]
- Koch, W.; Teipel, S.; Mueller, S.; Buerger, K.; Bokde, A.L.W.; Hampel, H.; Coates, U.; Reiser, M.; Meindl, T. Effects of aging on default mode network activity in resting state fMRI: Does the method of analysis matter? Neuroimage 2010, 51, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Binnewijzend, M.A.A.; Schoonheim, M.M.; Sanz-Arigita, E.; Wink, A.M.; van der Flier, W.M.; Tolboom, N.; Adriaanse, S.M.; Damoiseaux, J.S.; Scheltens, P.; van Berckel, B.N.M.; et al. Resting-state fMRI changes in Alzheimer’s disease and mild cognitive impairment. Neurobiol. Aging 2012, 33, 2018–2028. [Google Scholar] [CrossRef] [PubMed]
- Yu, Q.; Du, Y.; Chen, J.; Sui, J.; Adali, T.; Pearlson, G.D.; Calhoun, V.D. Application of Graph Theory to Assess Static and Dynamic Brain Connectivity: Approaches for Building Brain Graphs. Proc. IEEE 2018, 106, 886–906. [Google Scholar] [CrossRef] [PubMed]
- Meunier, D.; Lambiotte, R.; Fornito, A.; Ersche, K.D.; Bullmore, E.T. Hierarchical modularity in human brain functional networks. Front. Neuroinform. 2009, 3, 37. [Google Scholar] [CrossRef] [PubMed]
- Stelzmann, R.A.; Norman Schnitzlein, H.; Reed Murtagh, F. An english translation of alzheimer’s 1907 paper, “über eine eigenartige erkankung der hirnrinde”. Clin. Anat. 1995, 8, 429–431. [Google Scholar] [CrossRef]
- Hippius, H.; Neundörfer, G. The discovery of Alzheimer’s disease. Dialogues Clin. Neurosci. 2003, 5, 101. [Google Scholar] [CrossRef]
- Kraepelin, E. Vol I: Allgemeine Psychiatrie; Vol II: Klinische Psychiatrie. In Psychiatrie, 8th ed.; Barth: Leipzig, Germany, 1910. [Google Scholar]
- Kim, Y.B. Comparison of Data-Driven Analysis Methods for Identification of Functional Connectivity in fMRI; Massachusetts Institute of Technology: Cambridge, MA, USA, 2005. [Google Scholar]
- Cao, J.; Worsley, K. The geometry of correlation fields with an application to functional connectivity of the brain. Ann. Appl. Probab. 1999, 9, 1021–1057. [Google Scholar] [CrossRef]
- Hyde, J.S.; Jesmanowicz, A. Cross-correlation: An fMRI signal-processing strategy. Neuroimage 2012, 62, 848–851. [Google Scholar] [CrossRef]
- Smirnova, E. Statistical Analysis of Large Cross-Covariance and Cross-Correlation Matrices Produced by fMRI Images. J. Biom. Biostat. 2013, 5, 1–8. [Google Scholar] [CrossRef]
- Cecchi, G.A.; Rao, A.R.; Centeno, M.V.; Baliki, M.; Apkarian, A.V.; Chialvo, D.R. Identifying directed links in large scale functional networks: Application to brain fMRI. BMC Cell Biol. 2007, 8, S5. [Google Scholar] [CrossRef] [PubMed]
- Miezin, F.M.; Maccotta, L.; Ollinger, J.M.; Petersen, S.E.; Buckner, R.L. Characterizing the hemodynamic response: Effects of presentation rate, sampling procedure, and the possibility of ordering brain activity based on relative timing. Neuroimage 2000, 11, 735–759. [Google Scholar] [CrossRef] [PubMed]
- Sun, F.T.; Miller, L.M.; D’Esposito, M. Measuring interregional functional connectivity using coherence and partial coherence analyses of fMRI data. Neuroimage 2004, 21, 647–658. [Google Scholar] [CrossRef] [PubMed]
- Poldrack, R.A. Region of interest analysis for fMRI. Soc. Cogn. Affect. Neurosci. 2007, 2, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Jack, C.R.; Bernstein, M.A.; Fox, N.C.; Thompson, P.; Alexander, G.; Harvey, D.; Borowski, B.; Britson, P.J.; Whitwell, J.L.; Ward, C.; et al. The Alzheimer’s Disease Neuroimaging Initiative (ADNI): MRI methods. J. Magn. Reson. Imaging 2008, 27, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Du, Y.H.; Ding, X.T.; Wang, X.H.; Men, G.Z. Alteration of functional connectivity in patients with Alzheimer’s disease revealed by resting-state functional magnetic resonance imaging. Neural Regen. Res. 2020, 15, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Flandin, G.; Novak, M.J.U. fMRI Data Analysis Using SPM. In fMRI; Springer International Publishing: New York, NY, USA, 2020; pp. 89–116. [Google Scholar]
- Statistical Parametric Mapping—File Exchange—MATLAB Central. Available online: https://www.mathworks.com/matlabcentral/fileexchange/68729-statistical-parametric-mapping?s_tid=srchtitle (accessed on 1 July 2021).
