
Epidemiology and Time-Loss Shoulder Injuries in Professional South African Rugby Players: A Prospective Study That Focuses on Real-Time Collision Data during a Tackle

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Considerations
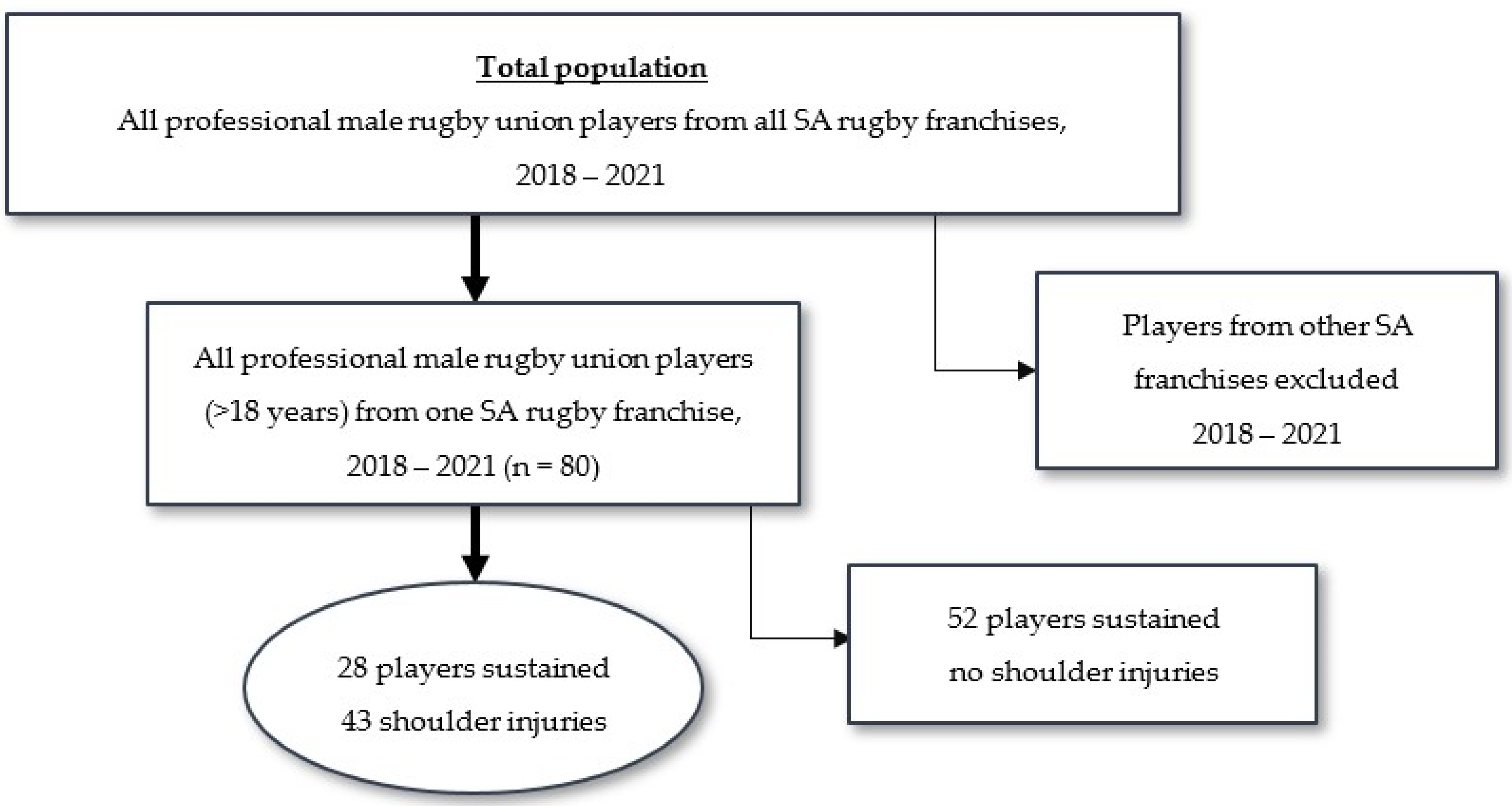
2.2. Participants
2.3. Data Collection
2.3.1. Definitions
2.3.2. GPS Data Collection
2.3.3. Injury Data Collection
2.3.4. Physical Outcome Variables and Specific Parameters Measured
2.3.5. Calculation of Player Exposure
2.4. Data Analysis
3. Results
3.1. Demographic Data
3.2. Frequency, Period Prevalence, and Incidence of Shoulder Injuries
Shoulder Injuries by Player Position
3.3. Severity of Shoulder Injuries (Tissue and Pathology Type) in the Context of Momentum
3.4. Severity of Shoulder Injuries (Tissue and Pathology Type) in the Context of Match Intensity and Collision
Match Intensity of Each Reported Shoulder Injury
4. Discussion
Strengths and Limitations
5. Conclusions
Future Recommendation
- Area(s) of importance in the shoulder that need special conditioning attention are the AC joint, muscle/tendon and ligaments.
