
Discomfort Glare Perception by Drivers—Establishing a Link between Subjective and Psychophysiological Assessment



Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Ethics
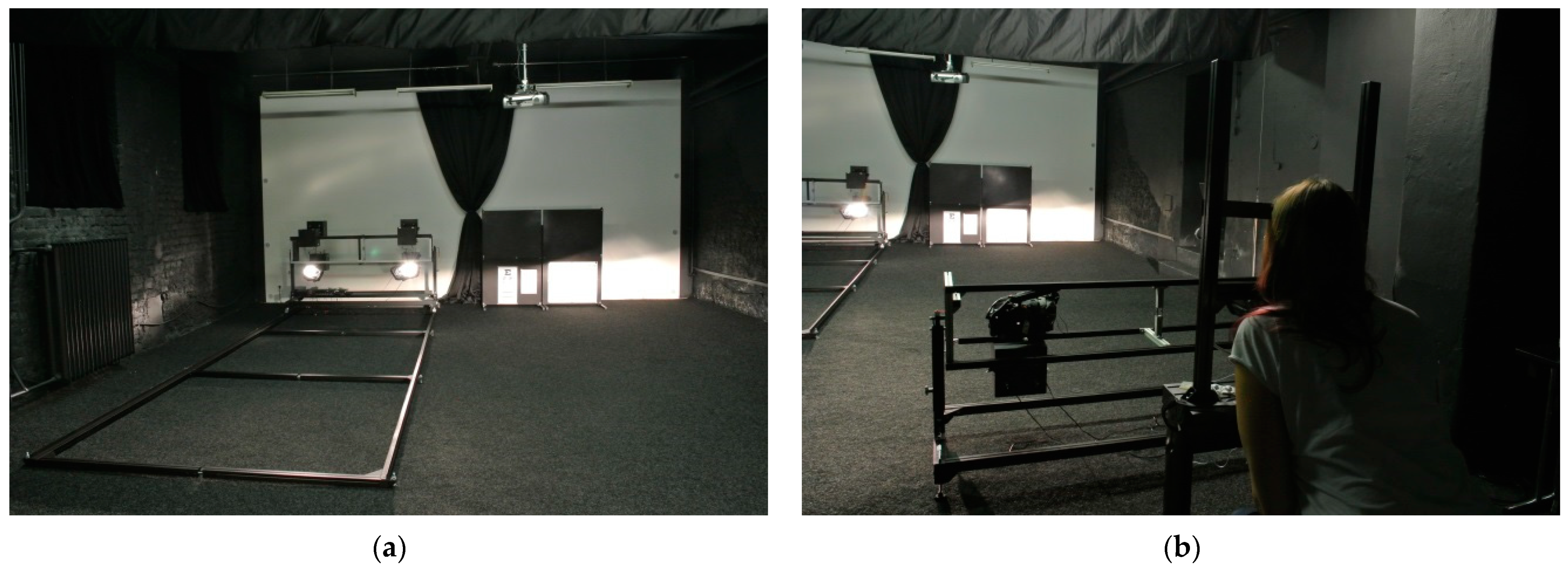
2.2. Laboratory Setting
Light Samples
- series reflector containing regular H7 bulb (CCT of 3200 K);
- series LED projector module (“white” LED, CCT of 5700 K);
- “yellow” adjusted LED projector module—module containing a PCB with the most yellowish LED color bin and the lens defocused to create the most blurred cut-off line possible while maintaining the headlamp legality as much as possible (CCT of 4700 K);
- “blue” adjusted LED projector module—module containing a PCB with the most bluish LED color bin and the lens focused to create the sharpest cut-off line possible while maintaining the headlamp legality as much as possible (CCT of 6200 K).
