
Postural Reactions to External Mediolateral Perturbations: A Review



Abstract
1. Introduction
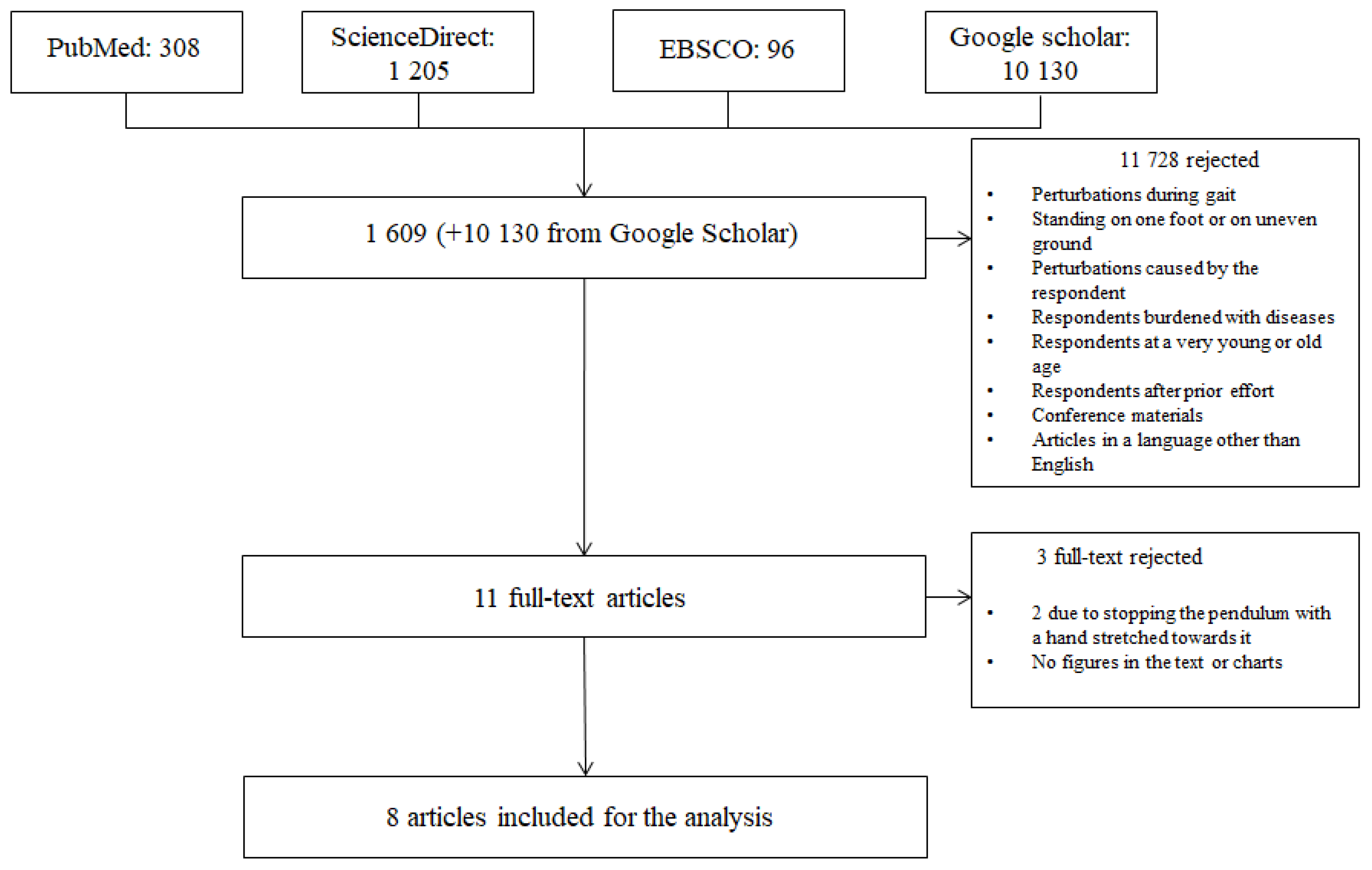
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility
2.3. Review Process
2.4. Quality Assessment
3. Results
3.1. Characteristics of Participants
3.2. Ways and Levels of Inducing Mediolateral Perturbations
3.3. Measured Outcomes
3.4. Description of the Sequence of Responses to Mediolateral Perturbations
4. Discussion
4.1. An Overview of the Research Methodology
4.2. Timeline of Response Sequences to Mediolateral Perturbations
4.3. Study Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Time [ms] | 80 | 87.1 | 85 | 90 | 95 | 97 | 110 |
| Event | Ipsi. angle change onset at pelvis push [15] Angle change onset in ankle joint opposite the perturbed side at pelvis push [15] | DF torque onset at max pert. | Torque onset in ankle joint opposite the perturbed side at pelvis push [15] | Angle change onset in AJ opposite the perturbed side at shoulder push [15] Ipsi. torque onset at pelvis push [15] | Ipsi. angle change onset at shoulder push [15] | Tibialis anterior EMG onset [19] | Ipsi. torque onset at shoulder push [15] Torque onset in ankle joint opposite the perturbed side at shoulder push [15] |
| Time [ms] | 135.5 | 160.5 | 163.6 | 172.3 | 175.6 | 190.1 | 191.2 |
| Event | DF torque onset at medial lateral pert. | PF angle change onset at minimal medial pert. | MMG onset and PF at maximal lateral pert. | MMG onset and PF at medium lateral pert. | MMG onset and DF at maximal lateral pert. | MMG onset and PF at medium lateral pert. | MMG onset and PF at maximal medial pert. |
| Time [ms] | 192.0 | 191.8 | 192.2 | 197.6 | 198.6 | 206.4 | 215.3 |
| Event | MMG onset and DF at maximal medial pert. | EMG onset and DF at maximal lateral pert. | EMG onset and DF at medium lateral pert. | MMG onset and DF at medium lateral pert. | Power absorbing onset at maximal lateral pert. | EMG onset and PF maximal lateral pert. | MMG onset and DF at medium medial pert. |
| Time [ms] | 230.6 | 232.5 | 241.8 | 250.1 | 250.9 | 272.9 | 279.6 |
| Event | MMG onset and PF at minimal lateral pert. | DF angle change onset at maximal medial pert. | EMG onset and DF at maximal medial pert. | DF torque onset at minimal lateral pert. | EMG onset and PF at medial lateral pert. | EMG onset and DF at medium medial pert. | EMG onset and DF at minimal lateral pert. |
| Time [ms] | 284.3 | 298.2 | 306.9 | 312.2 | 323.0 | 333.7 | 351.2 |
| Event | MMG onset and DF at minimal lateral pert. | MMG onset and PF at minimal medial pert. | DF torque onset at maximal medial pert. | MMG onset and DF at minimal medial pert. | Stepping foot lift of the plate [19] | Power generating onset at maximal medial pert. | EMG onset and PF at minimal lateral pert. |
| Time [ms] | 355.3 | 370.8 | 371.0 | 374.2 | 375.0 | 378.9 | 400.0 |
| Event | DF torque at medium medial pert. | PF torque onset at medium medial pert. | Power absorbing onset at maximal medial pert. | DF angle change onset at maximal lateral pert. | LSS step onset [4,5] | Power absorbing onset at minimal medial pert. | UCS step onset [4,5] |
| Time [ms] | 402.6 | 406.9 | 409.0 | 426.3 | 444.9 | 449.3 | 451.3 |
| Event | DF angle change onset at medium medial pert. | PF torque at maximal medial pert. | PF torque onset at minimal medial pert. | Power absorbing onset at minimal lateral pert. | DF angle change onset at minimal medial pert. | Power generating onset at medium medial pert. | EMG onset and DF at minimal medial pert. |
| Time [ms] | 455.3 | 458.4 | 461.0 | 502.1 | 504.6 | 505.0 | 519.1 |
| Event | Power generating onset at minimal lateral pert. | Peak of hip ext MG of DF at minimal lateral pert. | Stepping foot landing. Step length: 23.7 ± 11.9 cm; Heigth: 5.1 ± 2.0 cm; Step duration: 221 ± 175 ms [19]. | Power generating onset at medium medial pert. | DF angle change onset at medium medial pert. | Power absorbing onset at medium lateral pert. | DF torque onset at minimal medial pert. |
| Time [ms] | 525.0 | 529.5 | 531.9 | 532.0 | 542.7 | 555.1 | 565.8 |
| Event | PF angle change onset at maximal medial pert. | Peak MMG of PF at minimal lateral pert. | Peak of hip ext. MG of DF at medial lateral pert. | PF angle change onset at medium medial pert. | DF angle change onset at minimal lateral pert. | Power generating onset at maximal lateral pert. | PF torque onset at minimal lateral pert. |
| Time [ms] | 574.8 | 588.4 | 601.8 | 605.9 | 607 | 608.3 | 612.9 |
| Event | Peak of hip ext. MG of PF at medial lateral pert. | Peak MMG of DF at minimal laterel pert. | Peak of hip ext. MG of PF at minimal lateral pert. | Peak MMG of PF at medial lateral pert. | Shank peak angle (−5.8 ± 0.2 deg) at pelvis push. [15] | Peak of hip ext. MG of DF at medium medial pert. | Power generating onset at minimal medial pert. |
| Time [ms] | 627.0 | 641.3 | 662.4 | 667.9 | 676.8 | 679.0 | 679.9 |
| Event | Peak of hip ext. MG of DF at minimal medial pert. | PF angle change onset at minimal lateral pert. | Power absorbing onset at medium medial pert. | Peak power absorbing (0.16 ± 0.11 W/kg) at maximal lateral pert. | Peak PF angle (0.6 ± 0.4 deg) at minimal medial pert. | Peak MMG of DF at medial lateral pert. | Peak of hip ext. MG of DF at maximal lateral pert. |
| Time [ms] | 696.7 | 698.2 | 700.0 | 711.0 | 742.3 | 749.4 | 758.4 |
| Event | PF angle change onset at maximal lateral pert. | Peak MMG of DF at minimal medial pert. | LSS step termination. Step duration 325 ms; lateral displacement and step clarence normalised by height: 0.16 cm [4,5]. | Peak of hip ext. MG of PF at maximal lateral pert. | Peak MMG of PF at minimal medial pert. | Peak power absorbing (0.01 ± 0.01 W/kg) at minimal medial pert. | Peak MMG of DF at medium medial pert. |
| Time [ms] | 771.7 | 778.4 | 780.6 | 784.4 | 787.2 | 806.4 | 808.2 |
| Event | EMG onset of PF at medium medial pert. | Peak PF torque (0.12 ± 0.05 Nm/kg) at minimal medial pert. | Peak power generating (0.03 ± 0.02 W/kg) at medium lateral pert. | Peak power absorbing (0.02 ± 0.02 W/kg) at medium lateral pert. | Peak power absorbing (0.01 ± 0.01 W/kg) at minimal lateral pert. | PF angle change onset at medium lateral pert. | EMG onset at PF at maximal medial pert. |
| Time [ms] | 816.2 | 827.9 | 836.4 | 849.3 | 868.2 | 870.4 | 881 |
