
Online Audio-Visual Information on the Treatment of OSA with Mandibular Advancement Devices: Analysis of Quality, Reliability and Contents


 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Video Search Strategy
2.2. Video Metrics Analysis
2.3. Video Sources and Target Audience
2.4. Assessment of Video Quality and Reliability
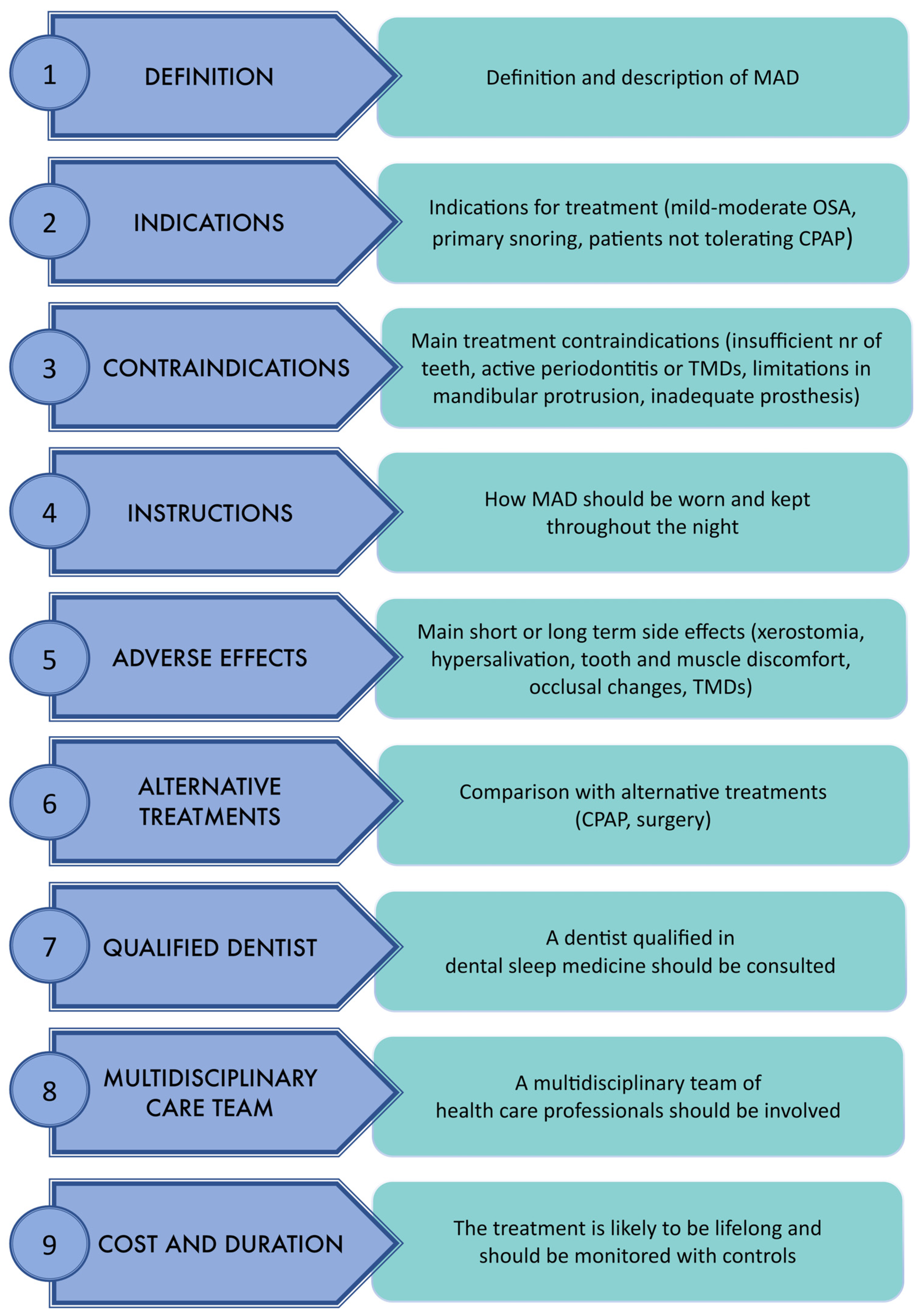
2.5. Video Content Analysis
2.6. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Source of Upload and Target Audience
3.3. Quality, Reliability and Content
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- US Preventive Services Task Force; Bibbins-Domingo, K.; Grossman, D.C.; Curry, S.J.; Davidson, K.W.; Epling, J.W.; García, F.A.R.; Herzstein, J.; Kemper, A.R.; Krist, A.H.; et al. Screening for Obstructive Sleep Apnea in Adults: US Preventive Services Task Force Recommendation Statement. JAMA 2017, 317, 407. [Google Scholar] [CrossRef] [PubMed]
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; Heinzer, R.; Ip, M.S.M.; Morrell, M.J.; Nunez, C.M.; Patel, S.R.; Penzel, T.; Pépin, J.-L.; et al. Estimation of the Global Prevalence and Burden of Obstructive Sleep Apnoea: A Literature-Based Analysis. Lancet Respir. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef] [PubMed]
- Lyons, M.M.; Bhatt, N.Y.; Pack, A.I.; Magalang, U.J. Global Burden of Sleep-disordered Breathing and Its Implications. Respirology 2020, 25, 690–702. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, M.; Acosta, L.; Hung, Y.-L.; Padilla, M.; Enciso, R. Effects of CPAP and Mandibular Advancement Device Treatment in Obstructive Sleep Apnea Patients: A Systematic Review and Meta-Analysis. Sleep Breath. 2018, 22, 555–568. [Google Scholar] [CrossRef] [PubMed]