2.3. Data Collection Procedure
2.3.1. Initial Participant Examination
- the car they usually drive and its type of headlamps;
- the frequency of their driving and their average mileage per month;
- the types of roads they usually drive on (in the city/outside of the city/on highways);
- how often they drive at dusk/dawn/at night; and
- about any eye defects (myopia, hyperopia, presbyopia, astigmatism, glaucoma, color blindness, etc.) that they might have, and the types of correction used for them (i.e., surgery, contact lenses/glasses, and whether these possess a blue-light filter or other types of tinting).
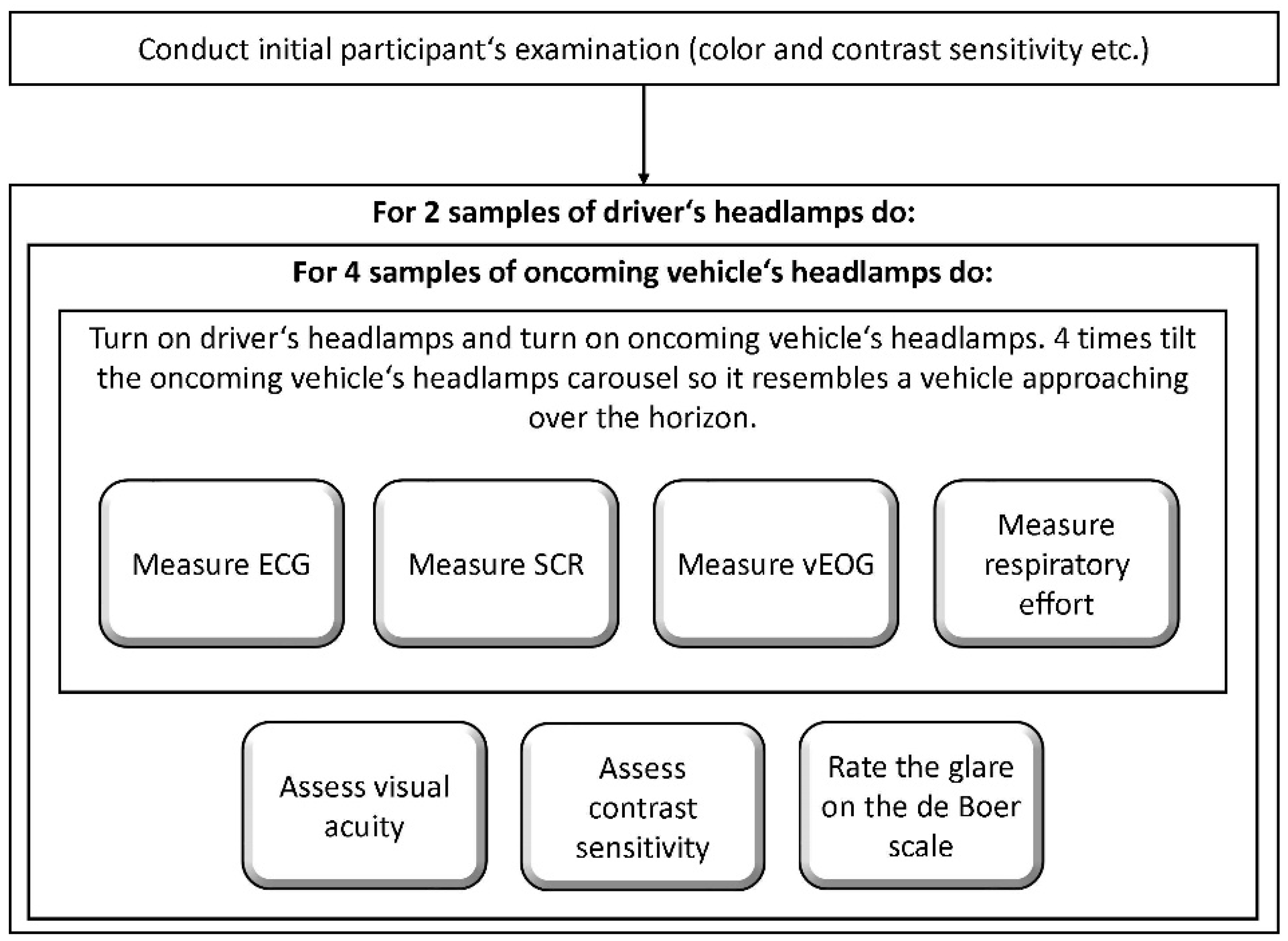
2.3.2. Experimental Procedure
2.4. Data Analysis
- participants react differently (in terms of SCR, HRV, blinking rate, and de Boer ratings) to glare by different light source combinations;
- glare by specific light source combinations leads to short-term changes in visual acuity and contrast sensitivity;
- preference for a specific light source (as measured by the tabletop experiment) plays a role in the reaction to glare (in terms of SCR, HRV, blinking rate, and de Boer ratings); and
- whether there is a link between the subjective de Boer rating and the psychophysiological variables.
