
The Impact of Systemic Simvastatin on Bone Remodeling Following Rapid Maxillary Expansion: An In Vivo Study
 , ,
, ,  , ,
, ,  , and
, and
Abstract
:1. Introduction
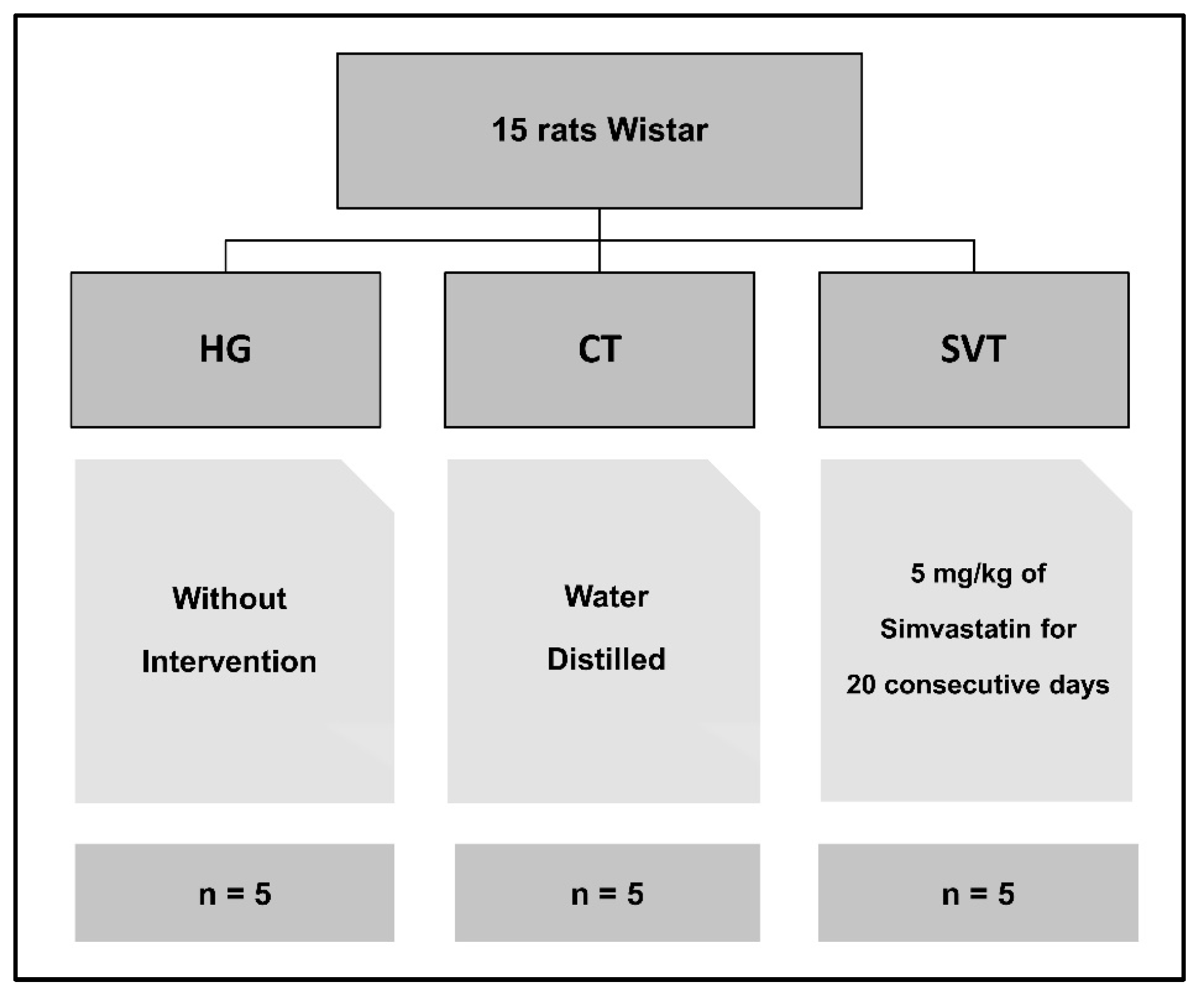
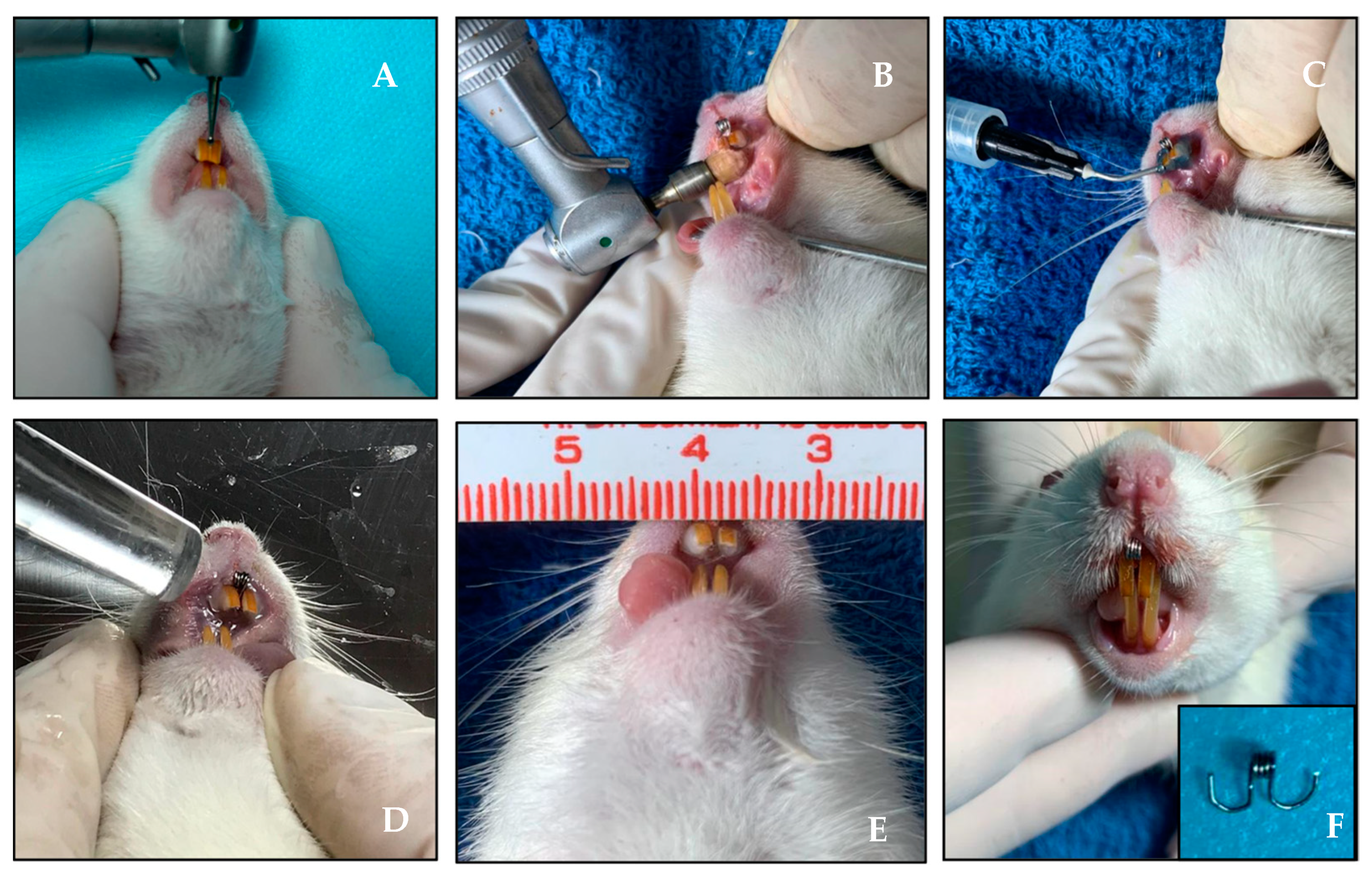
2. Materials and Methods
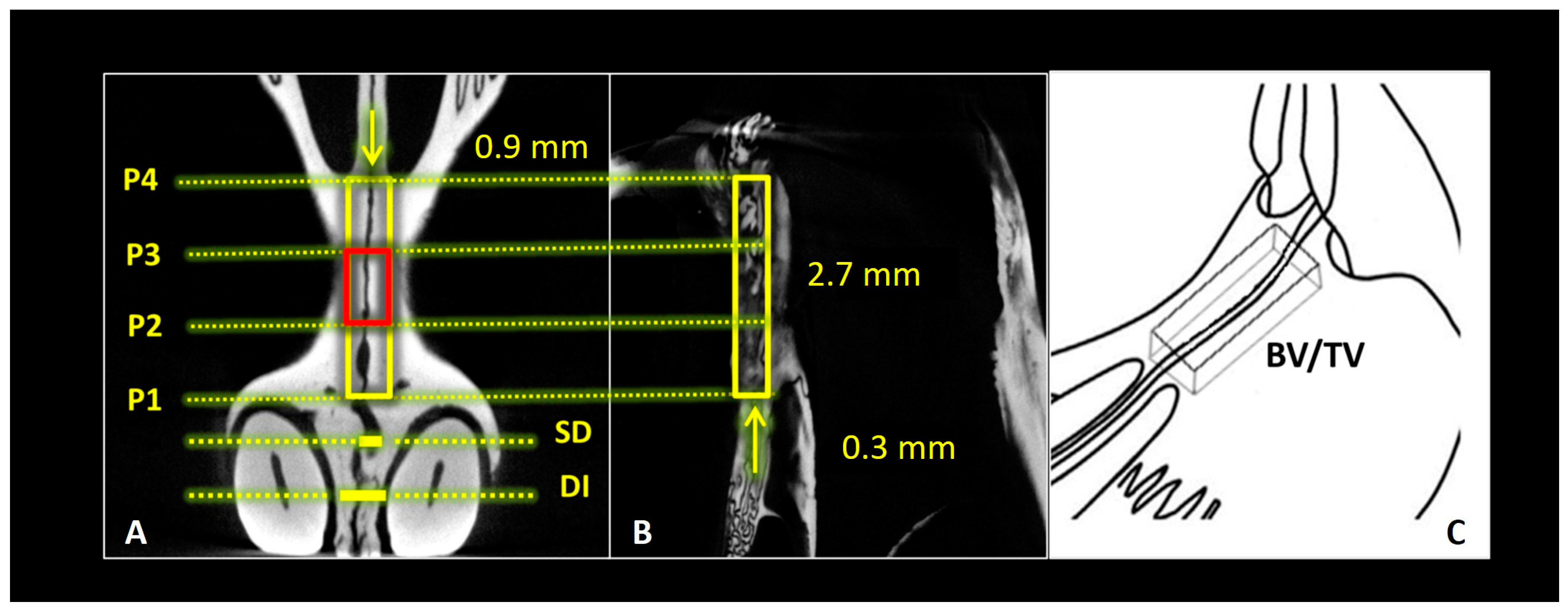
2.1. Micro-Computed Tomography
2.2. Histology and Histomorphometry
2.3. Statistical Analysis
3. Results
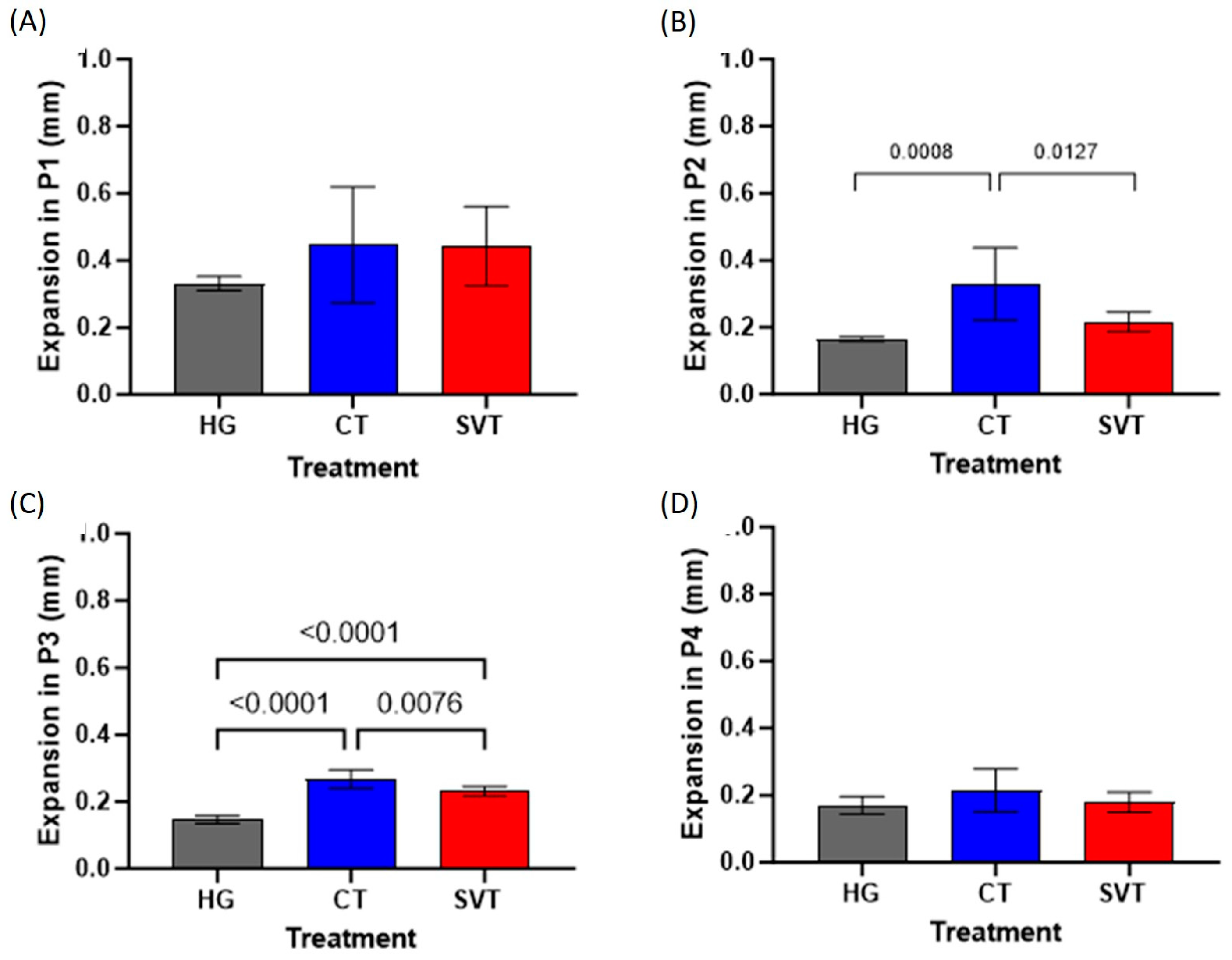
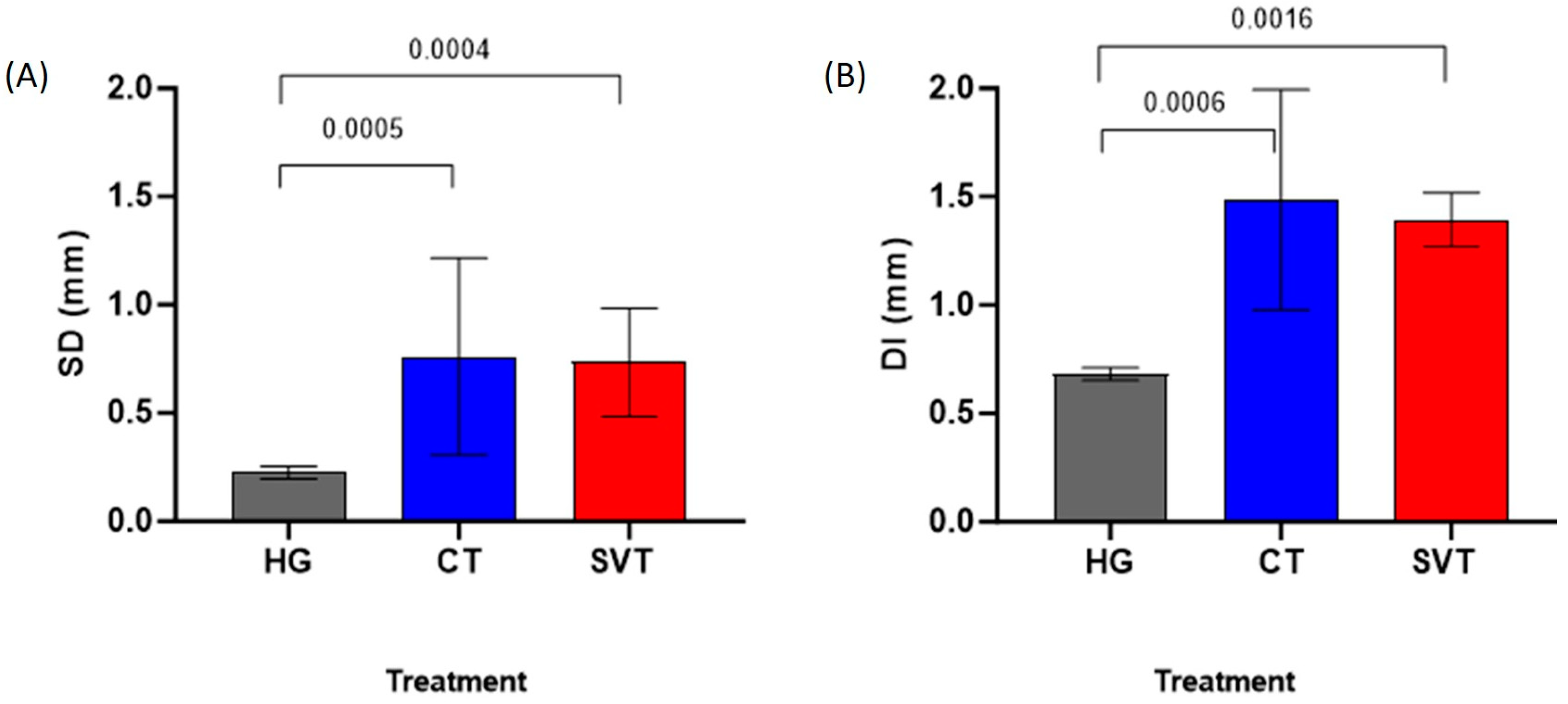
3.1. Palatine Suture Measurements
