1. Introduction
Modern medicine has experienced continual advancements in percutaneous galvanic current delivery for musculoskeletal injuries [
1,
2]. The clinical use of the same comprises oncological treatments [
3], known as electrolytic ablation, and chronic tendinitis [
4,
5], known as percutaneous needle electrolysis (PNE). The clinical use of electric currents has also been found to accelerate muscle regeneration in humans [
6].
Additionally, numerous in vivo as well as ex vivo studies have shown that cells can respond directionally to the application of electrical fields. This phenomenon is known as electrotaxis or galvanotaxis (reviewed by Cortese et al. [
7]). Vascular endothelial cells also respond to the phenomenon of electrotaxis, thereby enhancing angiogenesis [
8]. Additionally, cells involved in inflammatory or immune responses, such as lymphocytes [
9] or macrophages [
10], are also attracted to electrical currents. Furthermore, the migration mediated by electric currents involves cAMP and the G protein [
11,
12,
13]. Generally, cAMP and G proteins trigger many other events of cell signal transduction [
14,
15]. Therefore, electric currents can activate many specific cellular capacities.
Abat et al. [
16] assessed the effect of the application of PNE on a model of muscle lesions in rat by injecting intramuscular notexin. A small amount of intramuscular notexin caused a lesion of the whole muscle. The main results observed were that the application of a galvanic current induced a decrease in pro-inflammatory mediators (TNF-α and IL-1β) and an increased expression of anti-inflammatory proteins (PPAR-γ), as well as an increase in both the vascular endothelial growth factor (VEGF) and the VEGF–R1 receptor. More recently, Jorda et al. [
17] replicated the experiment of Abat et al., confirming that when applying PNE after injury, an increase in anti-inflammatory mediators and a reduction in pro-inflammatory mediators were observed. These authors reported that an overall promoted muscle regeneration was observed. Notexin creates a generalized lesion of the treated muscle. Plant et al. [
18] conducted a comparative study between the two myolytic agents; notexin and bupivacaine. The notexin caused a greater muscle injury and was more difficult to regenerate than with the bupicavaine. All previous studies used notexin to cause extensive muscle injury. However, muscle lesions in humans are usually localized and rarely extensive. In this study, bupivacaine has been used in order to produce very localized muscle injuries.
The neuromuscular synapse releases vesicles of acetylcholine as a neurotransmitter. These vesicles can be released massively, generating an action potential in the muscle fiber, or spontaneously. In spontaneous neurotransmission, isolated vesicles are released and stochastically distributed over time [
19]. An electromyographic-recording needle can record the spontaneous release of vesicles from several dozen muscle fibers [
20]. Electromyography devices usually incorporate a transducer that converts the electrical record into sound. Finally, the electromyographic record of spontaneous neuromuscular release is identified as a characteristic “endplate noise” [
20,
21]. No previous study has evaluated the restoration of neurotransmission after muscle injury. In this study, endplate noise was recorded as an indicator of the fully functional recovery of muscle fibers.
The purpose of this study was to determine the action of percutaneous needle electrolysis in muscle regeneration, by endplate noise recording, and functional reinnervation in an animal model based on bupivacaine-induced localized muscle injury.
2. Materials and Methods
2.1. Ethical Approval
The experiments on mice were carried out in accordance with the U.K. Animals (Scientific Procedures) Act, 1986, and in accordance with the guidelines of the European Community’s Council Directive (2010/63/EU) and the Spanish Royal Decree 53/2013 for the humane treatment of laboratory animals. The Animal Research Committee of the Universitat Rovira i Virgili (Reference number: 11337) reviewed and approved all experiments on animals. The experiments were performed 45 to 50 days post-natal on young adult Swiss male mice (Charles River, L’Arbresle, France). Mice were habituated to the facility for at least 1 week prior to studies and were housed in groups of four, with sawdust bedding and ad libitum access to water and food throughout. The animals’ room was maintained at a temperature of 22 ± 2 °C, a relative humidity of 50 ± 10%, and a 12-h light/dark automatic light cycle.
2.2. Experimental Groups
For the control series of the muscle injury, three groups were formed with three mice in each group. After BPV was injected into the right limb and the same volume of saline was injected into the left limb (control), electromyography assessments of both limbs were performed at 72 h and 7 and 10 days (see
Figure 1a).
