
A Novel Deep Dense Block-Based Model for Detecting Alzheimer’s Disease

Abstract
:1. Introduction
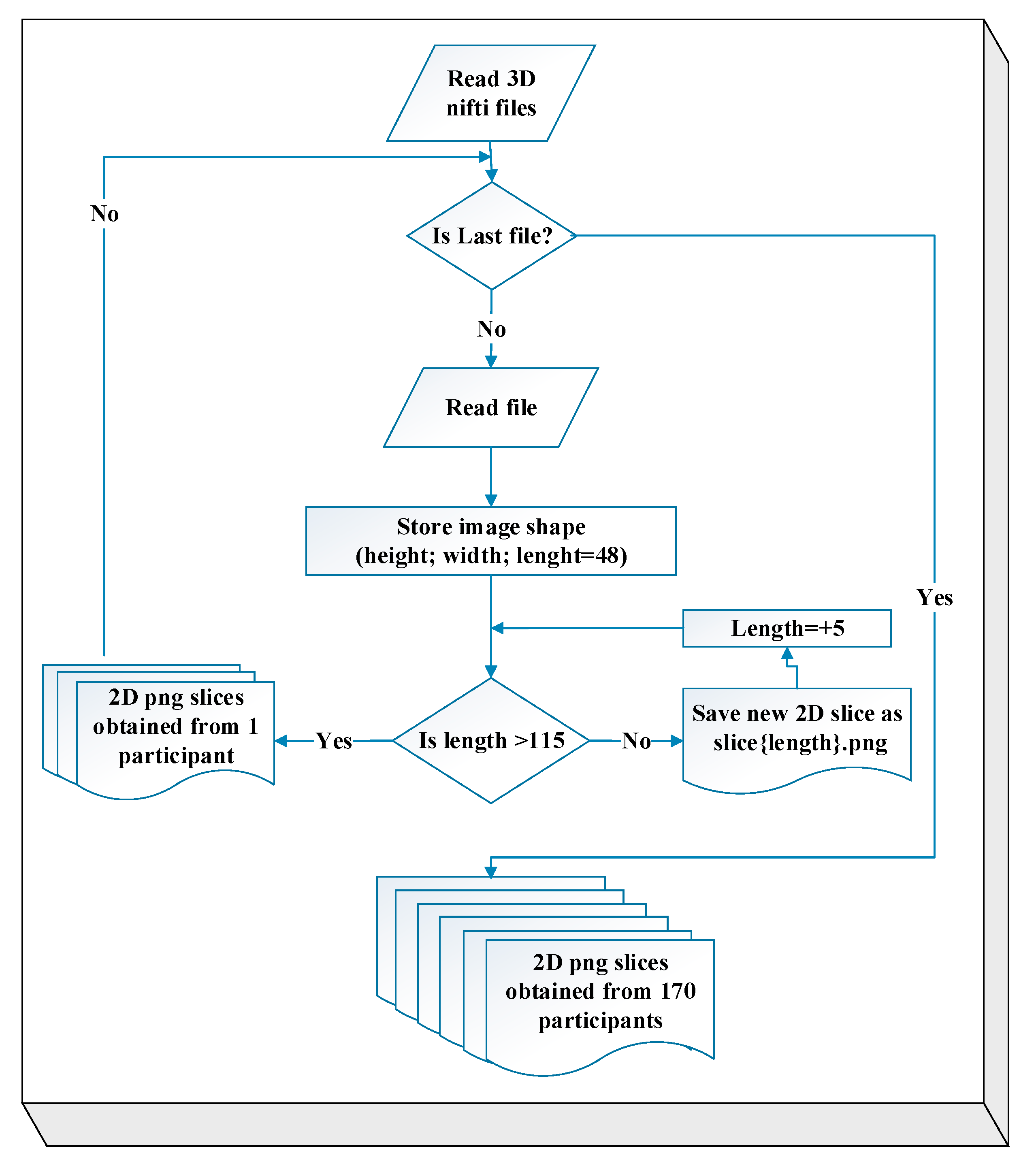
- Because MRI scans are inherently three-dimensional, they can be conceptualized as a stack of 2D MRI slices. From this stack, we selected the most informative slices for classification.
- MCI is a transitional stage between AD and CN. Therefore, it is difficult to diagnose. Therefore, in order to classify medical images, we employ the transfer-learning method using models trained on a large dataset.
- Transfer learning is used because there is limited data available, and it helps to reduce the costs of the learning process.