- Future research should investigate the potential risk factor analysis and the association between momentum and injuries.
- Future strength and conditioning research should evaluate various techniques, including tackle, breakdown, scrum, and maul skills, to decrease shoulder injury frequency and severity.
- Future research should note that the contact load/demand placed on specific positions during a training week is additional to match-play and uncontrollable, i.e., collisions per minute (frequency), intensity (meters per minute), and momentum (velocity variable) in contact scenarios.
- Future research should evaluate the function and protective factors that different protective wear offers in decreasing shoulder injury severity.
- In the current level of sport and participation, we recommend that healthcare workers focus specifically on shoulder injury prevention strategies in future research.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Donkin, C.; Venter, R.; Coetzee, D.; Kraak, W. Positional in-Match running demands of university rugby players in South Africa. Front. Psychol. 2020, 11, 1591. [Google Scholar] [CrossRef] [PubMed]
- Suarez-Arrones, L.; Portillo, J.; Pareja-Blanco, F.; de Villareal, E.S.; Sánchez-Medina, L.; Munguía-Izquierdo, D. Match-play activity profile in elite women’s rugby union players. J. Strength Cond. Res. 2014, 28, 452–458. [Google Scholar] [CrossRef]
- Roe, G.; Halkier, M.; Beggs, C.; Till, K.; Jones, B. The use of accelerometers to quantify collisions and running demands of rugby union match-play. Int. J. Perform. Anal. Sport 2016, 16, 590–601. [Google Scholar] [CrossRef]
- Sheehan, A.; Malone, S.; Walters, A.; Gabbett, T.; Collins, K. Match-play profile of elite rugby union, with special reference to repeated high-intensity effort activity (RHIE). Sport Sci. Health 2022, 18, 947–956. [Google Scholar] [CrossRef]
- Couderc, A.; Gabbett, T.J.; Piscione, J.; Robineau, J.; Peeters, A.; Igarza, G.; Thomas, C.; Hanon, C.; Lacome, M. Repeated high-intensity effort activity in international male rugby sevens. J. Strength Cond. Res. 2022, 24, 338–344. [Google Scholar] [CrossRef]
- Austin, D.J.; Gabbett, T.J.; Jenkins, D.G. Reliability and sensitivity of a repeated high-intensity exercise performance test for rugby league and rugby union. J. Strength Cond. Res. 2013, 27, 1128–1135. [Google Scholar] [CrossRef] [PubMed]
- Cunniffe, B.; Proctor, W.; Baker, J.S.; Davies, B. An evaluation of the physiological demands of elite rugby union using global positioning system tracking software. J. Strength Cond. Res. 2009, 23, 1195–1203. [Google Scholar] [CrossRef]
- Read, D.B.; Jones, B.; Phibbs, P.J.; Roe, G.A.; Darrall-Jones, J.D.; Weakley, J.J.; Till, K. Physical demands of representative match-play in adolescent rugby union. J. Strength Cond. Res. 2017, 31, 1290–1296. [Google Scholar] [CrossRef]
- Gabbett, T.J. Physiological and anthropometric characteristics of amateur rugby league players. Br. J. Sports Med. 2000, 34, 303–307. [Google Scholar] [CrossRef]
- Read, D.B.; Till, K.; Beasley, G.; Clarkson, M.; Heyworth, R.; Lee, J.; Weakley, J.J.; Phibbs, P.J.; Roe, G.A.; Darrall-Jones, J.; et al. Maximum running intensities during English academy rugby union match-play. Sci. Med. Footb. 2019, 3, 43–49. [Google Scholar] [CrossRef]
- Papalia, R.; Tecame, A.; Torre, G.; Narbona, P.; Maffulli, N.; Denaro, V. Rugby and shoulder trauma: A systematic review. Transl. Med. UniSa 2015, 12, 5–13. [Google Scholar]