- Thomas Yeo, B.T.; Krienen, F.M.; Sepulcre, J.; Sabuncu, M.R.; Lashkari, D.; Hollinshead, M.; Roffman, J.L.; Smoller, J.W.; Zöllei, L.; Polimeni, J.R.; et al. The organization of the human cerebral cortex estimated by intrinsic functional connectivity. J. Neurophysiol. 2011, 106, 1125–1165. [Google Scholar] [CrossRef]
- Wang, S.; Simon, B.P.; Bennett, D.A.; Schneider, J.A.; Malter, J.S.; Wang, D.S. The significance of Pin1 in the development of Alzheimer’s disease. J. Alzheimer’s Dis. 2007, 11, 13–23. [Google Scholar] [CrossRef]
- Amico, E.; Goñi, J. The quest for identifiability in human functional connectomes. Sci. Rep. 2018, 8, 8254. [Google Scholar] [CrossRef]
- Sorg, C.; Riedl, V.; Mühlau, M.; Calhoun, V.D.; Eichele, T.; Läer, L.; Drzezga, A.; Förstl, H.; Kurz, A.; Zimmer, C.; et al. Selective changes of resting-state networks in individuals at risk for Alzheimer’s disease. Proc. Natl. Acad. Sci. USA 2007, 104, 18760–18765. [Google Scholar] [CrossRef]
- Greicius, M.D.; Krasnow, B.; Reiss, A.L.; Menon, V. Functional connectivity in the resting brain: A network analysis of the default mode hypothesis. Proc. Natl. Acad. Sci. USA 2003, 100, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Li, R.; Fleisher, A.S.; Reiman, E.M.; Guan, X.; Zhang, Y.; Chen, K.; Yao, L. Altered default mode network connectivity in Alzheimer’s disease-A resting functional MRI and Bayesian network study. Hum. Brain Mapp. 2011, 32, 1868–1881. [Google Scholar] [CrossRef] [PubMed]
- Khoo, H.M.; Kishima, H.; Tani, N.; Oshino, S.; Maruo, T.; Hosomi, K.; Yanagisawa, T.; Kazui, H.; Watanabe, Y.; Shimokawa, T.; et al. Default mode network connectivity in patients with idiopathic normal pressure hydrocephalus. J. Neurosurg. 2016, 124, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Grieder, M.; Wang, D.J.J.; Dierks, T.; Wahlund, L.O.; Jann, K. Default Mode Network Complexity and Cognitive Decline in Mild Alzheimer’s Disease. Front. Neurosci. 2018, 12, 770. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.O.; Adali, T.; Calhoun, V.D. Estimating the number of independent components for functional magnetic resonance imaging data. Hum. Brain Mapp. 2007, 28, 1251–1266. [Google Scholar] [CrossRef] [PubMed]
- Supekar, K.; Menon, V.; Rubin, D.; Musen, M.; Greicius, M.D. Network analysis of intrinsic functional brain connectivity in Alzheimer’s disease. PLoS Comput. Biol. 2008, 4, e1000100. [Google Scholar] [CrossRef]
- Buckner, R.L.; Sepulcre, J.; Talukdar, T.; Krienen, F.M.; Liu, H.; Hedden, T.; Andrews-Hanna, J.R.; Sperling, R.A.; Johnson, K.A. Cortical hubs revealed by intrinsic functional connectivity: Mapping, assessment of stability, and relation to Alzheimer’s disease. J. Neurosci. 2009, 29, 1860–1873. [Google Scholar] [CrossRef]
- Du, Y.; Fu, Z.; Calhoun, V.D. Classification and prediction of brain disorders using functional connectivity: Promising but challenging. Front. Neurosci. 2018, 12, 525. [Google Scholar] [CrossRef]
- Shi, Y.; Zeng, W.; Deng, J.; Nie, W.; Zhang, Y. The Identification of Alzheimer’s Disease Using Functional Connectivity between Activity Voxels in Resting-State fMRI Data. IEEE J. Transl. Eng. Health Med. 2020, 8, 1–11. [Google Scholar] [CrossRef]
- Khazaee, A.; Ebrahimzadeh, A.; Babajani-Feremi, A. Application of advanced machine learning methods on resting-state fMRI network for identification of mild cognitive impairment and Alzheimer’s disease. Brain Imaging Behav. 2016, 10, 799–817. [Google Scholar] [CrossRef]
- Vidaurre, D.; Smith, S.M.; Woolrich, M.W. Brain network dynamics are hierarchically organized in time. Proc. Natl. Acad. Sci. USA 2017, 114, 12827–12832. [Google Scholar] [CrossRef] [PubMed]
- Dongiovanni, D.; Vaina, L.M. Select and Cluster: A Method for Finding Functional Networks of Clustered Voxels in fMRI. Comput. Intell. Neurosci. 2016, 2016, 4705162. [Google Scholar] [CrossRef] [PubMed]
- Dennis, E.L.; Thompson, P.M. Functional brain connectivity using fMRI in aging and Alzheimer’s disease. Neuropsychol. Rev. 2014, 24, 49–62. [Google Scholar] [CrossRef] [PubMed]
- Khosla, M.; Jamison, K.; Ngo, G.H.; Kuceyeski, A.; Sabuncu, M.R. Machine learning in resting-state fMRI analysis. Magn. Reson. Imaging 2019, 64, 101–121. [Google Scholar] [CrossRef]
- Fox, M.D.; Greicius, M. Clinical applications of resting state functional connectivity. Front. Syst. Neurosci. 2010, 4, 19. [Google Scholar] [CrossRef]
- Takamura, T.; Hanakawa, T. Clinical utility of resting-state functional connectivity magnetic resonance imaging for mood and cognitive disorders. J. Neural Transm. 2017, 124, 821–839. [Google Scholar] [CrossRef]
