
The Effects of Structural Characteristics of the Rollator on the Elderly’s Gait Strategies in Various Walking Environments


Abstract
:1. Introduction
2. Methodology
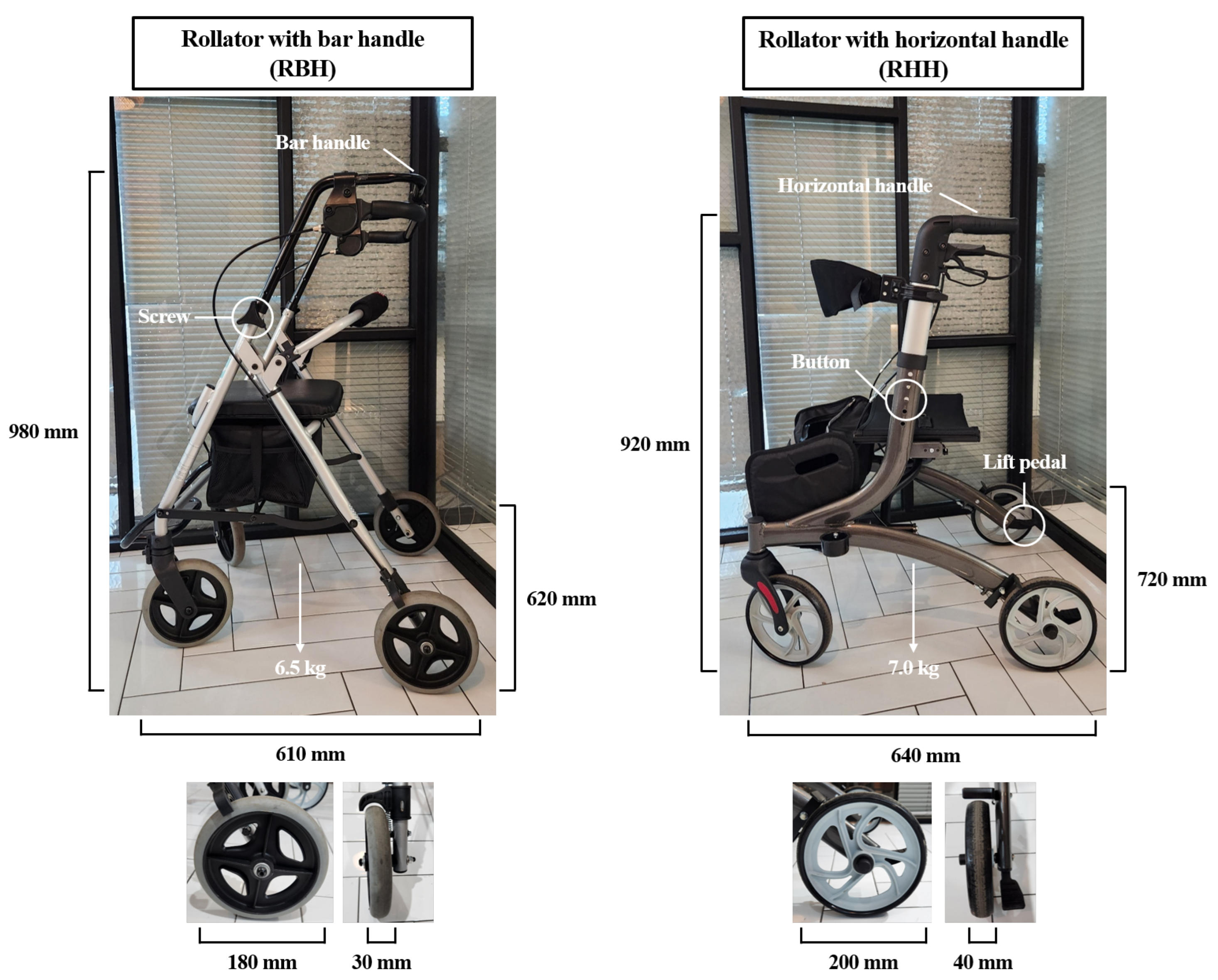
2.1. Structural Characteristics of Rollator
2.2. Subjects
2.3. Experimental Procedure
2.4. Experimental Setup
2.5. Data Analysis
2.6. Statistical Analysis
3. Results
3.1. Muscle Activity
3.2. Plantar Pressure Distribution
3.2.1. Mean Force
3.2.2. Peak Pressure
3.2.3. Contact Area
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coraci, D.; Tognolo, L.; Masiero, S. Rehabilitation of fall in elderly: The paradigm of a new medical vision. Appl. Sci. 2023, 13, 1898. [Google Scholar] [CrossRef]
- Hong, J.; Kong, H.J.; Yoon, H.J. Web-based telepresence exercise program for community-dwelling elderly women with a high risk of falling: Randomized controlled trial. JMIR mHealth uHealth 2018, 6, e9563. [Google Scholar] [CrossRef] [PubMed]
- Yoo, H.S.; Suh, E.K.; Kim, T.H. A study on technology acceptance of elderly living alone in smart city environment: Based on AI speaker. J. Ind. Distrib. Bus. 2020, 11, 41–48. [Google Scholar] [CrossRef]
- Afschrift, M.; De Groote, F.; Verschueren, S.; Jonkers, I. Increased sensory noise and not muscle weakness explains changes in non-stepping postural responses following stance perturbations in healthy elderly. Gait Posture 2018, 59, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Thies, S.B.; Bates, A.; Costamagna, E.; Kenney, L.; Granat, M.; Webb, J.; Howard, D.; Baker, R.; Dawes, H. Are older people putting themselves at risk when using their walking frames? BMC Geriatr. 2020, 20, 90. [Google Scholar] [CrossRef]
- Mundt, M.; Batista, J.P.; Markert, B.; Bollheimer, C.; Laurentius, T. Walking with rollator: A systematic review of gait parameters in older persons. Eur. Rev. Aging Phys. Act. 2019, 16, 15. [Google Scholar] [CrossRef]
- So, A.; Reeves, J.M.; Pearce, J.M. Open-source designs for distributed manufacturing of low-cost customized walkers. Inventions 2023, 8, 79. [Google Scholar] [CrossRef]
- Li, K.X.; Farrah, K. Walkers with Wheels versus Walkers without Wheels for Fall Prevention in Older Adults: A Review of the Comparative Clinical Effectiveness; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2019. [Google Scholar]
- Liu, H.; Thomas, P.; Salem, Y.; Miller, K.; McGee, M. Comparison of gait between walking up and down an incline with a walking device in older adults. Geriatr. Nurs. 2023, 53, 141–145. [Google Scholar] [CrossRef]
- Ippersiel, P.; Robbins, S.M.; Dixon, P.C. Lower-limb coordination and variability during gait: The effects of age and walking surface. Gait Posture 2021, 85, 251–257. [Google Scholar] [CrossRef]