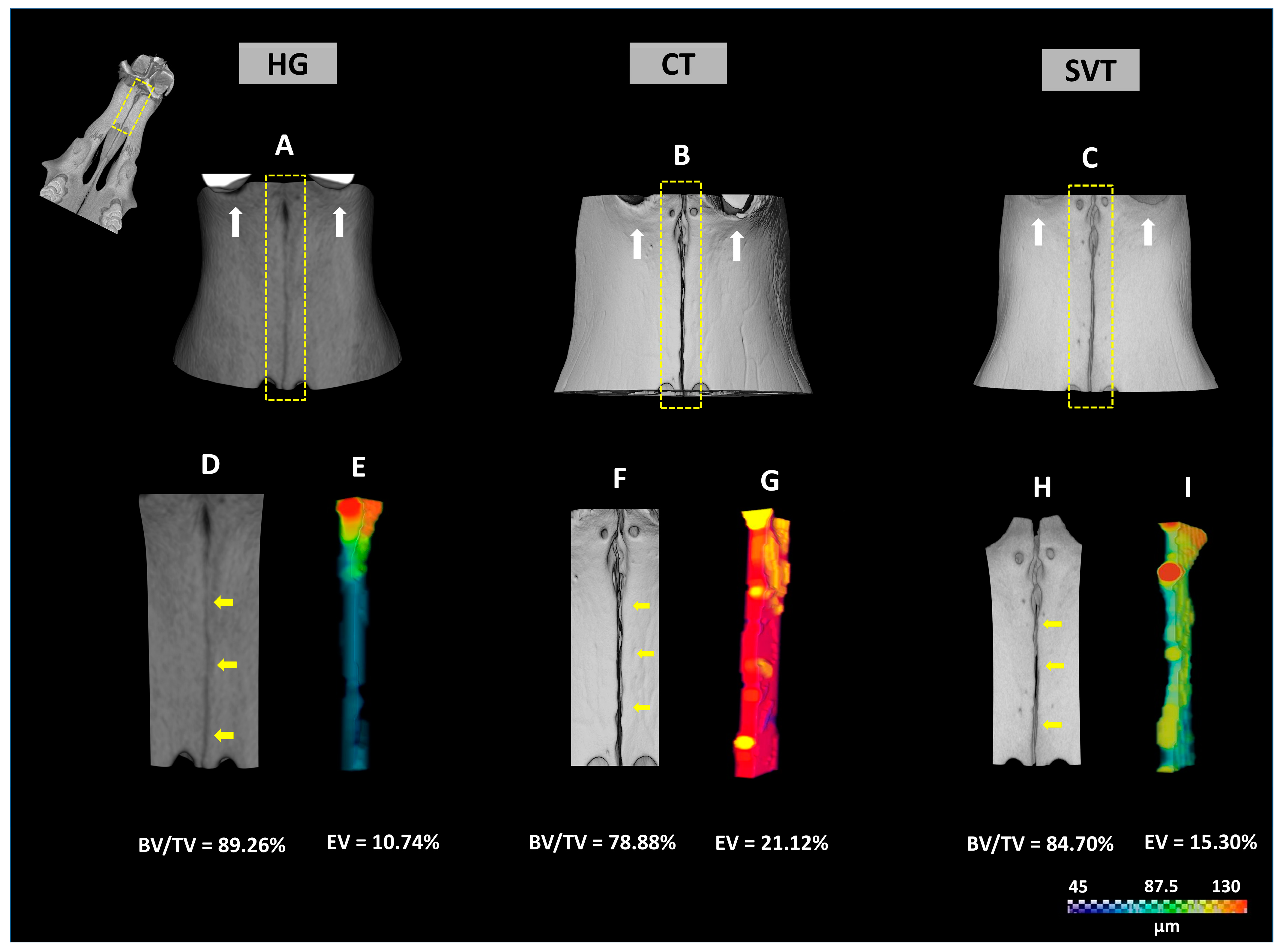
3.2. Three-Dimensional µCT Images Segmentation
3.3. Microtomographic Parameters
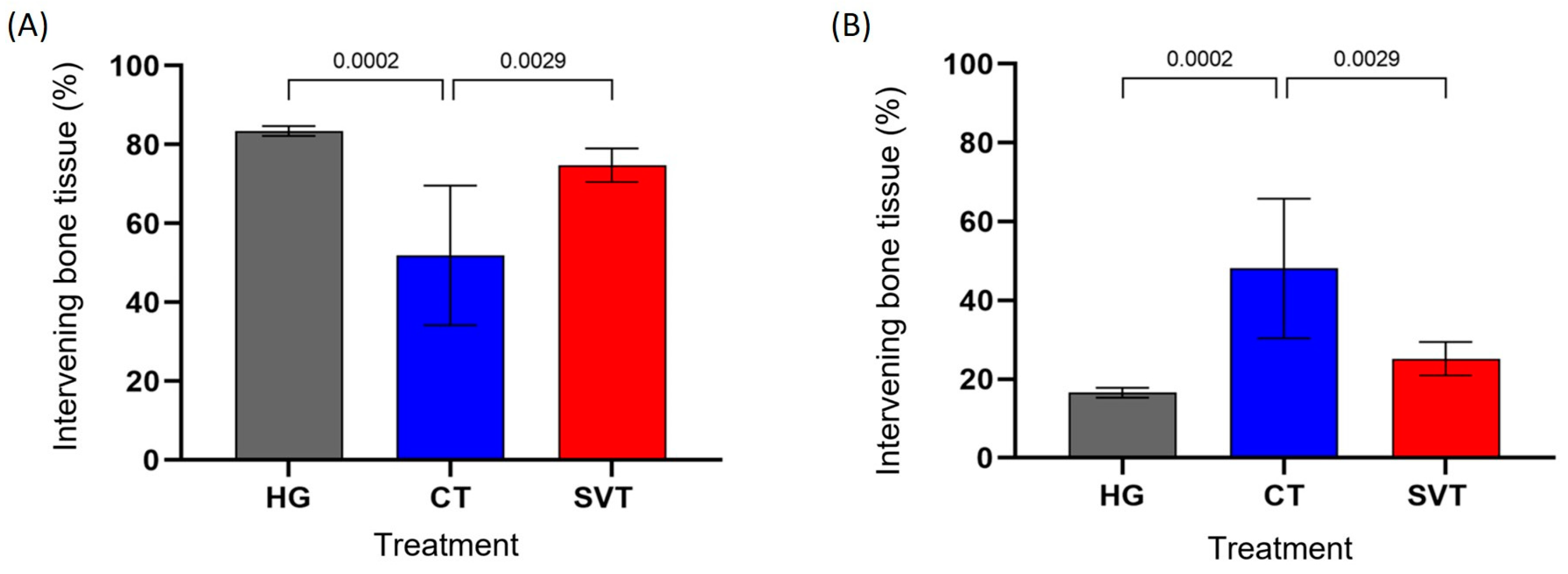
3.4. Histomorphometric Results
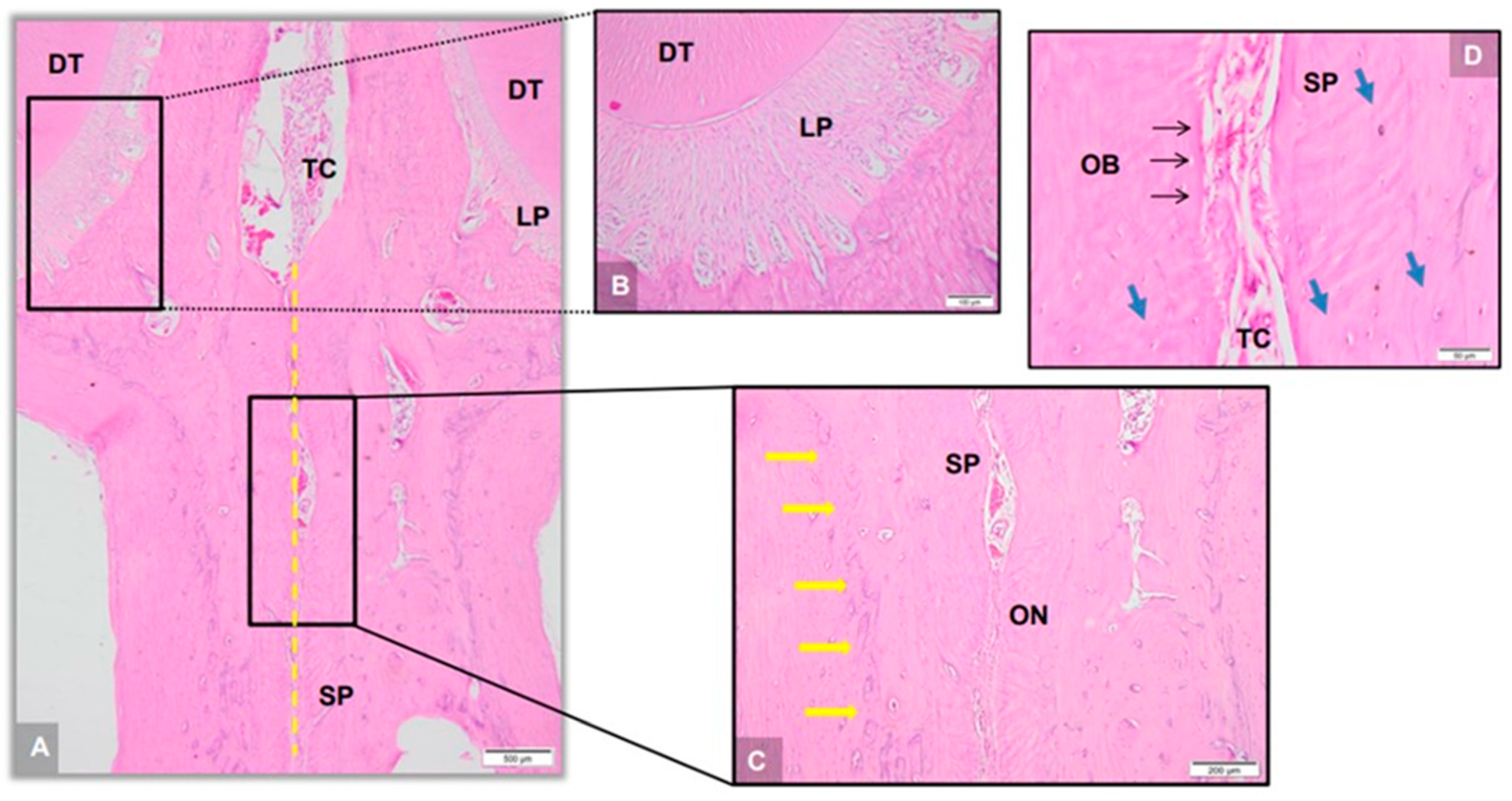
3.5. Descriptive Histology and Histomorphometry
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- da Luz Baratieri, C.; Alves, M., Jr.; Mattos, C.T.; Lau, G.W.; Nojima, L.I.; de Souza, M.M. Trans verse effects on the nasomaxillary complex one year after rapid maxillary expansion as the only intervention: A controlled study. Dent. Press J. Orthod. 2014, 19, 79–87. [Google Scholar] [CrossRef] [PubMed]