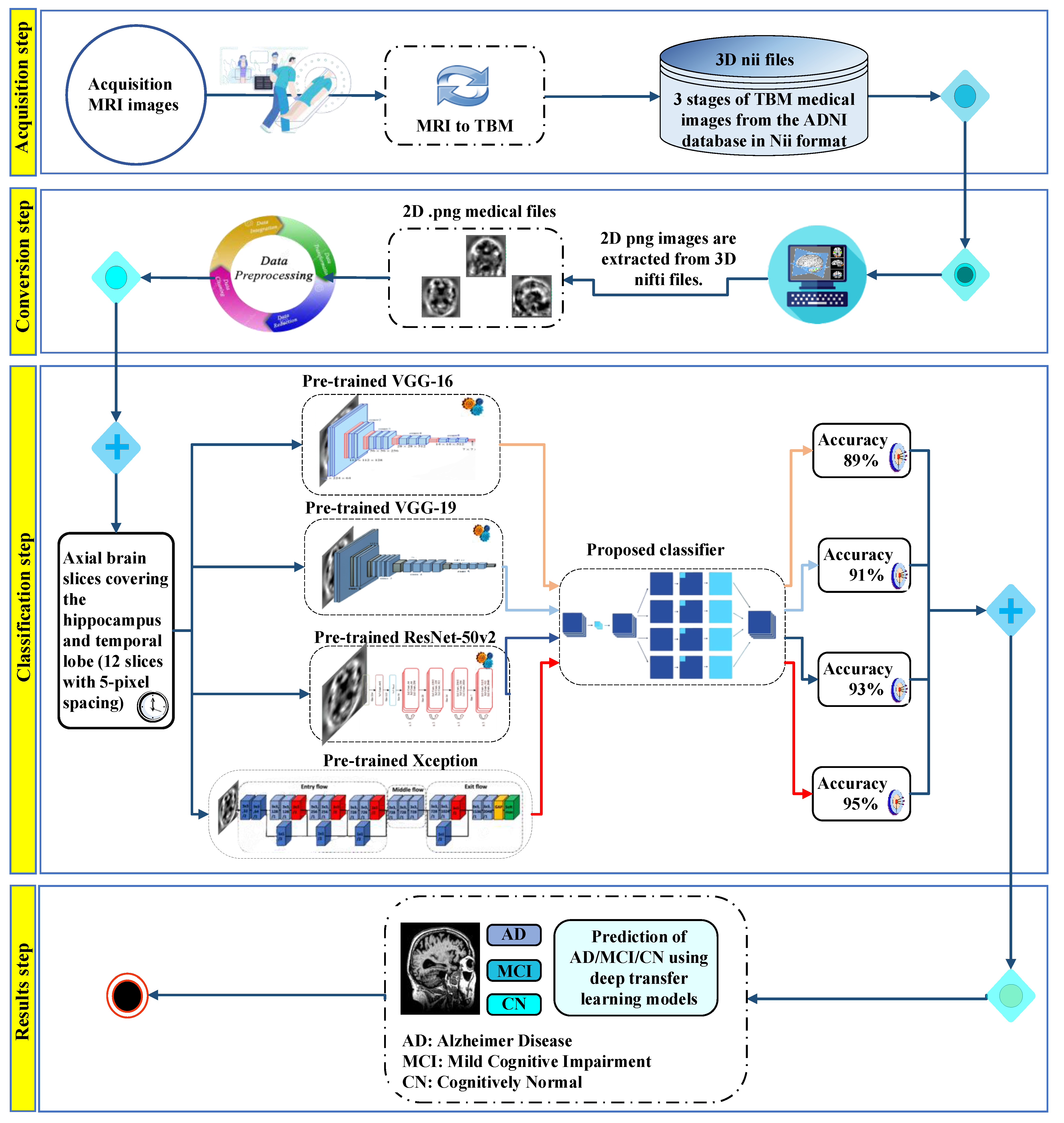
- Considering that morphometric images tend to yield more successful outcomes in disease diagnosis compared to raw or semi-processed MRI images, DL-based methods are employed for automatic feature extraction in the analysis of TBM images.