| Event | Peak PF torque (0.16 ± 0.06 Nm/kg) at medium medial pert. | Peak DF torque (0.41 ± 0.2 Nm/kg) at maximal lateral pert. | Peak DF torque at medium lateral pert. 0.22 ± 0.09 Nm/kg | EMG onset at PF at minimal medial pert. Peak MMG of PF at medium medial pert. | Peak DF angle (3.1 ± 1.6 deg) at medium medial pert. | PF torque onset at medium lateral pert. | Shank peak angle (−2.6 ± 0.2 deg) at shoulder push [15] |
| Time [ms] | 902.8 | 912.9 | 915.5 | 929.2 | 931.6 | 948.4 | 952.3 |
| Event | Peak power generating (0.01 ± 0.01 W/kg) at minimal lateral pert. | Peak power generating (0.02 ± 0.01 W/kg) at medium medial pert. | Peak DF angle (1.6 ± 1.0 deg) at minimal medial pert. | Peak of hip ext. MG of DF at maximal medial pert. | Peak power absorbing (0.02 ± 0.01 W/kg) at medium medial pert. | Peak DF angle (8.4 ± 5.5 deg) at maximal lateral pert. | Peak PF torque (0.06 ± 0.04 Nm/kg) at minimal lateral pert. |
| Time [ms] | 952.7 | 963.5 | 981.2 | 998.4 | 1002.3 | 1014.6 | 1025.0 |
| Event | Peak DF angle (4.2 ± 2.3 deg) at maximal medial pert. | Peak power generating (0.01 ± 0.01 W/kg) at minimal medial pert. | Peak MMG of PF at maximal lateral pert. | Peak PF angle (1.7 ± 1.0 deg) at medium medial pert. | Peak MMG of DF at maximal lateral pert. | Peak DF torque (0.13 ± 0.08 Nm/kg) at minimal lateral pert. | UCS step termination. Step duration 625 ms; lateral displacement and step clearance normalised by body heigth: 0.34 cm [4,5] |
| Time [ms] | 1033.1 | 1067.8 | 1076.7 | 1090.0 | 1116.4 | 1130.5 | 1139.8 |
| Event | PF torque onset at maximal lateral pert. | Peak MMG of PF at maximal medial pert. | Peak PF angle (98.2 ± 4.6 deg) at maximal medial pert. | Peak power generating (90.04 ± 0.03 W/kg) at maximal medial pert. | Peak PF torque 90.18 ± 0.09 Nm/kg) at maximal medial pert. | Peak MMG of DF at maximal medial pert. | Peak power generating (0.10 ± 0.08 W/kg) at maximal lateral pert. |
| Time [ms] | 1152.3 | 1174.4 | 1190.9 | 1203.9 | 1211.5 | 1244.9 | 1274.2 |
| Event | Peak PF angle (0.9 ± 0.3 deg) at minimal lateral pert. | Peak DF angle (2.9 ± 2.3 deg) at medium lateral pert. | Peak PF torque (0.06 ± 0.05 Nm/kg) at medium lateral pert. | Peak of hip ext. MG of PF at medium medial pert. | Peak DF angle (1.4 ± 0.7 deg) at minimal lateral pert. | Peak DF torque (0.13 ± 0.07 Nm/kg) at medium medial pert. | Peak of hip ext. MG of PF at minimal medial pert. |
| Time [ms] | 1294.0 | 1299.9 | 1302.1 | 1310.0 | 1318.4 | 1337.7 | 1396.1 |
| Event | Peak PF angle (1.1 ± 0.5 deg) at medium lateral pert. | Peak of hip ext. MG of PF at maximal medial pert. | Peak PF torque (0.14 ± 0.08 Nm/kg) at maximal lateral pert. | Peak DF torque (0.17 ± 0.10 Nm/kg) at maximal medial pert. | Peak DF torque (0.11 ± 0.09 Nm/kg) at minimal medial pert. | Peak power absorbing (0.06 ± 0.03 W/kg) at maximal medial pert. | Peak PF angle (1.3 ± 0.8 deg) at maximal lateral pert. |
| Time [ms] | 64.9 | 161.0 | 187.0 | 192.1 | 200.7 | 203.4 | 205.2 |
| Event | Knee ext. torque onset at medium medial pert. | Knee ext. torque onset at maximal medial pert. | Knee ext. MMG onset at maximal lateral pert. | Knee flex. MMG onset at maximal medial pert. | Power absorbing onset in knee at maximal lateral pert. | Knee flex. MMG onset at medial lateral pert. | Knee flex. MMG onset at maximal lateral pert. |
| Time [ms] | 213.1 | 215.7 | 224.5 | 225.0 | 225.2 | 226.7 | 244.9 |
| Event | Knee ext. torque onset at minimal medial pert. | Knee flex. torque onset at medial lateral pert. | Knee ext. MMG onset at medial lateral pert. | Knee flex. torque onset at maximal lateral pert. | Knee flex. MMG onset at medium medial pert. | MMG onset knee ext. at maximal medial pert. | Knee flex. torque onset at minimal lateral pert. |
| Time [ms] | 245.1 | 238.7 | 289.6 | 303.8 | 308.5 | 326.7 | 331.7 |
| Event | Knee ext. MMG onset at medium medial pert. | Angle change onset of knee flex. at maximal medial pert. | Knee flex. MMG onset at minimal lateral pert. | Knee ext. MMG onset at minimal lateral pert. | EMG onset of knee ext. at maximal lateral pert. | Knee ext. MMG onset at minimal medial pert. | Angle change onset of knee flex. at medium medial pert. |
| Time [ms] | 334.2 | 334.3 | 336.9 | 351.7 | 354.9 | 358.8 | 363.8 |
| Event | EMG onset of knee flex. at maximal medial pert. | Angle change onset of knee flex. MID L pert. | Power absorbing onset in knee at medial lateral pert. | Power absorbing onset at medium medial pert. | Knee flex. MMG onset at minimal medial pert. | Angle change onset of knee flex. at minimal medial pert. | Power absorbing onset at maximal medial pert. |
| Time [ms] | 366.1 | 378.9 | 388.3 | 395.7 | 405.9 | 411.0 | 429.8 |
| Event | Angle change onset of knee ext. at maximal medial pert. | Power absorbing onset in knee at minimal medial pert. | Power generating onset at maximal lateral pert. | Power absorbing onset at minimal lateral pert. | Power generating onset at maximal medial pert. | EMG onset of knee ext. at medial lateral pert. | EMG onset of knee flex. at medium medial pert. |
| Time [ms] | 464.3 | 470.1 | 482.6 | 487.3 | 494.8 | 495.0 | 505.3 |
| Event | Angle change onset of knee flex. at maximal laterel pert. | Angle change onset of knee flex. at mimimal lateral pert. | Angle change onset of knee ext. at maximal lateral pert. | EMG onset of knee ext. at maximal medial pert. | Knee ext. torque onset at medial lateral pert. | Angle change onset of knee ext. at minimal medial pert. | Power generating onset at medial lateral pert. |
| Time [ms] | 507.1 | 532.4 | 553.6 | 562.9 | 566.2 | 574.3 | 577.9 |
| Event | Angle change onset of knee ext. at minimal lateral pert. | EMG onset of knee flex. at maximal lateral pert. | Knee ext. torque onset at minimal lateralpert. | Knee ext. torque onset at maximal lateral pert. | Angle change onset of knee ext. at medium lateral pert. | Power generating onset at minimal lateralpert. | Peak of knee flex. torque (0.27 ± 0.15 Nm/kg) at medial lateral pert. |
| Time [ms] | 582.0 | 586.3 | 596.1 | 623.1 | 651.3 | 652.2 | 600.8 |
| Event | Peak of hip flex. torque (0.18 ± 0.10 Nm/kg) at minimal lateral pert. | Peak power absorbing (0.05 ± 0.03 W/kg) at medial lateral pert. | Knee ext. MMG onset at minimal lateral pert. | Peak MMG of knee flex. aminimal medial pert. | Peak MMG of knee flex. at minimal lateral pert. | Peak MMG of knee flex. at medial lateral pert. | EMG onset knee ext. at minimal lateral pert. |