- Reardon, C.; Tobin, D.P.; Tierney, P.; Delahunt, E. The worst case scenario: Locomotor and collision demands of the longest periods of gameplay in professional rugby union. PLoS ONE 2017, 12, e0177072. [Google Scholar] [CrossRef]
- Pollard, B.T.; Turner, A.N.; Eager, R.; Cunningham, D.J.; Cook, C.J.; Hogben, P.; Kilduff, L.P. The ball in play demands of international rugby union. J. Sci. Med. Sport 2018, 21, 1090–1094. [Google Scholar] [CrossRef]
- Tierney, P.; Tobin, D.; Blake, C.; Delahunt, E. Attacking 22 entries in rugby union: Running demands and differences between successful and unsuccessful entries. Scand. J. Med. Sci. Sports 2017, 27, 1934–1941. [Google Scholar] [CrossRef] [PubMed]
- Schwellnus, M.P.; Thomson, A.; Derman, W.; Jordaan, E.; Readhead, C.; Collins, R.; Morris, I.; Strauss, O.; Van der Linde, E.; Williams, A. More than 50% of players sustained a time-loss injury (>1 day of lost training or playing time) during the 2012 Super Rugby Union Tournament: A prospective cohort study of 17,340 player-hours. Br. J. Sports Med. 2014, 48, 1306–1315. [Google Scholar] [CrossRef]
- King, D.; Hume, P.; Gianotti, S.; Clark, T. A retrospective review over 1999 to 2007 of head, shoulder and knee soft tissue and fracture dislocation injuries and associated costs for rugby league in New Zealand. Int. J. Sports Exerc. Med. 2011, 32, 287–291. [Google Scholar] [CrossRef]
- Crichton, J.; Jones, D.R.; Funk, L. Mechanisms of traumatic shoulder injury in elite rugby players. Br. J. Sports Med. 2012, 46, 538–542. [Google Scholar] [CrossRef] [PubMed]
- Quarrie, K.L.; Hopkins, W.G.; Anthony, M.J.; Gill, N.D. Positional demands of international rugby union: Evaluation of player actions and movements. J. Sci. Med. Sport 2013, 16, 353–359. [Google Scholar] [CrossRef]
- Deutsch, M.; Kearney, G.; Rehrer, N. Time–motion analysis of professional rugby union players during match-play. J. Sports Sci. 2007, 25, 461–472. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.P.; Trewartha, G.; Higgitt, R.J.; El-Abd, J.; Stokes, K.A. The physical demands of elite English rugby union. J. Sports Sci. 2008, 26, 825–833. [Google Scholar] [CrossRef]
- Horsley, I.G.; Fowler, E.M.; Rolf, C.G. Shoulder injuries in professional rugby: A retrospective analysis. J. Orthop. Surg. Res. 2013, 8, 9. [Google Scholar] [CrossRef]
- Usman, J.; McIntosh, A.S. Upper limb injury in rugby union football: Results of a cohort study. Br. J. Sports Med. 2013, 47, 374–379. [Google Scholar] [CrossRef] [PubMed]
- Palmer-Green, D.S.; Stokes, K.A.; Fuller, C.W.; England, M.; Kemp, S.P.; Trewartha, G. Match injuries in English youth academy and schools rugby union: An epidemiological study. Am. J. Sports Med. 2013, 41, 749–755. [Google Scholar] [CrossRef]
- Roberts, S.P.; Trewartha, G.; England, M.; Shaddick, G.; Stokes, K.A. Epidemiology of time-loss injuries in English community-level rugby union. BMJ Open Sport Exerc. Med. 2013, 3, e003998. [Google Scholar] [CrossRef]
- Sundaram, A.; Bokor, D.J.; Davidson, A.S. Rugby Union on-field position and its relationship to shoulder injury leading to anterior reconstruction for instability. J. Sci. Med. Sport. 2011, 14, 111–114. [Google Scholar] [CrossRef]