- Kwee-Meier, S.T.; Mertens, A.; Jeschke, S. Age-induced changes in the lower limb muscle activities during uphill walking at steep grades. Gait Posture 2018, 62, 490–496. [Google Scholar] [CrossRef]
- Kim, T.W.; Kim, D.H.; Min, S.K.; Cho, E.H.; Lee, J.S. A comparative study on biomechanical variables of elderly women and elderly women at risk of fall in gait by environmental conditions. Korean J. Appl. Biomech. 2021, 31, 189–198. [Google Scholar]
- Arogunjo, E.O.; Markus, E.D.; Yskandar, H. Development of a holonomic robotic wheeled walker for persons with gait disorder. In Proceedings of the 2019 Open Innovations (OI), Cape Town, South Africa, 2–4 October 2019. [Google Scholar]
- Matthies, D.J.C.; Haescher, M.; Nanayakkara, S.; Bieber, G. Step detection for rollator users with smartwatches. In Proceedings of the 2018 ACM Symposium on Spatial User Interaction, Berlin, Germany, 13–14 October 2018. [Google Scholar]
- Bieber, G.; Chodan, W.; Bader, R.; Holle, B.; Herrmann, P.; Dreher, I. RoRo: A new robotic rollator concept to assist the elderly and caregivers. In Proceedings of the 12th ACM International Conference on Pervasive Tehcnologies Related to Assistive Environments, Rhodes, Greece, 5–7 June 2019. [Google Scholar]
- Zhao, X.; Zhu, Z.; Liu, M.; Zhao, C.; Zhao, Y.; Pan, J.; Wang, Z.; Wu, C. A smart robotic walker with intelligent close-proximity interaction capabilites for elderly mobility safety. Front. Neurorobot. 2020, 14, 575889. [Google Scholar] [CrossRef] [PubMed]
- Goncalves, C.; Lopes, J.M.; Moccia, S.; Berardini, D.; Migliorelli, L.; Santos, C.P. Deep learning-based approaches for human motion decoding in smart walkers for rehabilitation. Expert Syst. Appl. 2023, 228, 120288. [Google Scholar] [CrossRef]
- Sierra, M.S.D.; Munera, M.; Provot, T.; Bourgain, M.; Cifuentes, C.A. Evaluation of physical interaction during walker-assisted gait with the AGoRA Walker: Strategies based on virtual mechanical stiffness. Sensors 2021, 21, 3242. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Kim, S.C.; Lee, Y.I. Effect of a modified grip angle of a walker on the wrist deviation angle, muscle activation and palmar load during walker-assisted gait in elderly people. J. Phys. Ther. Sci. 2017, 29, 405–458. [Google Scholar] [CrossRef]
- Shokouhyan, S.M.; Blandeau, M.; Wallard, L.; Guerra, T.M.; Pudlo, P.; Gagnon, D.H.; Barbier, F. Sensorimotor time delay estimation by EMG signal processing in people living with spinal cord injury. Sensors 2023, 23, 1132. [Google Scholar] [CrossRef]
- Dickerson, L.C.; Queen, R.M. Foot posture and plantar loading with ankle bracing. J. Athl. Train. 2021, 56, 461–472. [Google Scholar] [CrossRef]
