Abstract
(1) Background: Different intervention strategies, such as reminiscence and music-based therapies, effectively mitigate the cognitive decline of individuals with dementia (IwD). An important challenge when implementing these approaches lies in the need for content customization. We designed Musiquence platform, a framework that allows the customization of music and reminiscence content in cognitive stimulation activities. (2) Methods: Here, we present a participatory design methodology for designing a seven-week customized cognitive stimulation program (CCSP) for IwD using Musiquence. We ran focus groups with 19 formal caregivers, who provided information regarding themes and music to be used in activities for IwD, and gathered preferences from 20 IwD. (3) Results: The CCSP consists of seven cycles of tasks combining the activities available in Musiquence, the seven preferential themes of IwD, and the seven songs most frequently referenced by formal caregivers. (4) Conclusions: Finally, we provide a set of guidelines to implement a participatory design approach for content development together with IwD.
1. Introduction
1.1. The Burden of Dementia and Non-Pharmacological Approaches as a Research Priority
The proportion of older adults is estimated to double from about 12% to 22% between 2015 and 2050 [1], which will increase the number of age-associated diseases, such as dementia, which already presents 10 million new cases every year [2]. Dementia is a clinical syndrome characterized by a progressive and irreversible deterioration of cognitive functioning, leading to cognitive impairment [3]. Consequently, emotional and behavioral domains are also affected, resulting in a progressive loss of functional abilities and autonomy [3,4,5].
In recent years, investigation of the consequences of cognitive deficits has grown, and ways to reduce the impact of both healthy and pathological age-related cognitive deficits are considered a research priority [3,4]. Even though pharmacological approaches are the first line of treatment for cognitive and behavioral symptoms, their effect is still limited to the early months of treatment [4]. Increasing evidence supports that non-pharmacological approaches (e.g., cognitive and psychosocial interventions), developed to be implemented in parallel with the former, can (1) maintain and improve cognition, (2) encourage social interaction, and (3) enhance the well-being of IwD [5,6]. However, there is still a need for investment in these approaches (e.g., positive approaches such as reminiscence, validation therapy, and reality orientation) to complement the medical and neurological models [7].
The most studied and well-established non-pharmacological intervention for individuals with mild to moderate dementia is Cognitive Stimulation Therapy (CST)] [8,9]. The CST program is an evidence-based approach developed by Spector and colleagues [10,11] which builds on the significant impact of reality orientation, reminiscence, and validation therapy. The underlying assumptions behind CST are:
- IwD can benefit from cognitive stimulation if we mobilize relatively preserved cognitive functions (e.g., crystallized abilities such as semantic memory and verbal skills);
- Even in advanced age, exposure to enriched environments (i.e., those that are socially, and cognitively challenging) can enhance cognitive reserve and neuroplasticity [12,13].
Concerning point 1, it is known that even in moderate to advanced stages of dementia, musical memory is one of the abilities that remain relatively intact [14]. It is hypothesized that music-processing abilities precede the development of lexical language functions. This hypothesis is corroborated by findings which demonstrate that IwD are still responsive to music even when unable to communicate verbally or recognize words. For instance, it has been shown that individualized music listening can lower depression symptomatology and agitation in IwD and can increase positive emotions [15].
Additionally, music is frequently associated with life experiences [16]. When studying musical memory in Alzheimer’s disease, Baird and Samson found that memories associated with specific music would be recollected longer than memories with no association with music [14]. This suggests that using music as a reminiscence element in cognitive stimulation programs can positively affect cognition [17]. Regarding point 2, it is of the utmost importance to enrich the environment for IwD. Here, combining both music and reminiscence-related elements, as well as customized cognitive stimulation programs, could impact cognitive reserve and neuroplasticity. However, there is a need to find frameworks that facilitate the combination of such elements, allowing the replication and customization of cognitive stimulation activities.
1.2. Interactive Technologies as a Valuable Tool to Implement Non-Pharmacological Approaches
Over the past few decades, the role of technological approaches in health settings has been a matter of scientific research. Marin and colleagues [18] described two possibilities of technology use in populations with cognitive impairment: (1) assistive technologies for cognition, such as “low tech” devices (e.g., written lists/checklists), “mid tech” devices (e.g., programmable wristwatches), and “high tech” devices (e.g., smartphones); and (2) rehabilitation technologies for cognition, such as “low tech” devices (e.g., paper-and-pencil worksheets), “mid tech” devices (e.g., Snoezelen), and “high tech” devices (e.g., serious games) [18].
