
Comparative Study of Ozonated Olive Oil and Extra Virgin Olive Oil Effects on Oral Hygiene

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Aim of the Study
2.2. Materials
2.3. Inclusion Criteria
- minimum 20 teeth, excluding third molars
- PPD ≤ 3 mm
- absence of periodontitis and orthodontic appliances, without known allergy to any of the mouthwash components
2.4. Exclusion Criteria
- last periodontal treatment < 6 months
- patients suffering from systemic pathologies that may influence therapy such as: diabetes, neoplasms, pathologies of bone metabolism, disorders that compromise healing, radiation, immunosuppressive therapies, and anticoagulant therapies
- patients affected by periodontal disease PPD (periodontal probing depth) > 3 mm
- taking antibiotics < 6 months; anti-inflammatory drugs < 3 months; cortisone; contraceptive hormones
2.5. Methods
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Population (Age, Gender, and Environment)
3.2. Indices Changes
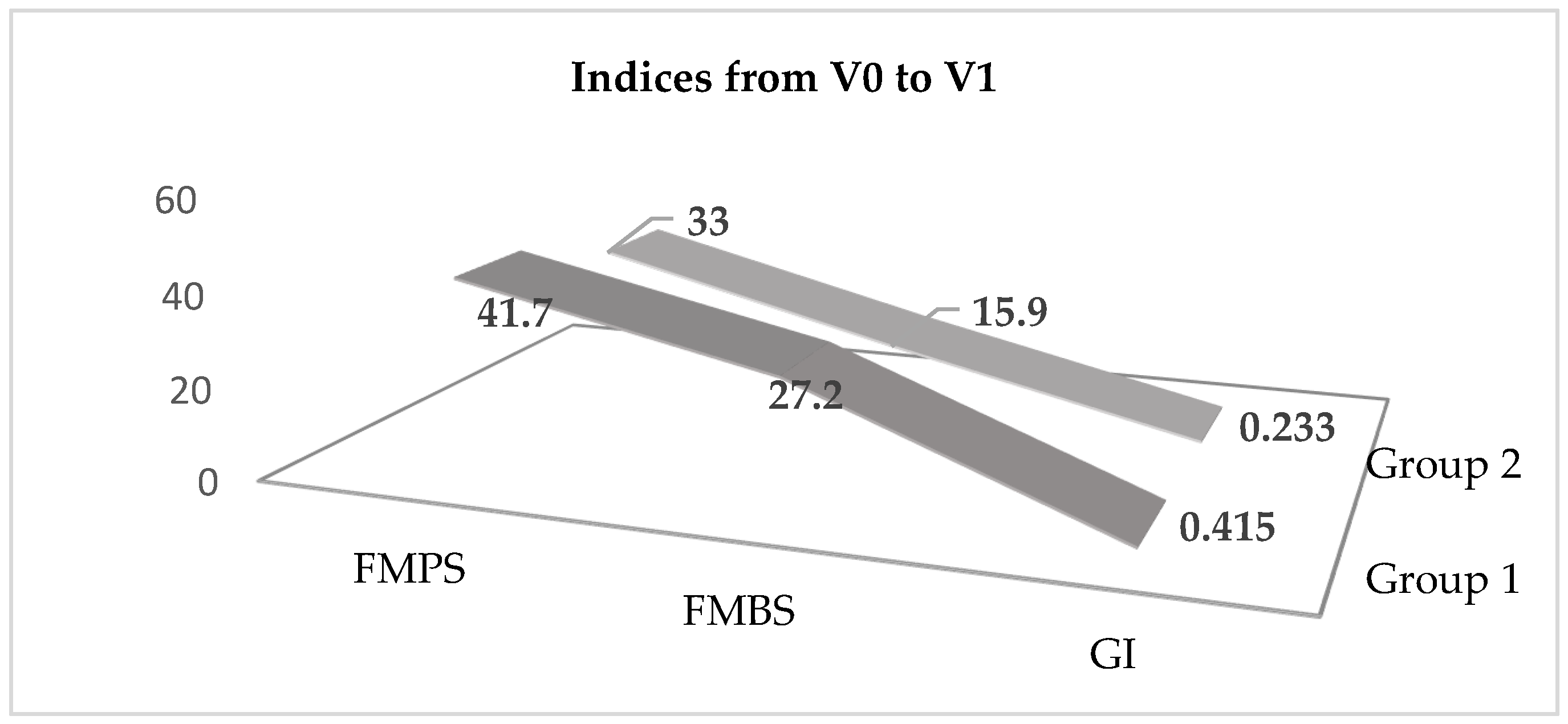
3.3. Variation of Indices from V0 to V1
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- De Almeida, N.R.; Beatriz, A.; Micheletti, A.C.; de Arruda, E.J. Ozonized vegetable oils and therapeutic properties: A review. Orbital. Electron. J. Chem. 2013, 4, 313–326. [Google Scholar] [CrossRef]
- Suh, Y.; Patel, S.; Kaitlyn, R.; Gandhi, J.; Joshi, G.; Smith, N.; Khan, S.A. Clinical utility of ozone therapy in dental and oral medicine. Med. Gas Res. 2019, 9, 163–167. [Google Scholar]
- Trombelli, L.; Farina, R.; Silva, C.O.; Tatakis, D.N. Plaque-induced gingivitis: Case definition and diagnostic considerations. J. Periodontol. 2018, 89, S46–S73. [Google Scholar] [CrossRef] [Green Version]
- Marilyn, E.L.; Vincent, D.E. Oral infections and antibiotic therapy. Otolaryngol. Clin. N. Am. 2011, 44, 57–78. [Google Scholar]
- Gupta, S.; Deepa, D. Applications of ozone therapy in dentistry. J. Oral Res. Rev. 2016, 8, 86. [Google Scholar]
- Kalemba, D.; Kunicka, A. Antibacterial and antifungal properties of essential oils. Curr. Med. Chem. 2003, 10, 813–829. [Google Scholar] [CrossRef]
- Takarada, K.; Kimizuka, R.; Takahashi, N.; Honma, K.; Okuda, K.; Kato, T. A comparison of the antibacterial efficacies of essential oils against oral pathogens. Oral Microbiol. Immunol. 2004, 19, 61–64. [Google Scholar] [CrossRef]
- Tricarico, G.; Rodrigues Orlandin, J.; Rocchetti, V.; Ambrosio, C.E.; Travagli, V. A critical evaluation of the use of ozone and its derivatives in dentistry. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 9071–9093. [Google Scholar]
- Ellen, R.P.; McCulloch, C.A. Evidence versus empiricism: Rational use of systemic antimicrobial agents for treatment of periodontitis. Periodontology 2000, 10, 29–44. [Google Scholar] [CrossRef]