- Mogell, K.; Blumenstock, N.; Mason, E.; Rohatgi, R.; Shah, S.; Schwartz, D. Definition of an Effective Oral Appliance for the Treatment of Obstructive Sleep Apnea and Snoring: An Update for 2019. J. Dent. Sleep Med. 2019, 6, 3. [Google Scholar] [CrossRef]
- Bosi, M.; Incerti Parenti, S.; Sanna, A.; Plazzi, G.; De Vito, A.; Alessandri-Bonetti, G. Non-Continuous Positive Airway Pressure Treatment Options in Obstructive Sleep Apnoea: A Pathophysiological Perspective. Sleep Med. Rev. 2021, 60, 101521. [Google Scholar] [CrossRef]
- Sia, C.-H.; Hong, Y.; Tan, L.W.L.; van Dam, R.M.; Lee, C.-H.; Tan, A. Awareness and Knowledge of Obstructive Sleep Apnea among the General Population. Sleep Med. 2017, 36, 10–17. [Google Scholar] [CrossRef]
- Osman, W.; Mohamed, F.; Elhassan, M.; Shoufan, A. Is YouTube a Reliable Source of Health-Related Information? A Systematic Review. BMC Med. Educ. 2022, 22, 382. [Google Scholar] [CrossRef]
- Datareportal YouTube Statistics and Trends. Available online: https://datareportal.com/essential-youtube-stats (accessed on 27 February 2023).
- Oberlo. 10 Statistiche YouTube Fondamentali per il 2022. Available online: https://www.oberlo.it/blog/statistiche-youtube#:~:text=Secondo%20le%20statistiche%20YouTube%20pi%C3%B9,tuoi%20sforzi%20di%20digital%20marketing (accessed on 27 February 2023).