Concerning interactive technologies for cognitive stimulation, Ferreira and colleagues [19] studied the interaction of IwD with different technologies, aiming to develop a serious game adapted to this clinical population. They concluded that although most IwD were able to perform the proposed tasks in the different technological devices (e.g., head-mounted display, leap motion), their performance and experience varied according to their profile (e.g., cognitive status, schooling, age), which suggested the need for customizing technology to IwD [19].
Accordingly, Ferreira and colleagues (2019) developed a platform—Musiquence—that is compatible with different technologies (such as computers, tablets, smartphones, and augmented reality) (cf. Figure 1,) and can be adapted to each patient’s needs (e.g., motor difficulties, vision problems, tremble) and cognitive profile. In addition, Musiquence incorporates two key elements of CST—music, and reminiscence—in cognitive stimulation activities for IwD, since the content can be personalized to the user [17]. Caregivers can add text, images, and music when creating cognitive stimulation tasks, according to the IwD’s personal preferences. Musiquence enables the gamification and personalization of the following six types of activities:
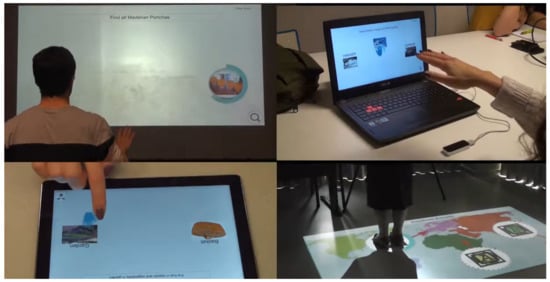
Figure 1.
Examples of Musiquence activities being performed in several types of technologies.
- Reality Orientation—a quiz-like activity that includes date and time information.
- Creative Drawings—a puzzle-like game in which missing parts must be drawn using real paper and crayons.
- Activities of Daily Living (ADL)—a puzzle-like game in which real physical objects (e.g., toothpaste) must be used to answer.
- Search Objects—an exploration game where hidden images (e.g., cats) must be found using a magnifying glass.
- Knowledge Quiz—a quiz-like activity in which the correct answer must be selected.
- Association—a categorizing activity where items must be organized according to the instructions (e.g., separate cars from motorcycles).
Musiquence includes an “editor” tool, in which the health professional can create, replicate, add, and eliminate different activities according to the defined goals. Then, activities are performed by IwD according to a pre-selected order. This allows systematic inclusion and presentation of multimodal stimuli that would not be easily implemented in paper-and-pencil cognitive stimulation activities [17].
1.3. Designing Interactive Technologies-Based CCSP’s for IwD
Even though technology has been continually evolving and is becoming more user-friendly for specific populations (such as dementia), there is still a need for standardized protocols for developing content to be integrated with technology-based customizable tasks [20,21]. It seems clear that if we aim to maximize the impact of reminiscence and music-based cognitive stimulation programs, the content of those tasks must be customized to the specific characteristics of the target IwD. Félix et al. (2020), in a case report with a CCSP, found that the personalization process increased IwD’s engagement and participation in the activities and promoted mood stability and better acceptance of the dementia diagnosis [22]. Additionally, involving formal caregivers and IwD in creating content may help overcome some limitations and engage caregivers and IwD to embrace technological solutions [23]. Unfortunately, literature reporting participatory design approaches involving IwD is still scarce.
Most studies report the involvement of IwD in the development of technological solutions (ex., supportive technologies) [20,23], provide general guidelines for the interaction between the researcher and IwD [24,25] or simply describe the challenges experienced in the implementation of such methodologies with this specific clinical population [26]. For example, Hendriks and colleagues (2014) concluded that aspects such as cognitive limitations, peculiarities of different types of dementia, lack of insight, and stress associated with the tasks, and burden for the researcher could hamper the implementation of a participatory design approach with IwD [26].
Some of the limitations of previous studies are related to the cognitive impairments caused by dementia, such as altered decision making and difficulty expressing wills and preferences [27]. The co-designing process demands certain levels of sensory, cognitive, and motor abilities that may be affected by dementia [27]. Still, IwD can maintain full or partial insight for a long time [28], which has led to a valorization of IwD’s feelings and wills over the last years, with several studies considering first-person perspectives of IwD in different contexts (e.g., developing technologies, evaluating services, and promoting emotional safety) [23,29]. Tanner (2012), in a reflection on co-researching with IwD, concluded that older IwD could make valuable contributions to research as both co-researchers and participants when able to communicate [21]. Warmoth et al. (2020) found that employing these participatory approaches (that consider IwD’s perspectives) is perceived as empowering by both IwD and their caregivers [28].
