Abstract
The inclusion of both maxillary permanent central incisors is uncommon. This condition compromises face aesthetics, phonation and masticatory function. Therefore, early diagnosis is essential to avoid complications and failures. There are various reasons for inclusion, but supernumerary teeth are the leading cause. Early causes of removal and rapid expansion of the palate determine a high probability of success with the spontaneous eruption of the impacted elements. However, it is often necessary to proceed with a surgical–orthodontic treatment. The inclination of teeth in relation to the midline and the root maturation degree determine prognosis and therapeutic timing. In this case report, the orthopantomogram (OPG) X-ray of a 9-year-old boy revealed two impacted supernumerary teeth in the anterior maxillary region, preventing the eruption of the permanent upper central incisors. The impacted supernumerary teeth were surgically removed at different times. A straight wire multibrackets technique associated with a fixed palatal appliance was used. The palatal appliance featured an osteomucous resin support at the level of the retroincisal papilla. Subsequently, surgical exposure was carried out using the closed eruption technique and elastic traction, bringing 11 and 21 back into the arch.
1. Introduction
Eruption anomalies are classified into position-related disorders (ectopic eruption and transpositions) and timing-related disorders (premature eruption, delayed eruption or impaction). These anomalies are also linked to age, sex, race or ethnicity. Both root developmental staging and patient age are used as criteria to diagnose prematurity or delayed eruption [1,2,3].
Eruption disorders are more frequent in the upper arch (69.9%) and the area of the incisors (51.2%). Furthermore, in 20.5% of cases, first-degree relatives present the same issue [4,5].
Impaction of the upper central incisors is a rare occurrence (0.06–0.12%), more frequent in men than in women (1.5:1) [4,6].
Traumatic and obstructive causes are the main factors related to impacted teeth [7].
Dental trauma at a young age could damage the non-erupted permanent tooth germ, reduce root development, and change eruption direction. This can lead to dilacerated tooth development with a high risk of uneruption without an orthognathic–surgical therapy [8,9].
Necrosis or ankylosis of a deciduous tooth and the simultaneous presence of systemic pathologies (endocrine diseases, cleidocranial dysostosis) can also determine dental inclusions [10,11].
The main obstructive causes are: odontomas (complex or compound); follicular cysts; thick mucosa; bone tissue formed as a result of the early extraction of a deciduous tooth; and supernumerary teeth [8].
The most common obstructive cause is determined by supernumerary teeth (ST), 77.8% of the ST are found in the maxilla, and 97.2% are in the frontal region. In the anterior maxillary region, the presence of one or more supernumerary teeth along the midline (1.5% to 3.5%) hinders the eruption of the incisors (28% to 60%) [5,12,13,14,15,16].
Although the percentage of upper central incisors uneruption or inclusion is low, its occurrence causes an aesthetic, phonetic and functional discomfort to the patient, arousing parents’ concern [7,14].
Parents of an impacted incisor affected child are usually motivated to seek an earlier orthodontic treatment than parents of a child with other orthodontic problems [8,17,18].
The diagnosis of impacted incisors is based on the clinical examination that ascertains and identifies the retained tooth. Palpating the corresponding alveolar area (both palatal and vestibular), a painless, incompressible, fibromucosal bump can be appreciated [19].
The diagnosis needs to be completed by radiological examinations:
- (1)
- Intraoral X-rays with periapical and occlusal projections confirm the presence, position and/or anomaly of the retained maxillary incisors and any underlying developmental anomaly or pathology. The buccolingual position of the non-erupted tooth can be localized using horizontal or vertical parallax.
- (2)
- Ortopanthomography X-ray (OPG X-ray) to evaluate the problem in relation to the entire arch, adjacent tooth and the staging of the eruption of the other dental elements.
- (3)
- Latero-Lateral Teleradiography (LLT) of the head with cephalometric trace to assess the height and inclination of the crown and root of the impacted tooth.
- (4)
- Cone-Beam Computed Tomography (CBCT) for a three-dimensional evaluation of impacted elements and surrounding structures.
All these data allow us to correctly plan the treatment and the optimal direction of traction in order to have a correct extrusion of the impacted tooth with adequate periodontal support [19,20,21].
Early treatment is essential because the non-erupted maxillary central incisor can cause various issues:
- (1)
- Compromission of the aesthetic aspect, phonation and alveolar ridge formation.
- (2)
- Increase of adjacent teeth tip, reducing the space for the non-erupted incisor.
- (3)
- Alteration of the eruptive path (deviation and delay) of the ipsilateral canine [10].
The treatment options for impacted incisors include:
- (1)
- Extraction of the impacted tooth followed by a prosthetic rehabilitation [22,23,24];
- (2)
- Extraction and repositioning of the lateral incisor in place of the central incisor with mesial canine and premolar movement, then coronoplasty;
- (3)
- Surgical-orthodontic recovery of the incisor [25,26].
Most of the patients requiring impacted central incisors treatment are less than 12 years old; for this reason, the prosthetic solution is not suitable. The extraction of the affected tooth would lead to a severe loss of alveolar bone, compromising the future insertion of an implant [18]. On the other side, the surgical–orthodontic solution allows complete alignment of natural teeth and does not require the creation of a prosthesis [25,26].
