Abstract
The modified goniometric platform (MGP) is a novel instrument used to measure trunk rotation while sitting. A lack of reliable and valid evidence has been reported to measure trunk rotation using MGP. Therefore, this study was aimed to investigate the intra- and inter-rater reliabilities and validity of the MGP for measuring trunk rotation while sitting. Methods: Seventeen participants performed right trunk rotation followed by left trunk rotation (three repetitions for each trial) and two random measurements at 40-minute intervals. Inter-rater and intra-rater reliabilities were calculated using intraclass correlation coefficients (ICCs). Validity was assessed using the Pearson correlation coefficient (r). Results: The test and re-test inter-rater reliabilities for right trunk rotation were 0.990 and 0.986, respectively, and those for left trunk rotation were 0.989 and 0.978, respectively. The intra-rater reliabilities for right trunk rotation were 0.949 and 0.954, respectively, and those for left trunk rotation were 0.944 and 0.946, respectively. The right and left trunk rotation validities were 0.986 and 0.981, respectively. Conclusion: MGP is reliable and valid for measuring right and left trunk rotations while sitting.
1. Introduction
Trunk rotation occurs frequently and plays a vital role in people’s daily activities. The restriction of trunk rotation is one of lower back pain’s symptoms [1,2,3]. A lower back pain patient is prescribed various trunk rotation exercises for pain release. Trunk rotation is also clinically used to evaluate and monitor the progression of trunk function recovered from malfunction, injury or surgery [4]. Inadequate trunk rotation may result in movement compensation while performing sport-specific techniques such as overhead throws during pitching in baseball [5,6]. Restricted trunk rotation forces external shoulder rotation to a greater-than-usual extent. The overloaded shoulder joint is then exposed to higher injury risks. In addition, restricted trunk rotation is also associated with lower limb injuries. Deficits in trunk rotation increase the internal knee varus moment and excessive force loading on the knee joints, and they may increase the risk of anterior cruciate ligament injury [7]. Based on the presented knowledge, trunk rotation is an important parameter associated with movement function and injuries. Therefore, there is an emerging interest in establishing the right instrument for trunk rotation measurements.
Though trunk rotation is a complex movement that involves thoracic and lumbar vertebrae in the transverse plane, the trunk rotation angle has been inconsistently defined in the literature. A commonly accepted definition is the cross angle between the line of both anterior superior iliac crests and the line of both shoulders’ acromion joints [8]. Another common definition is that the trunk rotation angle is measured by the angle changes of the line from the first thoracic vertebrae (T1) to the upper edge of the sacrum [4]. Three-dimensional (3D) motion analysis systems, three-dimensional magnetic resonance imaging (3D-MRI), two-dimensional video analysis, inclinometers, and goniometers have been developed to measure trunk rotation in different positions based on different definitions of trunk rotation. As a result, various protocols have been used to measure trunk rotation in different positions, such as upright standing, trunk flexion, sitting, and prone lying [5,9,10,11]. However, due to its structural complexity, there is no standard method for measuring trunk rotation.
3D motion analysis and 3D-MRI are costly instruments that require specific space and professional skill requirements [9,12]. Although these two devices are accurate, they are not the first considerations for measuring trunk rotation due to their complexity and price. Two-dimensional (2D) video analysis is a reliable and valid tool for measuring trunk rotation in the transverse plane. However, this device is relatively expensive, and moderate skill is required due to the additional matched software needed to analyse its data [13]. In contrast, goniometers and inclinometers are the least expensive instruments [14]. In a previous study, double inclinometers were separately placed onto the spinous process of the seventh cervical vertebra and sacral vertebra to measure trunk rotation in the standing position with a 90-degree trunk flexion. This position is challenging for a person with poor balance control [15]. A goniometer is a convenient portable device, but there are challenges associated with positioning and controlling the dynamic and fixed arms and identifying bony landmarks for users [16]. Thus, a more straightforward, portable, and inexpensive device for measuring trunk rotation is needed.