| Time [ms] | 627.1 | 653.2 | 659.0 | 679.0 | 693.4 | 697.8 | 699.5 |
| Event | EMG onset knee flex. at minimal medial pert. Peak power absorbing (0.02 ± 0.01 W/kg) at minimal lateral pert. | Peak MMG of knee ext. at minimal medial pert. | Peak of EMG of knee ext. at medial lateral pert. | Power generating onset at medium medial pert. | Peak power absorbing (0.17 ± 0.20 W/kg) at maximal lateral pert. | Peak MMG of knee ext. at medial lateral pert. | Peak of knee flex. angle (1.2 ± 1.1 deg) at medial lateral pert. |
| Time [ms] | 724.7 | 730.4 | 736.7 | 738.9 | 739.9 | 756.4 | 762.9 |
| Event | Power generating onset at minimal medial pert. | EMG onset knee flex. at medial lateral pert. | EMG onset of knee ext. at medium medial pert. | Peak EMG of knee ext. at maximal lateral pert. | Peak EMG of knee ext. at medium medial pert. | Peak EMG of knee ext. at minimal lateral pert. | Peak MMG of knee flex. at medium medial pert. |
| Time [ms] | 769.6 | 770.4 | 772.0 | 783.3 | 808.9 | 811.9 | 812.6 |
| Event | Peak power absorbing (0.01 ± 0.01 W/kg) at minimal medial pert. | Peak of hip ext torque (0.14 ± 0.07 Nm/kg) at minimal medial pert. | Peak MMG of knee ext. at medium medial pert. | Peak of knee flex. angle (5.6 ± 3.0 deg) at medium medial pert. | Peak power absorbing (0.03 ± 0.01 W/kg) at medium medial pert. | Peak of hip ext. torque (0.21 ± 0.10 Nm/kg) at medium medial pert. | Peak power generating (0.02 ± 0.01 W/kg) at minimal lateral pert. |
| Time [ms] | 818.5 | 844.8 | 856.7 | 862.7 | 876.4 | 890.2 | 891.7 |
| Event | EMG onset of knee flex. at minimal lateral pert. | EMG onset of knee ext. at minimal medial pert. | Peak EMG of knee flex. at medium medial pert. | Peak of knee flex. angle (2.4 ± 1.6 deg) at minimal medial pert. | Peak power generating (0.04 ± 0.02 W/kg) at medial lateral pert. | Peak of knee flex. angle (0.7 ± 0.3 deg) at minimal lateral pert. | Peak MMG of knee ext. at maximal lateral pert. |
| Time [ms] | 902.3 | 912.9 | 919.1 | 950.8 | 953.8 | 960.2 | 969.1 |
| Event | Peak of hip flex. angle (15.1 ± 8.6 deg) at maximal medial pert. | Angle ext. change onset of at medium medial pert. | Peak power generating (0.20 ± 0.23 W/kg) at maximal lateral pert. | Peak EMG of knee flex. at medial lateral pert. | Peak of knee flex. torque (0.48 ± 0.24 Nm/kg) at maximal lateral pert. | Knee flex. torque onset at minimal medial pert. | Peak EMG of knee flex. at minimal medial pert. |
| Time [ms] | 972.8 | 976.7 | 982.9 | 992.9 | 1020.5 | 1011.4 | 1027.6 |
| Event | Peak of knee flex. angle (5.4 ± 4.6 deg) at maximal lateral pert. | Peak power generating (0.01 ± 0.01 W/kg) at minimal medial pert. | Peak MMG of knee flex. at maximal medial pert. | Peak power generating (0.09 ± 0.07 W/kg) at maximal medial pert. | Peak EMG of knee ext. at maximal medial pert. | Peak knee ext. angle (0.8 ± 0.9 deg) at minimal medial pert. | Peak MMG of knee flex. at maximal lateral pert. |
| Time [ms] | 1046.0 | 1065.2 | 1082.1 | 1069.6 | 1078.5 | 1109.4 | 1122.1 |
| Event | Peak knee ext. angle (2.4 ± 2.0 deg) at maximal lateral pert. | Peak MMG of knee ext. at maximal medial pert. | Peak of hip ext. torque (0.24 ± 0.11 Nm/kg) at maximal medial pert. | Peak power generating (0.02 ± 0.01 W/kg) at medium medial pert. | Peak EMG of knee flex. at minimal lateral pert. | Peak EMG of knee flex. at maximal medial pert. | Peak EMG of knee ext. at minimal medial pert. |
| Time [ms] | 1184.0 | 1192.4 | 1193.7 | 1230.3 | 1235.9 | 1266.2 | 1262.9 |
| Event | Peak of knee ext. angle (1.9 ± 1.5 deg) at maximal medial pert. | Peak of knee ext. angle (1.4 ± 1.4 deg) at minimal lateral pert. | Peak EMG of knee flex. at maximal lateral pert. | Peak of knee ext. angle (1.8 ± 0.8 deg) at medial lateral pert. | Flex. torque onset at medium medial pert. | Peak of hip ext. torque (0.09 ± 0.06 Nm/kg) at minimal lateral pert. | Peak power absorbing (0.07 ± 0.06 W/kg) at maximal medial pert. |
| Time [ms] | 1344.1 | 1348.7 | 1353.2 | 1463.8 | 1470.8 | 1538.5 | 1762.4 |
| Event | Peak knee flex. torque (0.08 ± 0.06 Nm/kg) at minimal medial pert. | Peak of hip ext. torque (0.13 ± 0.09 Nm/kg) at maximal lateral pert. | Peak of knee ext. angle (1.4 ± 1.0 deg) at medium medial pert. | Peak of knee ext. torque (0.13 ± 0.07 Nm/kg) at medial lateral pert. | Knee flex. torque onset at maximal medial pert. | Peak of knee flex. torque (0.10 ± 0.09 Nm/kg) at medium medial pert. | Peak of knee flex. torque (0.22 ± 0.14 Nm/kg) at maximal medial pert. |
| Time [ms] | 55 | 65 | 62.3 | 63.3 | 65.4 | 70 | 75 |
| Event | Ipsi. torque onset at pelvis push [15] | Ipsi. angle change onset at pelvis push [15] | MMG onset of hip ABD at maximal lateral pert. | Hip ABD torque onset at medium medial pert. | MMG onset of hip ABD at maximal medial pert. | Torque onset change in HJ opposite the perturbed side at shoulder and pelvis push [15] | Angle change onset in HJ opposite the perturbed side at shoulder and pelvis push [15] |
| Time [ms] | 78.2 | 80 | 83.4 | 86.7 | 86.9 | 87.3 | 89.4 |
| Event | MMG onset of hip ABD at medium medial pert. | Ipsi. angle change onset at shoulder push [15] | Hip ABD torque onset at maximal medial pert. | MMG of hip flex. onset at maximal medial pert. | Hip flex. torque onset at medium medial pert. | MMG of hip ABD onset at minimal lateral pert. | MMG of hip ABD onset at medial lateral pert. |
| Time [ms] | 93.6 | 103.7 | 110 | 115.6 | 117.4 | 123.4 | 124.4 |
| Event | MMG of hip flex. onset at maximal lateral pert. | MMG of hip ext. onset at medium medial pert. | Ipsi. torque onset at shoulder push [15] | MMG of hip flex. onset at medial lateral pert. | Hip ABD torque onset at minimal medial pert. | MMG of hip flex. onset at medium medial pert. | Angle of hip flex. change onset at maximal lateral pert. |
| Time [ms] | 130.6 | 131.3 | 135.7 | 143.9 | 148.9 | 151.2 | 154.2 |
| Event | MMG of hip ext. onset at maximal lateral pert. | Power generation torque at medium medial pert. | Power generation torque at minimal medial pert. | MMG onset of hip ABD at minimal medial pert. | MMG of hip ext. onset at minimal lateral pert. | Hip ADD torque onset at maximal lateral pert. | MMG of hip ext. onset at medial lateral pert. |
| Time [ms] | 159.1 | 161.2 | 163.4 | 169.1 | 173.1 | 179.4 | 176.9 |