Treatment success rates depend on several factors:
- (1)
- The angle between impacted incisor and midline (if greater than 20 degrees, there are greater difficulties in treatment and a worse prognosis);
- (2)
- The level of the crown of the impacted tooth compared to the eruptive age;
- (3)
- The distance of the impacted incisor from the occlusal plane [8,25,27,28].
A study has verified that performing a rapid expansion with a Rapid Maxillary Expander (RME) immediately after the obstacle removal leads to an 82% chance of problem resolution with the eruption of the impacted element after 6–7 months from the obstacle removal, while without applying the RME, the percentages are reduced by 39% [25,29,30].
Several surgical techniques are commonly used to expose the maxillary teeth. One technique is the apical repositioning flap. It consists of the apical repositioning of a raised full-thickness-flap above the included tooth, leaving the element uncovered. Another technique is the closed eruption. It involves lifting a full-thickness flap, fixing an orthodontic bracket on the tooth surface, and then completely covering the tooth and bracket with tissue. These techniques offer some advantages when pulling impacted teeth [10,31,32].
The apically repositioned flap technique allows prompt reattachment of the bracket if unintentional detachment occurs. However, the closed eruption technique provides the most aesthetically pleasing result. This technique is most reliable when considering aesthetic and periodontal health. Vermette et al., recommended using the closed eruption technique when the tooth is in the center of the socket or when it is high, near the nasal spine. In these cases, the periodontal state of the exposed teeth after orthodontic treatment usually revealed an acceptable gingival profile and good adherent gingiva, an increase in bone level on the mesial, vestibular and distal surfaces, requiring no further mucogingival surgery [33].
Since many variables affect the recovery of an included tooth in a child after removing the supernumerary elements or the odontoma, most studies believe orthodontic treatment is necessary rather than waiting for the spontaneous eruption [8,25,34].
The treatment of impacted central incisors requires a different approach, and it is longer and more complicated, with the resolution of extraction with subsequent prosthetic rehabilitation as a valid alternative [35].
According to the latest literature data, the approach for this type of issue is mainly oriented to surgical–orthodontic treatments [36,37].
Undoubtedly, the best treatment choice is conservative, and it requires careful planning and close collaboration between orthodontists, oral surgeons and periodontists. Studies report that the prognosis of orthodontic–surgical treatment of impacted incisors is good, and failures occur when the etiology of the inclusion is dilaceration [36].
The treatment is relatively long, approximately two years, and is influenced by the initial height of the tooth included in the jaw [38].
2. Case Report
A 15-year and 6-months-old patient (F.F.) comes to our attention.
2.1. Clinical History
The patient had previously undergone orthodontic treatment since the age of 9, the presence of persistent deciduous (51 and 61), and two ST were found in areas 11 and 21 preventing their eruption (Figure 1).

Figure 1.
F.F. 9y, OPG X-ray initial clinical evaluation with persistent deciduous 51–61, supernumerary teeth and impacted incisors 11–21.
The two ST were removed at different times (10-years-old and 13-year-old), and a late rapid expansion (14-year-old) was performed without any improvement (Figure 2 and Figure 3).

Figure 2.
F.F. 13y OPG X-ray presence of one supernumerary tooth and impacted incisors 11–21.

Figure 3.
F.F. 14y OPG X-ray after RME.
2.2. Clinical Exams and Diagnosis
Patient in good health. Clinical evaluation revealed the absence of teeth 11 and 21.
The orthodontic situation was re-evaluated with new intraoral photos and X-rays (Figure 4 and Figure 5).

Figure 4.
(A–E) F.F. 15y 6m intraoral photos at the beginning of treatment: right (A), front (B), and left (C) view; occlusal upper (D), and occlusal lower (E) view.
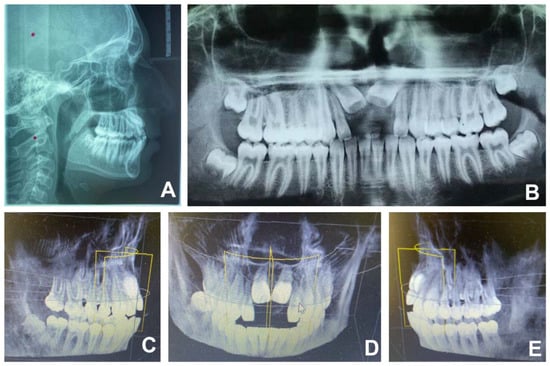
Figure 5.
(A–E) F.F. 15y 6m initial radiographic documentation: LLT (A), OPG X-ray (B), CBCT right (C), front (D), and left (E) view.
The patient had molar and canine class I, dental and skeletal malocclusion, counterclockwise mandibular growth with a tendency to brachycephalic growth, good transverse dimension arch and slight lower crowding. To confirm the position and relationship with adjacent structures, CBCT was recommended. The position of the two upper incisors was assessable with CBCT and LLT.