The goniometric platform, as a novel tool, is easy-to-use and low-cost equipment used to assess trunk rotation in the sitting position, and it was initially used by Sarioglu et al. [17]. Although the goniometric platform has good-to-excellent reliability for measuring right (α = 0.80) and left (α = 0.96) trunk rotations, its validity has not been confirmed [17]. In addition, the previous goniometric platform did not sufficiently consider ergonomic effects. Participants reported that the goniometric platform restricted their ability to perform maximum trunk rotation because of the distance between the table and the seat, indicating the need for further improvements to the platform [17]. Thus, the reliability and validity of the modified goniometric platform to measure trunk rotation in the sitting position required further investigation.
2. Materials and Methods
2.1. Participants
Seventeen healthy volunteer participants were recruited from the National Sports Institute of Malaysia (ISN) via convenient sampling (8 males: height of 171.67 ± 3.92 cm and weight of 78.93 ± 9.23 kg; 9 females: height of 157.12 ± 5.9 cm and weight of 54.48 ± 8.67 kg; age, from 20 to 47 years (27.71 ± 7.78)). The participants were excluded if they had (1) a history of fracture or traumatic injuries of the spine and upper limbs, (2) a history of orthopaedic surgery in the upper body, (3) any other orthopaedic or neurological problems in the upper body, or (4) complaints of pain around upper body. Each participant was randomly tested in two identical sessions that were at least 40 min apart. All participants voluntarily signed an informed consent form before formal enrolment in this study. Participants’ daily activities were not restricted during the interval test.
2.2. Sample Size
The sample size was calculated based on the fixed n = 3 (number of measurements), ρ0 = 0.7 (above 0.7 would be considered acceptable), ρ1 = 0.80 (above 0.8 would be considered good), α = 0.05, and β = 0.8 in this study. The sample size range was set from 12.8 (13) to 79.7 (80), following a previous study [18]. Therefore, the current study met the minimum sample size requirement.
2.3. Instruments
2.3.1. The Modified Goniometric Platform
The modified goniometric platform (MGP) with a size of 100 × 70 cm (length × width), comprising a plastic board with a dug-out semicircle with a 23 cm radius from the centre of the MGP, was placed on a rectangular table. Angles of 0° and 180° on the MGP were parallel to the table’s edge and the ground. The MGP was fixed on a table to avoid movement during the testing. The minimum unit of the MGP interval was 2°.
2.3.2. Two-Dimension Video Analyses
A video camera (Panasonic HDC-HS 900, Osaka, Japan) was set perpendicular to the ground on top of the squat rack (PR4000, height of 201 cm, and width of 112 cm) at a recording speed of 50 fps. The camera’s aperture covered the entire test scene, including each participant’s maximum left and right trunk rotation, the extension of both arms and hands at different angles, and the table and goniometric platform. The footage of the trunk rotation trials was further coded and analysed by an experienced video analyst (r = 0.94) using 2D video analyses and video tracking software (Dartfish, version:10 classic, Fribourg, Switzerland). The minimum unit of the 2D video analysis interval was 0.1°.
2.4. Data Collection
2.4.1. Initial Position
Participants were instructed to sit upright on a 50 cm tall wooden box with their head in a neutral position, chin tucked in, a hip–knee flexion angle of approximately 90° with a foam roller between the knees and feet flat on the ground and shoulder-width apart, and arms positioned straight ahead with fingers crossed together. Participants held an L-shaped tube perpendicular to the MGP, which served as a reading indicator. Participants sat in the middle of the fixed MGP with their frontal axis near a line that indicated angles of 0° and 180° and the sagittal axis close to the 90° angle of the MGP. The midline of both extended arms while holding the tube was at a 90° angle to the MGP in respect to the initial position (Figure 1).

Figure 1.
Initial position of each participant.
2.4.2. Familiarisation and Testing
Each participant practised three left and right trunk rotation trials before formally testing. Each participant started at the initial position and maximally rotated their trunk to the right, followed by maximum left trunk rotation. Verbal cues of “keep the trunk upright”, “no elevation of the shoulder”, “straight arms”, “hold L-shape tube vertically”, “head to follow the hand rotation”, and “no lifting the pelvis” were given during the trunk rotation tests. Each participant was asked to maintained approximately 3 s of right and left maximum trunk rotation, with three repetitions, and a physiotherapist (rater 1) and a sports science undergraduate student (rater 2) simultaneously recorded the MGP value. Meanwhile, the researcher (rater 1) pressed the light-voice synchronised sensor button to indicate scale reading for further 2D video analysis. In the 2D video analysis, the goniometer axis was located between the horizontal line (0° and 180°) and the 90° perpendicular line. The fixed arm of the goniometer was placed at the 90° mark of the MGP, and the dynamic arm was placed at the end-stop point of the L-shaped tube. The movement of the dynamic arm of the goniometer relative to its fixed arm was measured as the right or left trunk rotation angle (Figure 2). All participants were present for the test and re-test sessions, which were randomly performed.