Regarding the experimental series for the currents, three groups were formed with three mice each, and BPV was used to treat the two limbs of each animal. Forty-eight hours after the application of BPV, the destruction of the affected muscle fibers commence, followed by the inflammatory reaction [
22]. PNE was applied at this time. A needle was longitudinally inserted into the muscle package; however, the PNE protocol was only administered in the right limb of each animal. Thereafter, electromyography of both limbs was performed (left limb BPV; right limb BPV+PNE) at 72 h and 7 and 10 days (see
Figure 1b).
2.3. Experimental Protocols: Focal Muscle Injury and Percutaneous Needle Electrolysis
The muscle injury in the gastrocnemius was provoked in the posterior muscle package of the limb using an intramuscular administration of three injections of bupivacaine (BPV) on the midline of the distal third, middle third, and proximal third of the posterior muscle package (bupivacaine hydrochloride monohydrate, Sigma Aldrich, Madrid, Spain; the working solution was made up at 0.75% in saline solution at 0.9% at pH 6.5). The volume injected in each area was 0.02 mL, and the process was repeated 24 h after the first administration (total volume administrated was 0.12 mL). The same procedure and volume were applied in the control limb by administering 0.9% NaCl (saline solution). The gastrocnemius muscles were used for electromyographic recordings.
Single and highly localized subcutaneous infiltrations of BPV were performed in the cranial portion of the LAL muscle. As with the gastrocnemius muscle, these were limited to the middle third of the muscle. In this scenario, the injected volume was 0.02 mL in a single point, and the process was repeated 24 h after the first administration (total administrated volume was 0.04 mL). In this muscle, electric currents were not applied. The aim was to evaluate the effectiveness of focal BPV treatment.
For the intramuscular treatment administration of Microlance, a needle measuring 0.3 × 13 mm was used. For all injections, the depth of administration was controlled using a depth limiter placed on the external part of the needle cannula.
The protocol for PNE used during this study was 1.5 mA for five seconds with three repetitions. This was administered by inserting the needle longitudinally into the muscle package on the back of the right leg (anode), which had been inoculated with BPV 48 h beforehand. The cathode was subcutaneously inserted into the lumbosacral area of the mouse. The needles used were Physio Invasiva® Needles, 0.30 × 30 mm (PRIM, Madrid, Spain). The device generating electrical currents was a Physio Invasiva® 2.0 (PRIM, Madrid, Spain).
2.4. Endplate Noise Recordings
The needle EMG (nEMG) recordings were obtained from an anesthetized animal at a controlled room temperature of between 22 and 25.8 °C. The muscle used for this study was the gastrocnemius because of its ease of access and suitability. Recordings were obtained with an electromyography system (Medelec Mystro plus, GR20, Teca Medelec, London, UK) using a monopolar EMG needle (Natus Manufacturing Limited, Galway, Ireland). The needle was slowly inserted into the muscle and, once inside, it was moved in order to enable recording in all directions. The muscle was divided into twelve areas to cover both the entire muscle and avoid recording the same endplate noise twice. The recording needle was introduced into the gastrocnemius until an audible change was heard. The electromyography screen was then studied, and if it was correct (without an alternating current, artifacts, etc.), the endplate noise was recorded. The number of areas with endplate noise (maximum twelve) was recorded. During the endplate noise recording, the frequency was studied as the number of potentials per second that appeared, expressed in Hz.
The first record was made in the right gastrocnemius (control record). The left gastrocnemius was then recorded (experimental record). In order not to repeat or omit any area, a systematic order of the areas were followed, whereby the registration procedure commenced from the distal to the proximal end. In each area, the recording needle was inserted slowly and without making sudden movements and once placed, small turns were made, within each of the twelve areas, to locate any recordable signal. A zone was considered to have plaque noise when it appeared and was sustained for 5 s.
The gastrocnemius muscles were partially injured after the 12 insertions of the electromyographic recording electrode, so they could not be used for the morphological techniques (methylene blue and immunofluorescence). In order to optimize the mice, the morphological techniques were performed in the LAL muscle.
2.5. Sample Collection and Histology
At the end of the experiment, animals were deeply anaesthetized with isoflurane before being euthanized by exsanguination. The levator auris longus (LAL) was excised and dissected on a Sylgard-coated Petri dish containing normal Ringer solution continuously bubbled with 95% O2/5% CO2. The LAL muscles were used for methylene blue staining and immunological labeling.