The 11 and 21 presented a very apical position (immediately under the anterior nasal spine) and a significant inclination (51.2°) (Figure 6 and Table 1).
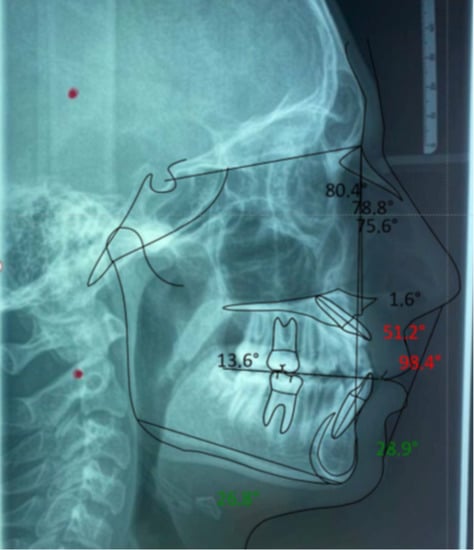
Figure 6.
F.F. 15y 6m Steiner’s cephalometric tracing.

Table 1.
F.F. 15y 6m Steiner’s cephalometric analysis.
The patient wore a removable prosthetic device for aesthetic and functional purposes to replace elements 21 and 11 (Figure 7).
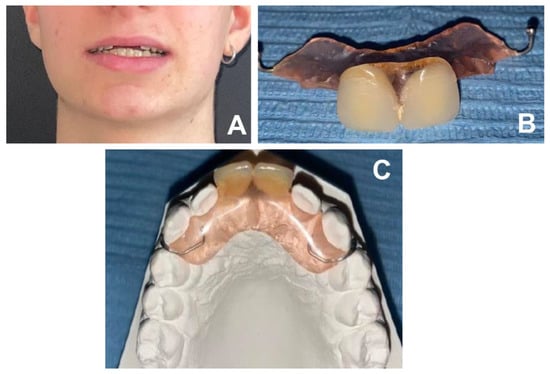
Figure 7.
(A–C) removable prosthetic device for aesthetic and functional purposes to replace elements 21 and 11: patient frontal smile (A); prosthetic device frontal view (B); cast model and prosthetic device occlusal view (C).
2.3. Therapeutic Plan
An orthodontic–surgical therapy that aimed to pull down the two elements and bring them into a more occlusal position was adopted. Initially, the elements of the upper arch were aligned with a fixed straight-wire multibrackets technique, which also made it possible to apply a pontic in areas 11 and 21, not to compromise the aesthetic and functional aspects of the patient. After osteotomy, a full-thickness flap was made to access the crowns using a scalpel. After dental exposure, two eyelets were bonded, and elastic tractions were applied. The flap was then positioned to cover the teeth and buttons according to the closed eruption technique. On 16 and 26, a fixed palatal appliance was cemented, with supports on 14/24 and a retroincisive papillae osteomucosal resin support. This was done to allow the elements to be pulled without causing unwanted movement of adjacent elements due to the action-reaction effect. The front resin portion was equipped with three loops to allow elastic traction in several directions (Figure 8).
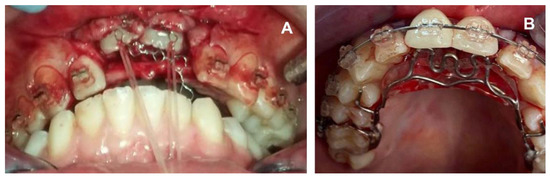
Figure 8.
(A,B) post-operative view before device placement (A); fixed palatal appliance with three loops and central incisors pontic (B).
After ten months, the upper incisors emerged from the gingiva and reached a more occlusal position. A further diode laser uncovering and modelling of the mucosa was carried out. A 0.019 × 0.025 steel arch was used as anchorage while central incisors were engaged with a 0.014 thermal nickel-titanium (NiTi) arch (Figure 9).

Figure 9.
Upper 0.019 × 0.025 steel arch with a 0.014 thermal nickel-titanium.
Subsequently, the prosthetic elements were removed, and the eyelets were replaced with metal brackets. This allowed the extrusion with the 0.014 thermal NiTi arch properly engaged (Figure 10).

Figure 10.
(A–C): Central incisors with eyelets (A); central incisors with brackets (B); central incisors extrusion with 0.014 thermal NiTi arch properly engaged (C).
After three months, the incisors were further extruded and almost aligned with the other elements of the upper arch. Thus, it was possible to engage the 0.014 thermal NiTi base arch. The metal brackets on 11 and 21 have been further replaced with aesthetic twin brackets.
The fixed orthodontic treatment was then also started in the lower arch.
3. Results
After 24 months of treatment (including COVID-19 lockdown periods), 11 and 21 were correctly positioned in the occlusal plane with good bone and periodontal support.
The patient improved the vertical dimension, the upper lip support and the smile aesthetics (Figure 11, Figure 12 and Figure 13).