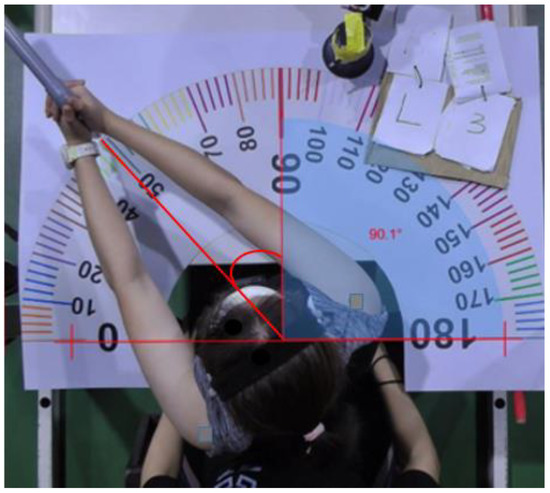
Figure 2.
Two-dimensional video analysis for the measurement of trunk rotation.
2.5. Statistical Analysis
All quantitative data in this study were analysed using version 22 of SPSS statistical software (IBM, Chicago, IL, USA). Demographic data are presented as the mean and standard deviation (mean ± SD). Intraclass correlation coefficients (ICCs) and 95% confidence intervals (CIs) were computed to determine inter-rater and intra-rater reliability measurements. Inter-rater reliability was based on ratings (k = 2), absolute agreement, and a 2-way mixed-effects model. The intra-rater reliability was based on mean ratings (k = 1), absolute agreement, and a 2-way mixed-effects model [19]. The reliability of an instrument is poor if its value is less than 0.5, moderate if the value is from 0.5 to 0.75, good if the value is from 0.75 to 0.9, and excellent if the value is greater than 0.90 [19]. The validity of the two instruments was based on the rater rating (k = 1), absolute agreement, and a 2-way mixed-effects model. The Pearson correlation coefficient (r) was calculated from the MGP and 2D video analysis data to establish the validity of the ICC values. In validity evaluation, a value of less than 0.1 is considered negligible, a value from 0.10 to 0.39 is considered weak, a value from 0.40 to 0.69 indicates a moderate correlation, a value from 0.70 to 0.89 indicate correlation, and a value from 0.90 to 1.00 indicates a very strong correlation [20]. The standard error of measurement (SEM) and minimal detectable changes (MDC) were calculated by referring to the work of Ries et al. [21]. A Bland–Altman plot analysis was used to describe the mean differences and 95% limits of agreement between the MGP and 2D video analyses [22].
3. Results
3.1. Inter-Rater Reliability
In the test session, the inter-rater reliabilities, as indicated by the ICCs, were 0.990 (95% CI, 0.982–0.993; p < 0.001) and 0.989 (95% CI, 0.980–0.993; p < 0.001) for right and left trunk rotations, respectively. For the retest session, which was 40 min after the first test, the inter-rater reliabilities for right and left trunk rotations were 0.986 (95% CI, 0.982–0.998; p < 0.001) and 0.978 (95% CI, 0.960–0.998, p < 0.001), respectively. The inter-rater reliability between the two raters was considered to have excellent strength because the ICC values were greater than 0.90 for all sessions (Table 1).

Table 1.
Inter-rater reliability of the MGP for left and right trunk rotations.
3.2. Intra-Rater Reliability
The intra-rater reliabilities of the right and left trunk rotations, as indicated by the ICCs for rater 1, were 0.949 (95% CI, 0.852–0.982; p < 0.001) and 0.944 (95% CI, 0.839–0.980; p < 0.001), respectively. The intra-rater reliabilities of the right and left trunk rotations, as indicated by the ICCs for rater 2, were 0.954 (95% CI, 0.858–0.984; p < 0.001) and 0.946 (95% CI, 0.840–0.981, p < 0.001), respectively. The intra-rater reliability was considered to have good-to-excellent strength (Table 2).