- Moreno-Dominguez, D.; Anwander, A.; Knösche, T.R. A hierarchical method for whole-brain connectivity-based parcellation. Hum. Brain Mapp. 2014, 35, 5000–5025. [Google Scholar] [CrossRef]
- Schoffelen, J.M.; Gross, J. Source connectivity analysis with MEG and EEG. Hum. Brain Mapp. 2009, 30, 1857–1865. [Google Scholar] [CrossRef]
- Power, J.D.; Fair, D.A.; Schlaggar, B.L.; Petersen, S.E. The development of Human Functional Brain Networks. Neuron 2010, 67, 735. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | NC (30 Total) | AD (29 Total) |
|---|---|---|
| 74.20 ± 5.96 | 72.01 ± 7.26 | |
| Sex(M/F) | 11/19 | 11/18 |
| 28.9 ± 1.7 | 21.0 ± 3.5 | |
| 0.14 ± 0.44 | 15 ± 7.47 | |
| 0 | 0.84 ± 0.23 |
| ML-Based Method | Conceptual Explanation and Limitations |
|---|---|
Supervised Learning:
|
|
Unsupervised Learning:
|
|
| Method Name | Challenges and Limitations |
|---|---|
| CCA | The hemodynamic response function (HRF) differs between subjects and even between brain areas within the same subject due to the full-lag space of blood’s hemodynamic response, which makes CCA unnecessary. It would be computationally expensive to calculate cross-correlation at all lags. To overcome this problem, many researchers compute correlation with zero lag. |
| CA | The low spatial and temporal resolution limits the analysis of FC using CA. The distribution of the electric current over the surface of the skull can be inaccurate, which is one of the challenges with this traditional method of mapping coherence in sensor space [53]. The exact amplitudes of the connections are not equivalent to region-to-region coherence amplitudes; therefore, the directionality of the network interaction cannot be identified by only considering coherence. Apart from this limitation, coherence provides a global assessment of all critical regions of network activity irrespective of source amplitudes, making it unsuitable for assessing rapid temporal changes in synchronized activity. |
| SPM | The model/seed-based method allows one to concentrate just on brain regions associated with prior knowledge while neglecting other brain sections or functions. As a result, complete brain exploration is beyond the scope of this method. It may necessitate data-driven approaches such as decomposition analysis and clustering analysis. |
| PCA | The challenge of determining the dimensionality of the primary space upon which we project the original data, or the number of principal components, remains unsolved. Initially, PCA was applied to fMRI datasets in several studies and helped the researcher explore helpful information related to FC. However, for lower contrast to noise ratio, PCA shows poor performance. |
| ICA | Although the ICA method for FC research is becoming increasingly popular, particularly with resting-state fMRI data, several problems need to be noted. Firstly, ICA is based on the premise that components (signal sources) are independent of one another, whether geographically or temporally. Violation of this premise would significantly reduce ICA’s efficacy. Second, the topic of how to select the number of independent components and how to threshold the IC maps remain unclear. |
| GT | Graph theory gives valuable information on the development of functional neural networks. However, it has limitations that need to be addressed. In graph theory research, conclusions can be reached when nodes are well defined as voxels or regions of interest. Node definition is quite tricky in developmental research since the nodes are likely to be identical across various subjects or sessions. Hence graphs may be considerably distorted [54]. As a result, employing graph theory necessitates a careful approach to node selection and a piece of knowledge that constructed graphs are only reliable when nodes are adequately defined. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chauhan, N.; Choi, B.-J. Comparison of Functional Connectivity Analysis Methods in Alzheimer’s Disease. Appl. Sci. 2022, 12, 8096. https://doi.org/10.3390/app12168096
Chauhan N, Choi B-J. Comparison of Functional Connectivity Analysis Methods in Alzheimer’s Disease. Applied Sciences. 2022; 12(16):8096. https://doi.org/10.3390/app12168096
Chicago/Turabian StyleChauhan, Nishant, and Byung-Jae Choi. 2022. "Comparison of Functional Connectivity Analysis Methods in Alzheimer’s Disease" Applied Sciences 12, no. 16: 8096. https://doi.org/10.3390/app12168096
APA StyleChauhan, N., & Choi, B.-J. (2022). Comparison of Functional Connectivity Analysis Methods in Alzheimer’s Disease. Applied Sciences, 12(16), 8096. https://doi.org/10.3390/app12168096