2.6. Methylene Blue
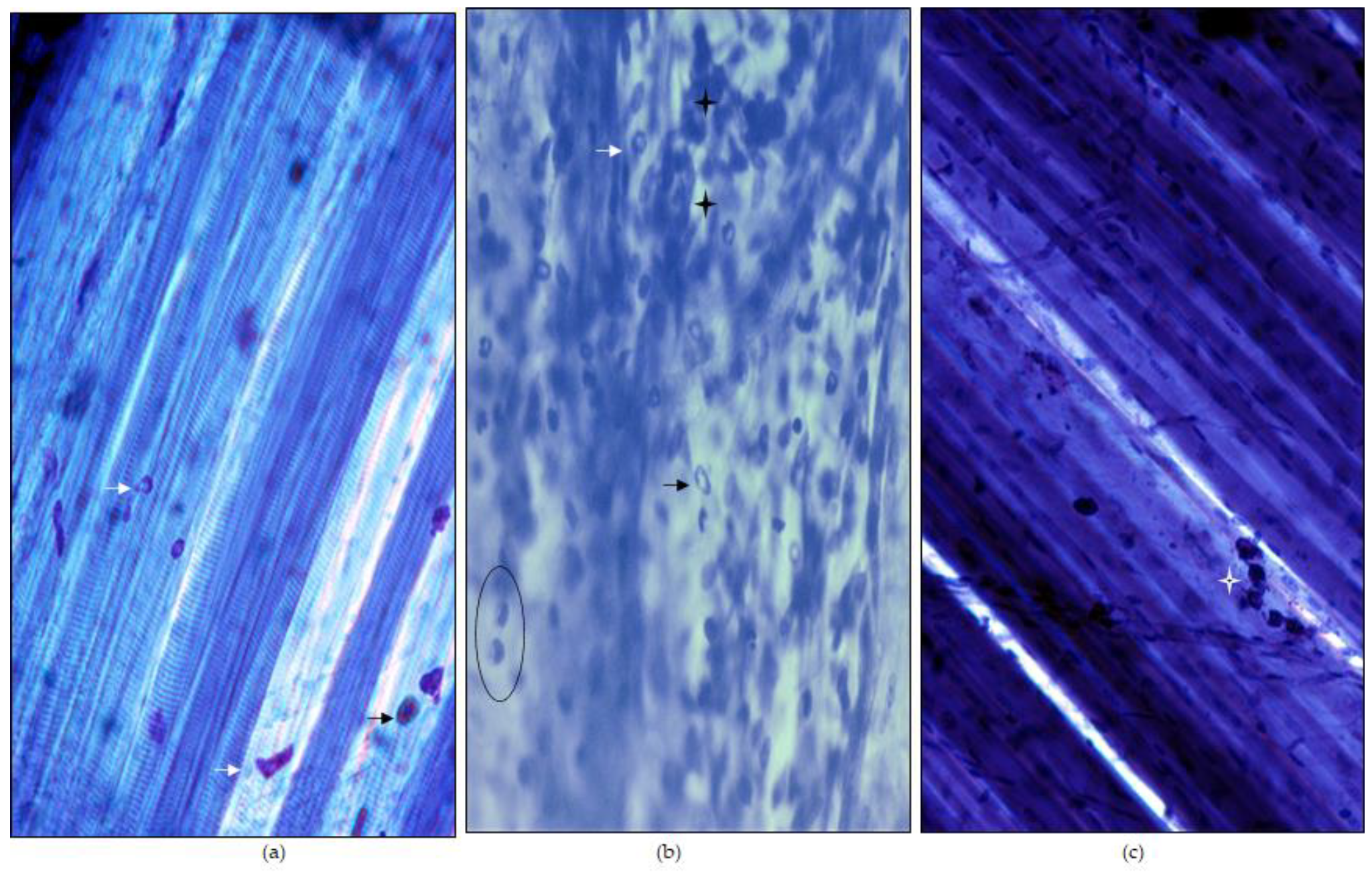
Whole LAL muscles were removed and exposed to 1% methylene blue (Sigma–Aldrich, Steinheim, Germany) dissolved in 1% borax for two minutes. Subsequently, the samples were washed with distilled water for three periods of two minutes each. Finally, dehydration procedures and mounting with epoxy resin were performed.