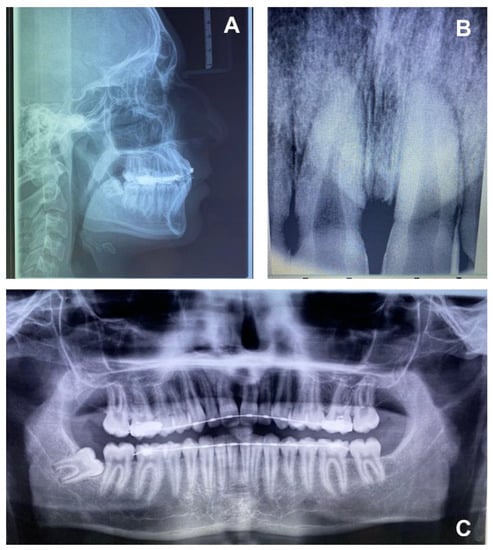
Figure 11.
(A–C) F.F. 17y 7m final radiographic documentation: LLT (A); central incisors intraoral X-ray (B); OPG X-ray (C).
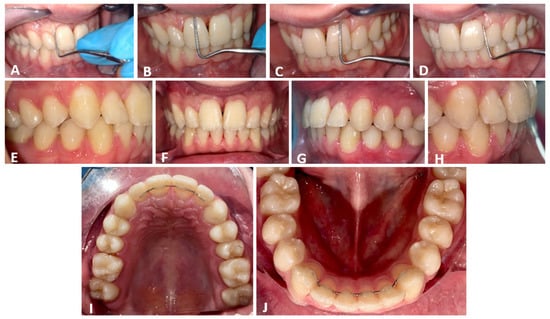
Figure 12.
(A–J) F.F. 17y 7m final intraoral photos: 11 periodontal probing (A,B); 21 periodontal probing (C,D); right (E), front (F) and left (G) view; overjet view (H); occlusal upper (I) and occlusal lower (J) view.
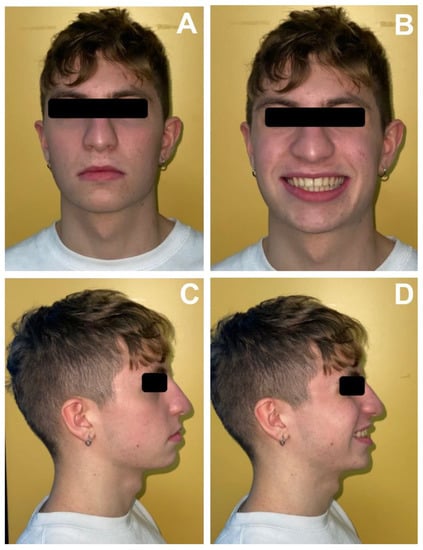
Figure 13.
(A–D) F.F. 17y 7m extraoral photos at the end of the treatment: frontal view closed lips (A); frontal view smiling (B); facial profile with closed lips (C); facial profile smiling (D).
4. Discussion
Careful treatment planning of impacted incisors is crucial for a favorable prognosis. It is always multidisciplinary as it requires the intervention of an orthodontist and an oral surgeon [6,16,39].
The choice of the orthodontic–surgical treatment plan with a closed eruption technique and elastic tractions was guided by several factors.
First of all, the patient’s age (adolescent) was considered: the patient wore a removable prosthesis that replaced the two missing incisors with significant discomfort [5,40].
Analyzing the patient’s clinical history, it emerged that no extrusion movement of the impacted incisors had occurred despite the patient having already removed the two supernumeraries in different periods and had already performed a rapid, although the late, expansion of the palate (14-year-old) [8]. The alternative solution of extraction of impacted teeth and implant therapy was then offered [26].
LLT and CBCT confirmed the unfavorable inclination and height of the crowns. The roots were already wholly developed, so there was no eruptive thrust. Furthermore, no lacerations were reported [33,41]. Parents were also informed of the possibility of treatment failure.
After aligning the upper arch with the straight-wire technique, a full-thickness flap, palatal bone removal and elastic traction with closed eruption were performed. The occlusal plane was stabilized by a molar cemented palatal device, with first upper premolars support arms and an osteo-mucosal support. Otherwise, it could have been affected by the reaction forces caused by extrusion forces [42].
The device choice has been made to allow the patient to have pontics in zone 11–21 during the treatment and not to have discomfort in social life.
During the OPG X-ray and intraoral X-ray examination, good palatal, mesial and distal bone margins were highlighted with more significant resorption on the vestibular side [2,43,44,45,46,47].
The roots were shorter, also in relation to the adjacent lateral incisors. According to the literature, the reabsorption may be due to the initial impediment caused by supernumeraries mobilization and to the orthodontic eruption movement [2].
The treatment lasted 25 months with several periods of inactivation because the patient was treated during the COVID-19 pandemic, including the first lockdown. The elements were correctly positioned on the occlusal plane with an excellent gingival margin [48,49,50].
Upper and lower restraint with retainers and Essix was adopted [51].
5. Conclusions
An early and accurate diagnosis supported by clinical and radiological examinations, such as OPG X-ray and CBCT, is essential.