- Georgiev, V.F.; Batakliev, T.T.; Anachkov, M.P.; Rakovsky, S.K. Study of Ozonated Olive Oil: Monitoring of the Ozone Absorption and Analysis of the Obtained Functional Groups. Ozone Sci. Eng. 2015, 37, 55–61. [Google Scholar] [CrossRef]
- Díaz, M.F.; Hernández, R.; Martínez, G.; Vidal, G.; Gómez, M.; Fernández, H.; Garcés, R. Comparative study of ozonized olive oil and ozonized sunflower oil. J. Braz. Chem. Soc. 2006, 17, 403–407. [Google Scholar] [CrossRef]
- Martin, S.L.; Sharon, S.; Carlos, J.C.; Man, H. Men and Oral Health: A Review of Sex and Gender Differences. Am. J. Mens Health 2021, 15, 15579883211016361. [Google Scholar]
- Mampieri, G.; Alushi, A.; Di Girolamo, M.; Rasicci, P.; Capogreco, M.; Marino, R.; Vanderlelie, J. Ozone therapy new protocols and innovations: A systematic review. J. Biol. Regul. Homeost. Agents 2022, 36, 117–121. [Google Scholar]
- Libonati, A.; Di Taranto, V.; Mea, A.; Montemurro, E.; Gallusi, G.; Angotti, V.; Nardi, R.; Paglia, L.; Marzo, G.; Campanella, V. Clinical antibacterial effectiveness Healozone Technology after incomplete caries removal. Eur. J. Paediatr. Dent. 2019, 20, 73–78. [Google Scholar]
- Sen, S.; Sen, S. Ozone therapy a new vista in dentistry: Integrated review. Med. Gas Res. 2020, 10, 189–192. [Google Scholar] [CrossRef]
- Badhe, H.; Kalaskar, R.; Balasubramanian, S.; Kamki, H.; Kalaskar, A. Antimicrobial Effect of Ozone Therapy in Deep Dentinal Carious Lesion: A Systematic Review. Int. J. Clin. Pediatr. Dent. 2022, 15, 252–260. [Google Scholar]
- Kapdan, A.; Kustarci, A.; Tunc, T.; Sumer, Z.; Arslan, S. Which is the most effective disinfection method in primary root canals: Conventional or newly developed ones? Niger. J. Clin. Pract 2015, 18, 538–543. [Google Scholar] [CrossRef] [Green Version]
- Goztas, Z.; Onat, H.; Tosun, G.; Sener, Y.; Hadimli, H.H. Antimicrobial effect of ozonated water, sodium hypochlorite and chlorhexidine gluconate in primary molar root canals. Eur. J. Dent. 2014, 8, 469–474. [Google Scholar] [CrossRef]
- Saini, R. Ozone therapy in dentistry: A strategic review. J. Nat. Sci. Biol. Med. 2011, 2, 151. [Google Scholar] [CrossRef] [Green Version]
- Pietrocola, G.; Ceci, M.; Preda, F.; Poggio, C.; Colombo, M. Evaluation of the antibacterial activity of a new ozonized olive oil against oral and periodontal pathogens. J. Clin. Exp. Dent. 2018, 10, e1103–e1108. [Google Scholar] [CrossRef]
- Cosola, S.; Giammarinaro, E.; Genovesi, A.M.; Pisante, R.; Poli, G.; Covani, U.; Marconcini, S. A short-term study of the effects of ozone irrigation in an orthodontic population with fixed appliances. Eur. J. Paediatr. Dent. 2019, 20, 15–18. [Google Scholar]