- skin conductance response (SCR);
- eye-blinking rate, computed from the vertical electrooculography (vEOG) signal;
- number of post-glare correctly identified characters from the Snellen, Tumbling E, and the Pelli–Robson chart, respectively; and
- the de Boer ratings for each light source combination.
2.4.1. Physiological Data Pre-Processing
2.4.2. Statistical Analyses
3. Results
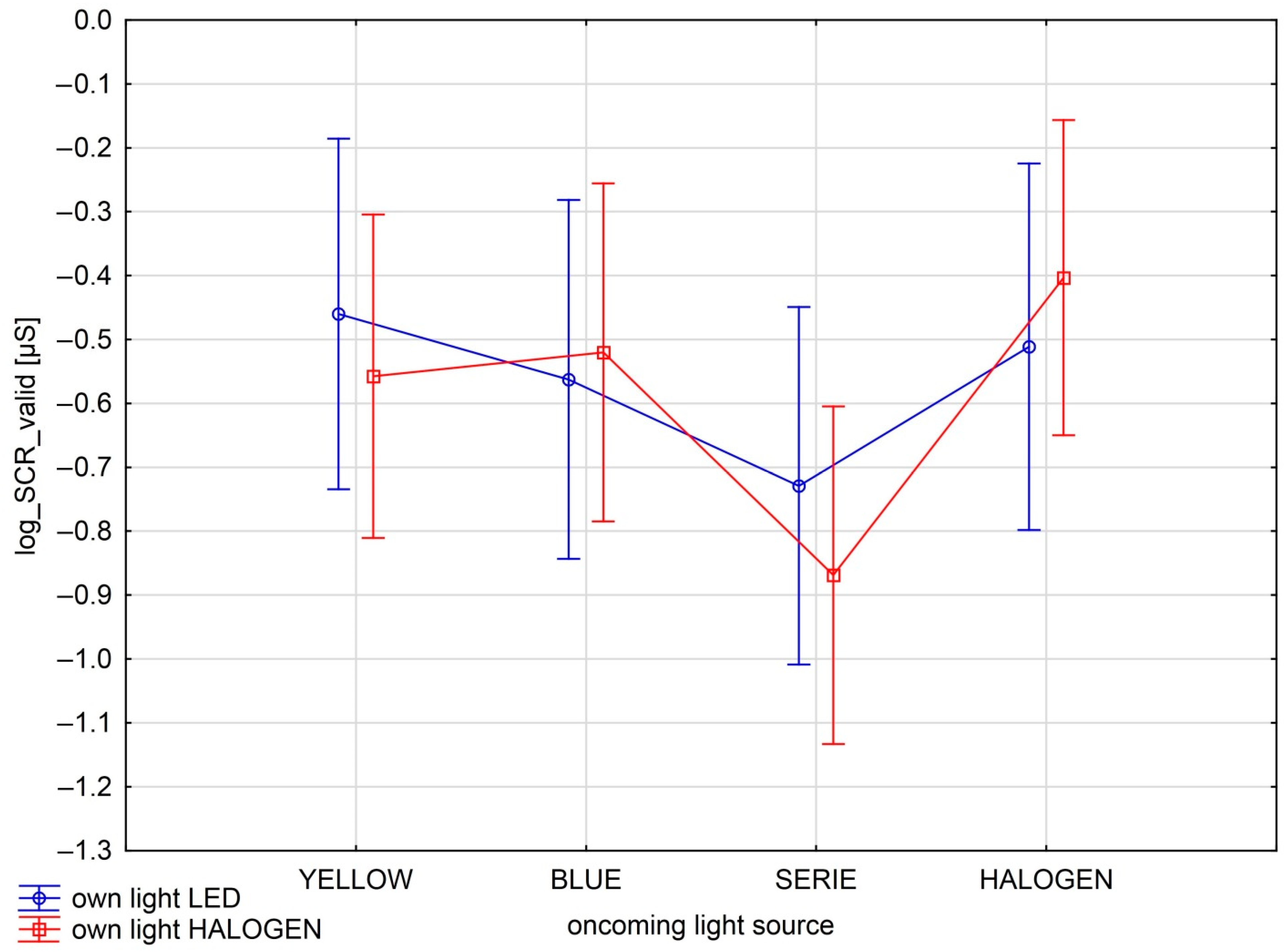
3.1. SCR and Different Light Combinations
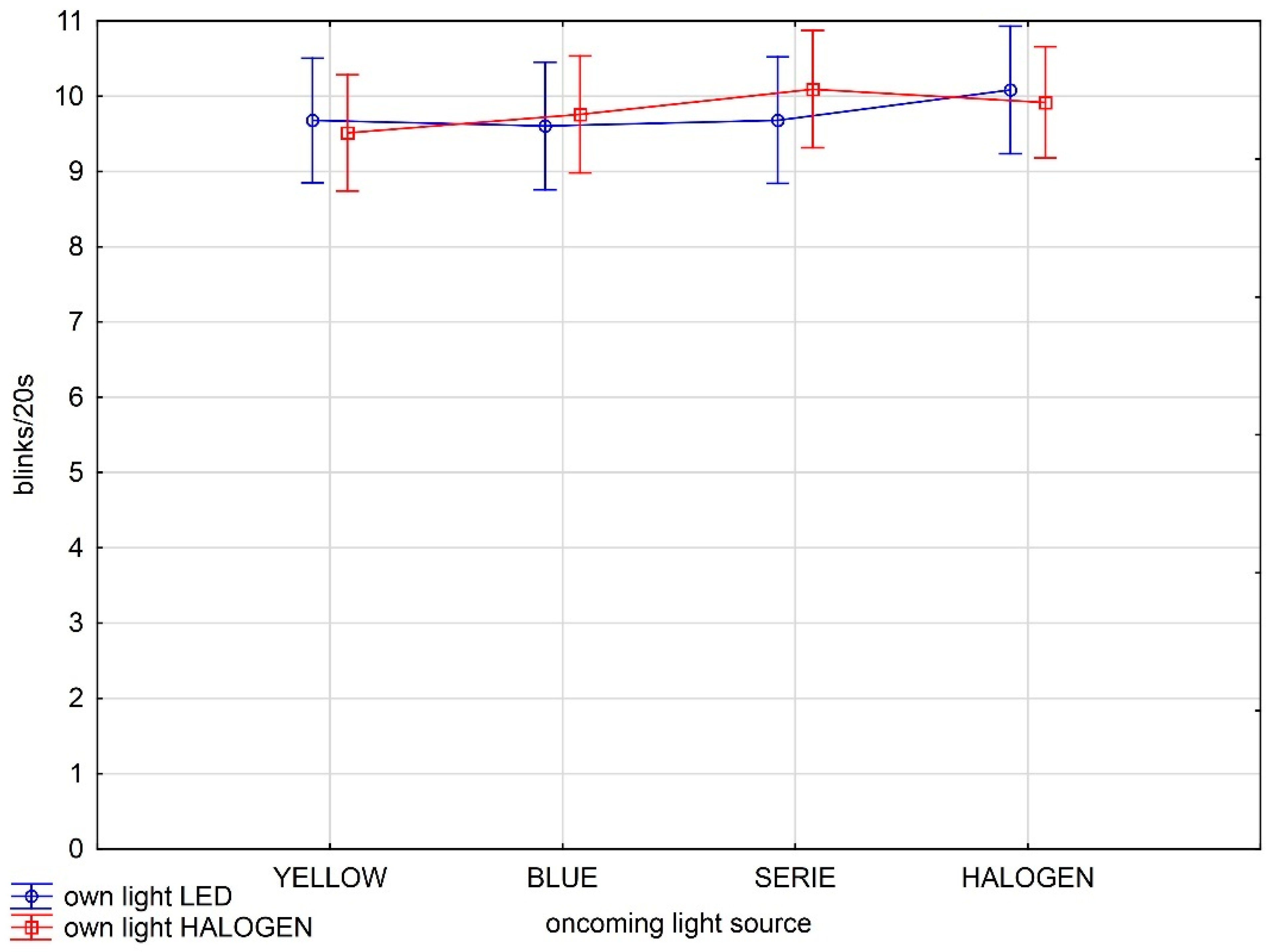
3.2. Blinking Frequency and Different Light Combinations
3.3. Visual Acuity and Contrast Sensitivity Post Glare
3.4. De Boer Scale Ratings
3.5. Simple Correlations between the Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Babizhayev, M.A. Glare Disability and Driving Safety. Ophthalmic Res. 2003, 35, 19–25. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Agreement Concerning the Adoption of Uniform Technical Prescriptions for Wheeled Vehicles, Equipment and Parts which can Be Fitted and/or Be Used on Wheeled Vehicles and the Conditions for Reciprocal Recognition of