It is crucial to evaluate the predictive eruption factors that influence the treatment plan, such as: age of the patient, history, compliance, distance from the occlusal plane, vertical position of unerupted incisors and inclination in relation to the midline.
A complication during the tooth eruption could adversely affect the occlusion development and potentially burden the child’s psychological evolution.
The early orthodontic interceptive treatment with obstacle removal and an orthopedic expansion with RME is fundamental.
Elastic tractions with the closed eruption technique for occlusal repositioning is preferred. This approach improves the intraosseous position and the mucogingival condition of the retained tooth.
In general, surgical–orthodontics treatment of impacted incisors has a good chance of success, but it is relatively time-consuming.
It is necessary to inform the patients and their parents of the failure risk and the increased treatment time, especially in the presence of impacted incisors in a very high alveolar position.
Author Contributions
Conceptualization, F.I., A.D.I., A.M.I., D.D.V., G.D., A.S., S.C., G.C., F.L. and A.P.; methodology, A.D.I., M.G., F.C., L.N., A.M., A.C., G.C., F.P., S.C. and M.C.; software, I.R.B., A.P., F.C., S.C., D.G., A.M., F.C. and G.D.; validation, F.I., F.L., F.C.,V.S., L.N., G.D., A.D.I., A.M.I. and A.S.; formal analysis, A.M.I., F.L., V.M.P., D.D.V., A.D.I., B.R. and G.M.; investigation, G.M., G.D., A.D.I., F.L., A.M.I., A.P., S.C., A.S. and F.I.; resources, A.M.I., S.C., A.P., G.D., A.D.I., F.I., I.R.B. and G.M.; data curation, G.D., F.C., F.L., M.G., A.M., G.C., M.G., F.I., D.D.V. and G.M.; writing—original draft preparation, A.D.I., A.M.I., G.D., M.G., A.S., F.C., F.L. and F.I.; writing—review and editing, F.I., F.L., D.D.V., G.M., M.G., A.S., V.S. and G.D.; visualization, F.L., A.S. and I.R.B.; supervision, M.G., D.D.V., F.I., A.D.I. and F.L.; project administration, F.I., G.D., G.M., A.P., G.C., S.C. and V.M.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The present clinical study was based in the University of Bari (Italy), in full accordance with ethical principles, including the World Medical Association Declaration of Helsinki and the additional requirements of Italian law. Furthermore, the University of Bari, Italy, classified the study to be exempt from ethical review as it carries only negligible risk and involves the use of existing data that contain only non-identifiable data about human beings. The patient signed a written informed consent form.
Informed Consent Statement
Informed consent was obtained from the subjects involved in the study. Written informed consent has been obtained from the patient and his parents to publish this paper.
Data Availability Statement
All experimental data to support the findings of this study are available contacting the corresponding author upon request.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| OPG | Orthopantomography X-ray |
| RME | Rapid Maxillary Expander |
| LLT | Latero-Lateral Teleradiography |
| CBCT | Cone Beam Computed Tomography |
| ST | Supernumerary teeth |
| FF | Patient name |
References
- Huber, K.; Suri, L.; Taneja, P. Eruption Disturbances of the Maxillary Incisors:A Literature Review. J. Clin. Pediatric Dent. 2008, 32, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Žarovienė, A.; Grinkevičienė, D.; Trakinienė, G.; Smailienė, D. Post-Treatment Status of Impacted Maxillary Central Incisors Following Surgical-Orthodontic Treatment: A Systematic Review. Medicina 2021, 57, 783. [Google Scholar] [CrossRef] [PubMed]
- Cirulli, N.; Ballini, A.; Cantore, S.; Farronato, D.; Inchingolo, F.; Dipalma, G.; Gatto, M.R.; Alessandri Bonetti, G. Mixed Dentition Space Analysis of A Southern Italian Population: New Regression Equations for Unerupted Teeth. J. Biol. Regul. Homeost. Agents 2015, 29, 515–520. [Google Scholar] [PubMed]
- Betts, N.J.; Vanarsdall, R.L.; Barber, H.D.; Higgins-Barber, K.; Fonseca, R.J. Diagnosis and Treatment of Transverse Maxillary Deficiency. Int. J. Adult Orthodon. Orthognath. Surg. 1995, 10, 75–96. [Google Scholar] [PubMed]
- Gábris, K.; Tarján, I.; Fábián, G.; Kaán, M.; Szakály, T.; Orosz, M. Frequency of supernumerary teeth and possibilities of treatment. Fogorv. Sz. 2001, 94, 53–57. [Google Scholar] [PubMed]
- Jain, S.; Raza, M.; Sharma, P.; Kumar, P. Unraveling Impacted Maxillary Incisors: The Why, When, and How. Int. J. Clin. Pediatr. Dent. 2021, 14, 149–157. [Google Scholar] [CrossRef]
- Brin, I.; Zilberman, Y.; Azaz, B. The Unerupted Maxillary Central Incisor: Review of Its Etiology and Treatment. ASDC J. Dent. Child. 1982, 49, 352–356. [Google Scholar]