Table 2.
Intra-rater reliability of the two measurements performed by raters.
3.3. Validity
The correlation between the MGP and 2D video analysis for measuring right trunk rotation (r = 0.986) and left trunk rotation (r = 0.981) was significant (p < 0.001), with explained variances of 97.2% and 96.2%, respectively (Table 3). Therefore, there was a strong relationship between the two instruments for measuring trunk rotation. The Bland–Altman plot showed the level of agreement between the two instruments for right trunk rotation measurements, with M = −0.706 ± 1.418 degrees (95% CI: −3.485–2.073) (Figure 3), and left trunk rotation, with M = −1.171 ± 1.814 degrees (95% CI: −4.723–2.384) (Figure 4).The majority of data points were close to the mean difference and within the 95% limits of agreement.
Table 3.
Validity of the MGP and video analysis.
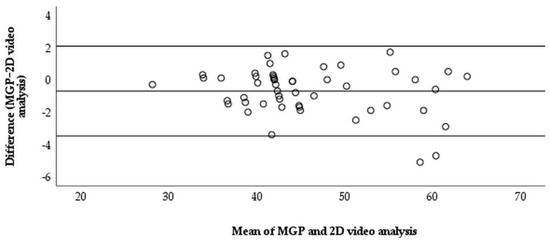
Figure 3.
The modified goniometric platform and video analysis measurement for right trunk rotation.
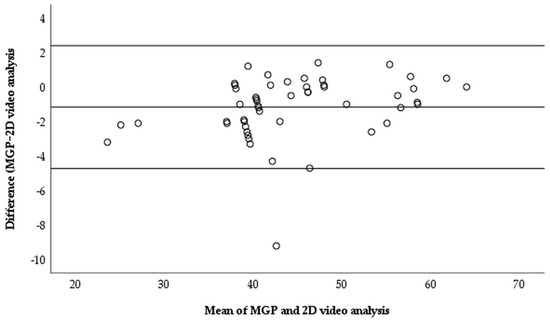
Figure 4.
The modified goniometric platform and video analysis measurement for left trunk rotation.
4. Discussion
This study has demonstrated excellent strength in the inter-rater reliability of the MGP for measuring left and right trunk rotation, with an intra-rater reliability of good-to-excellent strength. The results also showed no significant difference between the MGP and 2D video analyses in measuring the left and right trunk rotations occurring in the transverse plane. Therefore, MGP has strong validity and reliability as an instrument for evaluating trunk rotation in the seated position.
Trunk rotation was reported to have a good-to-excellent inter-rater reliability. The inter-rater coefficients of reliability of a standard 8-inch (20-centimetre) transparent plastic goniometer for measuring right and left trunk rotations in the sitting position were 0.870 (95% CI: 0.770–0.930) and 0.870 (95% CI: 0.760–0.930), respectively, indicating a good inter-rater reliability [23]. The right trunk rotation values measured by two previous raters were 54.4° ± 10.5° and 53.4° ± 11.0°, and those of the left trunk rotation were 53.7° ± 9.0° and 55.3° ± 11.1° [23]. In contrast, the right trunk rotations of the two raters in our study were 45.4° ± 8.2° and 45.3° ± 8.5°, and those of the left trunk rotations were 43.8° ± 9.1° and 46.0° ± 8.6°, which were smaller than previously reported values [23]. The difference between the two sets of findings may be due to two main reasons: age and the test protocol [10]. Healthy swimming athletes who are from 10 to 18 years of age (mean age: 13.52 ± 1.57 years) have excellent trunk rotation, which might be explained by the flexible shoulder joint caused by swimming, which is an open kinetic chain exercise, and their mean right trunk rotation angle range was found to be from 63.5° to 68.4°, which was bigger than our findings [2]. Sung et al. [24] also reported that age could affect the coordination pattern of the trunk and pelvis in the transverse plane, which could explain the smaller trunk rotation angles recorded in our study. In addition, the angle differences may have been caused by the fact that Johnson et al.’s study did not restrict pelvic movement during trunk rotation, as supported by Park et al.’s study [10], who study reported that trunk rotation movement patterns would differ due to age differences and shoulder–pelvic patterns. In our study, the inter-rater reliability of the MGP for trunk rotation (0.989–0.990) was higher than that reported by using other types of goniometers (0.736–0.853), such as bubble inclinometers, dual inclinometers, and smartphone clinometers [25]. Thus, the MGP could be a more reliable instrument for use by trained or even unskilled practitioners.