- de Julián-López, C.; Veres, J.; Marqués-Martínez, L.; García-Miralles, E.; Arias, S.; Guinot-Barona, C. Upper airway changes after rapid maxillary expansion: Three-dimensional analyses. BMC Oral Health 2023, 23, 618. [Google Scholar] [CrossRef] [PubMed]
- Fastuca Ry Colaboradores. Airway compartments volumen and oxygen saturation changes after rapid maxillary expansion: A longitudinal correlation study. Angle Orthod. 2015, 6, 955–961. [Google Scholar]
- Lima Filho, R.M.A.; Ruellas, A.C.O. Long-term maxillary changes in patients with skeletal Class II malocclusion treated with slow and rapid palatal expansion. Am. J. Orthod. Dentofac. Orthop. 2008, 134, 383–388. [Google Scholar] [CrossRef] [PubMed]
- de Almeida, A.M.; Ozawa, T.O.; Alves, A.C.M.; Janson, G.; Lauris, J.R.P.; Ioshida, M.S.Y.; Gari, D.G. Slow versus rapid maxillary expansion in bilateral cleft lip and palate: A CBCT randomized clinical trial. Clin. Oral Investig. 2017, 21, 1789–1799. [Google Scholar] [CrossRef] [PubMed]
- Gill, D.; Naini, F.; Mcnally, M.; Jones, A. The Management of Transverse Maxillary Deficiency. Dent. Update 2004, 31, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Golpasandhagh, L.; Samie, N.; Sabiza, S.; Rezaie, A. Histopathological evaluation of the effect of melatonin gel on bone regeneration in rat model. J. Indian Soc. Periodontol. 2023, 27, 368–373. [Google Scholar] [CrossRef]
- Bhattarai, G.; Poudel, S.B.; Kook, S.H.; Lee, J.C. Resveratrol prevents alveolar bone loss in an experimental rat model of periodontitis. Acta Biomater. 2016, 29, 398–408. [Google Scholar] [CrossRef]