| Event | MMG of hip ADD onset at medium medial pert. | Hip ADD torque onset at medial lateral pert. | EMG onset of hip ABD at maximal lateral pert. | MMG onset of hip ADD at maximal medial pert. | MMG of hip flex. onset at minimal lateral pert. | MMG of hip ADD onset at maximal lateral pert. | MMG of hip ext. onset at minimal medial pert. |
| Time [ms] | 177.9 | 180.6 | 181.2 | 183.6 | 183.7 | 193.0 | 193.4 |
| Event | Power generation torque at maximal medial pert. | EMG of hip ABD onset at medial lateral pert. | Hip flex. torque onset at maximal medial pert. | MMG of hip ext. onset at maximal medial pert. | Hip ext. torque onset at medial lateral pert. | Hip flex. angle change onset at medial lateral pert. | Hip flex. angle change onset at medium medial pert. |
| Time [ms] | 195.6 | 197.9 | 198.9 | 206.4 | 220.1 | 224.2 | 225.6 |
| Event | Hip ADD torque onset at minimal lateral pert. | MMG of hip ADD onset at medial lateral pert. | Hip flex. Torque onset at minimal medial pert. | Hip ext. torque onset at minimal lateral pert. | Hip ABD angle change onset at minimal medial pert. | EMG of hip ABD onset at minimal lateral pert. | EMG of hip flex. onset at maximal lateral pert. |
| Time [ms] | 226.6 | 234.2 | 233.17 | 233.57 | 235.61 | 246.2 | 256.7 |
| Event | MMG of hip flex. onset at minimal medial pert. | MMG of hip ADD onset at minimal lateral pert. | Pelvic up-down motion [24] | Pelvic ML motion [24] | Pelvic AP motion [24] | MMG of hip ADD onset at minimal medial pert. | EMG of hip ABD onset at maximal medial pert. |
| Time [ms] | 258.0 | 263.7 | 263.8 | 270.3 | 272.2 | 272.4 | 284.1 |
| Event | Power absorbing onset at minimal lateral pert. | Hip ADD angle change onset at minimal lateral pert. | Hip ABD angle change onset at medium medial pert. | Hip flex. angle chang onset at maximal medial pert. | EMG of hip flex. Onset at medial lateral pert. | Hip ABD angle change onset at maximal medial pert. | EMG of hip ext. onset at maximal lateral pert. |
| Time [ms] | 301.4 | 301.6 | 306.4 | 309.0 | 314.9 | 315.1 | 326.4 |
| Event | Hip flex. angle change onset at minimal medial pert. | EMG of hip ABD onset at medium medial pert. | Hip ext. torque onset at maximal lateral pert. | Power generation onset at maximal lateral pert. | EMG of hip ext. onset at medial lateral pert. | Power generation onset at medial lateral pert. | EMG of hip ADD onset at maximal medial pert. |
| Time [ms] | 332.6 | 342.5 | 347.7 | 363.0 | 370.9 | 388.9 | 389.3 |
| Event | EMG of hip ADD onset at minimal medial pert. | Power absorbing onset at medial lateral pert. | Hip ADD angle change onset at medial lateral pert. | Power absorbing onset at maximal lateral pert. | Hip ADD angle change onset at maximal lateral pert. | Peak power generating at minimal medial pert. | EMG of hip flex. onset at maximal medial pert. |
| Time [ms] | 415.4 | 418.6 | 430.8 | 444.0 | 473.4 | 479.6 | 480.4 |
| Event | Peak of hip ABD torque (0.10 ± 0.07 Nm/kg) at medium medial pert. | Hip flex. torque onset at medial lateral pert. | Hip flex. angle change onset at minimal lateral pert. | EMG of hip ADD onset at medium medial pert. | EMG of hip ext. onset at minimal lateral pert. | EMG of hip flex. onset at minimal lateral pert. | Hip ext. angle change onset at maximal medial pert. |
| Time [ms] | 480.6 | 490.9 | 504.7 | 510.4 | 513.9 | 523.5 | 523.7 |
| Event | Peak MMG of hip flex. at minimal lateral pert. | Peak MMG of hip ext. at minimal medial pert. | Peak power generating (0.03 ± 0.02 W/kg) at medium medial pert. | Peak of EMG of hip ABD at medial lateral pert. | Peak MMG of hip ABD at minimal lateral pert. | Peak of EMG of hip ABD at minimal lateral pert. | Peak of hip ABD torque (0.09 ± 0.06 Nm/kg) at minimal medial pert. |
| Time [ms] | 536.1 | 542.0 | 544.4 | 544.9 | 547.1 | 573.8 | 555.0 |
| Event | Peak MMG of hip flex. at medial lateral pert. | Peak power absorbing (0.05 ± 0.02 W/kg) at minimal lateral pert. | Peak of EMG of hip flex. at medial lateral pert. | Peak of EMG of hip ext. at medial lateral pert. | EMG of hip ADD onset at minimal lateral pert. | Peak power absorbing (0.15 ± 0.08 W/kg) at medial lateral pert. | EMG of hip ABD onset at minimal medial pert. |
| Time [ms] | 562.1 | 581.9 | 586.6 | 589.1 | 597.6 | 645.4 | 599.7 |
| Event | Peak of EMG of hip ADD at minimal medial pert. | EMG of hip ext. onset at medium medial pert. | Power absorbing onset at maximal medial pert. | EMG of hip ADD onset at maximal lateral pert. | EMG onset of hip flex. at medium medial pert. | Peak angle of hip flex. (2.1 ± 1.2 deg) at medial lateral pert. | Peak of EMG of hip ext. at minimal lateral pert. |
| Time [ms] | 601.9 | 604.7 | 607.6 | 611.1 | 615.6 | 621.3 | 624.3 |
| Event | Angle change onset of hip ABD at maximal lateral pert. | Peak of hip ext torque (0.40 ± 0.23 Nm/kg) at medial lateral pert. | Peak MMG of hip flex. at minimal medial pert. | EMG of hip ADD onset at medial lateral pert. | Peak of hip ADD torque (0.37 ± 0.11 Nm/kg) at minimal lateral pert. | Peak angle of hip ABD (2.4 ± 1.7 deg) at minimal medial pert. | Peak of hip ADD torque (0.79 ± 0.19 Nm/kg) at medial lateral pert. |
| Time [ms] | 626.9 | 634.4 | 637.0 | 644.4 | 651.1 | 656.4 | 663.7 |
| Event | Hip ADD torque onset at maximal medial pert. | Hip flex. torque onset at maximal lateral pert. | Peak of EMG of hip flex. at minimal lateral pert. | Peak MMG of hip ADD at minimal medial pert. | Peak MMG of hip ABD at minimal medial pert. | Peak of hip ABD torque (0.15 ± 0.09 Nm/kg) at maximal medial pert. | Peak of EMG of hip flex. at maximal lateral pert. |
| Time [ms] | 664.3 | 664.4 | 664.9 | 671.1 | 678.4 | 678.6 | 681.9 |
| Event | Peak of EMG of hip ABD at maximal lateral pert. | Peak of hip ADD torque (1.01 ± 0.19 Nm/kg) at maximal lateral pert. | Peak ABD hip angle (3.2 ± 2.1 deg) of at medium medial pert. | Peak hip flex. torque (0.19 ± 0.10 Nm/kg) at minimal medial pert. | Peak MMG of hip ABD at medial lateral pert. | Flex. hip torque onset at minimal lateral pert. | Hip ABD angle change onset of at medial lateral pert. |
| Time [ms] | 684.6 | 690.1 | 696.8 | 697.7 | 698.6 | 703.6 | 707.7 |
| Event | Peak MMG of hip ADD at minimal lateral pert. | Peak MMG of hip ext. at medial lateral pert. | Peak MMG of hip ABD at medium medial pert. | Peak of EMG of hip ADD at minimal lateral pert. 4 | Peak MMG of hip flex. at medium medial pert. | Peak power generating (0.08 ± 0.04 W/kg) at medial lateral pert. | Peak MMG of hip ext. at medium medial pert. |