Approvals Granted on the Basis of These United Nations Regulations. (Revision 3, Including the Amendments Which Entered into Force on 14 September 2017), Addendum 47: UN Regulation No. 48, Revision 12, Amendment 8; United Nations: New York, NY, USA, 2019; Available online: https://unece.org/fileadmin/DAM/trans/main/wp29/wp29regs/2019/E-ECE-324-Rev.1-Add.47-Rev.12-Amend.8.pdf (accessed on 14 December 2019).
- SAE International. SAE J1383 (R) Performance Requirements for Motor Vehicle Headlamps; SAE International: Warrendale, PA, USA, 2018. [Google Scholar] [CrossRef]
- Kent, M.G.; Fotios, S.; Altomonte, S. Discomfort glare evaluation: The influence of anchor bias in luminance adjustments. Light. Res. Technol. 2019, 51, 131–146. [Google Scholar] [CrossRef]
- Shi, L.; Zhang, Y.; Wang, Z.; Cheng, X.; Yan, H. Luminance parameter thresholds for user visual comfort under daylight conditions from subjective responses and physiological measurements in a gymnasium. Build. Environ. 2021, 205, 108187. [Google Scholar] [CrossRef]
- Andreassi, J.L. Psychophysiology: Human Behavior and Physiological Response; Routledge: London, UK, 2006. [Google Scholar]
- Cacioppo, J.T.; Tassinary, L.G.; Berntson, G. (Eds.) Handbook of Psychophysiology, 3rd ed.; Cambridge University Press: Cambridge, UK, 2007. [Google Scholar]
- Hamedani, Z.; Solgi, E.; Skates, H.; Hine, T.; Fernando, R.; Lyons, J.; Dupre, K. Visual discomfort and glare assessment in office environments: A review of light-induced physiological and perceptual responses. Build. Environ. 2019, 153, 267–280. [Google Scholar] [CrossRef]
- Hamedani, Z.; Solgi, E.; Hine, T.; Skates, H.; Isoardi, G.; Fernando, R. Lighting for work: A study of the relationships among discomfort glare, physiological responses and visual performance. Build. Environ. 2020, 167, 106478. [Google Scholar] [CrossRef]
- Bullough, J.D.; Fu, Z.; Van Derlofske, J. Discomfort and Disability Glare from Halogen and HID Headlamp Systems (No. 2002-01-0010); SAE Technical Paper; SAE International: Warrendale, PA, USA, 2002; Available online: https://pdfs.semanticscholar.org/2ab1/db31c1587b4b150126278b0b282dccf82456.pdf (accessed on 15 April 2019).