- Camus, E.J.; Moungondo, F.; Van Overstraeten, L. Biomechanics of wrist and elbow. In Human Orthorpaedic Biomechanics; Academic Press: Cambridge, MA, USA, 2022; pp. 325–338. [Google Scholar]
- Lee, Y.S.; Jin, H.; Arai, H.; Lim, J.Y. Handgrip strength: Should repeated measurements be performed in both hands? Geriatr. Gerontol. Int. 2021, 21, 426–432. [Google Scholar] [CrossRef]
- Kim, T.H.; Jung, S.R.; Kang, S.S.; Chang, S.R. Effects of combinational posture of shoulder, elbow and wrist on grip strength and muscle activity. J. Korean Soc. Saf. 2016, 31, 111–119. [Google Scholar] [CrossRef]
- Frigo, C.A.; Wyss, C.; Brunner, R. The effects of the rectus femoris muscle on knee and foot kinematics during the swing phase of normal walking. Appl. Sci. 2020, 10, 7881. [Google Scholar] [CrossRef]
- Kimata, K.; Otsuka, S.; Yokota, H.; Shan, X.; Hatayama, N.; Naito, M. Relationship between attachment site of tibialis anterior muscle and shape of tibia: Anatomical study of cadavers. J. Foot Ankle Res. 2022, 15, 54. [Google Scholar] [CrossRef]
- Gefner, S.C.; Hoevel, V.; Punt, I.M.; Schmid, S.; Armand, S.; Allet, L. Hip-abductor fatigue influences sagittal plane ankle kinematics and shank muscle activity during a single-leg forward jump. J. Electromyogr. Kinesiol. 2018, 43, 75–81. [Google Scholar] [CrossRef]
- Suica, Z.; Romkes, J.; Tal, A.; Maguire, C. Walking with a four wheeled walker (rollator) significantly reduces EMG lower-limb muscle activity in healthy subjects. J. Bodyw. Mov. Ther. 2016, 20, 65–73. [Google Scholar] [CrossRef]
- Alexander, N.; Schwameder, H. Effect of sloped walking on lower limb muscle forces. Gait Posture 2016, 47, 62–67. [Google Scholar] [CrossRef]
- Woo, B.H.; Park, Y.S. The effects of lower limb muscle activity on postural stability and ground type during gait in elderly women. Korean J. Sport Biomech. 2015, 25, 77–84. [Google Scholar] [CrossRef]
- Kim, J.; Lee, H.J.; Lee, S.H.; Lee, J.; Chang, W.H.; Ryu, G.H.; Kim, Y.H. Correlation between cardiopulmonary metabolic energy cost and lower-limb muscle activity during inclined treadmill gait in older adults. BMC Geriatr. 2021, 21, 469. [Google Scholar] [CrossRef] [PubMed]
- Adouni, M.; Shirazi-Adl, A.; Marouane, H. Role of gastrocnemius activation in knee joint biomechanics: Gastrocnemius acts as an ACL antagonist. Comput. Methods Biomech. Biomed. Eng. 2016, 19, 376–385. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Chang, W.H.; Hwang, S.H.; Choi, B.O.; Ryu, G.H.; Kim, Y.H. Age-related locomotion characteristics in association with balance function in young, middle-aged, and older adults. J. Aging Phys. Act. 2017, 25, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.; AI-Juaid, R.; AI-Amri, M. Gait stability characteristics in able-bodied individuals during self-paced inclined treadmill walking: Within-subject repeated-measure study. JMIR Form. Res. 2023, 7, e42769. [Google Scholar] [CrossRef] [PubMed]
