1. Introduction
The success of oral rehabilitation in patients undergoing implant treatment largely depends on the health of the tissues. As the oral cavity is a dynamic system, continuously colonised by interacting and proliferating microorganisms, it is extremely important to understand the microbiota and control causal factors before, during, and after implant placement to prevent the development of peri-implant disease [
1,
2].
Oral microbiota differ in everyone and, when in balance, these microorganisms do not cause any harm to the oral structure, a phenomenon known as eubiosis, characterised by a mutual beneficial relationship and a defence mechanism against other species [
1]. However, alterations in the host’s immune system, pH changes, decreased salivary flow, altered activity of salivary proteins, diet (high carbohydrate consumption), poor oral hygiene, tobacco use, diabetes, prolonged use of oral antibiotics/antimicrobials/antiseptics and genetic factors can lead to microbial imbalances. Under these circumstances, virulent and opportunistic microorganisms in dysbiosis can cause periodontal and peri-implant diseases [
1,
2,
3].
In peri-implant disease, the biofilm has been reported to contain significant amounts of Gram-negative bacteria, such as
Porphyromonas gingivalis,
Treponema denticola,
Tannerella forsythia and
Aggregatibacter actinomycetemcomitans, but
Candida spp.,
E. faecalis and
P. aeruginosa have also been found in implants with peri-implantitis [
4,
5,
6,
7].
Candida species in the oral cavity are commensal and it has been suggested that the subgingival environment can serve as a refuge, where, under favourable conditions, they can transform into opportunistic pathogens and induce oral diseases [
8,
9,
10].
P. aeruginosa is one of the most common microorganisms in healthcare-associated infections, with high mortality rates, especially in severely ill and immunocompromised patients. It is an opportunistic human pathogen characterised by intrinsic resistance to multiple antimicrobial agents. A recent study found significantly higher levels of
P. aeruginosa in oral epithelial cells of individuals with periodontitis compared to individuals with a healthy periodontium [
11]. In addition, El-Telbany M et al., 2022, isolated
P. aeruginosa in 3 out of 30 cases of peri-implantitis, demonstrating that in addition to its difficult elimination when organised in a biofilm, it also showed resistance to 13 out of 16 antibiotics tested, suggesting that resistance to antimicrobials of opportunistic pathogens in peri-implantitis has led to an urgent need to create alternative treatments to antibiotics for the treatment of these infections [
12].
E. faecalis are facultative anaerobic Gram-positive cocci. They are rarely found in the oral cavity under healthy conditions, but have a high occurrence in failed endodontic treatments, persistent periapical lesions, chronic periodontitis and have also been detected in cases of peri-implantitis [
4].
If peri-implantitis is not diagnosed and treated early, extensive bone loss will occur and compromise implant stability; therefore, microbiological diagnosis is important for a more appropriate and effective treatment.
In Portugal, as far as we know, there are no studies that have evaluated the prevalence of these opportunistic pathogens in implants and adjacent teeth and the implications both in terms of antibiotic prophylaxis and treatment that the presence of these microorganisms represents.
The aimed of this study was to detect Candida spp., E. faecalis and P. aeruginosa in the periodontal and peri-implant subgingival plaque with or without disease presence and to seek a correlation between the presence of these microorganisms and demographic data, hygiene habits, endodontic treatment and implant connection type.
3. Results
A total of 20 individuals with ages ranging from 26 to 86 years (mean = 52.25;
SD = 15.1), 70% of whom were female (
n = 14) with a mean age = 53.57, and 30% of whom were male (
n = 6) with a mean age = 49.16, agreed to participate in this study. The demographic characteristics, clinical parameters of the study population and collection sites are presented in
Table 1 and
Table 2, respectively. The analysed data regarding oral hygiene habits showed that 65% (
n = 13) brushed their teeth twice a day, with the majority, 85% (
n = 17), not using dental floss and 70% (
n = 14) not using an irrigator. Regarding smoking habits, 90% (
n = 18) were non-smokers, while the remaining 10% (
n = 2) had this habit. A total of 90% of the patients (
n = 18) did not have removable prostheses, while 10% (
n = 2) did. As for the presence of endodontic treatment, 80% (
n = 16) had one or more treated teeth. The study population included 25% (
n = 5) of patients with edentulous maxillae rehabilitated with prostheses supported by internal connection implants, 25% (
n = 5) with single-unit Cone morse connection implants, 20% (
n = 4) with single-unit internal connection implants, 15% (
n = 3) with single-unit external connection implants and 10% (
n = 2) rehabilitated with pontics up to three elements with an internal connection, while 5% (
n = 1) were Cone morse implants.