2. Related Work
3. Materials and Methods
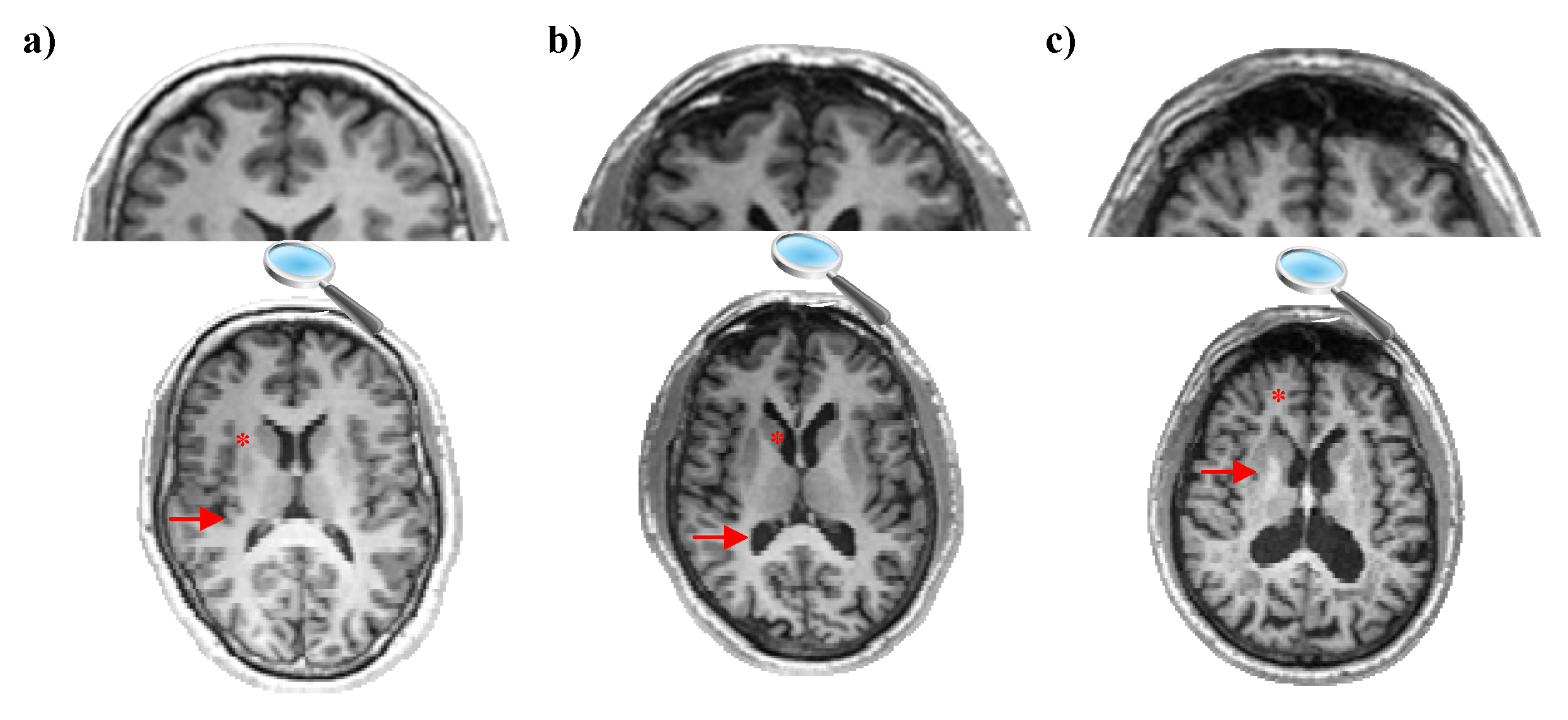
3.1. Tensor-Based Morphometry
- It can precisely and quantitatively measure the shape and size properties of brain structures with TBM.
- It can compress and reduce the data volume in brain images. This can help with faster data processing.
- It can be used to compare structural changes between different individuals, groups, or time points.
- TBM has the ability to make statistical analyses of brain structures.
3.2. Dataset and Pre-Processing
3.3. Proposed Classification Methods and Techniques
3.3.1. CNN-Based Architectures
3.3.2. Proposed Classifier
3.4. CNN Training Based on Transfer Learning
3.5. Evaluation Metrics
4. Results and Experiments
4.1. Experimental Settings
4.2. Hyperparameter and Optimization Techniques
4.3. Experimental Results
4.4. Performance Evaluation in Relation to Baseline Models
4.5. Comparison with Related Works
4.6. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Spencer, B.; Brüschweiler, S.; Sealey-Cardona, M.; Rockenstein, E.; Adame, A.; Florio, J.; Mante, M.; Trinh, I.; Rissman, R.A.; Konrat, R.; et al. Selective Targeting of 3 Repeat Tau with Brain Penetrating Single Chain Antibodies for the Treatment of Neurodegenerative Disorders. Acta. Neuropathol. 2018, 136, 69–87. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-H.; Kim, S.-W.; Lee, S.-H.; Cho, J.-Y.; Hwang, S.-H.; Lee, W.-W.; Lee, J.-W.; Kim, D.-K.; Jeon, Y.-D. The Mixture of Gastrodia Elata and Glycyrrhiza Uralensis Attenuates Scopolamine-Induced Cognitive Disorder. Appl. Sci. 2023, 13, 3690. [Google Scholar] [CrossRef]
- Reichman, W.; Coyne, A.; Amirneni, S.; Molino, B.; Egan, S. Negative Symptoms in Alzheimer’s Disease. Am. J. Psychiatry 1996, 153, 424–426. [Google Scholar] [CrossRef]
- Kosik, K.S.; Joachim, C.L.; Selkoe, D.J. Microtubule-Associated Protein Tau (Tau) Is a Major Antigenic Component of Paired Helical Filaments in Alzheimer Disease. Proc. Natl. Acad. Sci. USA 1986, 83, 4044–4048. [Google Scholar] [CrossRef] [PubMed]
- Pluta, R.; Ułamek-Kozioł, M.; Januszewski, S.; Czuczwar, S.J. Tau Protein Dysfunction after Brain Ischemia. J. Alzheimers. Dis. 2018, 66, 429–437. [Google Scholar] [CrossRef]
- Bolourchi, P. MCI Conversion Prediction Using 3D Zernike Moments and the Improved Dynamic Particle Swarm Optimization Algorithm. Appl. Sci. 2023, 13, 4489. [Google Scholar] [CrossRef]
- Chandra, A.; Dervenoulas, G.; Politis, M.; Initiative, A.D.N. Magnetic resonance imaging in Alzheimer’s disease and mild cognitive impairment. J. Neurol. 2019, 266, 1293–1302. [Google Scholar] [CrossRef] [Green Version]
- Çalişkan, A.; Çevik, U. An Efficient Noisy Pixels Detection Model for CT Images Using Extreme Learning Machines. Teh. Vjesn. 2018, 25, 679–686. [Google Scholar]
- Ashburner, J.; Friston, K.J. Voxel-Based Morphometry--the Methods. Neuroimage 2000, 11, 805–821. [Google Scholar] [CrossRef] [Green Version]
- Brambati, S.M.; Renda, N.C.; Rankin, K.P.; Rosen, H.J.; Seeley, W.W.; Ashburner, J.; Weiner, M.W.; Miller, B.L.; Gorno-Tempini, M.L. A Tensor Based Morphometry Study of Longitudinal Gray Matter Contraction in FTD. Neuroimage 2007, 35, 998–1003. [Google Scholar] [CrossRef] [Green Version]