A good-to-excellent within-day intra-rater reliability of the MGP in measuring trunk rotation at the sitting position was observed in this study. Our results were consistent with those of Furness et al. [26], who showed that the intra-rater reliabilities for the right and left sides were 0.970 and 0.980, respectively. Therefore, the MGP has excellent reproducibility compared to previously reported goniometer measurements. Furthermore, two within-day measurements using the MGP showed a very strong correlation (r > 0.90); this finding is supported by the work of Brouwer et al. [6]. Feijen et al. [2] reported that the intra-rater reliabilities of goniometric measurements for right and left trunk rotations in the lumbar lock rotation position were 0.910 (95% CI, 0.780–0.960) and 0.960 (0.890–0.980), respectively, which were similar to our findings. In conclusion, the seated trunk range of motion was shown to be relatively consistent within a day when measured using the MGP.
This is the first time the MGP was compared against a more precise measurement instrument, 2D video analysis, in quantifying transverse trunk rotation. In a previous study, 2D video analysis was shown strongly correlate with 3D motion capture, which was considered to be the relative standard instrument for measuring trunk rotation (r = 0.810–0.993) [27,28]. Therefore, 2D video analysis is a valid tool for measuring left and right trunk rotations in the transverse plane. The MGP showed a strong correlation with 2D video analysis for evaluating trunk rotations in the transverse plane (0.981–0.986) and is considered a valid instrument. The mean difference between the MGP and 2D video analysis on the right side was 0.706° (95% CI: −3.485°, 2.073°), and that on the left side was 1.171° (95% CI: 4.726°, 2.384°). The right trunk rotation angle was smaller than the left trunk rotation angle, indicating that some of the participants in this cohort may have trunk tightness. Previous studies have reported that trunk tightness reduces the trunk rotation range of motion [29,30]. In addition, the findings of this study were similar to those reported by Bucke et al. [31], who compared a digital goniometer and iPhone Clinometer apps, although they reported a greater variance (12° versus 8°, respectively). The MGP is valid, and it also shows a smaller variance than that observed using other digital goniometers. Therefore, the MGP may have more possibility to be applied in assessing trunk rotation.
The advantage of the MGP is that it is a cost-effective, instantly readable, and portable tool. It is a relatively straightforward tool that can be used by trained individuals with or without in-depth anatomical knowledge. Furthermore, it requires a minimum number of operators to implement the test. With all result in mind, some limitations of this study should be considered. First, the convenient sampling of this study limited its generalizability. Thus, the results are not meant for generalization. Second, the test was repeated randomly within an hour on the same day to control for the thermal effect of physical activity and environmental heat on the range of motion. Thus, the interpretation of these findings should be limited to two observations tested on the same day. In future research, the repeatability of the MGP for measuring trunk rotation between days should be examined.
5. Conclusions
This study demonstrated that the modified goniometric platform is a reliable and valid instrument for measuring trunk rotation in the sitting position. In addition, it could be a quick, easy, and cost-effective instrument used by trained individuals or researchers. Therefore, the modified goniometric platform may have potential for future applications in measuring trunk rotation.
Author Contributions
Conceptualization, J.G. and J.S.T.; methodology, J.G. and J.S.T.; validation, J.G. and J.S.T.; formal analysis, J.G. and J.S.T.; investigation, J.G. and J.S.T.; resources, J.G. and J.S.T.; data curation, J.G. and J.S.T.; writing—original draft preparation, J.G.; writing—review and editing, J.S.T., D.P., S.W., C.S.C., Y.R., A.S.B.M.A. and R.B.M.Y.; supervision, J.S.T., D.P., S.W., C.S.C., Y.R., A.S.B.M.A. and R.B.M.Y.; project administration, J.S.T. and S.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the National Sports Institute of Malaysia (ISNRG No. 008/2021-009/2021).