In
Figure 1, we can observe the distribution of the studied microorganisms. However, it is important to mention that numbers 4, 6, 16, 19 and 20 correspond to implant-supported complete dentures, which means the absence of teeth (which were not analysed).
For all positive cases of
E. faecalis,
Candida spp. and
P. aeruginosa, their relationship with the periodontal and peri-implant diagnosis was analysed through the following graphs, which showed a higher presence of these three opportunistic pathogens in both periodontal and peri-implant disease (
Figure 2).
All positive cases for the three microorganisms mostly had a diagnosis of periodontal and peri-implant disease. When comparing the presence of microorganisms according to the sampling site (peri-implant or periodontal subgingival plaque—
Table 1), it was observed that
E. faecalis had equal median values of CFU/mL in the adjacent tooth and the implant, although the values in the implant showed greater variability.
Candida spp. had higher median values in the implant (1.00 × 10
7 [1.00 × 10
6; 77,500,000.0]), compared to the adjacent tooth (500,040.0 [18.75; 25,750,000.0]), but these differences were not statistically significant.
P. aeruginosa also showed a higher CFU/mL in the peri-implant compared to the periodontal subgingival plaque of the adjacent tooth, but these differences did not reach statistical significance.
When comparing the values of
E. faecalis in individuals who underwent endodontic treatment with those who did not undergo endodontic treatment, it was found that those who underwent treatment had higher median values of
E. faecalis CFU/mL (1.00 × 10
6 [1.00 × 10
7; 1.00 × 10
8]) compared to those who did not undergo treatment (1.00 × 10
6 [1.00 × 10
6; 1.00 × 10
7]). However, these differences are not statistically significant (
Table 2).
Through
Table 3, we can observe that
E. faecalis had higher median values of CFU/mL in individuals with mucositis (1.00 × 10
7 [1.00 × 10
7; 1.00 × 10
8]), compared to individuals with peri-implant health (1.00 × 10
6 [750,003.75; 32,500,000.0]) and peri-implantitis (5,500,000.0 [1.00 × 10
6; 32,500,000.0]); however, these differences are not statistically significant.
When analysing the presence or absence of differences in the number of CFU/mL of
Candida spp. between individuals who use or do not use an irrigator, it was found that out of the six individuals who were positive for
Candida spp., the five individuals who did not use an irrigator had higher median values (1.00 × 10
7 [1.00 × 10
7; 1.00 × 10
7]) compared to the individual who used an irrigator (1.00 × 10
6 [1.00 × 10
6; 1.00 × 10
6])and these differences were statistically significant (
p = 0.025) (
Table 4).
The comparison of the number of CFU/mL of the microorganisms among the different types of implant connection was performed using the Kruskal–Wallis test (
Table 5), which revealed that individuals with Cone morse implants had significantly higher CFU/mL values of
E. faecalis (1.00 × 10
8 [1.00 × 10
7; 1.00 × 10
8]) compared to individuals with external hexagon (1.00 × 10
7 [1.00 × 10
7; 1.00 × 10
7]) and internal hexagon (1.00 × 10
6 [1.00 × 10
6; 1.00 × 10
7]]) implants (
H = 10.3;
p = 0.007). These differences were observed specifically between Cone morse and internal hexagon implants (
p = 0.005). Regarding the number of CFU/mL of
Candida spp., all three types of implants showed equal median values. As for
P. aeruginosa, individuals with Cone morse implants had higher CFU/mL values compared to internal hexagon and external hexagon implants, respectively, but these differences did not reach statistical significance.
When we examined the relationship between age and the presence of these three microorganisms (
Table 6), a weak to moderate negative correlation was found with
E. faecalis,
Candida spp. and
P. aeruginosa, but this did not reach statistical significance. The older the age, the higher the presence of these microorganisms in both the peri-implant and periodontal subgingival plaque of adjacent teeth.