- Chaushu, S.; Becker, T.; Becker, A. Impacted Central Incisors: Factors Affecting Prognosis and Treatment Duration. Am. J. Orthod. Dentofac. Orthop. 2015, 147, 355–362. [Google Scholar] [CrossRef]
- Laudadio, C.; Inchingolo, A.D.; Malcangi, G.; Limongelli, L.; Marinelli, G.; Coloccia, G.; Montenegro, V.; Patano, A.; Inchingolo, F.; Bordea, I.R.; et al. Management of Anterior Open-Bite in the Deciduous, Mixed and Permanent Dentition Stage: A Descriptive Review. J. Biol. Regul. Homeost. Agents 2021, 35, 271–281. [Google Scholar] [CrossRef]
- Chaushu, S.; Zilberman, Y.; Becker, A. Maxillary Incisor Impaction and Its Relationship to Canine Displacement. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 144–150; discussion 150. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Palmieri, G.; et al. Genetic Pattern, Orthodontic and Surgical Management of Multiple Supplementary Impacted Teeth in a Rare, Cleidocranial Dysplasia Patient: A Case Report. Medicina 2021, 57, 1350. [Google Scholar] [CrossRef]
- Das, D.; Misra, J. Surgical Management of Impacted Incisors in Associate with Supernumerary Teeth: A Combine Case Report of Spontaneous Eruption and Orthodontic Extrusion. J. Indian Soc. Pedod. Prev. Dent. 2012, 30, 329. [Google Scholar] [CrossRef]
- Alsweed, A.A.; Al-sughier, Z. Surgical Management of Unerupted Permanent Maxillary Central Incisors Due to Presence of Two Supernumerary Teeth. Int. J. Clin. Pediatr. Dent. 2020, 13, 421–424. [Google Scholar] [CrossRef]
- Zilberman, Y.; Malron, M.; Shteyer, A. Assessment of 100 Children in Jerusalem with Supernumerary Teeth in the Premaxillary Region. ASDC J. Dent. Child. 1992, 59, 44–47. [Google Scholar]
- Rajab, L.D.; Hamdan, M.A.M. Supernumerary Teeth: Review of the Literature and a Survey of 152 Cases. Int. J. Paediatr. Dent. 2002, 12, 244–254. [Google Scholar] [CrossRef]
- Šarac, Z.; Zovko, R.; Cvitanović, S.; Goršeta, K.; Glavina, D. Fusion of Unerupted Mesiodens with a Regular Maxillary Central Incisor: A Diagnostic and Therapeutic Challenge. Acta Stomatol. Croat. 2021, 55, 325–331. [Google Scholar] [CrossRef]
- Marinelli, G.; Inchingolo, A.D.; Inchingolo, A.M.; Malcangi, G.; Limongelli, L.; Montenegro, V.; Coloccia, G.; Laudadio, C.; Patano, A.; Inchingolo, F.; et al. White Spot Lesions in Orthodontics: Prevention and Treatment. A Descriptive Review. J. Biol. Regul. Homeost. Agents 2021, 35, 227–240. [Google Scholar] [CrossRef]
- Montenegro, V.; Inchingolo, A.D.; Malcangi, G.; Limongelli, L.; Marinelli, G.; Coloccia, G.; Laudadio, C.; Patano, A.; Inchingolo, F.; Bordea, I.R.; et al. Compliance of Children with Removable Functional Appliance with Microchip Integrated during Covid-19 Pandemic: A Systematic Review. J. Biol. Regul. Homeost. Agents 2021, 35, 365–377. [Google Scholar]
- Tanki, J.Z. Impacted Maxillary Incisors: Causes, Diagnosis and Management. IOSR-JDMS 2013, 5, 41–45. [Google Scholar] [CrossRef]
- Seehra, J.; Yaqoob, O.; Patel, S.; O’Neill, J.; Bryant, C.; Noar, J.; Morris, D.; Cobourne, M.T. National Clinical Guidelines for the Management of Unerupted Maxillary Incisors in Children. Br. Dent. J. 2018, 224, 779–785. [Google Scholar] [CrossRef]
- Cantore, S.; Ballini, A.; Farronato, D.; Malcangi, G.; Dipalma, G.; Assandri, F.; Garagiola, U.; Inchingolo, F.; De Vito, D.; Cirulli, N. Evaluation of an Oral Appliance in Patients with Mild to Moderate Obstructive Sleep Apnea Syndrome Intolerant to Continuous Positive Airway Pressure Use: Preliminary Results. Int. J. Immunopathol. Pharm. 2016, 29, 267–273. [Google Scholar] [CrossRef]
- Grassi, F.R.; Rapone, B.; Scarano Catanzaro, F.; Corsalini, M.; Kalemaj, Z. Effectiveness of Computer-Assisted Anesthetic Delivery System (StaTM) in Dental Implant Surgery: A Prospective Study. Oral Implant. 2017, 10, 381–389. [Google Scholar] [CrossRef]
- Corsalini, M.; Di Venere, D.; Carossa, M.; Ripa, M.; Sportelli, P. Comparative Clinical Study between Zirconium-Ceramic and Metal-Ceramic Fixed Rehabilitations. Oral Implantol. 2018, 11, 150–160. [Google Scholar]
- Lorusso, F.; Noumbissi, S.; Francesco, I.; Rapone, B.; Khater, A.G.A.; Scarano, A. Scientific Trends in Clinical Research on Zirconia Dental Implants: A Bibliometric Review. Materials 2020, 13, 5534. [Google Scholar] [CrossRef]
- Pavoni, C.; Franchi, L.; Laganà, G.; Baccetti, T.; Cozza, P. Management of Impacted Incisors Following Surgery to Remove Obstacles to Eruption: A Prospective Clinical Trial. Pediatr. Dent. 2013, 35, 364–368. [Google Scholar]
- Orthodontic Treatment of Impacted Teeth-Adrian Becker-John Wiley and Sons Ltd-| IBS. Available online: https://www.ibs.it/orthodontic-treatment-of-impacted-teeth-libro-inglese-adrian-becker/e/9781444336757 (accessed on 7 February 2022).
