1. Introduction
A hearing aid is a major instrument used to compensate for hearing disorders via amplifying sound. When hearing aids are used, an earplug is inserted into the ear canal to deliver sound. The coupling condition between the hearing aids and ears can influence audiological benefits, comfort, and fixation. When the earplug fits tightly to the ear, sound leak from the ear canal is reduced to suppress feedback problems. The output level from the transducer can be amplified enough to obtain sufficient benefits. The stable fixation of the earplug stabilizes the output. Unsuitable small earplugs may cause feedback problems and their falling from the ear. In contrast, a tight earplug can induce sensations of fullness, pain, and skin injury.
Ear shapes vary among patients. To achieve good conditions, a custom ear mold or shell is created for each patient instead of modular construction. To create the molds, the ear impression is first obtained via inserting a silicone material into the ear. After scanning the ear impressions, hearing aids are designed using specialized computer-aided design (CAD) software. This process is considered to be an established method. However, taking an ear impression involves some risks, such as the possibility of external and middle ear trauma or foreign bodies entering the canal and middle ear [
1,
2,
3]. As an alternative method, three-dimensional (3D) laser scanning was developed [
4], which avoids the risks related to taking the ear impression. However, this method is not popular in clinical practice.
In some cases, it is difficult to achieve sufficient benefit from hearing aids. A representative example of this is aural atresia. Some patients cannot wear hearing aids because of their atretic ear. Furthermore, atretic ears often accompany microtia. A modular construction is hardly fitted to such ears, and a custom ear mold is required for the fitting. However, most cases cannot achieve sufficient benefits due to poor gains or feedback problems [
5]. Instead of air conduction (AC) devices, bone conduction (BC) devices are used in these patients. Conventional BC hearing aids are the most common. The transducers of BC hearing aids are placed on the skull bone, such as the mastoid, to deliver the signals. This conduction form is effective in ears with aural atresia and microtia. Unfortunately, high contact pressure against the skull bone is required for the device to function properly. This fixation style can cause skin irritation, prolonged skin depression, and discomfort [
5,
6]. An esthetic problem owing to the headband is another issue. Recently, a new type of BC device—ADHEAR (MED-EL, Innsbruck, Austria)—was used in clinical practices. This device is placed on the mastoid via attachment to the adapter stuck to the skin behind the ear and can overcome the disadvantages of conventional BC hearing aids derived from its fixation style. Unfortunately, the signals may be deteriorated because the transducer is fixed without a static force. The recommended fitting range is ≤25 dB HL [
7].
Alternative options in atretic ears are implantable devices, such as bone-anchored hearing aids (BAHA; Cochlear Limited, Sydney, Australia), Bonebridge (MED-EL), and Vibrant Soundbridge (MED-EL) [
5,
7,
8,
9]. As the transducers of these devices are not fixed with high contact pressure, most of the demerits in conventional BC hearing aids are resolved. Furthermore, the signals are delivered directly to the skull bone, not percutaneously, which can improve the audiological benefits [
7]. In contrast, these devices require surgery, which is disadvantageous to conventional hearing aids. Upward of 20% of patients who undergo BC device implantation experience complications, such as tissue overgrowth, skin infection, and persistent pain at the abutment site [
10].
Cartilage conduction (CC) hearing devices are a new option for atretic ears [
11,
12,
13,
14,
15]. This device delivers sound to the aural cartilage using a small lightweight transducer. It can be used without static force using a headband. Therefore, wearing comfort and appearance are improved compared to conventional BC hearing aids. In cases of aural atresia, the signals are transmitted to the cochlea necessarily via the skull bone. The signals are percutaneously delivered to the cartilaginous tissues in a manner similar to conventional BC hearing aids. For conventional BC hearing aids, high contact pressure can reduce the attenuation of the transmission. In contrast, the transducer in CC hearing devices is usually placed without a static force. However, it can provide sufficient audiological benefits for daily use [
16,
17,
18]. The aided thresholds of CC hearing devices are better than those of ADHEAR [
19]. The performances of CC hearing devices in speech recognition are comparable to those of BC devices, such as BAHA, although the aided thresholds were slightly higher [
20]. They have been clinically used in Japan since 2017, and approximately 80% of patients with aural atresia purchased and continuously used CC hearing devices after daily use on trial [
17].