- Alexander, N.; Schwameder, H. Comparison of estimated and measured muscle activity during inclined walking. J. Appl. Biomech. 2016, 32, 150–159. [Google Scholar] [CrossRef]
- Kling, R.; Chung, A.; Cox, C.; Kimbro, E.; Grodzielanek, J.; Ayres, S.; Soangra, R. Surface inclination influences fall risk and lower extremity joint moments during walking. In Proceedings of the Human Factors and Ergonomics Society Annual Meeting, Seattle, WA, USA, 5–9 October 2020; SAGE Publications: Los Angles, CA, USA, 2020. [Google Scholar]
- Kondo, M.; Iwamoto, Y.; Kito, N. Relationship between forward propulsion and foot motion during gait in healthy young adults. J. Biomech. 2021, 121, 110431. [Google Scholar] [CrossRef] [PubMed]
- Osoba, M.Y.; Rao, A.K.; Agrawal, S.K.; Lalwani, A.K. Balance and gait in the elderly: A contemporary review. Laryngoscope Investig. Otolaryngol. 2019, 4, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Jerome, G.J.; Ko, S.U.; Kauffman, D.; Studenski, S.A.; Ferrucci, L.; Simonsick, E.M. Gait characteristics associated with walking speed decline in older adults: Results from the baltimore longitudinal study of aging. Arch. Gerontol. Geriatr. 2015, 60, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Gimunova, M.; Zvonar, M.; Mikeska, O. The effect of aging and gender on plantar pressure distribution during the gait in elderly. Acta Bioeng. Biomech. 2018, 20, 139–144. [Google Scholar] [PubMed]
- Han, J.T.; Hwangbo, G. Analysis of plantar foot pressure and pathway of COP depending on inclination of descending ramp. J. Korea Contents Assoc. 2010, 10, 257–265. [Google Scholar] [CrossRef]
- Landorf, K.B.; Ackland, C.A.; Bonanno, D.R.; Menz, H.B.; Forghany, S. Effects of metatarsal domes on plantar pressure in older people with a history of forefoot pain. J. Foot Ankle Res. 2020, 13, 18. [Google Scholar] [CrossRef]
- Lee, K.D.; Kim, D.W.; Yoo, J.H.; Kim, K.H.; Lee, T.Y.; Park, K.S.; Chung, G.S.; Park, S.B. Comparative analysis on gait patterns of the elderly and the young regarding to foot pressure. Korea J. Appl. Biomech. 2011, 21, 67–75. [Google Scholar]
- Alves, F.; Cruz, S.; Ribeiro, A.; Silva, A.B.; Martins, J.; Cunha, I. Walkability index for elderly health: A proposal. Sustainability 2020, 12, 7360. [Google Scholar] [CrossRef]
- Vieira, M.F.; Rodrigues, F.B.; de Sa E Souza, G.S.; Magnani, R.M.; Lehnen, G.C.; Campos, N.G.; Andrade, A.O. Gait stability, variability and complexity on inclined surfaces. J. Biomech. 2017, 54, 73–79. [Google Scholar] [CrossRef]