- Theeuwes, J.; Alferdinck, J.W.; Perel, M. Relation between glare and driving performance. Hum. Factors 2002, 44, 95–107. [Google Scholar] [CrossRef] [Green Version]
- Bullough, J.D.; Van Derlofske, J.; Dee, P.; Chen, J.; Akashi, Y. An Investigation of Headlamp Glare: Intensity, Spectrum and Size (No. HS-809 672); National Highway Traffic Safety Administration: Washington, DC, USA, 2004. Available online: https://www.nhtsa.gov/sites/nhtsa.dot.gov/files/final-report_rpi_glare_spectrum.pdf (accessed on 24 May 2019).
- Skinner, N.P.; Bullough, J.D. Influence of Intensity, Duration and Spectral Characteristics on Glare Recovery for Peripheral Visibility; SAE Technical Paper; SAE International: Warrendale, PA, USA, 2020. [Google Scholar] [CrossRef]
- Fekete, J.; Sik-Lányi, C.; Schanda, J. Night-Time Driving–New Light Sources in Car Headlamps–Visibility and Glare; CIE Midterm Meeting and Congreso Internacional de Iluminación: Léon, Spain, 2005; Available online: https://www.researchgate.net/profile/Cecilia-Sik-Lanyi/publication/228630501_Night-time_driving-new_light_sources_in_car_headlamps-visibility_and_glare/links/09e415143318e23c5d000000/Night-time-driving-new-light-sources-in-car-headlamps-visibility-and-glare.pdf (accessed on 25 April 2019).
- Shim, J.Y.; Park, S.-C. Correction and Evaluation for Color Aberration on the Cut-off Line of a Vehicle Headlamp. Korean J. Opt. Photonics 2019, 30, 8–14. [Google Scholar] [CrossRef]
- Kooi, F.L.; Alferdinck, J.W.A.M. Yellow Lessens Discomfort Glare: Physiological Mechanism(s); F-WR-2003-0023-H Report; TNO Human Factors: Soesterberg, The Netherlands, 2004. [Google Scholar]
- Sivak, M.; Olson, P.L. Toward the development of a field methodology for evaluating discomfort glare from automobile headlamps. J. Saf. Res. 1988, 19, 135–143. [Google Scholar] [CrossRef] [Green Version]
- De Boer, J.B. (Ed.) Visual perception in road traffic and the field of vision of the motorist. In Public Lighting; Philips Technical Library: Eindhoven, The Netherlands, 1967; pp. 11–96. [Google Scholar]
- Gellatly, A.W.; Weintraub, D.J. User Reconfigurations of the de Boer Rating Scale for Discomfort Glare; Report No. UMTRI-90-20; The University of Michigan: Ann Arbor, MI, USA, 1990; Available online: https://deepblue.lib.umich.edu/bitstream/handle/2027.42/64065/79690.pdf?sequence=1&isAllowed=y (accessed on 25 April 2019).