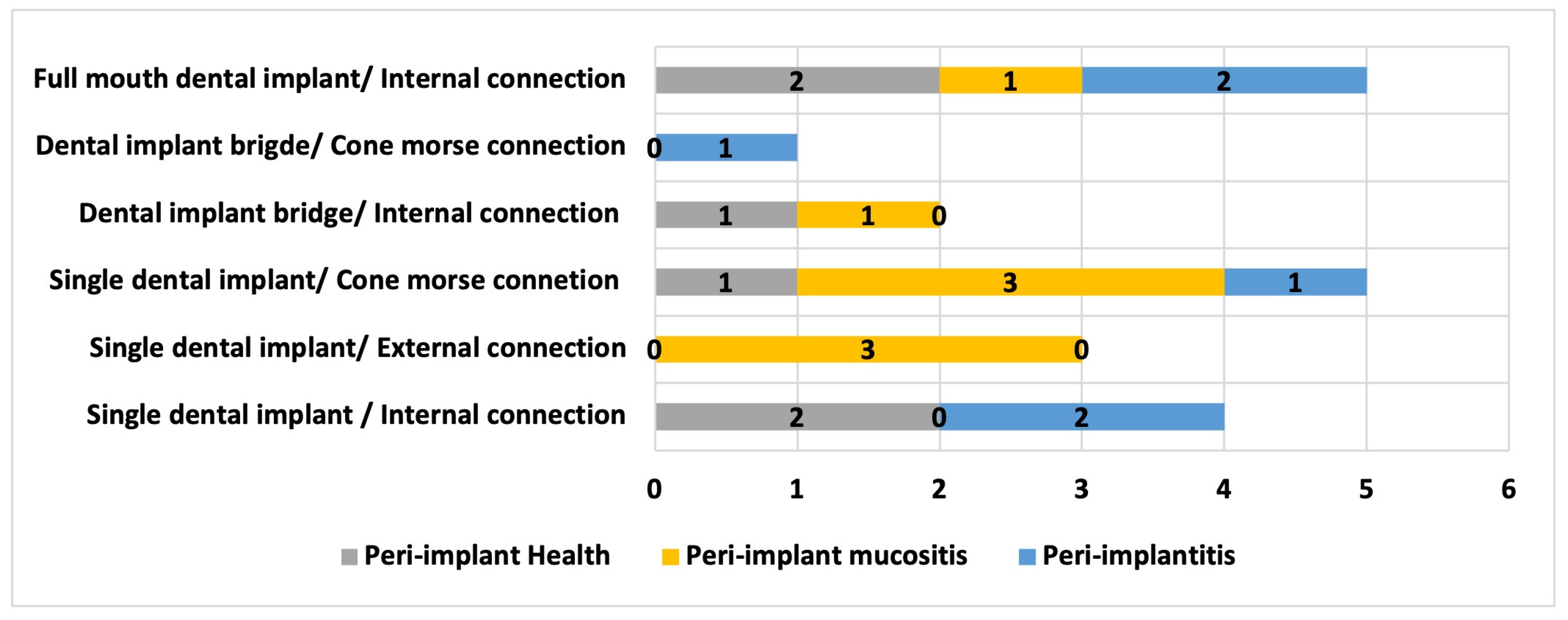
In
Figure 3, the relationship between the type of rehabilitation and the type of implant connection with the peri-implant diagnosis is presented, where it can be observed that there is a higher number of peri-implantitis cases in implants with internal connection.
4. Discussion
Approximately 10% of titanium implants present with premature failure, mainly due to bacterial infection within the first year of placement [
14].
Leonhardt et al., in 2003, evaluated the microflora in peri-implant lesions and demonstrated that facultative anaerobic periodontal pathogens and opportunistic species, such as
Staphylococcus spp.,
Enterococcus spp.,
Candida spp. and
P. aeruginosa, were also found around compromised implants [
15]. A recent study also found significantly higher levels of
P. aeruginosa in oral epithelial cells of individuals with periodontitis compared to those with a healthy periodontium [
11]. In our study, when we correlated the number of CFU/mL of
E. faecalis with peri-implant health, peri-implant mucositis and peri-implantitis, the median values were higher in peri-implant mucositis than in peri-implantitis, although these differences were not statistically significant. However, it should be noted that undiagnosed and untreated peri-implant mucositis can progress to peri-implantitis. Based on the Consensus Report of the Sixth European Workshop on Periodontology, Lindhe and Meyle reported an incidence of peri-implant mucositis of up to 80% and incidence of peri-implantitis between 28% and 56% [
13]. Several studies have quantified the incidence of peri-implantitis development in patients with a history of periodontitis, indicating that it is about six times more prevalent in patients with periodontitis than in patients without a history of periodontal disease. Other research indicates that teeth can be a source of bacteria in partially edentulous patients who have been rehabilitated with dental implants [
16,
17]. Regarding our study, we found that the majority of individuals diagnosed with periodontal disease (gingivitis and periodontitis) also had a diagnosis of peri-implant disease in the selected implant (peri-implant mucositis and peri-implantitis).