1.4. Aims of the Study
Considering the potential of new information and communication technologies (ICT) in delivering customized non-pharmacological interventions, this study’s primary goal is to use a participatory approach to create a protocol to support healthcare professionals and/or researchers in customizing cognitive stimulation activities for IwD.
Thus, we aimed to answer two research questions (RQ):
- RQ1: How can a participatory strategy be implemented to create content for a CCSP involving both IwD and formal caregivers?
- RQ2: Which guidelines should formal caregivers consider to engage IwD in the customization of CCSP?
2. Materials and Methods
Although Musiquence allows individualized content personalization, we decided to use the same content for all the study participants in order to ensure the CCSP is inclusive and targets the largest number of IwD possible. However, the same approach presented here can be implemented for everyone. As such, the themes and songs were personalized to a specific generation and location, avoiding bias in assessing Musiquence in a subsequent clinical impact and validity study.
2.1. Participants
This study was approved by the University of Madeira ethics department (02/2020). and all participants, or legal representatives, gave their informed consent. Our sample consisted of two groups of participants: (1) formal caregivers; and (2) IwD (the inclusion criteria is described in Table 1), recruited in healthcare institutions.

Table 1.
Inclusion criteria according to the sample group.
2.2. Procedure
- (1)
- Interviews with formal caregivers
Given the specificities of the target population, we approached institutions with expertise in the care of IwD in the Autonomous Region of Madeira (ARM). We had access to formal caregivers with diverse backgrounds (such as psychologists, nurses, physiotherapists, music therapists, and occupational therapists) that regularly developed activities for IwD. We gathered with small focus groups (4–5 people) and asked them about: (1) the type of activities they performed with IwD, (2) the songs used, and (3) the topics approached within those activities (Figure 2. Then, we identified a set of topics (e.g., Christmas) that originated themes (e.g., Festivities).
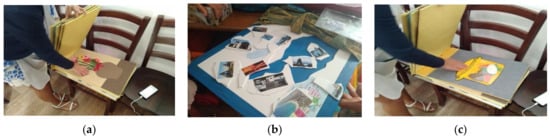
Figure 2.
Themes and activities used by formal caregivers for cognitive stimulation of IwD. (a) multi-sensorial stimulation activity; (b) reminiscence-based stimulation activity; and (c) activities of daily living-based stimulation activity.
- (2)
- Interviews with IwD
From the themes referenced by formal caregivers, the ones that received the most votes were presented to IwD, using a combination of a written subtitle and four representative images per theme. Their task consisted of selecting all the images by order of preference (the first was the most preferred image, and the last was the least preferred). Before starting the task, the researcher went through all images with the IwD to ensure that they all associated the same meaning to each image (Figure 3). The ranking of songs by preference would be confusing and challenging for IwD, leading to biased results, so it was decided to use the feedback provided by the formal caregivers.

Figure 3.
(a) Presentation of the most referred themes to IwD, using verbal and visual information; (b) researcher went through the images together with IwD to assure that they all assigned them the right meaning.
- (3)
- Development of the activities
The first step for developing the activities for our CCSP consisted of selecting the preferred themes. We ranked the themes by the mean ranking of their four most representative images—lower means corresponding to the preferred themes.
Hence, our CCSP for IwD was organized by a cycle of tasks—meaning that all six types of activities of Musiquence (reality orientation, creative drawings, ADL, knowledge quiz, association, search objects) would be performed on each cycle. Each cycle of tasks corresponds to a song, a theme, and four exercises per activity. The duration, frequency, and periodicity of the cognitive stimulation sessions were established based on CST principles [30].
2.3. Tools
We developed and used semi-structured sessions to perform the interviews with formal caregivers and IwD (questions are described in Table 2). Participants were encouraged to elaborate on their answers whenever possible.
Table 2.
Sample groups and topics approached during the information gathering process.
Concerning our second RQ, we registered all relevant information while interviewing both formal caregivers and IwD. Namely, we considered the experience of:
- Formal caregivers, in what concerns the development and implementation of cognitive stimulation activities of IwD (e.g., difficulties experienced);
- IwD when performing the implemented task (e.g., comments and feelings);
- The researcher, when implementing the task with IwD.
These registers were analyzed to provide guidelines on how to implement a participatory design approach for content creation with IwD.