- Lai, K.-L.; Niddam, D.M.; Fuh, J.-L.; Chen, W.-T.; Wu, J.-C.; Wang, S.-J. Cortical Morphological Changes in Chronic Migraine in a Taiwanese Cohort: Surface- and Voxel-Based Analyses. Cephalalgia 2020, 40, 575–585. [Google Scholar] [CrossRef] [PubMed]
- Cao, X.; Yang, F.; Zheng, J.; Wang, X.; Huang, Q. Aberrant Structure MRI in Parkinson’s Disease and Comorbidity with Depression Based on Multinomial Tensor Regression Analysis. J. Pers. Med. 2022, 12, 89. [Google Scholar] [CrossRef] [PubMed]
- Saglam, M.; Spataru, C.; Karaman, O.A. Forecasting Electricity Demand in Turkey Using Optimization and Machine Learning Algorithms. Energies 2023, 16, 4499. [Google Scholar] [CrossRef]
- Erkan, E.; Arserim, M.A. Mobile Robot Application with Hierarchical Start Position DQN. Comput. Intell. Neurosci. 2022, 2022, 4115767. [Google Scholar] [CrossRef]
- Çinarer, G.; Emiroğlu, B.G.; Yurttakal, A.H. Prediction of Glioma Grades Using Deep Learning with Wavelet Radiomic Features. Appl. Sci. 2020, 10, 6296. [Google Scholar] [CrossRef]
- Aydin, I.; Yaman, O.; Karakose, M.; Celebi, S.B. Particle Swarm Based Arc Detection on Time Series in Pantograph-Catenary System. In Proceedings of the 2014 IEEE International Symposium on Innovations in Intelligent Systems and Applications (INISTA) Proceedings, Alberobello, Italy, 23–35 June 2014; IEEE: Piscataway, NJ, USA, 2014. [Google Scholar]
- Golestani, R.; Gharbali, A.; Nazarbaghi, S. Assessment of Linear Discrimination and Nonlinear Discrimination Analysis in Diagnosis Alzheimer’s Disease in Early Stages. Adv. Alzheimer. Dis. 2020, 09, 21–32. [Google Scholar] [CrossRef]
- Syaifullah, A.H.; Shiino, A.; Kitahara, H.; Ito, R.; Ishida, M.; Tanigaki, K. Machine Learning for Diagnosis of AD and Prediction of MCI Progression from Brain MRI Using Brain Anatomical Analysis Using Diffeomorphic Deformation. Front. Neurol. 2020, 11, 576029. [Google Scholar] [CrossRef]
- Vedalankar, A.V.; Gupta, S.S.; Manthalkar, R.R. Addressing Architectural Distortion in Mammogram Using AlexNet and Support Vector Machine. Inform. Med. Unlocked 2021, 23, 100551. [Google Scholar] [CrossRef]
- Themistocleous, C.; Eckerström, M.; Kokkinakis, D. Identification of Mild Cognitive Impairment from Speech in Swedish Using Deep Sequential Neural Networks. Front. Neurol. 2018, 9, 975. [Google Scholar] [CrossRef]
- Lee, S.; Kim, J.; Kang, H.; Kang, D.-Y.; Park, J. Genetic Algorithm Based Deep Learning Neural Network Structure and Hyperparameter Optimization. Appl. Sci. 2021, 11, 744. [Google Scholar] [CrossRef]
- Çalışkan, A. Detecting Human Activity Types from 3D Posture Data Using Deep Learning Models. Biomed. Signal Process. Control. 2023, 81, 104479. [Google Scholar] [CrossRef]
- Birecikli, B.; Karaman, Ö.A.; Çelebi, S.B.; Turgut, A. Failure Load Prediction of Adhesively Bonded GFRP Composite Joints Using Artificial Neural Networks. J. Mech. Sci. Technol. 2020, 34, 4631–4640. [Google Scholar] [CrossRef]