2.7. Immunohistochemistry
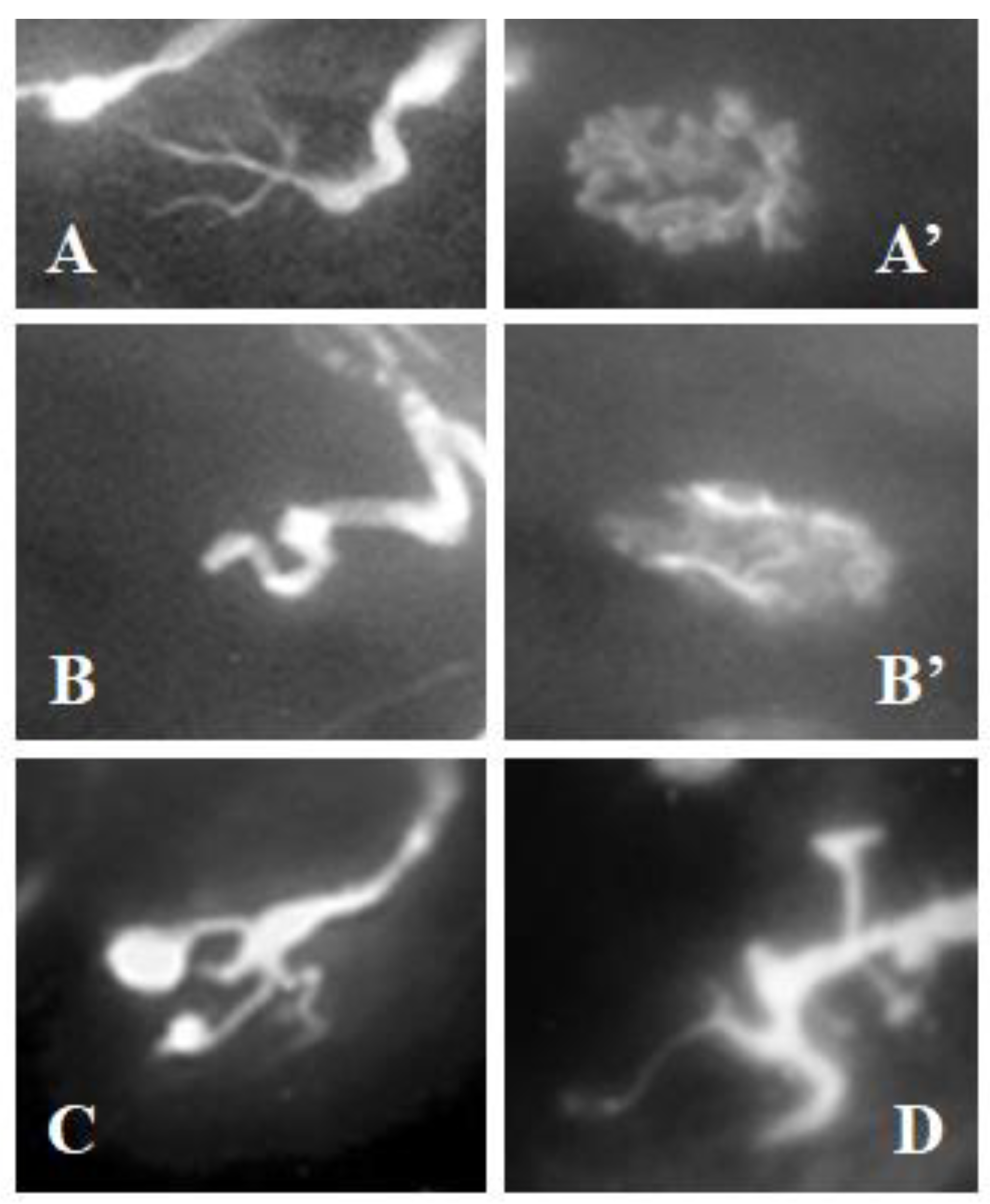
Whole LAL muscles were removed and fixed in 4% paraformaldehyde in PBS (pH 7.4) for 45 min at room temperature (~22 °C). The LALs were double labeled for axons with fluorescein isothiocyanate (FITC)-conjugated antibodies against 200-kD neurofilament protein monoclonal antibodies (Cat# N2912, Sigma–Aldrich, Steinheim, Germany; 1:500 in 1% BSA) and post-synaptic nicotinic acetylcholine receptors with Tetramethyl Rhodamine Isothiocyanate (TRITC)-α-bungarotoxin (Molecular Probes, Eugene, OR, USA; Cat# T1175). The muscles were mounted in Mowiol with p-phenylenediamine (Sigma–Aldrich, Steinheim, Germany).