Institutional Review Board Statement
The study protocol was approved by the National Sports Institute of Malaysia Research Ethics Committee (ISNRE/A/002/2022-009/2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Acknowledgments
The authors would like to thank Nicholas Lim Chin Shyuen and Ku Cai Ni from the Faculty of Applied Sciences, Tunku Abdul Rahman University College, for their assistance with the data collection.
Conflicts of Interest
There are no conflict of interest in this study, and all the authors did not accept financial or non-financial support.
References
- Montgomery, T.; Boocock, M.; Hing, W. The effects of spinal posture and pelvic fixation on trunk rotation range of motion. Clin. Biomech. 2011, 26, 707–712. [Google Scholar] [CrossRef] [PubMed]
- Feijen, S.; Kuppens, K.; Tate, A.; Baert, I.; Struyf, T.; Struyf, F. Intra-and interrater reliability of the ‘lumbar-locked thoracic rotation test’in competitive swimmers ages 10 through 18 years. Phys. Ther. Sport 2018, 32, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Masharawi, Y.; Haj, A.; Weisman, A. Lumbar axial rotation kinematics in an upright sitting and with forward bending positions in men with nonspecific chronic low back pain. Spine 2020, 45, 244–251. [Google Scholar] [CrossRef]
- Getnet, M.G.; Jember, G.; Janakiraman, B. Inter-and intra-observer reliability of scoliogauge app to assess the axial trunk rotation of scoliosis: Prospective reliability analysis study. Int. J. Surg. 2020, 27, 5–9. [Google Scholar] [CrossRef]
- Bullock, G.S.; Strahm, J.; Hulburt, T.C.; Beck, E.C.; Waterman, B.R.; Nicholson, K.F. The Relationship of Range of motion, Hip Shoulder Separation, and Pitching Kinematics. Int. J. Sports Phys. Ther. 2020, 15, 11–19. [Google Scholar]
- Brouwer, N.; Yeung, T.; Bobbert, M.; Besier, T. 3D trunk orientation measured using inertial measurement units during anatomical and dynamic sports motions. Scand. J. Med. Sci. Sports 2021, 31, 358–370. [Google Scholar] [CrossRef]
- Frank, B.; Bell, D.R.; Norcross, M.F.; Blackburn, J.T.; Goerger, B.M.; Padua, D.A. Trunk and hip biomechanics influence anterior cruciate loading mechanisms in physically active participants. Am. J. Sports Med. 2013, 41, 2676–2683. [Google Scholar] [CrossRef]
- Zhang, Z.; Li, S.; Wan, B.; Visentin, P.; Jiang, Q.; Dyck, M.; Li, H.; Shan, G. The influence of X-factor (trunk rotation) and experience on the quality of the badminton forehand smash. J. Hum. Kinet. 2016, 53, 9–22. [Google Scholar] [CrossRef]
- Intolo, P.; Carman, A.B.; Milosavljevic, S.; Abbott, J.H.; Baxter, G.D. The Spineangel®: Examining the validity and reliability of a novel clinical device for monitoring trunk motion. Man. Ther. 2010, 15, 160–166. [Google Scholar] [CrossRef]
- Park, W.H.; Kim, Y.H.; Lee, T.R.; Sung, P.S. Factors affecting shoulder–pelvic integration during axial trunk rotation in subjects with recurrent low back pain. Eur. Spine J. 2012, 21, 1316–1323. [Google Scholar] [CrossRef]
- Jung, S.H.; Ha, S.M.; Kim, J.H.; Gwak, G.T.; Kim, S.J. Reliability of axial-thoracolumbar spine rotation range measurements. J. Mech. Sci. Technol. 2018, 2, 20–23. [Google Scholar] [CrossRef][Green Version]
- Fujimori, T.; Iwasaki, M.; Nagamoto, Y.; Ishii, T.; Kashii, M.; Murase, T.; Yoshikawa, H. Kinematics of the thoracic spine in trunk rotation: In vivo 3-dimensional analysis. Spine 2012, 37, 1318–1328. [Google Scholar] [CrossRef] [PubMed]
- Sung, P.; Park, M. Lumbar spine coordination during axial trunk rotation in adolescents with and without right thoracic idiopathic scoliosis. Hum. Mov. Sci. 2020, 73, 102680. [Google Scholar] [CrossRef] [PubMed]
- Tayob, I. The Reliability of the Axial Rotation Measuring Device in Measuring Thoracic Spine Rotation Range of Motion. Master’s Thesis, University of Johannesburg, Johannesburg, South Africa, 2018. [Google Scholar]