In our study, when we analysed the number of CFU/mL of Candida spp. among individuals who used an irrigator and those who did not; we found that those who did not use an irrigator had higher median values compared to the individual who used an irrigator, and these differences were statistically significant. These data, although requiring further investigation regarding the usefulness of the irrigator in reducing the colonisation of peri-implant tissues, particularly by Candida species, may indicate an effect of this hygiene method, such as the cleansing action of saliva, preventing the presence of yeast in peri-implant plaque formation.
Alrabiah et al. reported that the subgingival environment can serve as a refuge for various
Candida species [
8]. In addition to adhering to teeth and oral mucosal surfaces, yeast can also adhere to non-biological surfaces such as titanium implants. While the presence of oral
Candida species in the subgingival region plays a role in the aetiopathogenesis of periodontal diseases (such as chronic periodontitis and aggressive periodontitis), the contribution of oral yeast to the occurrence and progression of peri-implant diseases remains uncertain [
18]. As in the study by Alrabiah et al., a higher presence of
Candida was found in individuals with peri-implantitis compared to those without peri-implantitis. In our study, all cases of peri-implantitis revealed the presence of
Candida spp.
Some risk factors associated with an increased oral presence of
Candida include smoking and compromised oral hygiene status. These are the same risk factors that have been shown to increase the risk of peri-implant diseases. The results of the present study are in line with the study by Darwazeh et al., which showed a significantly higher presence of
Candida in patients with poor oral hygiene [
19].
According to Flanagan et al.,
E. faecalis is present in the majority of endodontic infections and is difficult to eliminate through endodontic treatment, so it can persist in the root canals and the surrounding alveolar bone. This bacterium often remains in the alveolar bone after the extraction of these teeth and can colonise the implant after its placement, which can lead to marginal bone loss and, consequently, implant loss. Although there are few studies linking
E. faecalis to peri-implant disease, it appears to play a key role in bone loss around the implant or in peri-implantitis. This author even suggests that
E. faecalis can cause infection both individually and in multi-species [
20]. When comparing the median CFU/mL values of
E. faecalis in individuals with endodontically treated teeth and those without endodontic treatment, it was found that those who underwent endodontic treatment had higher median CFU/mL values of
E. faecalis than those who did not. Although these differences were not statistically significant, the role of endodontically treated teeth adjacent to implants should be further analysed to evaluate their role in the colonisation of peri-implant plaque and the development of peri-implantitis.
Various modifications to implant design have been made in recent years to reduce the space between the implant and the prosthetic component to reduce bacterial proliferation, but with limited success. Generally, implants have a polished cervical collar that prevents the adhesion of microorganisms, as the connector region is in contact with soft tissues and not intraosseous [
21]. High roughness and hydrophilicity are suggestive of an important role in bacterial adhesion and colonisation on implant surfaces, but they also have benefits for the process of osseointegration [
22]. In addition, although studies suggest that there is no significant difference regarding the shape or macrostructure of the implant (external or internal connection), the external connection shows a greater response of the soft tissues due to infiltration [
23,
24].
In our study, the highest bacterial colonisation by
E. faecalis and
P. aeruginosa was found in implants with Morse taper connections, while the lowest was associated with implants with internal hexagon connections, contradicting the results of the study by Romanos et al. in 2016, which found that prosthetic components with Cone morse connections had lower bacterial counts, since this type of connection has a frictional locking system that allows for intimate adaptation in the deeper internal portions of the system, reducing micro-movements during loading. However, in the study by Romanos et al., a higher quantity of
Prevotella,
Selenomonas, Eubacterium and
Fusobacterium was detected in the internal connection, and only Ochrobactrum was detected in the Cone morse taper connection, which were not analysed in our study. Khorshidi et al., in 2016, also concluded that, overall, the Cone morse connection seems to have an obvious advantage in terms of microbial sealing capability, although their study mainly focused on the presence of
Streptococcus mutans [
25].


 ,
, 




{kind=link}
{kind=link}
{kind=link}