- Culha, Y.; Culha, M.G.; Acaroglu, R. Evaluation of YouTube Videos Regarding Clean Intermittent Catheterization Application. Int. Neurourol. J. 2020, 24, 286–292. [Google Scholar] [CrossRef]
- Drozd, B.; Couvillon, E.; Suarez, A. Medical YouTube Videos and Methods of Evaluation: Literature Review. JMIR Med. Educ. 2018, 4, e3. [Google Scholar] [CrossRef]
- ElKarmi, R.; Hassona, Y.; Taimeh, D.; Scully, C. YouTube as a Source for Parents’ Education on Early Childhood Caries. Int. J. Paediatr. Dent. 2017, 27, 437–443. [Google Scholar] [CrossRef]
- Abukaraky, A.; Hamdan, A.; Ameera, M.; Nasief, M.; Hassona, Y. Quality of YouTube TM Videos on Dental Implants. Med. Oral. 2018, 23, e463. [Google Scholar] [CrossRef]
- Hegarty, E.; Campbell, C.; Grammatopoulos, E.; DiBiase, A.T.; Sherriff, M.; Cobourne, M.T. YouTubeTM as an Information Resource for Orthognathic Surgery. J. Orthod. 2017, 44, 90–96. [Google Scholar] [CrossRef]
- Sezici, Y.L.; Gediz, M.; Dindaroğlu, F. Is YouTube an Adequate Patient Resource about Orthodontic Retention? A Cross-Sectional Analysis of Content and Quality. Am. J. Orthod. Dentofac. Orthop. 2022, 161, e72–e79. [Google Scholar] [CrossRef] [PubMed]
- Kodonas, K.; Fardi, A. YouTube as a Source of Information about Pulpotomy and Pulp Capping: A Cross Sectional Reliability Analysis. Restor. Dent. Endod. 2021, 46, e40. [Google Scholar] [CrossRef] [PubMed]
- Hatipoğlu, Ş.; Gaş, S. Is Information for Surgically Assisted Rapid Palatal Expansion Available on YouTube Reliable? J. Oral. Maxillofac. Surg. 2020, 78, 1017.e1–1017.e10. [Google Scholar] [CrossRef] [PubMed]
- Incerti Parenti, S.; Gamberini, S.; Fiordelli, A.; Bortolotti, F.; Laffranchi, L.; Alessandri-Bonetti, G. Online Information on Mandibular Advancement Device for the Treatment of Obstructive Sleep Apnea: A Content, Quality and Readability Analysis. J. Oral. Rehabil. 2023, 50, 210–216. [Google Scholar] [CrossRef]
- Desai, T.; Shariff, A.; Dhingra, V.; Minhas, D.; Eure, M.; Kats, M. Is Content Really King? An Objective Analysis of the Public’s Response to Medical Videos on YouTube. PLoS ONE 2013, 8, e82469. [Google Scholar] [CrossRef]
- Lena, Y.; Dindaroğlu, F. Lingual Orthodontic Treatment: A YouTubeTM Video Analysis. Angle Orthod. 2018, 88, 208–214. [Google Scholar] [CrossRef]
- Nason, K.; Donnelly, A.; Duncan, H.F. YouTube as a Patient-Information Source for Root Canal Treatment. Int. Endod. J. 2016, 49, 1194–1200. [Google Scholar] [CrossRef]
- Hassona, Y.; Taimeh, D.; Marahleh, A.; Scully, C. YouTube as a Source of Information on Mouth (Oral) Cancer. Oral. Dis. 2016, 22, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Yavan, M.A.; Gökçe, G. YouTube as a Source of Information on Adult Orthodontics: A Video Analysis Study. J. World Fed. Orthod. 2022, 11, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Nagpal, S.J.S.; Karimianpour, A.; Mukhija, D.; Mohan, D.; Brateanu, A. YouTube Videos as a Source of Medical Information during the Ebola Hemorrhagic Fever Epidemic. SpringerPlus 2015, 4, 457. [Google Scholar] [CrossRef]
- Ozdede, M.; Peker, I. Analysis of Dentistry YouTube Videos Related To COVID-19. Braz. Dent. J. 2020, 31, 392–398. [Google Scholar] [CrossRef]
- Singh, A.G.; Singh, S.; Singh, P.P. YouTube for Information on Rheumatoid Arthritis—A Wakeup Call? J. Rheumatol. 2012, 39, 899–903. [Google Scholar] [CrossRef]
- Silberg, W.M. Assessing, Controlling, and Assuring the Quality of Medical Information on the Internet: Caveant Lector et Viewor—Let the Reader and Viewer Beware. JAMA 1997, 277, 1244. [Google Scholar] [CrossRef]
- Radonjic, A.; Fat Hing, N.N.; Harlock, J.; Naji, F. YouTube as a Source of Patient Information for Abdominal Aortic Aneurysms. J. Vasc. Surg. 2020, 71, 637–644. [Google Scholar] [CrossRef]
- Charnock, D.; Shepperd, S.; Needham, G.; Gann, R. DISCERN: An Instrument for Judging the Quality of Written Consumer Health Information on Treatment Choices. J. Epidemiol. Community Health 1999, 53, 105–111. [Google Scholar] [CrossRef]
- Fox, S. Health topics. Pew Internet and American Life Project. 2011. Available online: http://pewinternet.org/Reports/2011/HealthTopics.aspx (accessed on 1 March 2023).