- Zakrzewski, W.; Dobrzynski, M.; Nowicka, J.; Pajaczkowska, M.; Szymonowicz, M.; Targonska, S.; Sobierajska, P.; Wiglusz, K.; Dobrzynski, W.; Lubojanski, A.; et al. The Influence of Ozonated Olive Oil-Loaded and Copper-Doped Nanohydroxyapatites on Planktonic Forms of Microorganisms. Nanomaterials 2020, 10, 1997. [Google Scholar] [CrossRef]
- Azarpazhooh, A.; Limeback, H. The application of ozone in dentistry: A systematic review of literature. J. Dent. 2008, 36, 104–116. [Google Scholar] [CrossRef]
- Smith, N.; Wilson, A.; Gandhi, J.; Vatsia, S.; Khan, S. Ozone therapy: An overview of pharmacodynamics, current research, and clinical utility. Med. Gas Res. 2017, 7, 212–219. [Google Scholar]
- Monzillo, V.; Lallitto, F.; Russo, A.; Poggio, C.; Scribante, A.; Arciola, C.R.; Bertuccio, F.R.; Colombo, M. Ozonized gel against four Candida species: A pilot study and clinical perspectives. Materials 2020, 13, 1731. [Google Scholar] [CrossRef] [Green Version]
- Bayer, S.; Kazancioglu, H.O.; Acar, A.H.; Demirtas, N.; Kandas, N.O. Comparison of laser and ozone treatments on oral mucositis in an experimental model. Lasers Med. Sci. 2017, 32, 673–677. [Google Scholar] [CrossRef]
- Al-Omiri, M.K.; Alhijawi, M.; Alzarea, B.K.; Hassan, R.S.A.; Lynch, E. Ozone treatment of recurrent aphthous stomatitis: A double blinded study. Sci. Rep. 2016, 6, 27772. [Google Scholar] [CrossRef]
- Colombo, M.; Ceci, M.; Felisa, E.; Poggio, C.; Pietrocola, G. Cytotoxicity evaluation of a new ozonized olive oil. Eur. J. Dent. 2018, 12, 585–589. [Google Scholar] [CrossRef] [Green Version]
- Santos, G.M.; Pacheco, R.L.; Bussadori, S.K.; Santos, E.M.; Riera, R.; de Oliveira Cruz Latorraca, C.; Mota, P.; Bellotto, E.F.B.C.; Martimbianco, A.L.C. Effectiveness and Safety of Ozone Therapy in Dental Caries Treatment: Systematic Review and Meta-analysis. J. Evid. Based Dent. Pract. 2020, 20, 101472. [Google Scholar] [CrossRef]
- Nagayoshi, M.; Fukuizumi, T.; Kitamura, C.; Yano, J.; Terashita, M.; Nishihara, T. Efficacy of ozone on survival and permeability of oral microorganisms. Oral. Microbiol. Immunol. 2004, 19, 240–246. [Google Scholar] [CrossRef]
- Shruthi, N.; Sardhar, M.; Shaswata, K.; Anish, V.; Deepan, C.; Vijay, K.C. Comparison of Ozonated Olive Oil and Chlorhexidine Gel as an Adjunct to Nonsurgical Periodontal Therapy for the Treatment of Chronic Periodontitis: A Randomized Controlled Clinical Trial. J. Pharm. Bioallied Sci. 2022, 14, S94–S98. [Google Scholar]
- Nardi, G.M.; Cesarano, F.; Papa, G.; Chiavistelli, L.; Ardan, R.; Jedlinski, M.; Mazur, M.; Grassi, R.; Grassi, F.R. Evaluation of Salivary Matrix Metalloproteinase (MMP-8) in Periodontal Patients Undergoing Non-Surgical Periodontal Therapy and Mouthwash Based on Ozonated Olive Oil: A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2020, 17, 6619. [Google Scholar] [CrossRef]