| Time [ms] | 716.1 | 716.3 | 719.0 | 726.5 | 728.8 | 730.8 | 732.4 |
| Event | Peak of hip ext. torque (0.24 ± 0.15 Nm/kg) at minimal lateral pert. | Peak of EMG of hip ext. at maximal lateral pert. | Peak MMG of hip ABD at maximal lateral pert. | Peak of EMG of hip ADD at medium medial pert. | EMG onset of hip ext. at maximal medial pert. | Peak angle of hip ADD (2.2 ± 1.2 deg) at minimal lateral pert. | Power generating onset at minimal lateral pert. |
| Time [ms] | 739.9 | 749.7 | 753.2 | 761.9 | 762.9 | 765.9 | 771.0 |
| Event | Peak of EMG of hip ext. at medium medial pert. | Peak angle of hip flex. (2.4 ± 1.2 deg) at minimal medial pert. | Peak power generating (0.21 ± 0.12 W/kg) at maximal lateral pert. | Peak power absorbing (0.26 ± 0.11 W/kg) at maximal lateral pert. | Peak power generating (0.13 ± 0.19 W/kg) at maximal medial pert. | Peak of hip flex. torque (0.27 ± 0.15 Nm/kg) at medium medial pert. | Peak angle of hip flex. (4.3 ± 2.3 deg) at medium medial pert. |
| Time [ms] | 772.9 | 773.0 | 787.1 | 793.1 | 807.2 | 807.9 | 810.1 |
| Event | Peak MMG of hip ADD at medium medial pert. | Peak of EMG of hip flex at medium medial pert. | Power absorbing onset at minimal medial pert. | Peak angle of hip ADD (2.9 ± 1.8 deg) at medial lateral pert. | Angle change onset of hip ext. at minimal lateral pert. | Power absorbing onset at medium medial pert. | Peak MMG of hip ADD at medial lateral pert. |
| Time [ms] | 818.7 | 834.2 | 835.9 | 842.7 | 842.9 | 844.7 | 856.4 |
| Event | Peak MMG of hip ADD at medial lateral pert. | EMG onset of hip ext. atminimal medial pert. | Angle change onset of hip ADD at maximal medial pert. | Peak MMG of hip flex. at maximal lateral pert. | Angle change onset of hip ADD at medium medial pert. | Peak MMG of hip ext. at minimal lateral pert. | EMG onset hip flex at minimal medial pert. |
| Time [ms] | 863.0 | 868.3 | 872.3 | 873.7 | 873.9 | 874.9 | 881.2 |
| Event | Peak MMG of hip ABD at maximal medial pert. | Hip ADD torque onset at medium medial pert. | Peak angle of hip flex. at minimal lateral pert. 0.9 ± 0.3 deg | Peak MMG of hip ADD at maximal medial pert. | Peak MMG of hip flex. at maximal medial pert. | Peak of hip ext torque (0.48 ± 0.31 Nm/kg) at maximal lateral pert. | Angle change onset of hip ext. at maximal lateral pert. |
| Time [ms] | 885.9 | 890.2 | 892.8 | 899.4 | 912.6 | 921.5 | 924.2 |
| Event | Angle change onset of hip ABD at minimal lateral pert. | Peak MMG of hip ABD at medium medial pert. | Peak MMG of hip ABD atminimal medial pert. | Peak angle of hip ABD (5.5 ± 2.4 deg) at maximal medial pert. | Peak MMG of hip flex. at maximal medial pert. | Peak angle of hip ext. (1.8 ± 1.6 deg) at maximal medial pert. | Peak MMG of hip ext. at maximal lateral pert. |
| Time [ms] | 930.5 | 953.9 | 962.7 | 971.9 | 982.9 | 1016.2 | 1020.9 |
| Event | Peak power generating (0.05 ± 0.06 W/kg) at minimal lateral pert. | Hip ABD torque onset at minimal lateral pert. | Peak MMG of hip ext. at minimal medial pert. | Peak MMG of hip ext. at maximal medial pert. | Peak angle of hip flex. (6.9 ± 4.3 deg) at maximal lateral pert. | Peak angle of hip ADD (3.9 ± 2.3 deg) at maximal lateral pert. | Peak MMG of hip ext. at maximal medial pert. |
| Time [ms] | 1025.5 | 1026.4 | 1037.0 | 1039.3 | 1061.3 | 1066.7 | 1067.3 |
| Event | Angle change onset of hip ext. at medial lateral pert. | Hip ADD torque onset at minimal medial pert. | Peak of hip flex. torque (0.32 ± 0.13 Nm/kg) at maximal medial pert. | Peak MMG of hip ADD at maximal lateral pert. | Hip ABD torque onset at medial lateral pert. | Peak power absorbing (0.03 ± 0.02 W/kg) at minimal medial pert. | Hip ADD angle change onset of at minimal medial pert. |
| Time [ms] | 1069.8 | 1072.7 | 1092.8 | 1097.2 | 1122.8 | 1213.9 | 1215.1 |
| Event | Peak MMG of hip ADD at maximal medial pert. | Peak MMG of hip ABD at maximal medial pert. | Hip ABD torque onset at maximal lateral pert. | Peak MMG of hip ADD at maximal lateral pert. | Hip ext. torque onset at minimal medial pert. | Peak MMG of hip flex. at minimal medial pert. | Angle change onset of hip ext. at minimal medial pert. |
| Time [ms] | 1223.0 | 1228.2 | 1245.2 | 1251.8 | 1252.3 | 1256.7 | 1312.8 |
| Event | Peak angle of hip flex. (9.1 ± 5.9 deg) at maximal medial pert. | Peak angle of hip ext. (1.9 ± 1.3 deg) at maximal lateral pert. | Ext. torque onset at medium medial pert. | Peak power absorbing (0.04 ± 0.02 W/kg) at medium medial pert. | Peak of hip flex. torque (0.25 ± 0.15 Nm/kg) at maximal lateral pert. | Hip ext. torque onset at maximal medial pert. | Angle change onset of hip ext. at medium medial pert. |
| Time [ms] | 1318.1 | 1346.1 | 1347.1 | 1311.4 | 1352.7 | 1357.9 | 1360.2 |
| Event | Peak power absorbing (0.11 ± 0.09 W/kg) at maximal medial pert. | Peak of hip ABD torque (0.04 ± 0.03 Nm/kg) at minimal lateral pert. | Peak of hip flex. torque (0.15 ± 0.10 N m/kg) at medial lateral pert. | Peak angle of hip ABD (2.4 ± 1.4 deg) at maximal lateral pert. | Peak angle of hip ADD (2.8 ± 3.4 deg) at maximal medial pert. | Peak angle of hip ABD (1.1 ± 0.8 deg) at minimal lateral pert. | Peak angle of hip ABD (1.8 ± 0.7 deg) at medial lateral pert. |
| Time [ms] | 1370.8 | 1386.7 | 1387.2 | 1407.3 | 1417.8 | 1430.9 | 1432.0 |
| Event | Peak of hip ABD torque (0.04 ± 0.03 Nm/kg) at medial lateral pert. | Peak of hip ADD torque (0.11 ± 0.08 Nm/kg) at minimal medial pert. | Peak angle of hip ext. (1.1 ± 0.7 deg) at minimal lateral pert. | Peak angle of hip ext. (1.4 ± 0.4 deg) at medial lateral pert. | Peak of hip ADD torque (0.19 ± 0.10 Nm/kg) at medium medial pert | Peak of hip flex. torque (0.09 ± 0.05 Nm/kg) at minimal lateral pert. | Peak of hip ext. torque (0.09 ± 0.09 Nm/kg) at minimal medial pert. |
| Time [ms] | 1486.4 | 1586.0 | 1593.2 | 1613.1 | 1606.2 | 1665.6 | 1667.8 |
| Event | Peak angle of hip ADD (1.5 ± 0.5 deg) at medium medial pert. | Peak angle of hip ADD (1.1 ± 0.5 deg) at minimal medial pert. | Peak of hip ABD torque (0.08 ± 0.05 Nm/kg) at maximal lateral pert. | Peak angle of hip ext. (0.9 ± 0.7 deg) at minimal medial pert. | Peak of hip ADD torque (0.32 ± 0.19 Nm/kg) at maximal medial pert. | Peak of hip ext. torque (0.17 ± 0.11 Nm/kg) at maximal medial pert. | Peak of hip ext. torque (0.13 ± 0.10 Nm/kg) at medium medial pert. |
| Time [ms] | 1729.7 | ||||||
| Event | Peak angle of hip ext. (1.4 ± 1.0 deg) at medium medial pert. |