- Brooks, J.H.; Fuller, C.; Kemp, S.; Reddin, D.B. Epidemiology of injuries in English professional rugby union: Part 1 match injuries. Br. J. Sports Med. 2005, 39, 757–766. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.; Trewartha, G.; Kemp, S.; Stokes, K. A meta-analysis of injuries in senior men’s professional Rugby Union. Sports Med. 2013, 43, 1043–1055. [Google Scholar] [CrossRef] [PubMed]
- Lynch, E.; Lombard, A.J.; Coopoo, Y.; Shaw, I.; Shaw, B.S. Shoulder injury incidence and severity through identification of risk factors in rugby union players. Pak. J. Med. Sci. 2013, 29, 1400. [Google Scholar] [CrossRef] [PubMed]
- Fuller, C.W.; Molloy, M.G.; Bagate, C.; Bahr, R.; Brooks, J.H.; Donson, H.; Kemp, S.P.T.; McCrory, P.; McIntosh, A.S.; Meeuwisse, W.H.; et al. Consensus statement on injury definitions and data collection procedures for studies of injuries in rugby union. Br. J. Sports Med. 2007, 41, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R.; Clarsen, B.; Derman, W.; Dvorak, J.; Emery, C.; Finch, C.; Hägglund, M.; Junge, A. International Olympic Committee consensus statement: Methods for recording and reporting of epidemiological data on injury and illness in sports. Br. J. Sports Med. 2020, 54, 372–389. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, S.; Till, K.; Weaving, D.; Jones, B. The use of microtechnology to quantify the peak match demands of the football codes: A systematic review. Sports Med. 2018, 48, 2549–2575. [Google Scholar] [CrossRef] [PubMed]
- Johnston, R.J.; Watsford, M.L.; Pine, M.J.; Spurrs, R.W.; Sporri, D. Assessment of 5 Hz and 10 Hz GPS units for measuring athlete movement demands. Int. J. Perform. Anal. Sport 2013, 13, 262–274. [Google Scholar] [CrossRef]
- Johnston, R.D.; Gabbett, T.J.; Jenkins, D.G.; Hulin, B.T. Influence of physical qualities on post-match fatigue in rugby league players. J. Sci. Med. Sport 2015, 18, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Orr, R.; Cheng, H.L. Incidence and characteristics of injuries in elite Australian junior rugby league players. J. Sci. Med. Sport 2016, 19, 212–217. [Google Scholar] [CrossRef]
- Hausler, J.; Halaki, M.; Orr, R. Application of global positioning system and microsensor technology in competitive rugby league match-play: A systematic review and meta-analysis. Sports Med. 2016, 46, 559–588. [Google Scholar] [CrossRef]
- Yeomans, C.; Kenny, I.C.; Cahalan, R.; Warrington, G.D.; Harrison, A.J.; Purtill, H.; Lyons, M.; Campbell, M.J.; Glynn, L.G.; Comyns, T.M. Injury trends in Irish amateur rugby: An epidemiological comparison of men and women. Sports Health 2021, 13, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Rae, K.; Orchard, J. The orchard sports injury classification system (OSICS) version 10. Clin. J. Sport Med. 2007, 17, 201–204. [Google Scholar] [CrossRef] [PubMed]
- Best, J.P.; McIntosh, A.S.; Savage, T.N. Rugby World Cup 2003 injury surveillance project. Br. J. Sports Med. 2005, 39, 812–817. [Google Scholar] [CrossRef]
- Fuller, C.; Laborde, F.; Leather, R.; Molloy, M.G. International rugby board rugby world cup 2007 injury surveillance study. Br. J. Sports Med. 2008, 42, 452–459. [Google Scholar] [CrossRef]
- Quarrie, K.L.; Hopkins, W.G. Tackle injuries in professional rugby union. Am. J. Sports Med. 2008, 36, 1705–1716. [Google Scholar] [CrossRef]
- Eaton, C.; George, K. Position specific rehabilitation for rugby union players. Part I: Empirical movement analysis data. Phys. Ther. Sport 2006, 7, 22–29. [Google Scholar] [CrossRef]