- Indurkar, M.S.; Verma, R. Effect of ozonated oil and chlorhexidine gel on plaque induced gingivitis: A randomized control clinical trial. J. Indian Soc. Periodontol. 2016, 20, 32–35. [Google Scholar]
- Nogales, C.G.; Ferrari, P.H.; Kantorovich, E.O.; Lage-Marques, J.L. Ozone therapy in medicine and dentistry. J. Contemp. Dent. Pract. 2008, 9, 75–84. [Google Scholar] [CrossRef]
- Tedesco, T.K.; Calvo, A.F.B.; Pássaro, A.L.; Araujo, M.P.; Ladewig, N.M.; Scarpini, S.; Lara, J.S.; Braga, M.M.; Gimenez, T.; Raggio, D.P. Nonrestorative treatment of initial caries lesion in primary teeth: A systematic review and network meta-analysis. Acta Odontol. Scand. 2022, 80, 1–8. [Google Scholar] [CrossRef]
- Kronenberg, O.; Lussi, A.; Ruf, S. Preventive effect of ozone on the development of white spot lesions during multibracket appliance therapy. Angle Orthod. 2009, 79, 64–69. [Google Scholar] [CrossRef] [Green Version]
- Rapone, B.; Ferrara, E.; Santacroce, L.; Topi, S.; Gnoni, A.; Dipalma, G.; Mancini, A.; Di Domenico, M.; Tartaglia, G.M.; Scarano, A.; et al. The Gaseous Ozone Therapy as a Promising Antiseptic Adjuvant of Periodontal Treatment: A Randomized Controlled Clinical Trial. Int. J. Environ. Res. Public Health 2022, 16, 985. [Google Scholar] [CrossRef]
- Lynch, E. Evidence-based efficacy of ozone for root canal irrigation. J. Esthet. Restor. Dent. 2008, 20, 287–293. [Google Scholar] [CrossRef]
- Hoigne, J.; Bader, H. The role of hydroxyl radical reactions in ozonation processes in aqueous solutions. Water Res. 1976, 10, 377.e86. [Google Scholar] [CrossRef]
- Patel, P.V.; Patel, A.; Kumar, S.; Holmes, J.C. Effect of subgingival application of topical ozonated olive oil in the treatment of chronic periodontitis: A randomized, controlled, double-blind, clinical and microbiological study. Minerva Stomatol. 2012, 61, 381–398. [Google Scholar]
- Ximenes, M.; Cardoso, M.; Astorg, F.; Arnold, R.; Pimenta, L.A.; de Sousa Vieria, R. Antimicrobial activity of ozone and NaF-chlorhexidine on early childhood caries. Braz. Oral Res. 2017, 5, 31.e2. [Google Scholar] [CrossRef] [Green Version]
- Mummolo, S.; Nota, A.; Caruso, S.; Quinzi, V.; Marchetti, E.; Marzo, G. Salivary Markers and Microbial Flora in Mouth Breathing Late Adolescents. BioMed Res. Int. 2018, 5, 8687608. [Google Scholar] [CrossRef]
- Srikanth, A.; Sathish, M.; Sri Harsha, A.V. Application of ozone in the treatment of periodontal disease. J. Pharm. Bioallied Sci. 2013, 5, S89–S94. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Baseline Characteristics of the Two Groups | Group 1 Ozonated Olive Oil MD ± DS | Group 2 Extra Virgin Olive Oil MD ± DS | ||
|---|---|---|---|---|
| Age (years) | 40.33 ± 9.09 | 40.62 ± 0.16 | ||
| Gender Women | 21 | Percentage% 51.21 | 20 | Percentage% 48.78 |
| Men | 17 | 56.66 | 13 | 43.34 |