| Time [ms] | 86.7 | 93.1 | 94.6 | 95.2 | 96 | 100.5 | 101.1 |
| Event | CoP lateral displacement onset at maximal pert. | CoM medial displacement onset at maximal pert. | CoP medial displacement onset at medial pert. | CoP medial displacement onset at maximal pert. | Weight transfer onset at 50% preload [25] | CoP lateral displacement onset at medial pert. | CoM lateral displacement onset at maximal pert. |
| Time [ms] | 104 | 109.0 | 114.0 | 114.6 | 115.0 | 120 | 125.8 |
| Event | Weight transfer onseta at 65% preload [25] | CoM medial displacement onset at minimal pert. | CoM lateral displacement onset at medial pert. | CoP medial displacement onset at minimal pert. | CoP lateral displacement onset at minimal pert. | Weight transfer onset at 80% preload [25] | CoM medial displacement onset at medial pert. |
| Time [ms] | 131.2 | 140 | 150 | 156.6 | 191.1 | 234 | 622.4 |
| Event | CoM lateral displacement onsetat minimal pert. | GRF onset under the initial swing leg; LSS [5] | GRF onset under the initial swing leg; UCS [5] | CoP ML displacement onset [24] | CoP AP displacement onset [24] | Weight transfer time [19] | Peak CoP medial displacementat minimal pert. 86.7 ± 12.8 mm |
| Left step, swing leg: CoP ML: 0.045 ± 0.009 m; CoP AP: −0.031 ± 0.006 m; stance leg: CoP ML: −0.074 ± 0.005 m; CoP AP: −0.051 ± 0.006 m | |||||||
| Right step, swing leg: CoP ML: −0.040 ± 0.007 m; CoP AP: −0.030 ± 0.004 m; stance leg: CoP ML: 0.089 ± 0.007 m; CoP AP: −0.049 ± 0.007 m | |||||||
| Time [ms] | 642.7 | 656.6 | 662.4 | 674.7 | 721.1 | 746.8 | 756.7 |
| Event | Peak CoP lateral displacementat minimal pert. (74.2 ± 10.3 mm) | Peak CoP lateral displacement at medial pert. (145.3 ± 16.3 mm) | Peak CoP medial displacement at medial pert. (145.6 ± 11.7 mm) | Peak CoM medial displacementat minimal pert. (30.4 ± 10.4 mm) | Peak CoM lateral displacementat minimal pert. (30.3 ± 9.0 mm) | Peak CoM lateral displacement at medial pert. (60.7 ± 11.9 mm) | Peak CoM medial displacement at medial pert. (63.7 ± 12.1 mm) |
| Time [ms] | 798.9 | 835.2 | 991.3 | 975.6 | |||
| Event | Peak CoP medial displacement at maximal pert. (174.2 ± 15.8 mm) | Peak CoP lateral displacement at maximal pert. (175.3 ± 13.4 mm) | Peak CoM lateral displacement at maximal pert. (119.1 ± 27.9 mm) | Peak CoM medial displacement at maximal pert. (122.2 ± 21.1 mm) | |||
References
- Rogers, M.W.; Mille, M.L. Balance perturbations. Handb. Clin. Neurol. 2018, 159, 85–105. [Google Scholar] [CrossRef] [PubMed]
- Kędziorek, J.; Błażkiewicz, M. Effect of voluntary muscle contraction on postural stability in healthy adults. Adv. Rehabil. 2021, 35, 33–37. [Google Scholar] [CrossRef]
- Morasso, P. Centre of pressure versus centre of mass stabilization strategies: The tightrope balancing case. R. Soc. Open Sci. 2020, 7, 200111. [Google Scholar] [CrossRef] [PubMed]
- Horak, F.B.; Nashner, L.M. Central programming of postural movements: Adaptation to altered support-surface configurations. J. Neurophysiol. 1986, 55, 1369–1381. [Google Scholar] [CrossRef] [PubMed]
- Mille, M.L.; Johnson, M.E.; Martinez, K.M.; Rogers, M.W. Age-dependent differences in lateral balance recovery through protective stepping. Clin. Biomech. 2005, 20, 607–616. [Google Scholar] [CrossRef]
- Patton, J.L.; Hilliard, M.J.; Martinez, K.; Mille, M.L.; Rogers, M.W. A simple model of stability limits applied to sidestepping in young, elderly and elderly fallers. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2006, 2006, 3305–3308. [Google Scholar] [CrossRef]
- Welch, T.D.; Ting, L.H. Mechanisms of motor adaptation in reactive balance control. PLoS ONE 2014, 9, e96440. [Google Scholar] [CrossRef]
- Petró, B.; Papachatzopoulou, A.; Kiss, R.M. Devices and tasks involved in the objective assessment of standing dynamic balancing—A systematic literature review. PLoS ONE 2017, 12, e0185188. [Google Scholar] [CrossRef]
- Hof, A.L.; Curtze, C. A stricter condition for standing balance after unexpected perturbations. J. Biomech. 2016, 49, 580–585. [Google Scholar] [CrossRef]
- Tan, J.L.; Perera, T.; McGinley, J.L.; Yohanandan, S.A.C.; Brown, P.; Thevathasan, W. Neurophysiological analysis of the clinical pull test. J. Neurophysiol. 2018, 120, 2325–2333. [Google Scholar] [CrossRef]
- Williams, H.G.; McClenaghan, B.A.; Dickerson, J. Spectral characteristics of postural control in elderly individuals. Arch. Phys. Med. Rehabil. 1997, 78, 737–744. [Google Scholar] [CrossRef] [PubMed]
- Kędziorek, J.; Błażkiewicz, M.; Kaczmarczyk, K. Using nonlinear measures to evaluate postural control in healthy adults during bipedal standing on an unstable surface. Acta Bioeng. Biomech. 2022, 24, 9–17. [Google Scholar] [CrossRef]
- Winter, D.A. Human balance and posture control during standing and walking. Gait Posture 1995, 3, 193–214. [Google Scholar] [CrossRef]
- Henry, S.M.; Fung, J.; Horak, F.B. EMG responses to maintain stance during multidirectional surface translations. J. Neurophysiol. 1998, 80, 1939–1950. [Google Scholar] [CrossRef] [PubMed]
- Rietdyk, S.; Patla, A.E.; Winter, D.A.; Ishac, M.G.; Little, C.E. Balance recovery from medio-lateral perturbations of the upper body during standing. J. Biomech. 1999, 32, 1149–1158. [Google Scholar] [CrossRef]
- Nashner, L.M. Adapting reflexes controlling the human posture. Exp. Brain Res. 1976, 26, 59–72. [Google Scholar] [CrossRef]
- Nashner, L.M.; McCollum, G. The organization of human postural movements: A formal basis and experimental synthesis. Behav. Brain Sci. 2010, 8, 135–150. [Google Scholar] [CrossRef]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef]
- Luchies, C.W.; Wallace, D.; Pazdur, R.; Young, S.; DeYoung, A.J. Effects of age on balance assessment using voluntary and involuntary step tasks. J. Gerontol. A Biol. Sci. Med. Sci. 1999, 54, M140–M144. [Google Scholar] [CrossRef]
- Zhu, R.T.; Lyu, P.-Z.; Li, S.; Tong, C.Y.; Ling, Y.T.; Ma, C.Z. How Does Lower Limb Respond to Unexpected Balance Perturbations? New Insights from Synchronized Human Kinetics, Kinematics, Muscle Electromyography (EMG) and Mechanomyography (MMG) Data. Biosensors 2022, 12, 430. [Google Scholar] [CrossRef]