- Headey, J.; Brooks, J.H.; Kemp, S.P. The epidemiology of shoulder injuries in English professional rugby union. Am. J. Sports Med. 2007, 35, 1537–1543. [Google Scholar] [CrossRef] [PubMed]
- Bird, Y.; Waller, A.E.; Marshall, S.W.; Alsop, J.; Chalmers, D.; Gerrard, D. The New Zealand Rugby Injury and Performance Project: V. Epidemiology of a season of rugby injury. Br. J. Sports Med. 1998, 32, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Silva, P. A study on prevalence and risk factors associated with injuries of inter-university rugby players in Sri Lanka based on playing position. BMJ 2021, 55, A97–A98. [Google Scholar]
- Funk, L.; Snow, M. SLAP tears of the glenoid labrum in contact athletes. Clin. J. Sport Med. 2007, 17, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Bevan, T.; Chew, S.; Godsland, I.; Oliver, N.S.; Hill, N.E. A game for all shapes and sizes? Changes in anthropometric and performance measures of elite professional rugby union players 1999–2018. BMJ Open Sport Exerc. Med. 2022, 8, e001235. [Google Scholar] [CrossRef]
- Hendricks, S.; Karpul, D.; Lambert, M. Momentum and kinetic energy before the tackle in rugby union. J. Sports Sci. Med. 2014, 13, 557–563. [Google Scholar] [PubMed]
- Fuller, C.W.; Ashton, T.; Brooks, J.H.; Cancea, R.J.; Hall, J.; Kemp, S.P. Injury risks associated with tackling in rugby union. Br. J. Sports Med. 2010, 44, 159–167. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Injury Severity (Time-Loss in Days) | Momentum (kg·m/s) | Player Position $ | Tissue Type | Pathology Type | Diagnosis |
|---|---|---|---|---|---|
| Career Ender (n = 1) | 864.8 | Wing | Ligament/Joint capsule | AC Joint dislocation | AC Joint dislocation n = 1 (100%) |
| >28 days (n = 14) | 926.6 | Lock | Ligament/Joint capsule | AC Joint sprain | AC Joint sprain n = 4 (29%) Shoulder dislocation n = 4 (29%) AC Joint dislocation n = 2 (14%) Biceps muscle tear n = 1 (7%) Clavicle fracture n = 1 (7%) Pectoralis major tear n = 1 (7%) Shoulder muscle rupture/tear n = 1 (7%) |
| 878.5 | Lock | Ligament/Joint capsule | Shoulder dislocation | ||
| 862.4 | Loose-forward | Ligament/Joint capsule | AC Joint sprain | ||
| 802.5 | Loose-forward | Ligament/Joint capsule | AC Joint sprain | ||
| 799.0 | Wing | Ligament/Joint capsule | AC Joint dislocation | ||
| 791.7 | Lock | Muscle/Tendon | Shoulder muscle rupture/tear | ||
| 777.8 | Loose-forward | Bone | Clavicle fracture | ||
| 746.5 | Lock | Muscle/Tendon | Pectoralis major tear | ||
| 742.0 | Loose Forward | Muscle/Tendon | Biceps muscle tear | ||
| 676.3 | Wing | Ligament/Joint capsule | Shoulder dislocation | ||
| 628.7 | Scrumhalf | Ligament/Joint capsule | Shoulder dislocation | ||
| 623.0 | Fullback | Ligament/Joint capsule | Shoulder dislocation | ||
| 611.5 | Wing | Ligament/Joint capsule | AC Joint dislocation | ||
| 448.4 | Flyhalf | Ligament/Joint capsule | AC Joint sprain | ||
| 8–28 days (n = 19) | 1003.5 | Lock | Ligament/Joint capsule | AC Joint sprain | AC Joint sprain n = 11 (58%) Contusion n = 2 (11%) Shoulder muscle rupture/tear n = 2 (11%) AC Joint dislocation n = 1 (5%) Muscle strain n = 1 (5%) SC Joint dislocation n = 1 (5%) SC Joint sprain n = 1 (5%) |
| 843.2 | Prop | Ligament/Joint capsule | AC Joint sprain | ||
| 806.8 | Loose-forward | Ligament/Joint capsule | AC Joint sprain | ||
| 783.2 | Lock | Ligament/Joint capsule | AC Joint sprain | ||
| 767.6 | Lock | Ligament/Joint capsule | AC Joint sprain | ||