- Strutzenberger, G.; Leutgeb, L.; Clauben, L.; Schwameder, H. Gait on slopes: Differences in temporo-spatial, kinematic and kinetic gait parameters between walking on a ramp and on a treadmill. Gait Posture 2022, 91, 73–78. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| FT | OT | UT | US | DS | ||
|---|---|---|---|---|---|---|
| FCU (%) | RBH | 8.409 ± 2.740 | 29.071 ± 5.621 | 26.895 ± 4.717 | 16.121 ± 2.769 | 12.420 ± 3.306 |
| RHH | 8.799 ± 2.972 | 13.683 ± 3.264 * | 21.170 ± 5.269 * | 19.116 ± 5.968 | 15.091 ± 3.633 * | |
| ECRL (%) | RBH | 17.623 ± 2.807 | 23.183 ± 2.933 | 34.829 ± 7.675 | 21.695 ± 3.958 | 23.896 ± 5.974 |
| RHH | 14.953 ± 3.509 | 17.561 ± 4.033 * | 24.497 ± 4.853 * | 12.406 ± 2.821 * | 14.660 ± 2.752 * | |
| RF (%) | RBH | 28.967 ± 4.206 | 26.415 ± 5.326 | 31.130 ± 5.052 | 29.491 ± 4.814 | 29.857 ± 5.155 |
| RHH | 26.952 ± 4.609 | 24.884 ± 3.810 | 28.467 ± 4.598 * | 29.428 ± 4.697 | 27.829 ± 4.869 | |
| TA (%) | RBH | 30.443 ± 4.751 | 28.850 ± 4.110 | 31.029 ± 4.608 e | 30.140 ± 3.213 | 25.517 ± 4.875 |
| RHH | 30.192 ± 5.781 | 33.297 ± 3.940 * | 26.305 ± 3.534 * | 31.241 ± 4.758 | 28.139 ± 4.304 | |
| BF (%) | RBH | 28.617 ± 4.294 | 34.536 ± 6.540 | 36.481 ± 6.319 | 32.305 ± 6.728 | 31.757 ± 5.475 |
| RHH | 28.652 ± 5.050 | 30.987 ± 4.391 * | 33.187 ± 5.468 * | 34.165 ± 7.822 | 32.298 ± 5.478 | |
| GM (%) | RBH | 35.648 ± 2.815 | 32.132 ± 3.209 | 33.725 ± 5.644 | 40.592 ± 4.022 | 37.728 ± 5.690 |
| RHH | 37.910 ± 3.300 | 31.647 ± 3.710 | 32.277 ± 4.495 | 38.458 ± 3.788 | 37.122 ± 6.184 |
| FT | OT | UT | US | DS | |||
|---|---|---|---|---|---|---|---|
| Mean force (N/kg) | H | RBH | 0.715 ± 0.124 | 0.584 ± 0.114 | 0.498 ± 0.107 | 0.510 ± 0.103 | 0.905 ± 0.175 |
| RHH | 0.688 ± 0.128 | 0.600 ± 0.104 | 0.500 ± 0.114 | 0.510 ± 0.090 | 0.935 ± 0.189 | ||
| LTs | RBH | 0.780 ± 0.149 | 0.604 ± 0.135 | 0.516 ± 0.119 | 0.580 ± 0.110 | 0.829 ± 0.145 | |
| RHH | 0.738 ± 0.144 * | 0.604 ± 0.135 | 0.560 ± 0.142 * | 0.639 ± 0.124 | 0.829 ± 0.164 | ||
| FF | RBH | 3.025 ± 0.239 | 2.381 ± 0.238 | 2.318 ± 0.246 | 2.548 ± 0.267 | 2.619 ± 0.216 | |
| RHH | 2.947 ± 0.228 | 2.359 ± 0.177 | 2.511 ± 0.296 * | 2.625 ± 0.221 | 2.554 ± 0.219 | ||
| MF | RBH | 0.888 ± 0.303 | 0.994 ± 0.324 | 1.045 ± 0.303 | 0.778 ± 0.244 | 0.798 ± 0.315 | |
| RHH | 0.864 ± 0.296 | 1.076 ± 0.281 * | 1.039 ± 0.304 | 0.775 ± 0.244 | 0.765 ± 0.296 | ||
| HF | RBH | 3.183 ± 0.283 | 3.321 ± 0.237 | 3.304 ± 0.274 | 2.873 ± 0.301 | 2.086 ± 0.252 | |
| RHH | 3.079 ± 0.330 | 3.153 ± 0.287 | 2.988 ± 0.290 * | 2.784 ± 0.306 | 2.075 ± 0.261 | ||
| Peak pressure (kPa) | H | RBH | 98.889 ± 19.800 | 84.809 ± 20.347 | 74.767 ± 18.358 | 74.372 ± 15.870 | 138.162 ± 39.642 |
| RHH | 93.716 ± 18.307 | 87.553 ± 21.044 | 77.584 ± 19.000 | 74.968 ± 14.636 | 138.332 ± 38.158 | ||