There are three types of transducers utilized in CC hearing devices. The first type is a simple transducer that is fixed using double-sided tape. The other two transducers are the ear chip-attached and ear chip-embedded types (
Figure 1) [
14]. One of the differences between them is their size. The ear chip-embedded type can be chosen when the ear chip is large enough to embed the transducer. The stability of the transducer can be improved in the order of simple, ear chip-attached, and ear chip-embedded types. In a previous study, the continuous use rate increased in the same order [
21]. Thus, the ear chip types are usually employed, if possible. In the process of CC hearing device fitting, taking an ear impression is required to create the ear chip to couple the transducer to the ear, similar to an ear mold or shell. There is a big variation in the shape of the ear among patients with microtia and aural atresia. Furthermore, otoplasty also results in a big variation. The stable fixation of the transducer on the aural cartilage is considered important to achieve sufficient benefit. Therefore, the shape of the ear chip can influence the benefit.
Meanwhile, when patients with aural atresia visit the hospital, some patients undergo a computed tomography (CT) scan of the ear for diagnosis. CT scans precisely describe the local anatomical structures. Particularly, the boundary between the tissues and air can be clearly described. Therefore, if CT was performed, CT images may be utilized for CAD to create ear chips instead of ear impressions, and the risks related to taking the ear impression can be avoided. Considering the cost and risk of radiation exposure, CT examination is not appropriate for creating ear impressions. However, if CT was already performed for other purposes, the creation of an ear chip utilizing CT images may become one of the options. In contrast, the reproduction of the structure designed using the CT image may be inferior to that of the ear impression because of the limitation of the resolution depending on the slice width. In this study, the ear chip of the CC hearing device was designed not only via ear impression but also via CT images of patients with aural atresia who underwent a CT scan of the ear. Aided thresholds and subjective evaluations were compared between both methods. This exploratory study aimed to investigate whether CT images can be used for CAD to create hearing devices.
2. Materials and Methods
2.1. Patients
All patients visited our hospital to fit the CC hearing devices. The inclusion criteria were as follows: CT was performed for the diagnosis and evaluation of ear malformation before fitting, hearing loss was predominantly derived from aural atresia or severe stenosis, and CC hearing devices were fitted to the atretic ear to compensate for hearing loss. Three patients participated in the study (
Table 1).
Patient 1 was a woman with bilateral microtia and congenital aural atresia. She had previously undergone bilateral otoplasty without any surgical repair of congenital aural atresia. She had used conventional BC hearing aids, the transducers of which induced the hollow of the skull bone and local pain. She visited our hospital to fit CC hearing devices instead of BC hearing aids. Her right ear canal showed severe stenosis, and CT findings revealed that the ear canal occluded completely with soft tissue density. Her left ear was closed completely, and CT findings revealed no existence of the ear canal.
Patient 2 was a man with right severe stenosis of the ear canal, accompanying mild anomaly of the auricula. The diameter of the entrance of the ear canal was approximately 1 mm, and CT found that the ear canal was completely occluded with soft tissue density. His left ear was normal. He had tried to use an AC hearing aid on his right ear. However, the hearing aid was not stably fixed, and he gave up on its continuous use. He visited our hospital to fit a CC hearing device into his right ear.
Patient 3 was a man with right microtia and bilateral severe stenosis. No cavity in the ear canal was observed from the outside, and CT findings revealed that the ear canal was completely occluded with soft tissue density. Although he had used an AC hearing aid on his left ear, sufficient benefits were not obtained. He visited our hospital to fit CC hearing devices into both ears. Due to severe microtia, a simple transducer type was fitted to the right ear. Thus, solely the left ear was a subject of this study.
This study was approved by the Ethics Committee of Nara Medical University (No. 1981). Participants (or their parents if the participant’s age was <20 years) provided written informed consent before enrollment.