| 767.4 | Lock | Ligament/Joint capsule | AC Joint sprain | ||
| 763.9 | Lock | Muscle/Tendon | Contusion | ||
| 757.4 | Centre | Ligament/Joint capsule | AC Joint dislocation | ||
| 742.0 | Loose-forward | Ligament/Joint capsule | SC Joint dislocation | ||
| 741.7 | Fullback | Muscle/Tendon | Shoulder muscle rupture/tear | ||
| 712.5 | Prop | Muscle/Tendon | Muscle strain | ||
| 709.2 | Lock | Ligament/Joint capsule | AC Joint sprain | ||
| 708.3 | Lock | Ligament/Joint capsule | AC Joint sprain | ||
| 702.0 | Loose-forward | Ligament/Joint capsule | AC Joint sprain | ||
| 672.1 | Centre | Muscle/Tendon | Shoulder muscle rupture/tear | ||
| 672.0 | Centre | Ligament/Joint capsule | SC Joint sprain | ||
| 598.9 | Lock | Muscle/Tendon | Contusion | ||
| 558.9 | Centre | Ligament/Joint capsule | AC Joint sprain | ||
| 449.4 | Prop | Ligament/Joint capsule | AC Joint sprain | ||
| 1–7 days (n = 9) | 884.0 | Centre | Muscle/Tendon | Contusion | Contusion n = 2 (22%) Neuropraxia n = 2 (22%) SC Joint sprain n = 2 (22%) AC Joint sprain n = 1 (11%) Impingement n = 1 (11%) Muscle strain n = 1 (11%) |
| 843.8 | Lock | Ligament/Joint capsule | SC Joint sprain | ||
| 828.6 | Centre | Nerve | Neuropraxia | ||
| 828.0 | Prop | Ligament/Joint capsule | AC Joint sprain | ||
| 709.2 | Prop | Ligament/Joint capsule | SC Joint sprain | ||
| 709.2 | Prop | Muscle/Tendon | Muscle strain | ||
| 666.4 | Centre | Muscle/Tendon | Contusion | ||
| 665.0 | Centre | Nerve | Impingement | ||
| 623.7 | Hooker | Nerve | Neuropraxia |
| Injury Severity (Time-Loss in Days) | Match Intensity (m/min) | Collisions (Amount/min) | Player Position $ | Tissue Type | Pathology Type | Diagnosis |
|---|---|---|---|---|---|---|
| Career Ender (n = 1) | 51.3 | 0.13 | Wing | Ligament/Joint capsule | AC Joint dislocation | AC Joint dislocation n = 1 (100%) |
| >28 days (n = 14) | 80.9 | 0.03 | Wing | Ligament/Joint capsule | AC Joint dislocation | AC Joint sprain n = 4 (29%) Shoulder dislocation n = 4 (29%) AC Joint dislocation n = 2 (14%) Biceps muscle tear n = 1 (7%) Clavicle fracture n = 1 (7%) Pectoralis major tear n = 1 (7%) Shoulder muscle rupture/tear n = 1 (7%) |
| 86.1 | 0.2 | Flyhalf | Ligament/Joint capsule | AC Joint Sprain | ||
| 73.5 | 0.09 | Scrumhalf | Ligament/Joint capsule | Shoulder dislocation | ||
| 73.5 | 0.4 | Fullback | Ligament/Joint capsule | Shoulder dislocation | ||
| 66.7 | 0.44 | Wing | Ligament/Joint capsule | Shoulder dislocation | ||
| 68.5 | 0.2 | Lock | Muscle/Tendon | Pectoralis major tear | ||
| 72 | 0.25 | Loose-forward | Muscle/Tendon | Biceps muscle tear | ||
| 63.1 | 0.5 | Lock | Ligament/Joint capsule | Shoulder dislocation | ||
| 59.4 | 0.14 | Loose-forward | Bone | Clavicle Fracture | ||
| 62 | 0.35 | Loose-forward | Ligament/Joint capsule | AC Joint Sprain | ||
| 59.2 | 0.3 | Lock | Ligament/Joint capsule | AC Joint Sprain | ||
| 55.6 | 0.2 | Loose-forward | Ligament/Joint capsule | AC Joint Sprain | ||
| 51 | 0.16 | Lock | Muscle/Tendon | Shoulder muscle rupture/tear | ||
| 39 | 0.14 | Wing | Ligament/Joint capsule | AC Joint dislocation | ||
| 8–28 days (n = 19) | 79.8 | 0.12 | Prop | Ligament/Joint capsule | AC Joint Sprain | AC Joint sprain n = 11 (58%) Contusion n = 2 (11%) Shoulder muscle rupture/tear n = 2 (11%) AC Joint dislocation n = 1 (5%) Muscle strain n = 1 (5%) SC Joint dislocation n = 1 (5%) SC Joint sprain n = 1 (5%) |