- Fox, S.; Rainie, L. The Online Health Care Revolution: How the Web Helps Americans Take Better Care of Themselves: Pew Charitable Trusts: Washington, DC, USA. 2000. Available online: https://www.pewresearch.org/internet/2000/11/26/the-online-health-care-revolution/ (accessed on 1 March 2023).
- Why Is Audiovisual Media Considered a Powerful Tool and Means of Communication? By David Weedmark. Available online: https://smallbusiness.chron.com/audiovisual-media-considered-powerful-tool-means-communication-33541.html (accessed on 1 March 2023).
- Al-Silwadi, F.M.; Gill, D.S.; Petrie, A.; Cunningham, S.J. Effect of Social Media in Improving Knowledge among Patients Having Fixed Appliance Orthodontic Treatment: A Single-Center Randomized Controlled Trial. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 231–237. [Google Scholar] [CrossRef]
- Boyer, C.; Gaudinat, A.; Hanbury, A.; Appel, R.D.; Ball, M.J.; Carpentier, M.; van Bemmel, J.H.; Bergmans, J.-P.; Hochstrasser, D.; Lindberg, D.; et al. Accessing Reliable Health Information on the Web: A Review of the HON Approach. Precis. Healthc. Through Inform. 2017, 245, 1004–1008. [Google Scholar]
- Bezner, S.K.; Hodgman, E.I.; Diesen, D.L.; Clayton, J.T.; Minkes, R.K.; Langer, J.C.; Chen, L.E. Pediatric Surgery on YouTubeTM: Is the Truth out There? J. Pediatr. Surg. 2014, 49, 586–589. [Google Scholar] [CrossRef]
- Etzel, C.M.; Bokshan, S.L.; Forster, T.A.; Owens, B.D. A Quality Assessment of YouTube Content on Shoulder Instability. Physician Sportsmed. 2022, 50, 289–294. [Google Scholar] [CrossRef]
- Leong, A.Y.; Sanghera, R.; Jhajj, J.; Desai, N.; Jammu, B.S.; Makowsky, M.J. Is YouTube Useful as a Source of Health Information for Adults with Type 2 Diabetes? A South Asian Perspective. Can. J. Diabetes 2018, 42, 395–403.e4. [Google Scholar] [CrossRef] [PubMed]
- Kazi, M.R.; Rumana, N.; Al Mamun, M.; Abedin, T.; Lasker, M.A.A.; Ahmed, S.W.; Turin, T.C. YouTube as a Source of Educational Information about CPAP Use for Sleep Apnea. J. Commun. Healthc. 2020, 13, 284–288. [Google Scholar] [CrossRef]
- Wu, V.; Lee, D.J.; Vescan, A.; Lee, J.M. Evaluating YouTube as a Source of Patient Information for Functional Endoscopic Sinus Surgery. Ear Nose Throat J. 2022, 101, 396–401. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Dental Sleep Medicine. Practice Guidelines for Dental Sleep Medicine. Available online: https://www.aadsm.org/guidelines.php (accessed on 2 March 2023).