- Islam, J.; Zhang, Y. Brain MRI Analysis for Alzheimer’s Disease Diagnosis Using an Ensemble System of Deep Convolutional Neural Networks. Brain Inform. 2018, 5, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, J.; Chen, M.; Li, Y.; Gao, Y.; Li, Y.; Cai, S.; Wang, J. Multisite Autism Spectrum Disorder Classification Using Convolutional Neural Network Classifier and Individual Morphological Brain Networks. Front. Neurosci. 2020, 14, 629630. [Google Scholar] [CrossRef] [PubMed]
- Karaman, Ö.A.; Tanyıldızı Ağır, T.; Arsel, İ. Estimation of Solar Radiation Using Modern Methods. Alex. Eng. J. 2021, 60, 2447–2455. [Google Scholar] [CrossRef]
- Aydin, I.B.; Celebi, S.B.; Barmada, S.; Tucci, M. Fuzzy Integral-Based Multi-Sensor Fusion for Arc Detection in the Pantograph-Catenary System. Proc. Inst. Mech. Eng. 2018, 232, 159–170. [Google Scholar] [CrossRef]
- Kumari, R.; Nigam, A.; Pushkar, S. An Efficient Combination of Quadruple Biomarkers in Binary Classification Using Ensemble Machine Learning Technique for Early Onset of Alzheimer Disease. Neural Comput. Appl. 2022, 34, 11865–11884. [Google Scholar] [CrossRef]
- Gunawardena, K.A.N.N.P.; Rajapakse, R.N.; Kodikara, N.D. Applying Convolutional Neural Networks for Pre-Detection of Alzheimer’s Disease from Structural MRI Data. In Proceedings of the 2017 24th International Conference on Mechatronics and Machine Vision in Practice (M2VIP), Auckland, New Zealand, 21–23 November 2017; IEEE: Piscataway, NJ, USA, 2017. [Google Scholar]
- Cruz, R.S.; Lebrat, L.; Bourgeat, P.; Dore, V.; Dowling, J.; Fripp, J.; Fookes, C.; Salvado, O. Going Deeper with Brain Morphometry Using Neural Networks. In Proceedings of the 2021 IEEE 18th International Symposium on Biomedical Imaging (ISBI), Nice, France, 13–16 April 2021; IEEE: Piscataway, NJ, USA, 2021. [Google Scholar]
- Savaş, S. Detecting the Stages of Alzheimer’s Disease with Pre-Trained Deep Learning Architectures. Arab. J. Sci. Eng. 2022, 47, 2201–2218. [Google Scholar] [CrossRef]
- Turkson, R.E.; Qu, H.; Mawuli, C.B.; Eghan, M.J. Classification of Alzheimer’s Disease Using Deep Convolutional Spiking Neural Network. Neural Process. Lett. 2021, 53, 2649–2663. [Google Scholar] [CrossRef]
- Farooq, A.; Anwar, S.; Awais, M.; Rehman, S. A Deep Cnn Based Multi-Class Classifcation of Alzheimer’s Disease Using MRI. In Proceedings of the 2017 IEEE International Conference on Imaging systems and techniques (IST), Beijing, China, 18–20 October 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 1–6. [Google Scholar]
- Xia, Z.; Yue, G.; Xu, Y.; Feng, C.; Yang, M.; Wang, T.; Lei, B. A Novel End-to-End Hybrid Network for Alzheimer’s Disease Detection Using 3D CNN and 3D CLSTM. In Proceedings of the 2020 IEEE 17th International Symposium on Biomedical Imaging (ISBI), Iowa City, IA, USA, 3–7 April 2020; IEEE: Piscataway, NJ, USA, 2020. [Google Scholar]
- Ashraf, A.; Naz, S.; Shirazi, S.H.; Razzak, I.; Parsad, M. Deep Transfer Learning for Alzheimer Neurological Disorder Detection. Multimed. Tools Appl. 2021, 80, 30117–30142. [Google Scholar] [CrossRef]
- Mehmood, A.; Yang, S.; Feng, Z.; Wang, M.; Ahmad, A.S.; Khan, R.; Maqsood, M.; Yaqub, M. A Transfer Learning Approach for Early Diagnosis of Alzheimer’s Disease on MRI Images. Neuroscience 2021, 460, 43–52. [Google Scholar] [CrossRef]