| 72.3 | 0.48 | Centre | Muscle/Tendon | Shoulder muscle rupture/tear | ||
| 72 | 0.25 | Loose-forward | Ligament/Joint capsule | SC Joint Dislocation | ||
| 67.8 | 0.24 | Lock | Ligament/Joint capsule | AC Joint Sprain | ||
| 67.4 | 0.35 | Centre | Ligament/Joint capsule | AC Joint dislocation | ||
| 66.8 | 0.15 | Centre | Ligament/Joint capsule | AC Joint Sprain | ||
| 63.2 | 0.17 | Loose-forward | Ligament/Joint capsule | AC Joint Sprain | ||
| 62.8 | 0.25 | Fullback | Muscle/Tendon | Shoulder muscle rupture/tear | ||
| 62.2 | 0.51 | Lock | Ligament/Joint capsule | AC Joint Sprain | ||
| 59.8 | 0.48 | Lock | Ligament/Joint capsule | AC Joint Sprain | ||
| 59.3 | 0.11 | Centre | Ligament/Joint capsule | SC Joint Sprain | ||
| 58.4 | 0.35 | Loose-forward | Ligament/Joint capsule | AC Joint Sprain | ||
| 57.4 | 0.1 | Prop | Muscle/Tendon | Muscle strain | ||
| 56.9 | 0.33 | Lock | Ligament/Joint capsule | AC Joint Sprain | ||
| 52.1 | 0.11 | Lock | Muscle/Tendon | Contusion | ||
| 45.5 | 0.17 | Lock | Muscle/Tendon | Contusion | ||
| 27.7 | 0.2 | Lock | Ligament/Joint capsule | AC Joint Sprain | ||
| 14.3 | 0 | Prop | Ligament/Joint capsule | AC Joint Sprain | ||
| 101.2 | 0.13 | Lock | Ligament/Joint capsule | AC Joint Sprain | ||
| 1–7 days (n = 9) | 85.5 | 0.22 | Centre | Nerve | Neuropraxia | Contusion n = 2 (22%) Neuropraxia n = 2 (22%) SC Joint sprain n = 2 (22%) AC Joint sprain n = 1 (11%) Impingement n = 1 (11%) Muscle strain n = 1 (11%) |
| 84.6 | 0.45 | Centre | Muscle/Tendon | Contusion | ||
| 74.3 | 0.18 | Centre | Muscle/Tendon | Contusion | ||
| 68.9 | 0.17 | Prop | Muscle/Tendon | Muscle strain | ||
| 64.6 | 0.21 | Lock | Ligament/Joint capsule | SC Joint Sprain | ||
| 62.5 | 0.16 | Hooker | Nerve | Neuropraxia | ||
| 51.3 | 0.14 | Prop | Ligament/Joint capsule | AC Joint Sprain | ||
| 48.6 | 0.14 | Prop | Ligament/Joint capsule | SC Joint Sprain | ||
| 40.1 | 0.8 | Centre | Nerve | Impingement |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Louwrens, J.G.; Jansen van Rensburg, A.; Viljoen, C.T.; Hendricks, S.; Botha, T.; Janse van Rensburg, D.C. Epidemiology and Time-Loss Shoulder Injuries in Professional South African Rugby Players: A Prospective Study That Focuses on Real-Time Collision Data during a Tackle. Appl. Sci. 2023, 13, 10944. https://doi.org/10.3390/app131910944
Louwrens JG, Jansen van Rensburg A, Viljoen CT, Hendricks S, Botha T, Janse van Rensburg DC. Epidemiology and Time-Loss Shoulder Injuries in Professional South African Rugby Players: A Prospective Study That Focuses on Real-Time Collision Data during a Tackle. Applied Sciences. 2023; 13(19):10944. https://doi.org/10.3390/app131910944
Chicago/Turabian StyleLouwrens, Jan Gerhardus, Audrey Jansen van Rensburg, Carel T. Viljoen, Sharief Hendricks, Tanita Botha, and Dina C. (Christa) Janse van Rensburg. 2023. "Epidemiology and Time-Loss Shoulder Injuries in Professional South African Rugby Players: A Prospective Study That Focuses on Real-Time Collision Data during a Tackle" Applied Sciences 13, no. 19: 10944. https://doi.org/10.3390/app131910944
APA StyleLouwrens, J. G., Jansen van Rensburg, A., Viljoen, C. T., Hendricks, S., Botha, T., & Janse van Rensburg, D. C. (2023). Epidemiology and Time-Loss Shoulder Injuries in Professional South African Rugby Players: A Prospective Study That Focuses on Real-Time Collision Data during a Tackle. Applied Sciences, 13(19), 10944. https://doi.org/10.3390/app131910944