- Olson, K.A.; Goehring, M.T. Intra and inter-rater reliability of a goniometric lower trunk rotation measurement. J. Back Musculoskelet. Rehabil. 2009, 22, 157–164. [Google Scholar] [CrossRef]
- Katkar, M.; Phutane, V.; Ghogale, I.; Sohani, S.; Rawankar, A. Design of Optical Fiber Goniometer Having Physiotherapeutic Application for Measurement of Tilt in Human Joints. In Proceedings of the 2021 IEEE International Conference on Electronics, Computing and Communication Technologies (CONECCT), Bangalore, India, 9–11 July 2021. [Google Scholar]
- Sarioglu, K.; Pekyavas, N.O. A Comparison Between People With and Without Subacromial Impingement Syndrome and a New Method for Measuring Thoracolumbar Fascia Flexibility. J. Chiropr. Med. 2021, 20, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Walter, S.; Eliasziw, M.; Donner, A. Sample size and optimal designs for reliability studies. Stat. Med. 1998, 17, 101–110. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation coefficients: Appropriate use and interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef] [PubMed]
- Ries, J.D.; Echternach, J.L.; Nof, L.; Gagnon Blodgett, M. Test-retest reliability and minimal detectable change scores for the timed “up & go” test, the six-minute walk test, and gait speed in people with Alzheimer disease. Phys Ther. 2009, 89, 569–579. [Google Scholar]
- Bland, J.M.; Altman, D. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Johnson, K.D.; Kim, K.; Yu, B.; Saliba, S.A.; Grindstaff, T.L. Reliability of thoracic spine rotation range-of-motion measurements in healthy adults. J. Athl. Train. 2012, 47, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Sung, P.S.; Lee, K.J.; Park, W.H. Coordination of trunk and pelvis in young and elderly individuals during axial trunk rotation. Gait Posture 2012, 36, 330–331. [Google Scholar] [CrossRef] [PubMed]
- Hwang, D.; Lee, J.H.; Moon, S.; Park, S.W.; Woo, J.; Kim, C. The reliability of the nonradiologic measures of thoracic spine rotation in healthy adults. Phys. Ther. Rehabil. Sci. 2017, 6, 65–70. [Google Scholar] [CrossRef]
- Furness, J.; Schram, B.; Cox, A.J.; Anderson, S.L.; Keogh, J. Reliability and concurrent validity of the iPhone® Compass application to measure thoracic rotation range of motion (ROM) in healthy participants. PeerJ 2018, 6, e4431. [Google Scholar] [CrossRef]
- Navarro, I.; Candotti, C.T.; Amaral, M.A.; Dutra, V.H.; Gelain, G.M.; Loss, J.F. Validation of the Measurement of the Angle of Trunk Rotation in Photogrammetry. J. Manip. Physiol. Ther. 2020, 43, 50–56. [Google Scholar] [CrossRef]
- Straub, R.K.; Powers, C.M. Utility of 2D video analysis for assessing frontal plane trunk and pelvis motion during stepping, landing, and change in direction tasks: A validity study. Int. J. Sports Phys. Ther. 2022, 17, 139–147. [Google Scholar] [CrossRef]
- Cano-de-la-Cuerda, R.; Vela-Desojo, L.; Moreno-Verdú, M.; Ferreira-Sánchez, M.; Macías-Macías, Y.; Miangolarra-Page, J.C. Trunk range of motion is related to axial rigidity, functional mobility and quality of life in Parkinson’s Disease: An exploratory study. Sensors 2020, 20, 2482. [Google Scholar] [CrossRef]
- Van den Hoorn, W.; Cholewicki, J.; Coppieters, M.W.; Klyne, D.M.; Hodges, P.W. Trunk stiffness decreases and trunk damping increases with experimental low back pain. J. Biomech. 2020, 112, 110053. [Google Scholar] [CrossRef]
- Bucke, J.; Spencer, S.; Fawcett, L.; Sonvico, L.; Rushton, A.; Heneghan, N.R. Validity of the digital inclinometer and iphone when measuring thoracic spine rotation. J. Athl. Train. 2017, 52, 820–825. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).