- Iodice, M.; Jost, S.; Dumortier, D. Testing experimental methods for discomfort glare investigations. In Proceedings of the 29th CIE Session, Washington, DC, USA, 14–22 June 2019; International Commission on Illumination, CIE: Vienna, Austria, 2019; pp. 317–324. [Google Scholar]
- Lee, H.S.; Kim, J.Y.; Subramaniyam, M.; Park, S.; Min, S.N. Evaluation of quantitative glare technique based on the analysis of bio-signals. Ergonomics 2017, 60, 1376–1383. [Google Scholar] [CrossRef]
- Pierson, C.; Wienold, J.; Bodart, M. Review of factors influencing discomfort glare perception from daylight. Leukos 2018, 14, 111–148. [Google Scholar] [CrossRef]
- Viktorová, L.; Dominik, T.; Stanke, L.; Dostál, D. Člověk a světlo: (Re)konstrukce deBoerovy škály pro oslnění v českém jazyce. Jemná Mech. Opt. 2020, 3, 82–84. [Google Scholar]
- McCamy, C.S. Correlated color temperature as an explicit function of chromaticity coordinates. Color Res. Appl. 1992, 17, 142–144. [Google Scholar] [CrossRef]
- Hara, A.; Ohide, H.; Miyagawa, K.; Takeuchi, T.; Nakatani, Y.; Yokoyama, H.; Amano, T. Acute Effects of Caffeine on Blood Pressure and Heart Rate in Habitual and Non-Habitual Coffee Consumers: A Randomized, Double-Blind, Placebo-Controlled Study. Iryo Yakugaku (Jpn. J. Pharm. Health Care Sci.) 2014, 40, 383–388. [Google Scholar] [CrossRef] [Green Version]
- Piquet-Thepot, M.-M. Contribution à l’anthropologie des Corses: Anthropologie de la tête (suite). Bull. Mem. Soc. D’anthropol. Paris 1968, 3, 183–218. [Google Scholar] [CrossRef]
- Nischler, C.; Michael, R.; Wintersteller, C.; Marvan, P.; van Rijn, L.J.; Coppens, J.E.; van den Berg, T.J.T.P.; Emesz, M.; Grabner, G. Iris Color and Visual Functions. Arbeitsphysiologie 2013, 251, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Stringham, J.M.; Garcia, P.V.; Smith, P.A.; McLin, L.N.; Foutch, B.K. Macular Pigment and Visual Performance in Glare: Benefits for Photostress Recovery, Disability Glare, and Visual Discomfort. Investig. Ophthalmol. Vis. Sci. 2011, 52, 7406–7415. [Google Scholar] [CrossRef] [Green Version]
- Marié, S.; Montés-Micó, R.; Martínez-Albert, N.; García-Marqués, J.V.; Cerviño, A. Evaluation of Physiological Parameters on Discomfort Glare Thresholds Using LUMIZ 100 Tool. Transl. Vis. Sci. Technol. 2021, 10, 28. [Google Scholar] [CrossRef]
- Broschmann, D.; Kuchenbecker, J. Plates for Color Vision Testing; Thieme Publishing Group: Stuttgart, Germany, 2013. [Google Scholar]
- Singh, G.; Bhinder, H.S. Closed Chamber Thermometry and Humidity Measurements in Normal and Dry Eye Patients: A Pilot Study. Eur. J. Ophthalmol. 2003, 13, 343–350. [Google Scholar] [CrossRef]
- Tsubota, K.; Yamada, M. Tear Evaporation from the Ocular Surface. Investig. Ophthalmol. Vis. Sci. 1992, 33, 2942–2950. [Google Scholar]
- Puell, M.C.; Benítez-del-Castillo, J.M.; Martínez-de-la-Casa, J.; Sánchez-Ramos, C.; Vico, E.; Pérez-Carrasco, M.J.; Pedraza, C.; del-Hierro, A. Contrast Sensitivity and Disability Glare in Patients with Dry Eye. Acta Ophthalmol. Scand. 2006, 84, 527–531. [Google Scholar] [CrossRef]
- Huang, F.-C.; Tseng, S.-H.; Shih, M.-H.; Chen, F.K. Effect of Artificial Tears on Corneal Surface Regularity, Contrast Sensitivity, and Glare Disability in Dry Eyes. Ophthalmology 2002, 109, 1934–1940. [Google Scholar] [CrossRef]
- Maheshkumar, K.; Dilara, K.; Maruthy, K.N.; Sundareswaren, L. Validation of PC-Based Sound Card with Biopac for Digitalization of ECG Recording in Short-Term HRV Analysis. N. Am. J. Med. Sci. 2016, 8, 307–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva Moreira, P.; Chaves, P.; Dias, R.; Dias, N.; Almeida, P.R. Validation of Wireless Sensors for Psychophysiological Studies. Sensors 2019, 19, 4824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westermann, H. Informal Document No. 30 (48th GRE, 9–12 April) 2002 (Agenda Items 1.2 and 4.2) History and Scientific Back-Up; United Nations: New York, NY, USA, 2002; Available online: https://unece.org/DAM/trans/doc/2011/wp29gre/GRE-48-30e.pdf (accessed on 17 May 2021).