3. Results
3.1. Interviews with Formal Caregivers and IwD
Concerning our sample, we invited 19 formal caregivers (1 male and 18 females), aged between 24 and 45 years old (M = 31.7; SD = 7.17) and with 12 to 17 years of formal education (M = 15.33; SD = 1.63); and 20 IwD (9 males and 11 females), with ages between 55 and 86 years old (M = 74; SD = 9.62) and 3 to 17 years of formal education (M = 6; SD = 4.18). From the 20 IwD, 15 lived in an institutional setting and 5 lived in a community setting. Sociodemographic data of institutional IwD were obtained from the institutions.
From the interviews with formal caregivers, 21 themes were referred to as the most prevalent in developing activities for IwD. From the 21 themes, we selected the 14 with the most votes to be presented to IwD, which they arranged by preference to reduce the poll of themes to seven favorites: public figures; festivities; regional traditions; flowers; agriculture; typical regional recipes; and foods (cf. Figure 4). These seven themes were then used to customize the content for the CCSP, with each cycle of tasks corresponding to one song, one theme, and four exercises per activity. The 14 sessions were spread over seven weeks, originating seven cycles of tasks (Figure 4).
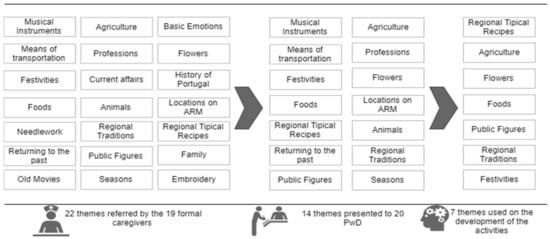
Figure 4.
Themes given by the formal caregivers, themes presented to IwD, and themes used in the development of the activities (IwD’s favorites).
Regarding the songs most used by formal caregivers most often to develop and perform tasks with IwD, we identified 81 songs, most of them from before the year 2000. We grouped the songs into five broad categories: Regional Artists, Portuguese Artists, Folk Music, Eurovision, and Fado. We selected the seven most referenced songs to match the number of task cycles. Each cycle of tasks corresponded to one of the most frequently mentioned songs. The preferred theme was matched with the song with the most votes; the second preferred theme was matched with the song with the second highest number of votes, and subsequently for the remaining five cycles of tasks (cf. Table 3).
Table 3.
Sessions, themes, and songs corresponding to each cycle of tasks.
We structured our CCSP according to the six activities available on Musiquence. Since reality orientation and reminiscence are two key principles of CST [30], we decided that all sessions should start with Musiquence’s “Reality Orientation” activity, and all content should be related to the past (e.g., a period in which IwD were adolescents or younger adults). The reality orientation activity should include questions about the present time (e.g., day of the week, month) and place (e.g., city, address). The remaining activities were randomly distributed through the two weekly sessions of each cycle of tasks. Since “ADL” and “Creative Drawings” activities have the same structure, they should be interchangeable. For instance, participants may have to complete the task using an actual physical object or draw the correct answer to complete the task. The difficulty level is increased at the end of each cycle of tasks (cf. Figure 5).
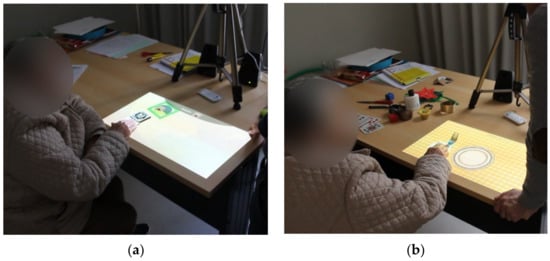
Figure 5.
(a) IwD performing Search activity, on Musiquence, in an AR-format; (b) IwD performing ADL activity, on Musiquence, in an AR-format and using real physical objects to answer.
3.2. Guidelines
As a result of this participatory approach, we outlined some guidelines that need to be considered when working with IwD, and are organized in the following topics:
- Communicating with IwD;
- Music content selection;
- Reminiscence content selection.
4. Discussion
Our study aimed to systematically and informedly customize the content of a cognitive stimulation program for IwD living in ARM, using the Musiquence platform.
To the best of our knowledge, no similar studies aimed to include formal caregivers’ and IwD’s perspectives to customize content for cognitive stimulation activities implemented in interactive technologies. Still, our results are consistent with the existing literature, reporting that participatory design approaches are crucial to the development of technologies and content for people with special needs [23]. We experienced that, due to dementia-related cognitive deficits, IwD may not always provide the sought information explicitly. Hence, a close collaboration between researchers, formal caregivers, and IwD is required to successfully unveil information that reflects their perspectives and preferences, which can help to assure their engagement and motivation when performing the intervention.