- Incerti Parenti, S.; Bortolotti, F.; Alessandri-Bonetti, G. Oral Appliances for Obstructive Sleep Apnea. J. World Fed. Orthod. 2019, 8, 3–8. [Google Scholar] [CrossRef]
- Alessandri-Bonetti, G.; D’Antò, V.; Stipa, C.; Rongo, R.; Incerti-Parenti, S.; Michelotti, A. Dentoskeletal Effects of Oral Appliance Wear in Obstructive Sleep Apnoea and Snoring Patients. Eur. J. Orthod. 2016, 39, cjw078. [Google Scholar] [CrossRef] [PubMed]
- Bartolucci, M.L.; Bortolotti, F.; Martina, S.; Corazza, G.; Michelotti, A.; Alessandri-Bonetti, G. Dental and Skeletal Long-Term Side Effects of Mandibular Advancement Devices in Obstructive Sleep Apnea Patients: A Systematic Review with Meta-Regression Analysis. Eur. J. Orthod. 2019, 41, 89–100. [Google Scholar] [CrossRef]
- Ramar, K.; Dort, L.C.; Katz, S.G.; Lettieri, C.J.; Harrod, C.G.; Thomas, S.M.; Chervin, R.D. Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring with Oral Appliance Therapy: An Update for 2015: An American Academy of Sleep Medicine and American Academy of Dental Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep. Med. 2015, 11, 773–827. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Video Metrics | Mean | SD |
|---|---|---|
| Video length (min) | 4.64 | 2.59 |
| Number of views | 34,149.21 | 132,175.72 |
| Number of likes | 701.56 | 4369.44 |
| Number of dislikes | 0 | 0 |
| Number of comments | 45.71 | 190.31 |
| Interaction Index | 35.06 | 266.55 |
| Video Power Index | 34.73 | 165.76 |
| Source of Upload | VIQI | m-DISCERN | JAMA | Content | ||||
|---|---|---|---|---|---|---|---|---|
| Mean | 95%CI | Mean | 95%CI | Mean | 95%CI | Mean | 95%CI | |
| Healthcare professionals | 12.38 | 11.28–13.47 | 2.13 | 1.73–2.52 | 1.90 | 1.62–2.19 | 3.25 | 2.66–3.84 |
| Hospital/University | 13.00 | 11.70–14.30 | 3.00 | 1.70–4.30 | 2.25 | 0.25–4.25 | 2.75 | 0.75–4.75 |
| Commercial | 11.21 | 9.61–12.81 | 1.43 | 1.13–1.73 | 2.07 | 1.80–2.35 | 2.36 | 1.66–3.06 |
| Laypeople | 7.92 | 5.90–9.95 | 1.15 | 0.93–1.40 | 1.54 | 1.22–1.85 | 1.54 | 0.60–2.48 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Incerti-Parenti, S.; Bartolucci, M.L.; Biondi, E.; Fiordelli, A.; Paganelli, C.; Alessandri-Bonetti, G. Online Audio-Visual Information on the Treatment of OSA with Mandibular Advancement Devices: Analysis of Quality, Reliability and Contents. Appl. Sci. 2023, 13, 5727. https://doi.org/10.3390/app13095727
Incerti-Parenti S, Bartolucci ML, Biondi E, Fiordelli A, Paganelli C, Alessandri-Bonetti G. Online Audio-Visual Information on the Treatment of OSA with Mandibular Advancement Devices: Analysis of Quality, Reliability and Contents. Applied Sciences. 2023; 13(9):5727. https://doi.org/10.3390/app13095727
Chicago/Turabian StyleIncerti-Parenti, Serena, Maria Lavinia Bartolucci, Elena Biondi, Andrea Fiordelli, Corrado Paganelli, and Giulio Alessandri-Bonetti. 2023. "Online Audio-Visual Information on the Treatment of OSA with Mandibular Advancement Devices: Analysis of Quality, Reliability and Contents" Applied Sciences 13, no. 9: 5727. https://doi.org/10.3390/app13095727