- Boucsein, W. Electrodermal Activity; Springer: Boston, MA, USA, 2012. [Google Scholar]
- Stern, R.M.; Ray, W.J.; Quigley, K.S. Psychophysiological Recording, 2nd ed.; Oxford University Press: New York, NY, USA, 2001. [Google Scholar]
- Lawrence, C.A.; Barry, R.J. ERPs and the Evoked Cardiac Response to Auditory Stimuli: Intensity and Cognitive Load Effects. Acta Neurobiol. Exp. 2009, 69, 552–559. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Photometry Test Point | Homologation Value | CoP Value |
|---|---|---|
| HV | max. 625 cd | max. 880 cd |
| BR | max. 1750 cd | max. 2100 cd |
| B50L 1 | max. 350 cd | max. 520 cd |
| 50L | max. 18,480 cd | max. 15,840 cd |
| 75R | min. 10,100 cd | min. 8080 cd |
| Photometry Test Point and Gradient | Halogen Bulb Reflector | Series LED Module | Bluish LED Module | Yellowish LED Module |
|---|---|---|---|---|
| HV | 427 cd | 356 cd | 206 cd | 1323 cd |
| BR | 249 cd | 241 cd | 205 cd | 430 cd |
| B50L 1 | 234 cd | 185 cd | 139 cd | 369 cd |
| 50L | 8028 cd | 8517 cd | 7502 cd | 14,900 cd |
| 75R | 13,598 cd | 18,440 cd | 13,340 cd | 28,360 cd |
| Gradient | 0.299 | 0.295 | 0.413 | 0.212 |
| Photometry Test Point and Gradient | Halogen Bulb Reflector | Series LED Module | Bluish LED Module | Yellowish LED Module |
|---|---|---|---|---|
| HV | 475 cd | 436 cd | 248 cd | 558 cd |
| BR | 261 cd | 275 cd | 199 cd | 298 cd |
| B50L 1 | 267 cd | 238 cd | 205 cd | 271 cd |
| 50L | 5934 cd | 13,280 cd | 7732 cd | 7536 cd |
| 75R | 15,256 cd | 25,730 cd | 12,260 cd | 22,150 cd |
| Gradient | 0.233 | 0.291 | 0.377 | 0.198 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stanke, L.; Viktorová, L.; Dominik, T. Discomfort Glare Perception by Drivers—Establishing a Link between Subjective and Psychophysiological Assessment. Appl. Sci. 2022, 12, 3847. https://doi.org/10.3390/app12083847
Stanke L, Viktorová L, Dominik T. Discomfort Glare Perception by Drivers—Establishing a Link between Subjective and Psychophysiological Assessment. Applied Sciences. 2022; 12(8):3847. https://doi.org/10.3390/app12083847
Chicago/Turabian StyleStanke, Ladislav, Lucie Viktorová, and Tomáš Dominik. 2022. "Discomfort Glare Perception by Drivers—Establishing a Link between Subjective and Psychophysiological Assessment" Applied Sciences 12, no. 8: 3847. https://doi.org/10.3390/app12083847