| Environment Urban | 27 | 38.02 | 12 | 61.98 |
| Rural | 22 | 30.98 | 10 | 69.01 |
| Descriptives Statistics t-Test | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Ozonated Olive Oil Group 1 | N | Mean | Std. Deviation | SEM | 95% Confidence Interval for Mean | ||||
| Lower Bound | Upper Bound | T | p Value | Df | |||||
| FMPS 0 | 31 | 112.10700 | 150.06167 | 33.55481 | 22.90983 | 159.50017 | 2.7035 | 0.0102 | 58 |
| FMPS 1 | 31 | 20.90200 | 15.62014 | 3.49277 | |||||
| FMBS 0 | 31 | 40.59100 | 17.84195 | 3.25748 | 20.12495 | 34.28505 | 7.6916 | 0.0001 | 58 |
| FMBS 1 | 31 | 13.38600 | 7.54811 | 1.37809 | |||||
| GI 0 | 31 | 1.3094 | 0.3028 | 0.0535 | 0.3119 | 0.6040 | 6.2758 | 0.0001 | 58 |
| GI 1 | 31 | 0.8514 | 0.2560 | 0.0484 | |||||
| Descriptives Statistics t-Test | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Olive Oil Group 2 | N | Mean | Std. Deviation | SEM | 95% Confidence Interval for Mean | ||||
| Lower Bound | Upper Bound | T | p Value | Df | |||||
| FMPS0 | 30 | 150.96484 | 282.59950 | 50.75637 | 19.96657 | 119.9935 | 2.3988 | 0.0195 | 61 |
| FMPS1 | 30 | 30.97125 | 15.65427 | 2.76731 | |||||
| FMBS 0 | 30 | 37.24516 | 20.18458 | 3.62526 | 6.27238 | 24.69601 | 3.3623 | 0.0014 | 60 |
| FMBS 1 | 30 | 21.76097 | 15.81244 | 2.84000 | |||||
| GI 0 | 30 | 1.3260 | 0.2796 | 0.0510 | 0.1002 | 0.3658 | 3.5128 | 0.0009 | 58 |
| GI 1 | 30 | 1.0930 | 0.2320 | 0.0424 | |||||
| Comparing Scores between Group 1 and Group 2 V0-V1 | T | Df | Sig. | Mean Difference | 95% Confidence Interval for Mean | |
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| FMPS | 0.5625 | 59 | 0.005 | −0.01800 | −0.08206 | 0.04606 |
| FMBS | 7.4371 | 59 | 0.0001 | 0.27200 | 0.19882 | 0.34518 |
| GI | 3.2860 | 59 | 0.0017 | −0.21700 | −0.34914 | −0.08486 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feier, R.; Sireteanu Cucui, R.M.; Ratiu, R.F.; Baciu, D.; Galea, C.; Sachelarie, L.; Nistor, C.; Cocos, D.; Hurjui, L.L.; Cernei, E.R. Comparative Study of Ozonated Olive Oil and Extra Virgin Olive Oil Effects on Oral Hygiene. Appl. Sci. 2023, 13, 2831. https://doi.org/10.3390/app13052831
Feier R, Sireteanu Cucui RM, Ratiu RF, Baciu D, Galea C, Sachelarie L, Nistor C, Cocos D, Hurjui LL, Cernei ER. Comparative Study of Ozonated Olive Oil and Extra Virgin Olive Oil Effects on Oral Hygiene. Applied Sciences. 2023; 13(5):2831. https://doi.org/10.3390/app13052831
Chicago/Turabian StyleFeier, Ramona, Radu Mircea Sireteanu Cucui, Ramona Flavia Ratiu, Dana Baciu, Carmen Galea, Liliana Sachelarie, Claudia Nistor, Dorin Cocos, Loredana Liliana Hurjui, and Eduard Radu Cernei. 2023. "Comparative Study of Ozonated Olive Oil and Extra Virgin Olive Oil Effects on Oral Hygiene" Applied Sciences 13, no. 5: 2831. https://doi.org/10.3390/app13052831