- Matsuda, H. MRI Morphometry in Alzheimer’s Disease. Ageing Res. Rev. 2016, 30, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Sato, R.; Kudo, K.; Udo, N.; Matsushima, M.; Yabe, I.; Yamaguchi, A.; Tha, K.K.; Sasaki, M.; Harada, M.; Matsukawa, N.; et al. A Diagnostic Index Based on Quantitative Susceptibility Mapping and Voxel-Based Morphometry May Improve Early Diagnosis of Alzheimer’s Disease. Eur. Radiol. 2022, 32, 4479–4488. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Avants, B.; Patel, S.; Whyte, J.; Coslett, B.H.; Pluta, J.; Detre, J.A.; Gee, J.C. Structural Consequences of Diffuse Traumatic Brain Injury: A Large Deformation Tensor-Based Morphometry Study. Neuroimage 2008, 39, 1014–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aggarwal, A.N.; Agarwal, R.; Gupta, D.; Dhooria, S.; Behera, D. Correction for Aggarwal Et Al., Interferon Gamma Release Assays for Diagnosis of Pleural Tuberculosis: A Systematic Review and Meta-analysis. J. Clin. Microbiol. 2016, 54, 2451–2459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hua, X.; Leow, A.D.; Parikshak, N.N.; Lee, S.; Chiang, M.C.; Toga, A.W.; Jack, C.R.; Weiner, M.W.; Thompson, P.M. Tensor-based Morphometry as a Neuroimaging Biomarker for Alzheimer’s Disease: An MRI Study of 676 AD, MCI, and Normal Subjects. Neuroimage 2008, 43, 458–469. [Google Scholar] [CrossRef] [Green Version]
- Hua, X.; Hibar, D.P.; Ching, C.R.K.; Boyle, C.P.; Rajagopalan, P.; Gutman, B.A.; Leow, A.D.; Toga, A.W.; Jack, C.R.J.; Harvey, D.; et al. Unbiased Tensor-Based Morphometry: Improved Robustness and Sample Size Estimates for Alzheimer’s Disease Clinical Trials. Neuroimage 2013, 66, 648–661. [Google Scholar] [CrossRef] [Green Version]
- O’Shea, R.J.; Sharkey, A.R.; Cook, G.J.R.; Goh, V. Systematic Review of Research Design and Reporting of Imaging Studies Applying Convolutional Neural Networks for Radiological Cancer Diagnosis. Eur. Radiol. 2021, 31, 7969–7983. [Google Scholar] [CrossRef]
- Qian, S.; Liu, H.; Liu, C.; Wu, S.; Wong, H.S. Adaptive Activation Functions in Convolutional Neural Networks. Neurocomputing 2018, 272, 204–212. [Google Scholar] [CrossRef]
- Zhang, S.; Li, C.; Ye, W. Damage Localization in Plate-like Structures Using Time-Varying Feature and One-Dimensional Convolutional Neural Network. Mech. Syst. Signal Process. 2021, 147, 107107. [Google Scholar] [CrossRef]
- Low, J.X.; Choo, K.W. Classification of Heart Sounds Using Softmax Regression and Convolutional Neural Network. In Proceedings of the 2018 International Conference on Communication Engineering and Technology, Singapore, 24–26 February 2018; ACM: New York, NY, USA, 2018. [Google Scholar]
- Huang, H.; Zheng, S.; Yang, Z.; Wu, Y.; Li, Y.; Qiu, J.; Cheng, Y.; Lin, P.; Lin, Y.; Guan, J.; et al. Voxel-Based Morphometry and a Deep Learning Model for the Diagnosis of Early Alzheimer’s Disease Based on Cerebral Gray Matter Changes. Cereb. Cortex 2023, 33, 754–763. [Google Scholar] [CrossRef]
- Chollet, F. Xception: Deep Learning with Depthwise Separable Convolutions. In Proceedings of the IEEE conference on computer vision and pattern recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 1251–1258. [Google Scholar]