2.8. Statistical Procedure
Values are expressed as the mean ± SEM. The values are expressed as the “percentage of change”. This is defined as: [experimental value/control value] × 100. We used the two-tailed Welch’s t-test for unpaired values because our variances were not equal. This test was chosen as it is more conservative than the ordinary t-test. Differences were considered significant at p < 0.05.
4. Discussion
This study performed a controlled experimental partial muscle injury. We found that, in lesioned areas, an axonal retraction occurred, which justifies the decreased spontaneous neurotransmission. Furthermore, the application of PNE improved the functional recovery of the injured muscle tissue.
4.1. Muscular Damage by Bupivacaine
Initially, a highly localized, easily reproducible lesion was achieved. Bupivacaine was chosen because it is described as a contact myolytic agent [
23]. Toxins such as notexin have been more recently used [
16], but nevertheless, those toxins have been proven to cause more extensive and serious injury than bupivacaine [
17].
The myotoxic effects of BPV have been known since the 1980s. The works by Tomas i Ferrer et al. [
22] as well as Benoit and Belt [
23] have demonstrated that intramuscular treatment produces a degeneration of the muscle tissue without affecting the nerves or the intramuscular vessel, although it does provoke a retraction of the axon in the neuromuscular junction due to the destruction of muscle fibers within 24 and 48 h. In the present study, we performed a controlled lesion, which was observable with methylene blue.
The axonal retraction secondary to the lesion of the muscle fibers is associated with the decrease in the number of areas and the reduction in the frequency of the endplate noise in the electromyography recordings obtained in the present study. As there were fewer functional axonal branches, the probability of ACh release was reduced, with a reduction in all associated parameters.
The axonal branches remained in the area affected by BPV until the myotube phase, which is when they completely reoccupied the synaptic contacts. This occurred between days five and seven [
22]. Furthermore, Plant et al. [
18] observed that the greatest degeneration of muscle tissue treated with BPV occurred within 48–72 h. There was also a correlation between the tissue degeneration observed with histological tissues and the functional study in which the contractile properties were assessed. During both periods, a partial degeneration of the tissue was recorded, which, on a functional level, represented a decrease in the capacity to generate isometric strength. In the present study, the electromyographic recording at 72 h showed a decrease in the number of areas with endplate noise as well as a decreased frequency. This is compatible with findings reported by Plant [
18]. These authors found a recovery of the treated tissues in the recordings performed on days 7 and 10, leading to an increase in the isometric strength.
Thus, by assuming a functional recovery of acetylcholine release, it should be possible to electromyographically record a recovery of endplate noise to control values. However, in the present study, on day 7, the initial values were still not obtained, and only in a number of areas were these values observed on day 10. Therefore, although morphological recovery of the synaptic contacts was shown, they were not yet completely operational.
4.2. Muscles Partially Injured with BPV and Treated with Percutaneous Needle Electrolysis
Electrical currents are beginning to be used to treat patients with muscle injuries in order to accelerate regeneration. Thus, for example, Hollis and McClure [
6] described the case of a muscle lesion of the tibialis anterior secondary to a reparatory surgery of the ankle which, after several weeks, recovered rapidly by applying electrical currents.
In previous works, Guo and coworkers [
24] and Fujiya et al. [
25] stated that electro stimulation protocols with microcurrents enhanced the recovery of muscle tissue during the regeneration phase of muscles damaged with a cardiotoxin. These authors described an increase in the transcription box protein 7 (PAX-7) in the muscle treated with micro currents. PAX 7 is expressed in the activated satellite cells. These cells proliferate and differentiate to mature fibers and replace those damaged in situations of muscle injury [
26]. The mechanisms described by those previous works may also be implicated in the faster regeneration observed in samples exposed to galvanic current in the present study.