| LTs | RBH | 73.334 ± 13.278 | 59.605 ± 11.758 | 55.407 ± 11.804 | 60.574 ± 11.568 | 79.932 ± 13.933 | |
| RHH | 71.828 ± 13.331 | 61.329 ± 10.855 | 59.545 ± 12.985 * | 64.246 ± 12.589 | 81.002 ± 13.326 | ||
| FF | RBH | 116.477 ± 16.505 | 93.276 ± 13.376 | 90.891 ± 12.924 | 103.684 ± 14.076 | 104.421 ± 14.709 | |
| RHH | 112.484 ± 15.505 * | 93.290 ± 12.630 | 96.905 ± 15.147 * | 106.200 ± 15.461 | 99.986 ± 13.540 * | ||
| MF | RBH | 51.982 ± 6.452 | 56.435 ± 6.979 | 59.692 ± 7.095 | 48.382 ± 7.404 | 45.947 ± 7.630 | |
| RHH | 50.712 ± 7.013 | 65.035 ± 7.372 * | 59.436 ± 7.631 | 48.519 ± 7.783 | 44.811 ± 8.481 | ||
| HF | RBH | 95.530 ± 9.907 | 94.408 ± 9.458 | 98.938 ± 9.708 | 88.443 ± 10.935 | 71.456 ± 8.701 | |
| RHH | 94.138 ± 12.109 | 95.671 ± 11.330 | 91.313 ± 9.206 * | 86.362 ± 11.686 | 71.402 ± 10.676 | ||
| Contact Area (NICA) | H | RBH | 0.069 ± 0.007 | 0.063 ± 0.007 | 0.063 ± 0.008 | 0.060 ± 0.007 | 0.088 ± 0.008 |
| RHH | 0.070 ± 0.008 | 0.066 ± 0.006 | 0.060 ± 0.008 | 0.059 ±0.007 | 0.087 ± 0.009 | ||
| LTs | RBH | 0.101 ± 0.013 | 0.089 ± 0.013 | 0.088 ± 0.016 | 0.091 ± 0.012 | 0.126 ± 0.014 | |
| RHH | 0.100 ± 0.014 * | 0.093 ± 0.011 | 0.086 ± 0.014 | 0.098 ± 0.014 | 0.126 ± 0.017 | ||
| FF | RBH | 0.372 ± 0.021 | 0.328 ± 0.024 | 0.351 ± 0.022 | 0.357 ± 0.022 | 0.384 ± 0.020 | |
| RHH | 0.380 ± 0.022 * | 0.343 ± 0.020 | 0.358 ± 0.022 | 0.365 ± 0.021 | 0.381 ± 0.022 | ||
| MF | RBH | 0.144 ± 0.024 | 0.162 ± 0.030 | 0.169 ± 0.029 | 0.148 ± 0.027 | 0.142 ± 0.025 | |
| RHH | 0.144 ± 0.026 | 0.164 ± 0.026 | 0.166 ± 0.028 | 0.149 ± 0.026 | 0.142 ± 0.027 | ||
| HF | RBH | 0.314 ± 0.022 | 0.358 ± 0.018 | 0.358 ± 0.025 | 0.344 ± 0.031 | 0.260 ± 0.021 | |
| RHH | 0.305 ± 0.025 * | 0.334 ± 0.018 | 0.329 ± 0.020 * | 0.329 ± 0.023 | 0.263 ± 0.026 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, J.-Y.; Kim, J.-J. The Effects of Structural Characteristics of the Rollator on the Elderly’s Gait Strategies in Various Walking Environments. Appl. Sci. 2023, 13, 11044. https://doi.org/10.3390/app131911044
Jung J-Y, Kim J-J. The Effects of Structural Characteristics of the Rollator on the Elderly’s Gait Strategies in Various Walking Environments. Applied Sciences. 2023; 13(19):11044. https://doi.org/10.3390/app131911044
Chicago/Turabian StyleJung, Ji-Yong, and Jung-Ja Kim. 2023. "The Effects of Structural Characteristics of the Rollator on the Elderly’s Gait Strategies in Various Walking Environments" Applied Sciences 13, no. 19: 11044. https://doi.org/10.3390/app131911044
APA StyleJung, J.-Y., & Kim, J.-J. (2023). The Effects of Structural Characteristics of the Rollator on the Elderly’s Gait Strategies in Various Walking Environments. Applied Sciences, 13(19), 11044. https://doi.org/10.3390/app131911044