Concerning our first RQ, we intended to identify the preferential content for IwD living in the ARM to be implemented on a CCSP. During the interview, formal caregivers mentioned that it was challenging to personalize activities while closely supervising their performance. Additionally, we realized that there is still a considerable lack of specialized care units for IwD in the ARM and, consequently, limited human resources to develop occupational activities for IwD, which represented a challenge when recruiting our sample.
As an alternative to personalizing the interventions’ content, formal caregivers mentioned finding common interests of different IwD. For example, most IwD had similar ages and similar life experiences, facilitating the choice of songs and themes to use. Finding these shared experiences was our starting point to customize the content and generalize it to all participants. From these interviews with formal caregivers, we also understood the importance of customizing the content of cognitive stimulation activities, which led us to rely on a platform that responds to this need: Musiquence.
Concerning our second RQ, we considered the information provided by formal caregivers, the reports of IwD, and the experience of the researcher in implementing the task, and created a set of guidelines on how to perform this type of study. Before defining the contribution and role of IwD in the participatory design, it was important to gather information about the patient’s cognitive profile to determine the most preserved and impaired cognitive functions, the stage of dementia, and the sociodemographic background. Most of the institutions from which we recruited our sample only provided the patients’ Mini-Mental State Examination (MMSE) [31] score, a cognitive screening tool that does not allow a comprehensive and detailed assessment of cognitive functioning. As such, for the purposes of our study, having more information would be useful when determining the type and difficulty level of the tasks to be developed. Concomitantly, we found some supportive guidelines to be used when such participatory design approaches are adopted:
- 1.
- Communicating with patients
Most participants from our study had a low literacy level, a low-skilled occupation (e.g., farmer, seamstress), and had little or no contact with technological devices. Consequently, we had to support them in fully comprehending the study’s objectives and verbally expressing their preferences. Hence, we collected their preferences by employing what we thought was a straightforward task—selecting their preferred images. However, our decision to use 4 representative images for each theme resulted in a total of 56 images presented to IwD, which may have been overwhelming for some of our participants. We felt that cognitive deficits affected IwD’s ability to express their wills and preferences, which compromised their decision making when confronted with the need to select the images. Even though all our participants successfully completed the task, they could not always justify their choice and sometimes felt confused when trying to do so.
As such, when introducing task goals, it is important to guarantee that the interviewer speaks clearly, slowly, and uses short and simple sentences: this is crucial to ensure that IwD understand what they need to accomplish. Thus, our task instructions were straightforward: “What are your favorite images? Please choose them one by one”, which we found to be adequate most of the time. None of our participants expressed doubts or concerns about the previous instruction. Our major difficulty was that our participants sometimes forgot the provided instruction. To overcome this, we repeated instructions during the task. Repeating the same instructions allowed them to refocus and keep the task goal in mind. Additionally, some participants were aware of their forgetfulness, which made them feel uncomfortable, so we did not wait for them to request the repetition of the instruction. When they seemed lost or confused, we simply repeated the instruction and encouraged them to continue.
- 2.
- Music content selection
During the focus groups with formal caregivers, we understood that it could be difficult for IwD to recall the different songs presented for the necessary time to allow them to organize them by order of preference. As such, we decided to question formal caregivers about the most used songs when developing activities with IwD, as well as their reaction to these songs. For instance, we asked them to mention songs to which IwD commonly sang or danced. There was a high level of agreement between formal caregivers in terms of the most frequently used songs.
- 3.
- Reminiscence content selection
During task performance, all participants recognized the presented images. It was very common for them to recall specific memories from their past, which was a great accomplishment of our work. When asked to select their favorite image, it was difficult for them to choose only one, as several images reminded them of personal experiences. They were able to recall those experiences and explain them to the researcher. During the selection of images, IwD were unaware of the theme that each image represented, but they were commonly able to make that association. For example, concerning the themes “Typical regional recipes” and “Festivities”, most IwD categorized the visual stimulus as belonging to such categories.
Accordingly, ensuring stimuli quality and familiarity is crucial: we included images that depicted familiar objects, people, foods, and landscapes to ensure that IwD interpreted them correctly. Some participants named images but assigned them different meanings. In these cases, we redirected them to the intended meaning. Nonetheless, despite our efforts to clarify each image’s meaning, it could have been beneficial to include fewer images per theme and find alternative ways of presenting them, since impaired processing abilities and decision-making deficits expressed by IwD can affect performance.