There appears to be proof that electrical currents applied to lesioned muscles induce a decrease in pro-inflammatory mediators (TNF-α and IL-1β), as well as an increased expression of anti-inflammatory proteins (PPAR-γ) and an increase in vascular endothelial growth factor (VEGF) and its VEGF-R1 receptor [
16]. Recently, the team led by Soraya L Valles [
17] replicated the study by Abat et al., finding similar results but with more mediators. For example, the galvanic current prevented the increase of proinflammatory mediators, such as the cytokine IL-6 and the chemokines CCL3, CCL4 and CCL5. In addition, they described a decrease in the expression of CCR8 and NF-κB after treatment with galvanic current. In contrast, an increase in the anti-inflammatory mediators IL-10 and IL-13 after galvanic current treatment can aid in recovery from notexin-induced damage. All of these results indicate that galvanic currents can improve muscle regeneration. Therefore, these currents have an anti-inflammatory action. However, they facilitate the revascularization of the lesioned area. In addition, it is important to note that the endothelial cells respond to electrotaxis, thereby generating angiogenesis [
8]. In parallel, electrotaxis phenomena have been linked to cells involved in inflammatory or immune responses [
9,
23]. Muscle regeneration after a focal lesion was described many years ago [
26,
27]. First, an inflammatory reaction occurs, which produces a “flushing out” of the necrotic waste in the lesioned area. Thereafter, the satellite cells that are activated proliferate and fuse to create a myotube. Finally, the myotubes synthesize the actin and myosin myofilaments that form sarcomeres to fuse with those previously existing. Efficient muscle regeneration requires appropriate muscle irrigation [
28], and electrical currents may facilitate this irrigation [
8]. Furthermore, an effective inflammatory reaction facilitates complete muscle regeneration [
2,
27]. Electric currents facilitate the inflammatory reaction and muscle irrigation, thereby facilitating muscle regeneration. Our findings revealed that electromyographic recovery of endplate noise in muscles treated percutaneously with galvanic current is relatively quick (72 h), coinciding with the inflammatory reaction.
4.3. New Therapies in Muscular Regeneration
In recent decades, novel strategies have been developed to improve muscle regeneration. For example, the use of bone marrow mesenchymal stem cells (BM-MSCs) (see review by [
29]). Thus, BM-MSCs could promote regeneration of musculoskeletal tissue and activate myogenic differentiation of satellite cells. Furthermore, BM-MSCs also promote nerve regeneration in case the injury also has neural consequences [
30]. However, these strategies are often used for severe and substance-loss injuries. In injuries without loss of substance, such as sports injuries, there is not much progress. Cryotherapy, possibly one of the oldest non-pharmacological therapies in muscle regeneration [
31], continues to be used successfully. In these years, several variations have been introduced in cryotherapy, varying the exposure to cold only of the affected limb or the entire body, duration of treatment, time of application post-injury, etc. [
32]). In contrast, microwave heating has been applied with relative success [
33]. Platelet-rich plasma injections have also been tested but showed no effect compared to the control [
34,
35]. Extracorporeal shock wave therapy can accelerate regeneration after acute skeletal muscle injury [
36], but it requires many applications over several weeks. The PNE therapy that is evaluated in this study is applied in a much localized and effective way in the injured area. Its main advantage lies precisely on the fact that it is quick and easy to apply for an expert professional. In addition, the infrastructure needed is portable and minimal. Moreover, PNE can also be applied in combination with others such as diathermia or more complex therapies such as BM-MSC and even those that are pharmacological based on the professional’s choice.
4.4. Limitations of the Work
The use of mice in translational science has several limitations. Unlike athletes, the state of well-being of mice can only be known indirectly. Thus, a mild annoyance that may be critical for an athlete may be missed in a mouse study.
The significant size difference between the muscles of mice and athletes may also have implications. Percutaneous electrolysis in the muscles of mice can easily encompass the entire muscle treated with a single central insertion. However, in the case of athletes, it is essential to use ultrasound to insert the needle into the injured area.
In summary, the histological and functional evidence observed in this study demonstrates that the application of PNE during muscle regeneration in an animal model of muscle injury reduces the recovery time of the damaged muscle tissue.


 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}