- Rajinikanth, V.; Joseph Raj, A.N.; Thanaraj, K.P.; Naik, G.R. A Customized VGG19 Network with Concatenation of Deep and Handcrafted Features for Brain Tumor De-tection. Appl. Sci. 2020, 10, 3429. [Google Scholar] [CrossRef]
- Syed, A.H.; Khan, T.; Khan, S.A. Deep Transfer Learning Techniques-Based Auto-mated Classification and Detection of Pulmonary Fibrosis from Chest CT Images. Pro-Cesses 2023, 11, 443. [Google Scholar] [CrossRef]
- Krstinić, D.; Braović, M.; Šerić, L.; Božić-Štulić, D. Multi-Label Classifier Performance Evaluation with Confusion Matrix. In Proceedings of the Computer Science & Information Technology, Dubai, United Arab Emirates, 28–29 November 2020; AIRCC Publishing Corporation: Chennai, India, 2020. [Google Scholar]
- Safari, S.; Baratloo, A.; Elfil, M.; Negida, A. Evidence Based Emergency Medicine Part 2: Positive and Negative Predictive Values of Diagnostic Tests. Emergency 2015, 3, 87–88. [Google Scholar]
- Héberger, K.; Kollár-Hunek, K. Sum of Ranking Differences for Method Discrimination and Its Validation: Comparison of Ranks with Random Numbers. J. Chemom. 2011, 25, 151–158. [Google Scholar] [CrossRef]
- Yang, L.; Hanneke, S.; Carbonell, J. A Theory of Transfer Learning with Applications to Active Learning. Mach. Learn. 2013, 90, 161–189. [Google Scholar] [CrossRef]
- Buvaneswari, P.R.; Gayathri, R. Deep Learning-Based Segmentation in Classification of Alzheimer’s Disease. Arab. J. Sci. Eng. 2021, 46, 5373–5383. [Google Scholar] [CrossRef]
- Chen, S.; Zhang, J.; Wei, X.; Zhang, Q. Alzheimer’s Disease Classification Using Structural MRI Based on Convolutional Neural Networks. In Proceedings of the 2020 2nd International Conference on Big-data Service and Intelligent Computation, Xiamen China, 3–5 December 2020; ACM: New York, NY, USA, 2020. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | CN | MCI | AD |
|---|---|---|---|
| Number | 54 | 88 | 28 |
| Gender (M/F) | 30/24 | 47/41 | 16/12 |
| Age (mean ± std) | 74.4 ± 5.5 year | 73.8 ± 5.4 years | 75.0 ± 5.0 year |
| Data Set | AD | CN | MCI | Total Scans |
|---|---|---|---|---|
| Training set | 246 | 491 | 811 | 1548 |
| Validation set | 62 | 123 | 203 | 388 |
| Test set | 84 | 126 | 196 | 406 |
| Layer | Output Shape | Parameter |
|---|---|---|
| Flatten | (18,432) | 0 |
| Dense | (128) | 2,359,424 |
| dropout | (128) | 0 |
| dense | (64) | 8256 |
| dropout | (64) | 0 |
| flatten | (64) | 0 |
| dense | (3) | 195 |
| Total Parameter | 23,229,355 | |
| Training Parameters | ||||||
|---|---|---|---|---|---|---|
| Learning Rate | Batch Size | Optimizer | Loss Function | Number of Epochs | Re-Scaling | Metrics |
| 1 × 10−3 | 32 | Adam | Categorical crossentopy | 200 | 1/0.255 | accuracy |
| Classes | Original Data | Augmentation Techniques | ||
|---|---|---|---|---|
| Rotation | Flipping | Zoom | ||
| 45° | Horizontal | (20%) | ||
| AD | 308 | 308 | 308 | 308 |
| CN | 614 | 614 | 614 | 614 |
| MCI | 1014 | 1014 | 1014 | 1014 |
| Total | 1936 | 5808 | ||
| Models | Training Accuracy | Validation Accuracy | Test (Macro Avg) | ||||
|---|---|---|---|---|---|---|---|
| Accuracy | Specificity | Precision | Sensitivity | F1-Score | |||
| VGG-16 + PPC | 94.98% | 90.55% | 89.66% | 94.94 | 87.94 | 89.04 | 88.14 |
| VGG-19 + PPC | 95.63% | 93.39% | 91.63% | 95.89 | 90.07 | 90.89 | 90.32 |