2.2. Design via Ear Impression
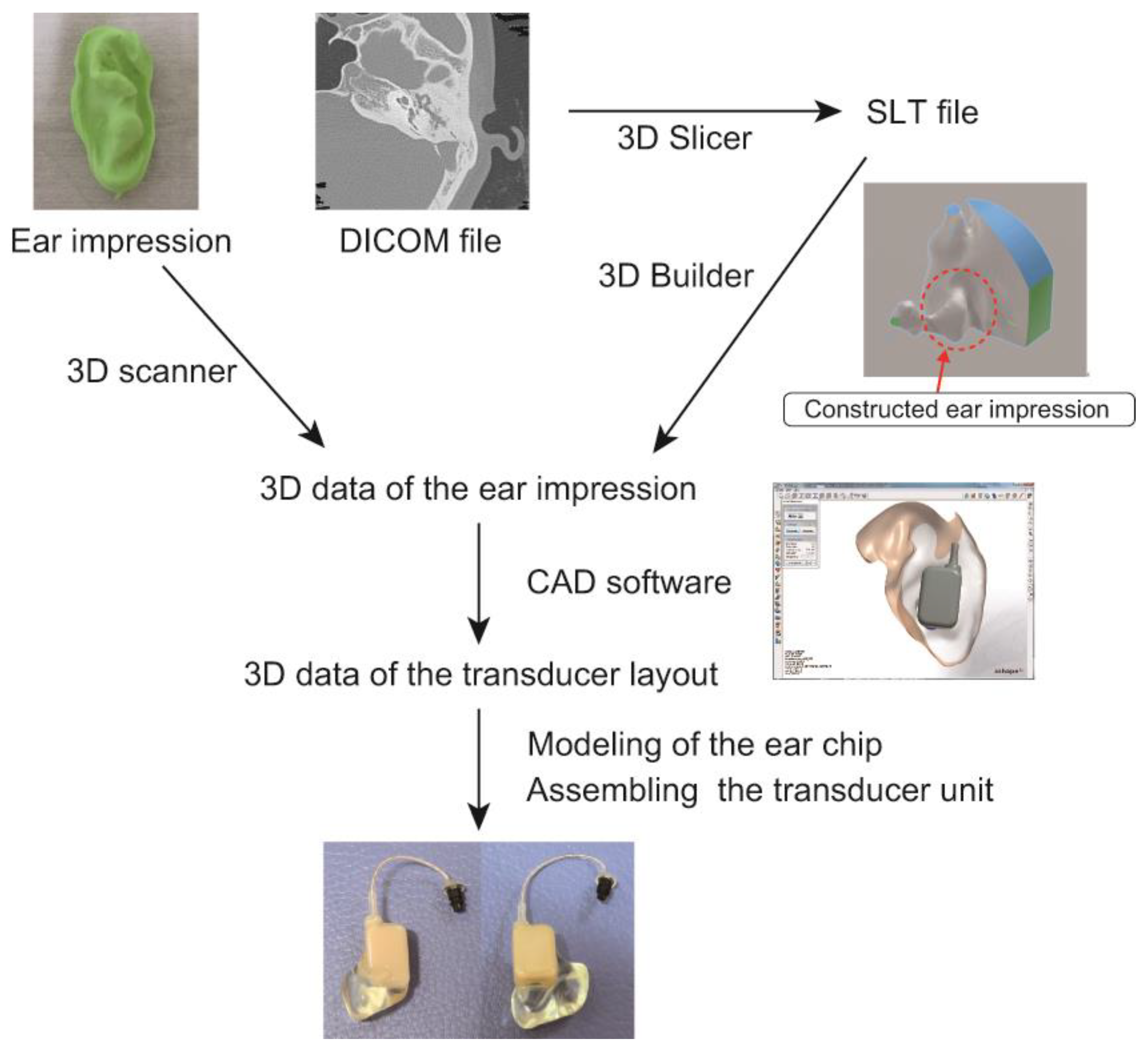
Ear impression was performed according to the method usually used in clinical practice. The ear impression was obtained using a silicone material. The appropriate length of the wire connecting the transducer to the body of the hearing device was determined using a special gauge. The transducer type was chosen based on the shape of the ear. The ear impression, information on the wire length and transducer type, and photographs of the ear were sent to the manufacturing factory. In the manufacturing factory, the ear impression was 3D scanned, and, based on the obtained 3D data, the shape and layout of the transducer were determined using CAD software to create the transducer (
Figure 2). The length of the wire was chosen according to the order sheet.
2.3. Design via CT Images
Figure 2 shows the process of designing the transducer based on the CT images. The CT images examined before fitting were recorded using the Digital Imaging and Communications in Medicine (DICOM) format, which is usually used for the transmission of the images in medical institutions. The data were sent to the manufacturing factory separately from the ear impression. In the manufacturing factory, the DICOM format was first converted into the SLT format, which is a 3D data format, using a 3D Slicer image computing platform [
22]. Next, the described object was reversed to obtain the 3D data of the ear impression using 3D Builder (Microsoft, Redmond, WA, USA). Using these obtained data, instead of those obtained via the real ear impression, the hearing devices were designed on the CAD software to create the ear chip. The length of the wire and the type of transducer were determined based on CT images in the manufacturing factory. Both manufacturing processes were individually performed without knowledge of the other processes.