- Adina, S.; Dipalma, G.; Bordea, I.R.; Lucaciu, O.; Feurdean, C.; Inchingolo, A.D.; Septimiu, R.; Malcangi, G.; Cantore, S.; Martin, D.; et al. Orthopedic Joint Stability Influences Growth and Maxillary Development: Clinical Aspects. J. Biol. Regul. Homeost. Agents 2020, 34, 747–756. [Google Scholar] [CrossRef]
- Di Venere, D.; Nardi, G.M.; Lacarbonara, V.; Laforgia, A.; Stefanachi, G.; Corsalini, M.; Grassi, F.R.; Rapone, B.; Pettini, F. Early Mandibular Canine-Lateral Incisor Transposition: Case Report. Oral Implant. 2017, 10, 181–189. [Google Scholar] [CrossRef]
- Coloccia, G.; Inchingolo, A.D.; Inchingolo, A.M.; Malcangi, G.; Montenegro, V.; Patano, A.; Marinelli, G.; Laudadio, C.; Limongelli, L.; Di Venere, D.; et al. Effectiveness of Dental and Maxillary Transverse Changes in Tooth-Borne, Bone-Borne, and Hybrid Palatal Expansion through Cone-Beam Tomography: A Systematic Review of the Literature. Medicina 2021, 57, 288. [Google Scholar] [CrossRef] [PubMed]
- Cardarelli, D.F. Il trattamento funzionale elastodontico con apparecchi AMCOP: Funzione, estetica e postura. Dental Tribune, 3 July 2019. [Google Scholar]
- Özer, M.; Şener, I.; Bayram, M. Bilaterally Impacted Maxillary Central Incisors: Surgical Exposure and Orthodontic Treatment: A Case Report. J. Contemp. Dent. Pract. 2006, 7, 98–105. [Google Scholar] [CrossRef]
- Farronato, M.; Farronato, D.; Inchingolo, F.; Grassi, L.; Lanteri, V.; Maspero, C. Evaluation of Dental Surface after De-Bonding Orthodontic Bracket Bonded with a Novel Fluorescent Composite: In Vitro Comparative Study. Appl. Sci. 2021, 11, 6354. [Google Scholar] [CrossRef]
- Becker, A.; Brin, I.; Ben-Bassat, Y.; Zilberman, Y.; Chaushu, S. Closed-Eruption Surgical Technique for Impacted Maxillary Incisors: A Postorthodontic Periodontal Evaluation. Am. J. Orthod. Dentofac. Orthop. 2002, 122, 9–14. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Pede, C.D.; et al. The Efficacy of a New AMCOP® Elastodontic Protocol for Orthodontic Interceptive Treatment: A Case Series and Literature Overview. Int. J. Environ. Res. Public Health 2022, 19, 988. [Google Scholar] [CrossRef]
- Tsai, T.-P. Surgical Repositioning of an Impacted Dilacerated Incisor in Mixed Dentition. J. Am. Dent. Assoc. 2002, 133, 61–66. [Google Scholar] [CrossRef]
- Farronato, G.; Giannini, L.; Galbiati, G.; Maspero, C. A 5-Year Longitudinal Study of Survival Rate and Periodontal Parameter Changes at Sites of Dilacerated Maxillary Central Incisors. Prog. Orthod. 2014, 15, 3. [Google Scholar] [CrossRef][Green Version]
- Patianna, A.G.; Ballini, A.; Meneghello, M.; Cantore, S.; Inchingolo, A.M.; Dipalma, G.; Inchingolo, A.D.; Inchingolo, F.; Malcangi, G.; Lucchese, A.; et al. Comparison of Conventional Orthognathic Surgery and “Surgery-First” Protocol: A New Weapon against Time. J. Biol. Regul. Homeost. Agents 2019, 33, 59–67, DENTAL SUPPLEMENT. [Google Scholar]
- Ho, K.; Liao, Y. Predictors of Surgical-Orthodontic Treatment Duration of Unilateral Impacted Maxillary Central Incisors. Orthod. Craniofacial Res. 2011, 14, 175–180. [Google Scholar] [CrossRef]
- Maspero, C.; Cappella, A.; Dolci, C.; Cagetti, M.G.; Inchingolo, F.; Sforza, C. Is Orthodontic Treatment with Microperforations Worth It? A Scoping Review. Children 2022, 9, 208. [Google Scholar] [CrossRef]