- Matjacić, Z.; Voigt, M.; Popović, D.; Sinkjaer, T. Functional postural responses after perturbations in multiple directions in a standing man: A principle of decoupled control. J. Biomech. 2001, 34, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Pidcoe, P.E.; Rogers, M.W. A closed-loop stepper motor waist-pull system for inducing protective stepping in humans. J. Biomech. 1998, 31, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Mille, M.L.; Johnson-Hilliard, M.; Martinez, K.M.; Zhang, Y.; Edwards, B.J.; Rogers, M.W. One step, two steps, three steps more … Directional vulnerability to falls in community-dwelling older people. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 1540–1548. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-J.; Liang, J.N.; Chen, B.; Aruin, A.S. Characteristics of medial-lateral postural control while exposed to the external perturbation in step initiation. Sci. Rep. 2019, 9, 16817. [Google Scholar] [CrossRef]
- Inacio, M.; Creath, R.; Rogers, M.W. Effects of aging on hip abductor-adductor neuromuscular and mechanical performance during the weight transfer phase of lateral protective stepping. J. Biomech. 2019, 82, 244–250. [Google Scholar] [CrossRef]
- Matjacić, Z.; Johannesen, I.L.; Sinkjaer, T. A multi-purpose rehabilitation frame: A novel apparatus for balance training during standing of neurologically impaired individuals. J. Rehabil. Res. Dev. 2000, 37, 681–691. [Google Scholar]
- Claudino, R.; dos Santos, E.C.; Santos, M.J. Compensatory but not anticipatory adjustments are altered in older adults during lateral postural perturbations. Clin. Neurophysiol. Off. J. Int. Fed. Clin. Neurophysiol. 2013, 124, 1628–1637. [Google Scholar] [CrossRef]
- Martelli, D.; Vashista, V.; Micera, S.; Agrawal, S.K. Direction-Dependent Adaptation of Dynamic Gait Stability Following Waist-Pull Perturbations. IEEE Trans. Neural Syst. Rehabil. Eng. A Publ. IEEE Eng. Med. Biol. Soc. 2016, 24, 1304–1313. [Google Scholar] [CrossRef]
- Madehkhaksar, F.; Klenk, J.; Sczuka, K.; Gordt, K.; Melzer, I.; Schwenk, M. The effects of unexpected mechanical perturbations during treadmill walking on spatiotemporal gait parameters, and the dynamic stability measures by which to quantify postural response. PLoS ONE 2018, 13, e0195902. [Google Scholar] [CrossRef]
- Roeles, S.; Rowe, P.J.; Bruijn, S.M.; Childs, C.R.; Tarfali, G.D.; Steenbrink, F.; Pijnappels, M. Gait stability in response to platform, belt, and sensory perturbations in young and older adults. Med. Biol. Eng. Comput. 2018, 56, 2325–2335. [Google Scholar] [CrossRef]
- Chouamo, A.K.; Griego, S.; Lopez, F.A.S. Reaction time and hand dominance. J. Sci. Med. 2020, 3, 1–7. [Google Scholar]
- de Graaf, J.B.; Frolov, A.; Fiocchi, M.; Nazarian, B.; Anton, J.L.; Pailhous, J.; Bonnard, M. Preparing for a motor perturbation: Early implication of primary motor and somatosensory cortices. Hum. Brain Mapp. 2009, 30, 575–587. [Google Scholar] [CrossRef] [PubMed]
- Cè, E.; Longo, S.; Limonta, E.; Coratella, G.; Rampichini, S.; Esposito, F. Peripheral fatigue: New mechanistic insights from recent technologies. Eur. J. Appl. Physiol. 2020, 120, 17–39. [Google Scholar] [CrossRef] [PubMed]
- Ling, Y.T.; Ma, C.Z.; Shea, Q.T.; Zheng, Y.-P. Sonomechanomyography (SMMG): Mapping of Skeletal Muscle Motion Onset during Contraction Using Ultrafast Ultrasound Imaging and Multiple Motion Sensors. Sensors 2020, 20, 5513. [Google Scholar] [CrossRef] [PubMed]
- McGlone, F.; Reilly, D. The cutaneous sensory system. Neurosci. Biobehav. Rev. 2010, 34, 148–159. [Google Scholar] [CrossRef] [PubMed]

| PubMed | Google Scholar | ScienceDirect | EBSCO |
|---|---|---|---|
| (postural control) AND (perturbation) AND (medio-lateral) | (postural control) AND (perturbation) AND (medio-lateral) | (postural control) AND (perturbation) AND (medio-lateral) | (postural control) AND (perturbation) AND (medio-lateral) NOT (treadmill) |
| (postural control) AND (medio lateral) AND (pushing) NOT (treadmill) | |||
| (postural control) AND (medial perturbation) NOT (treadmill) | (postural control) AND (medial perturbation) NOT (treadmill) NOT (walking) NOT (walk) NOT (older) NOT (disease) NOT (unilateral) NOT(children) NOT (monopedal) NOT (cortex) | (postural strategy) AND (balance) AND (medio lateral direction perturbation) AND (standing) | (postural control) AND (medial perturbation) NOT (treadmill) |
| (postural control) AND (medio lateral) AND (perturbation) AND (standing) | (postural control) AND (medio lateral) AND (perturbation) AND (standing) | ||
| (postural equilibrium) AND (medio lateral) AND (perturbation) NOT (gait) | (postural equilibrium) AND (medio lateral perturbation) NOT (gait) | ||
| (postural control) AND (standing) AND (external perturbations) AND (healthy adults) | (postural control strategy) AND (medio lateral) AND (perturbation) |
| Study and Quality | Study Group: Age (Years); Body Mass (kg); Body Height (cm) | Aim/Partipant Task | Equipment/Perturbation Source/Place of Impact/Essential Description/Start of the Measurement | Results/Findings |
|---|---|---|---|---|
| Luchies et al. (1999) [19] Quality: 13/19 | Young (Y): 13 W Age: 20.9 ± 2.5 Weight 62 ± 5.4 Height: 170.3 ± 6.9 Elderly (E): 11 W Age: 68 ± 4.1 Weight: 69 ± 14.6 Height: 165.8 ± 6.8 | Aim: to investigate whether the performance on an involuntary step task was comparable to the performance on a voluntary step task. Subjects stepped as fast as possible in the direction of a minimally destabilizing lateral waist pull (voluntary step task), or they responded naturally to a large destabilizing lateral waist pull (involuntary step task). | Kinematics-Optotrak System (200 Hz). Two force plates measured the GRF from both legs (2000 Hz). EMG bilateral (2000 Hz): TA. Pulling/Pelvis. Safety harness. The second harness around the waist incorporates padded blocks. Lateral pulls were produced using electronically released weight and cable systems. The waist pull distances were 8.7% and 1.3% of the waist height. Start of the measurements: when the waist pull force exceeded a 5 N. |
|
| Rietdyk et al. (1999) [15] Quality: 13/19 | 10 M Age: 26 ± 4.2 Weight: 86 ± 8.2 Height: 181.6 ± 7.1 | Aim: to provide insights into the underlying motor mechanisms used in postural control by determining the joint moments during balance recovery from ML perturbations. Participants were instructed that they would be receiving pushes to the trunk or pelvis, and that they should attempt to maintain balance without taking a step. | 42 infrared emitting diodes (IREDs) were placed on the participant; three IREDs (40 Hz) were placed on the perturbation device; uni-axial force transducer. Two force plates (480 Hz). Pushing/Pelvis and Shoulder. The impulse of ML perturbation: Shoulder: 13.1 to 28.9 Ns; Pelvis: 16.8 to 31.4 Ns. Start of the measurements: Bias + 2SD. |