2.4. Fitting and Evaluation
After the hearing devices were created, they were fitted to the ears and their audiological benefits were examined. The adjustment of the device was first performed using the impression-based transducer. The benefits were evaluated via subjective impression, aided thresholds, functional gains, and speech audiometry. The audiometric results were judged according to the Japanese guidelines for the evaluation of hearing aid fitting [
23]. If the benefits were insufficient, the device was adjusted again. After the completion of the adjustment, the CT-based transducer was connected to the body of the hearing aid instead of the impression-based transducer. The hearing aid gains were maintained without adjustments to evaluate the difference in the benefits between the transducers. During the fitting and trial, the patients were not informed which transducer was designed based on the ear impression or CT images.
After the evaluation, the hearing device was tried in daily life. Patients 1 and 2 tried both transducers for 4 weeks. During the trial, the patients could interchange between the two transducers to compare their benefits. For Patient 3, the completion of the CT-based transducer was delayed. Therefore, the impression-based transducer was first tried for 4 weeks, and after the CT-based transducer was created, both transducers were alternately tried for 2 weeks.
After the trial, the subjective benefits of each CC hearing device were measured using questionnaires, which is consistent with the aforementioned Japanese guidelines for the evaluation of hearing aid fitting, and the evaluation was performed according to these guidelines [
23]. In comparing the subjective benefits between both transducers, the subjective patient preferences in terms of hearing, wearing comfort, and appearance were recorded, and the patients determined the devices they wanted to purchase and use continuously.
3. Results
Figure 3 shows a comparison of the two transducers. The shapes of the CT-based transducer were not always identical to those of the impression-based transducer. However, both transducers were worn smoothly without any serious problems. Although the slice width of CT ranged from 0.4 to 1.0 mm (
Table 1), the surfaces of the transducers were not especially rough, and the quality of their shape was acceptable for use in daily life.
Table 1 lists the mass of the transducers. In most cases, the mass of the CT-based transducer was slightly larger than that of the impression-based transducer.
Figure 4 shows the thresholds aided by the hearing aids. No significant differences were observed between the two transducers. After the trial in daily life, there was no obvious difference in subjective hearing. The assessment of hearing after wearing hearing aids was performed according to the Japanese guidelines for the evaluation of hearing aid fitting [
23]. As no remarkable differences in subjective hearing were observed between both transducers, the assessment using 10 questionnaires mentioned in the guidelines was performed for CC hearing devices together, not separately between two transducers. The assessments were judged to be sufficient.
Table 2 shows the subjective patient preference after the 2–4-week trial. Comparing both devices, although hearing was subjectively better with the CT-based transducer in Patient 1, the stability of the CT-based transducer in the right ear was inferior, and wearing comfort was better with the impression-designed transducer in the left ear. After the trial, Patient 1 chose the transducer designed based on ear impression for the hearing aids. Subjective hearing was also better with the CT-based transducer in Patient 2. However, wearing comfort and appearance were inferior to those of the impression-based transducer. Patient 2 also chose the impression-designed transducer for the hearing aid. In contrast, in Patient 3, no difference in the subjective patient hearing and wearing comfort was observed between the two transducers. However, the mass of the CT-based transducer was smaller. Patient 3 chose the CT-based transducer because of its better appearance.
Summarizing the results, the CT-based transducer provided subjectively better hearing in three ears, whereas no difference was found in the aided thresholds between the two devices. Wearing comfort was better with the impression-based transducers. The subjective appearance varied among the patients. Finally, the CT-based transducer was chosen by one of the three patients.
4. Discussion
In terms of coupling to the ear, the transducer designed via ear impression was expected to be better because of its advantages in reproducibility. For a CT-based transducer, reproducibility depends on the slice width. The surface of the transducer became smoother as the slice width decreased. The shape and mass of the CT-based transducer did not correspond to those of the impression-based transducer. The mass of the impression-based transducer was smaller in Patients 1 and 2 but larger in Patient 3. The mass of a transducer depends on its shape. During CAD, the shape is determined through considering the overall shape of the ear, and the slice width does not significantly influence the overall shape. Thus, the design based on CT images was not disadvantageous in terms of mass.
The placement of the transducer unit and the arrangement of the wire influence the shape of the transducer and are determined through considering the ear structure, including the auricular and surrounding areas. However, an impression of the ear cannot inform the 3D structure of the auricular and surrounding areas. In clinical practice, information on the wire length and a photograph of the ear partially compensate for these insufficiencies. In contrast, CT images provide a 3D structure of the ear. Therefore, information concerning the wire length and photographs of the ear are not required for creating hearing aids. A CT-aided design is considered to have the advantage of completely understanding the ear structure. Wearing comfort was subjectively better for the device designed via ear impression, implying that the details of the surface may be important for comfort. No esthetic advantage was observed between the two designs. The surface of the transducer is invisible during usage, which may mask the disadvantages of the surface details.