- Corsalini, M.; Di Venere, D.; Sportelli, P.; Magazzino, D.; Ripa, M.; Cantatore, F.; Cagnetta, C.; Rinaldis, C.; Montemurro, N.; Giacomo, A.; et al. Evaluation of Prosthetic Quality and Masticatory Efficiency in Patients with Total Removable Prosthesis Study of 12 Cases. ORAL Implantol. 2018, 11, 230–240. [Google Scholar]
- Chew, M.T.; Ong, M.M.-A. Orthodontic-Surgical Management of an Impacted Dilacerated Maxillary Central Incisor: A Clinical Case Report. Pediatr. Dent. 2004, 26, 341–344. [Google Scholar]
- Vermette, M.E.; Kokich, V.G.; Kennedy, D.B. Uncovering Labially Impacted Teeth: Apically Positioned Flap and Closed-Eruption Techniques. Angle Orthod. 1995, 65, 23–32. [Google Scholar] [CrossRef]
- Quaglia, E.; Moscufo, L.; Corsalini, M.; Coscia, D.; Sportelli, P.; Cantatore, F.; Rinaldis, C.; Rapone, B.; Carossa, M.; Carossa, S. Polyamide vs Silk Su.utures in the Healing of Postextraction Sockets: A Split Mouth Study. ORAL Implantol. 2018, 11, 115–120. [Google Scholar] [CrossRef]
- Rapone, B.; Ferrara, E.; Corsalini, M.; Converti, I.; Grassi, F.R.; Santacroce, L.; Topi, S.; Gnoni, A.; Scacco, S.; Scarano, A.; et al. The Effect of Gaseous Ozone Therapy in Conjunction with Periodontal Treatment on Glycated Hemoglobin Level in Subjects with Type 2 Diabetes Mellitus: An Unmasked Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, E5467. [Google Scholar] [CrossRef]
- Grassi, F.R.; Grassi, R.; Rapone, B.; Alemanno, G.; Balena, A.; Kalemaj, Z. Dimensional Changes of Buccal Bone Plate in Immediate Implants Inserted through Open Flap, Open Flap and Bone Grafting and Flapless Techniques: A Cone-Beam Computed Tomography Randomized Controlled Clinical Trial. Clin. Oral Implant. Res. 2019, 30, 1155–1164. [Google Scholar] [CrossRef]
- Rapone, B.; Corsalini, M.; Converti, I.; Loverro, M.T.; Gnoni, A.; Trerotoli, P.; Ferrara, E. Does Periodontal Inflammation Affect Type 1 Diabetes in Childhood and Adolescence? A Meta-Analysis. Front. Endocrinol. 2020, 11, 278. [Google Scholar] [CrossRef]
- Rapone, B.; Ferrara, E.; Santacroce, L.; Cesarano, F.; Arazzi, M.; Liberato, L.D.; Scacco, S.; Grassi, R.; Grassi, F.R.; Gnoni, A.; et al. Periodontal Microbiological Status Influences the Occurrence of Cyclosporine-A and Tacrolimus-Induced Gingival Overgrowth. Antibiotics 2019, 8, 124. [Google Scholar] [CrossRef]
- Patano, A.; Cirulli, N.; Beretta, M.; Plantamura, P.; Inchingolo, A.D.; Inchingolo, A.M.; Bordea, I.R.; Malcangi, G.; Marinelli, G.; Scarano, A.; et al. Education Technology in Orthodontics and Paediatric Dentistry during the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 6056. [Google Scholar] [CrossRef]
- Cantore, S.; Ballini, A.; De Vito, D.; Martelli, F.S.; Georgakopoulos, I.; Almasri, M.; Dibello, V.; Altini, V.; Farronato, G.; Dipalma, G.; et al. Characterization of Human Apical Papilla-Derived Stem Cells. J. Biol. Regul. Homeost. Agents 2017, 31, 901–910. [Google Scholar]
- Ballini, A.; Cantore, S.; Fotopoulou, E.A.; Georgakopoulos, I.P.; Athanasiou, E.; Bellos, D.; Paduanelli, G.; Saini, R.; Dipalma, G.; Inchingolo, F. Combined Sea Salt-Based Oral Rinse with Xylitol in Orthodontic Patients: Clinical and Microbiological Study. J. Biol. Regul. Homeost. Agents 2019, 33, 263–268. [Google Scholar]
- Di Venere, D.; Pettini, F.; Nardi, G.M.; Laforgia, A.; Stefanachi, G.; Notaro, V.; Rapone, B.; Grassi, F.R.; Corsalini, M. Correlation between Parodontal Indexes and Orthodontic Retainers: Prospective Study in a Group of 16 Patients. Oral Implantol. 2017, 10, 78. [Google Scholar] [CrossRef]













Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).