|
| Matjacić et al. (2001) [21] Quality: 13/19 | 8 M Age: 31 ± 6.7 Weight 75.8 ± 11.4 Height: 182 ± 8.8 | Aim: to assess functional postural responses by analyzing the net joint torques (NJT) in the ankles and the hips, resulting from perturbations delivered in multiple directions to subjects standing quietly. To stand relaxed prior to perturbation and attain the same posture throughout the trial after recovering from perturbation. | Two AMTI force plates (100 Hz). Multi-purpose rehabilitation frame (MRF) consists of two 2-dof rot joints, two 1-dof rot joints, two vertical supportive rods and a bracing system. Cylindrical pegs were used to constrain the position and orientation of the feet. Inclination angles of the MRF collected by potentiometers (Spectrol 157-9002-103) mounted to one of the 2-dof joints of the MRF. Pulling/Pelvis. Max perturbation amplitude: 34–60 Nm. Start of the measurements: 500 ms prior to the beginning of the perturbation and lasting for 3.5 s. |
|
| Mille et al. (2005) [5] Quality: 13/19 | Y: 10 Age: 24 ± 1.4 Weight: 60.9 ± 6.3 Height: 167.3 ± 5 E: 10 Age: 73.3 ± 6.3 Weight: 62.7 ± 14.2 Height: 159.3 ± 5.1 | Aim: to determine age-related differences in protective stepping behavior in response to lateral waist-pull perturbations of postural balance. Subjects were instructed to react naturally to prevent themselves from falling. | Kinematics-Motus six-camera system (60 Hz). Two force plates (500 Hz). Pulling/Pelvis. Safety harness. Protective stepping responses were evoked by a motor-driven, waist-pull system [22]. The lateral pulls of constant magnitude (amplitude: 22.5 cm; velocity 31.5 cm/s; acceleration: 900 cm/s2). Two cables were attached on one end to a rigid connection on a belt at the level of the subject’s waist and on the other end to the puller system. Start of the measurements: 5 s after start of kinematics and GRF recording. |
|
| Mille et al. (2013) [23] Quality: 12/19 | Y: 26 (7 M, 19 W) Age: 23.5 ± 3.2 Weight: 70.3 ± 13.4 Height: 169.6 ± 9 E: 49 (11 M, 38 W) Non-faller: 30 (no data) Age: 72.5 ± 5.9 Weight: 66.4 ± 13.1 Height: 163.5 ± 8.2 Faller: 19 (no data) Age: 75.2 ± 7.8 Weight: 68.1 ± 12.1 Height: 161.2 ± 5.3 | Aim: to determine the stepping response patterns evoked by different directions of externally-applied postural disturbances in younger and older adults, in relation to falls. To react naturally to prevent themselves from falling. | Kinematics-Motus six-camera system (60 Hz). Two force plates (500 Hz). Motorized pelvic-pull system. Balance perturbed through a pulley cable and switching system (displacement: 18 cm; velocity: 36 cm/s, acceleration: 720 cm/s2). Pulling/Pelvis. Start of the measurements: 5 s after start of kinematics. |
|
| Lee et al. (2019) [24] Quality: 13/19 | 11 (5 M, 6 W) Age: 28.09 ± 4.35 Weight: 71.09 ± 18.75 Height: 167 ± 7 | Aim: to examine the effects of external perturbation and landing orientation on ML control stability in step initiation. To stand still with feet shoulder-width apart, and even body weight distribution between feet. | One force platform AMTI (1000 Hz). EMG bilateral (Myopac, 1000 Hz): TA, MG, RF, BF, GMed, EO, RA, ES. Two accelerometers: (1) the pendulum accelerometer (model 208CO3, PCB Piezotronics Inc, USA); (2) the participant accelerometer (model 1356a16, PCB Piezotronics Inc, USA) on the dorsal surface at the level of L5/S1. A pendulum (30 cm long wooden stick) and a flag. Pushing/Shoulder. A load (5% of the individual’s body mass) was attached to the pendulum. Initial angle of 30° to the vertical (0.8 m from the body). Released 1–2 s after the start of data collection. Start of the measurements: 0 ms indicates pendulum release. |
|
| Inacio et al. (2019) [25] Quality: 13/19 | Y: 15 (7 M, 8 W) Age: 29.1 ± 1.1 Weight: 70 ± 3.6 Height: 174 ± 7 E: 15 (9 M, 6 W) Age: 71.3 ± 0.9 Weight: 80.4 ± 4.1 Height: 170 ± 2 | Aim: this study investigated the influence of hip abductor–adductor neuromuscular performance on the weight transfer phase of lateral protective stepping. To stand still and recover balance with a single lateral step. | Kinematics-Vicon System (120 Hz). Two AMTI force plates (600 Hz). EMG bilateral (1500 Hz): GMed, TFL, ADD. A motorized waist-pull system [22]. To laterally shift their weight to distribute 50%, 65%, or 80% of BW onto the pre-determined stepping limb, using real-time visual feedback of the vertical GRF provided by a monitor. Pulling/Pelvis. Start of the measurements: moment of perturbation triggering. |
|
| Zhu et al. (2022) [20] Quality: 12/19 | 12 (6 M, 6 W) Age: 20.9 ± 0.7 Weight: 58.3 ± 6.2 Height: 169.9 ± 6.9 | Aim: to investigate how rapidly the lower-limb muscles and joints would respond to the unexpected standing balance perturbations. To stand still and recover balance with a single lateral step. | Kinematics- eight-camera Vicon System (250 Hz). Two AMTI force plates (1000 Hz). EMG (2000 Hz) unilateral: TA, GMed, RF, ST, IL, GMax, AM. The waist-pull, hardness system. The maximal ML pulling displacements was set as 4%, 6%, and 8% of each participant’s height. The pulling magnitude corresponded to the 1/3, 2/3, and 3/3 of the maximal pulling displacement, respectively. Each pull’s duration, displacement, and velocity were measured based on the flash time of infrared light. Pulling/Pelvis. Start of the measurements: start of balance perturbation. |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borkowski, R.; Błażkiewicz, M. Postural Reactions to External Mediolateral Perturbations: A Review. Appl. Sci. 2023, 13, 1696. https://doi.org/10.3390/app13031696
Borkowski R, Błażkiewicz M. Postural Reactions to External Mediolateral Perturbations: A Review. Applied Sciences. 2023; 13(3):1696. https://doi.org/10.3390/app13031696
Chicago/Turabian StyleBorkowski, Rafał, and Michalina Błażkiewicz. 2023. "Postural Reactions to External Mediolateral Perturbations: A Review" Applied Sciences 13, no. 3: 1696. https://doi.org/10.3390/app13031696
APA StyleBorkowski, R., & Błażkiewicz, M. (2023). Postural Reactions to External Mediolateral Perturbations: A Review. Applied Sciences, 13(3), 1696. https://doi.org/10.3390/app13031696