Improvement in audiometric tests is an important benefit of hearing devices. In terms of subjective evaluation, hearing aids designed using CT images were better (Patients 1 and 3). However, no significant differences were observed between the aided thresholds of the two devices. A small difference that could not be detected via the audiometric test might exist. Such an insignificant difference is considered easy to compensate for through adjustments.
The dominant sound transmission pathway to the cochlea depends on the ear condition. In a normal ear, there are three candidates for theoretical transmission pathways to the cochleae: direct AC, cartilage BC, and cartilage AC [
24,
25,
26]. In contrast, in atretic ears, the AC pathway does not exist because of obstruction in the ear canal. In cases with fibrotic aural atresia, fibrotic tissue may be connected to the ossicles. Sound can travel to the cochlea via these fibrotic tissues and ossicles (fibrotic tissue pathway) without skull bone vibration, which achieves excellent benefits from CC hearing devices [
27,
28]. In this study, there was no fibrotic tissue pathway in four ears. Thus, the dominant sound transmission pathways to the cochlea in the four ears were considered to be cartilage BC.
The coupling condition may be related to the audiometric test results. Although wearing comfort was better with the device designed based on ear impression in two patients (Patients 1 and 2), hearing was not better. This contradiction may imply that the differences were insignificant. Thus, CC hearing devices designed based on CT images are not entirely disadvantageous compared to those designed based on the ear impression and, therefore, can be considered a viable option.
There are several hearing device options for aural atretic ears [
7]. Among them, conventional BC hearing aids and ADHEAR are used without surgical treatment in the same manner as CC hearing devices. One of the differences among the three devices is their fixation style. Both ADEHAR and CC hearing devices do not require a static force for fixation, making them different from conventional BC hearing aids. Regarding aided thresholds, despite the lack of a static force, CC hearing devices can provide the same hearing levels as those of conventional BC hearing aids [
13]. The patients in the present study achieved benefits comparable to those reported in previous studies [
17]. CC hearing devices have better aided hearing levels than ADHEAR [
19], which may result from the difference not only in the transducer output, but also place of fixation, thickness of the fixation tape, and mass of the transducer. Regarding the fixation place, the thresholds for cartilage stimulation are better than those for mastoid stimulation at low frequencies when the simple-type transducer is used [
28]. In ADHEAR and CC hearing devices with simple-type transducers, the surface of the transducer in contact with the body is regular. In contrast, ear chip-type transducers are created based on the shape of the ear. The surface of the transducer in contact with the body shows varies between patients. Different from ADHEAR and CC hearing devices with simple-type transducers, the process of designing the shape of the transducer is extremely important to obtain optimal results.
The process of designing a hearing device based on the ear impression is an established method used in clinical practice. However, the process of designing a hearing device based on CT images was not optimized and must be improved before clinical use. Some current demerits of transducers designed using CT images may be improved via optimization. Compared to the conventional process, the merits of the design using CT images are as follows: no risks related to taking the ear impression, the advantage of understanding the shape of the ear in 3D, no physical transport or shipment of an ear impression is necessary, and CT images can be sent instantly via the Internet; therefore, CC hearing devices can be created without visiting the hospital. Furthermore, CT-based devices can be utilized in patients with allergy to the impression materials. In contrast, the disadvantages include the requirement of a CT scanner and reliance of the ear chip shape details on the CT image slice width. If a CT scan was not performed for diagnosis or other purposes, radiation exposure and examination costs are other demerits. The aim of this study was to investigate the possibility of creating transducers using CT images in place of ear impressions, not to compare the benefits between both devices. As a result, CT images obtained in clinical practices could be used for creating the transducer, and the performance of the CT-based transducer was not remarkably inferior to that of the impression-based transducer. As this was an exploratory study, further studies are needed to establish the design process and clarify the influence of the CT slice width on the transducer quality and audiological benefits.
This study did not evaluate the coupling of the ear mold and shell of AC hearing aids designed using CT images of the ear. For CC hearing devices, the coupling condition to the ear is more important because it directly influences sound transmission. Therefore, the current results suggest that CT images can also be utilized to create ear molds and shells for AC hearing aids.

 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}