| ResNet-50V2 + PPC | 97.54% | 94.01% | 93.35% | 96.59 | 92.41 | 92.82 | 92.57 |
| Xception + PPC | 97.60% | 95.89% | 95.81% | 97.92 | 95.01 | 95.41 | 95.21 |
| Models | Class | Precision | Sensitivity | F1-Score | Accuracy |
|---|---|---|---|---|---|
| VGG-16 + PPC | AD | 0.78 | 0.93 | 0.85 | 89.66% |
| CN | 0.91 | 0.79 | 0.85 | ||
| MCI | 0.95 | 0.95 | 0.95 | ||
| Macro Average | 0.88 | 0.89 | 0.88 | ||
| VGG-19 + PPC | AD | 0.80 | 0.90 | 0.85 | 91.63% |
| CN | 0.95 | 0.87 | 0.91 | ||
| MCI | 0.95 | 0.95 | 0.95 | ||
| Macro Average | 0.90 | 0.91 | 0.90 | ||
| ResNet-50V2 + PPC | AD | 0.88 | 0.93 | 0.90 | 93.35% |
| CN | 0.94 | 0.90 | 0.92 | ||
| MCI | 0.95 | 0.96 | 0.96 | ||
| Macro Average | 0.92 | 0.93 | 0.93 | ||
| Xception + PPC | AD | 0.92 | 0.94 | 0.93 | 95.81% |
| CN | 0.95 | 0.95 | 0.95 | ||
| MCI | 0.98 | 0.97 | 0.97 | ||
| Macro Average | 0.95 | 0.95 | 0.95 |
| Models | Accuracy | Precision | Sensitivity | F1-Score | Training Time (s) | Average Time Per Epoch (s) | Test Time (s) |
|---|---|---|---|---|---|---|---|
| VGG-16 (Baseline) | 85.96% | 84.08 | 85.49 | 84.55 | 2594.75 | 12,97 | 1.39 |
| VGG-19 (Baseline) | 87.44% | 86.02 | 86.98 | 86.45 | 3174.44 | 15.87 | 4.77 |
| ResNet-50V2 (Baseline) | 87.93% | 86.60 | 87.13 | 86.81 | 2749.96 | 13.74 | 5.52 |
| Xception (Baseline) | 89.16% | 88.10 | 88.76 | 88.35 | 2982.52 | 14,91 | 4.72 |
| VGG-16 + PPC | 89.66% | 87.94 | 89.04 | 88.14 | 3192.16 | 15.96 | 1.91 |
| VGG-19 + PPC | 91.63% | 90.07 | 90.89 | 90.32 | 2844.81 | 14.22 | 4.88 |
| ResNet-50V2 + PPC | 93.35% | 92.41 | 92.82 | 92.57 | 2668.44 | 13.34 | 3.38 |
| Xception + PPC | 95.81% | 95.01 | 95.41 | 95.21 | 3130.86 | 15.65 | 5.04 |
| Reference | Biomarker | Database | Method(s) | ACC (AD, MCI, CN) | Participant | Approach |
|---|---|---|---|---|---|---|
| [32] | MRI | ADNI | SNN + CNN | NC/AD: 90.15% | 450 | ROI |
| MCI/AD: 87.30% | ||||||
| NC/MCI: 83.90% | ||||||
| NC/MCI: 87% | ||||||
| MCI/AD: 68% | ||||||
| [54] | VBM | ADNI | SegNet + ResNet-101 | AD/CN/MCI: 96% | 240 | ROI |
| [55] | VBM | ADNI | LeNet | NC/AD: 93.83% | 479 | 3D subject level |
| AlexNet | NC/AD: 96.22% | |||||
| VGGNet | NC/AD: 96.08% | |||||
| GoogLeNet | NC/AD: 97.15% | |||||
| ResNet | NC/AD: 94.60% | |||||
| [56] | VBM | ADNI | CNN | MCI: 80.9% | 188 | 3D subject level |
| In this study | TBM | ADNI | Xception + PPC | AD/CN/MCI: %95.81 | 170 | ROI |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Çelebi, S.B.; Emiroğlu, B.G. A Novel Deep Dense Block-Based Model for Detecting Alzheimer’s Disease. Appl. Sci. 2023, 13, 8686. https://doi.org/10.3390/app13158686
Çelebi SB, Emiroğlu BG. A Novel Deep Dense Block-Based Model for Detecting Alzheimer’s Disease. Applied Sciences. 2023; 13(15):8686. https://doi.org/10.3390/app13158686
Chicago/Turabian StyleÇelebi, Selahattin Barış, and Bülent Gürsel Emiroğlu. 2023. "A Novel Deep Dense Block-Based Model for Detecting Alzheimer’s Disease" Applied Sciences 13, no. 15: 8686. https://doi.org/10.3390/app13158686
APA StyleÇelebi, S. B., & Emiroğlu, B. G. (2023). A Novel Deep Dense Block-Based Model for Detecting Alzheimer’s Disease. Applied Sciences, 13(15), 8686. https://doi.org/10.3390/app13158686