Additionally, it can be helpful to combine different sensory elements: this may enhance the performance of IwD. We presented different themes with visual (e.g., images) and verbal aids (e.g., oral and written) and found them to be effective with our participants.
Currently, we are conducting a longitudinal clinical study with IwD living in the ARM, with the aim of assessing the impact of the CCSP on cognition (e.g., attention, memory, language), mood (e.g., anxious, depressive symptoms), functionality, and quality of life. Neuropsychological assessments will target the referred domains and will be performed in three different moments: pre-CCSP, post-CCSP, and follow-up (3 to 6 months). We gathered some usability results from our first two participants, who have already finished the 14-session CCSP intervention in an augmented reality (AR) format. Participant 1 (P1) was an 85-year-old embroiderer with three years of formal education and a formal diagnosis of Vascular Dementia, while participant 2 (P2) was a stay-at-home wife of 76 years old with three years of formal education and a diagnosis of Lewy Body Dementia. Even though P1 and P2 had low digital literacy, both could autonomously perform all tasks available on Musiquence (P1 became autonomous on the sixth session, and P2 on the eighth). P1 usually sang during sessions and provided personal information related to the themes and songs used—for instance, on the typical recipes theme, she would explain to the researcher how to prepare the meals; also, P1 mentioned enjoying this task in particular due to the use of multisensorial stimuli (e.g., during the “Foods” theme sessions, we combined fruit-based odors) and the set of songs played during sessions. As for P2, she initially resisted participation in our study, since she had no experience with technology. Nevertheless, at the end of the CCSP, P2 mentioned appreciating the themes and songs used, expressing her joy in recalling some of the stimuli we used, such as, for instance, the tool used by the milkman to carry the milk through the village. Overall, at the end of the intervention, we verified that both participants improved their ability to interact with Musiquence, meaning there has been a learning effect throughout sessions.
Our usability results are consistent with the findings of Ferreira et al. (2018). The authors performed a study with IwD to test the feasibility of Musiquence in an AR format and found that the participants enjoyed performing the different activities and were able to autonomously finish all of them [32]. Moreover, the same authors studied the usability of this tool with healthcare professionals, who reported that the platform was easy to use [33].
5. Conclusions
Overall, involving formal caregivers and IwD had a significantly positive impact on the development of our CCSP. By involving IwD in the content design process, we have promoted their engagement and participation in the CCSP. Customizing cognitive stimulation content according to IwD needs, preferences, and previous experiences is of utmost relevance, as we believe it can enhance the effects of reminiscence. By including familiar and meaningful content, we expect to promote broader cognitive, behavioral, and quality of life benefits, and also to potentiate participation and engagement of IwD in the CCSP.
We consider that this participatory design approach successfully achieved its goals by creating a CCSP for IwD to be implemented in the ARM, providing us with a set of guidelines on how to perform this type of participatory design approach with this specific clinical population. So far, IwD that have integrated our longitudinal study have provided positive feedback on the CCSP content, and Musiquence’s usability.
Nonetheless, we believe that it could be interesting to implement our participatory design approach with a larger sample of formal caregivers and IwD, as well as including informal caregivers (such as family members), in order to obtain additional information on IwD’s interests and preferences Additionally, it is important to consider that our CCSP was based on interests and preferences of IwD aged between 55 and 86 years living in the ARM. Therefore, our CCSP is not recommended to be implemented with individuals outside of the age range or living outside of this geographic region.
Finally, one of our major limitations was not finding similar studies. We believe that including IwD in the content selection and design process may enhance their adherence to the tasks and, consequently, potentiate the gains of the cognitive intervention.
Author Contributions
Conceptualization, M.S., J.C., L.F., A.L.F. and S.B.i.B.; methodology, M.S., J.C. and A.L.F.; validation: S.B.i.B.; formal analysis, M.S.; investigation, M.S., J.C. and L.F.; resources, S.B.i.B.; data curation, M.S.; writing—original draft preparation, M.S. and J.C.; writing—review and editing, L.F., A.L.F. and S.B.i.B.; visualization, M.S., J.C., L.F., A.L.F. and S.B.i.B.; supervision, A.L.F. and S.B.i.B.; project administration, S.B.i.B.; funding acquisition, S.B.i.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Portuguese national funding agency for science, research, and technology through NOVA LINCS, grant number UIDB/04516/2020, BRaNT project PTDC/CCI-COM/31046/2017 and Ph.D. scholarship SFRH/BD/145919/2019; by LARSyS (PTDC/CCI-COM/31046/2017); and by INTERREG program MAC2/1.1b/352.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the University of Madeira ethics department (02/2020). All participants, or their legal representatives, gave their informed consent.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Mental Health of Older Adults. Available online: https://www.who.int/news-room/fact-sheets/detail/mental-health-of-older-adults (accessed on 9 November 2022).
- Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 9 November 2022).
- National Collaborating Centre for Mental Health; Britain, G. Dementia: The NICE-SCIE Guideline on Supporting People with Dementia and Their Carers in Health and Social Care; British Psychological Society and Royal College of Psychiatrists: London, UK, 2007. [Google Scholar]
- Ravdin, L.D.; Katzen, H.L. Handbook on the Neuropsychology of Aging and Dementia; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Woods, B. Dementia Care: Progress and Prospects. J. Ment. Health 1995, 4, 115–124. [Google Scholar] [CrossRef]
- Spector, A.; Woods, B.; Orrell, M. Cognitive Stimulation for the Treatment of Alzheimer’s Disease. Expert Rev. Neurother. 2008, 8, 751–757. [Google Scholar] [CrossRef] [PubMed]
- Bahar-Fuchs, A.; Clare, L.; Woods, B. Cognitive Training and Cognitive Rehabilitation for Mild to Moderate Alzheimer’s Disease and Vascular Dementia. Cochrane Database Syst. Rev. 2013, 6, 1–73. [Google Scholar] [CrossRef]
- Woods, B.; Aguirre, E.; Spector, A.E.; Orrell, M. Cognitive Stimulation to Improve Cognitive Functioning in People with Dementia. Cochrane Database Syst. Rev. 2012, 2, 1–56. [Google Scholar] [CrossRef] [PubMed]
- Aguirre, E.; Hoare, Z.; Streater, A.; Spector, A.; Woods, B.; Hoe, J.; Orrell, M. Cognitive Stimulation Therapy (CST) for People with Dementia—Who Benefits Most? Int. J. Geriatr. Psychiatry 2013, 28, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Spector, A.; Orrell, M.; Davies, S.; Woods, B. Can Reality Orientation Be Rehabilitated? Development and Piloting of an Evidence-Based Programme of Cognition-Based Therapies for People with Dementia. Neuropsychol. Rehabil. 2001, 11, 377–397. [Google Scholar] [CrossRef]
- Spector, A.; Thorgrimsen, L.; Woods, B.O.B.; Royan, L.; Davies, S.; Butterworth, M.; Orrell, M. Efficacy of an Evidence-Based Cognitive Stimulation Therapy Programme for People with Dementia: Randomised Controlled Trial. Br. J. Psychiatry 2003, 183, 248–254. [Google Scholar] [CrossRef]
- Hall, L.; Orrell, M.; Stott, J.; Spector, A. Cognitive Stimulation Therapy (CST): Neuropsychological Mechanisms of Change. Int. Psychogeriatr. 2013, 25, 479–489. [Google Scholar] [CrossRef]
- Krell-Roesch, J.; Syrjanen, J.A.; Vassilaki, M.; Machulda, M.M.; Mielke, M.M.; Knopman, D.S.; Kremers, W.K.; Petersen, R.C.; Geda, Y.E. Quantity and Quality of Mental Activities and the Risk of Incident Mild Cognitive Impairment. Neurology 2019, 93, e548–e558. [Google Scholar] [CrossRef]
- Baird, A.; Samson, S. Memory for Music in Alzheimer’s Disease: Unforgettable? Neuropsychol. Rev. 2009, 19, 85–101. [Google Scholar] [CrossRef]
- Huber, A.; Oppikofer, S.; Meister, L.; Langensteiner, F.; Meier, N.; Seifert, A. Music & Memory: The Impact of Individualized Music Listening on Depression, Agitation, and Positive Emotions in Persons with Dementia. Act. Adapt. Aging 2021, 45, 70–84. [Google Scholar]
- Van der Steen, J.T.; Smaling, H.J.; Van der Wouden, J.C.; Bruinsma, M.S.; Scholten, R.J.; Vink, A.C. Music-Based Therapeutic Interventions for People with Dementia. Cochrane Database Syst. Rev. 2018, 7, 1–99. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, L.D.A.; Cavaco, S.; Badia, S.B.i. Musiquence: A Framework to Customize Music and Reminiscence Cognitive Stimulation Activities for the Dementia Population. In Proceedings of the 2019 5th Experiment International Conference (exp. at’19), Funchal, Portugal, 12–14 June 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 359–364. [Google Scholar]
- Marin, A.G.; Seiciu, P.L.; Popescu, A.M.; Bighea, A.; Berteanu, M. Technology for Post-Stroke Cognitive Rehabilitation. Int. J. Pharma Med. Biol. Sci. 2015, 4, 146. [Google Scholar]
- Ferreira, L.D.A.; Ferreira, H.; Cavaco, S.; Cameirão, M.; Badia, S.B.i. User Experience of Interactive Technologies for People with Dementia: Comparative Observational Study. JMIR Serious Games 2020, 8, e17565. [Google Scholar] [CrossRef]
- Span, M.; Hettinga, M.; Groen-van de Ven, L.; Jukema, J.; Janssen, R.; Vernooij-Dassen, M.; Eefsting, J.; Smits, C. Involving People with Dementia in Developing an Interactive Web Tool for Shared Decision-Making: Experiences with a Participatory Design Approach. Disabil. Rehabil. 2018, 40, 1410–1420. [Google Scholar] [CrossRef]
- Tanner, D. Co-Research with Older People with Dementia: Experience and Reflections. J. Ment. Health 2012, 21, 296–306. [Google Scholar] [CrossRef]
- Félix, S.B.; Ribeiro, O.; Maia, H. Personalized Cognitive Stimulation through Personhood: A Case Report on Dementia Diagnosis Acceptance and Therapeutic Engagement. Clin. Gerontol. 2020, 43, 233–239. [Google Scholar] [CrossRef]
- Suijkerbuijk, S.; Nap, H.H.; Cornelisse, L.; IJsselsteijn, W.A.; De Kort, Y.A.; Minkman, M. Active Involvement of People with Dementia: A Systematic Review of Studies Developing Supportive Technologies. J. Alzheimer’s Dis. 2019, 69, 1041–1065. [Google Scholar] [CrossRef]
- Hendriks, N.; Truyen, F.; Duval, E. Designing with Dementia: Guidelines for Participatory Design Together with Persons with Dementia. In Proceedings of the IFIP Conference on Human-Computer Interaction, Cape Town, South Africa, 2–6 September 2013; Springer: Berlin/Heidelberg, Germany, 2013; pp. 649–666. [Google Scholar]
- Lindsay, S.; Brittain, K.; Jackson, D.; Ladha, C.; Ladha, K.; Olivier, P. Empathy, Participatory Design and People with Dementia. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Austin, TX, USA, 5–10 May 2012; pp. 521–530. [Google Scholar]
- Hendriks, N.; Huybrechts, L.; Wilkinson, A.; Slegers, K. Challenges in Doing Participatory Design with People with Dementia. In Proceedings of the 13th Participatory Design Conference: Short Papers, Industry Cases, Workshop Descriptions, Doctoral Consortium Papers, and Keynote Abstracts-Volume 2, Windhoek, Namibia, 6–10 October 2014; pp. 33–36. [Google Scholar]
- Wang, G.; Marradi, C.; Albayrak, A.; van der Cammen, T.J. Co-Designing with People with Dementia: A Scoping Review of Involving People with Dementia in Design Research. Maturitas 2019, 127, 55–63. [Google Scholar] [CrossRef]
- Johannessen, A.; Engedal, K.; Haugen, P.K.; Dourado, M.C.N.; Thorsen, K. “To Be, or Not to Be”: Experiencing Deterioration among People with Young-Onset Dementia Living Alone. Int. J. Qual. Stud. Health Well-Being 2018, 13, 1490620. [Google Scholar] [CrossRef]
- Grobosch, S.; Wolf, F.; Juchems, S.; Kuske, S. Emotional Safety of People Living with Dementia: A Systematic Review. J. Ment. Health 2020, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Spector, A.; Orrell, M.; Woods, B. Cognitive Stimulation Therapy (CST): Effects on Different Areas of Cognitive Function for People with Dementia. Int. J. Geriatr. Psychiatry 2010, 25, 1253–1258. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”: A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Andrade Ferreira, L.D.; Cavaco, S.; Bermúdez i Badia, S. Feasibility Study of an Augmented Reality System for People with Dementia; The Eurographics Association: Eindhoven, The Netherlands, 2018; pp. 141–148. [Google Scholar] [CrossRef]
- Ferreira, L.; Cavaco, S.; Badia, S.B.I. A Usability Study with Healthcare Professionals of a Customizable Framework for Reminiscence and Music Based Cognitive Activities for People with Dementia. In Proceedings of the 23rd Pan-Hellenic Conference on Informatics, Nicosia, Cyprus, 28–30 November 2019; pp. 16–23. [Google Scholar]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).