- Ozec, I.; Kilic, E.; Gumus, C.; Goze, F. Effect of local simvastatin application on mandibular defects. J. Craniofac. Surg. 2007, 18, 546–550. [Google Scholar] [CrossRef]
- Giroux, L.M.; Davignon, J.; Naruszewicz, M. Simvastatin inhibits the oxidation of low-density lipoproteins by activated human monocyte-derived macrophages. Biochim. Biophys. Acta 1993, 1165, 335–338. [Google Scholar] [CrossRef]
- Davignon, J.; Laaksonen, R. Low-density lipoprotein-independent effects of statins. Curr. Opin. Lipidol. 1999, 10, 543–559. [Google Scholar] [CrossRef] [PubMed]
- Jain, M.K.; Ridker, P.M. Anti-inflammatory effects of statins: Clinical evidence and basic mechanisms. Nat. Rev. Drug Discov. 2005, 4, 977–987. [Google Scholar] [CrossRef] [PubMed]
- Han, G.; Chen, Y.; Hou, J.; Liu, C.; Chen, C.; Zhuang, J.; Meng, W. Effects of simvastatin on relapse and remodeling of periodontal tissues after tooth movement in rats. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 550.e1–550.e7. [Google Scholar] [CrossRef]
- Mundy, G.; Garret, R.; Harris, S.; Chan, J.; Chen, D.; Rossini, G.; Boyce, B.; Zhao, M.; Gutierrez, G. Stimulation of bone formation in vitro and in rodents by statins. Science 1999, 286, 1946–1949. [Google Scholar] [CrossRef] [PubMed]
- Vasconcelos, J.W.; Leite, L.M.S.; Vasconcelos, G.A.; Araujo, I.M.S.M.; Ferro, L.S.G. Evaluation of simvastatin in the process of fracture consolidation in rat tibias. Rev. Bras. Ortop. 2013, 48, 191–195. [Google Scholar] [CrossRef]
- Yasuda, H. Discovery of the RANKL/RANK/OPG system. J. Bone Miner. Metab. 2021, 39, 2–11, Erratum in J. Bone Miner. Metab. 2021, 39, 12. [Google Scholar] [CrossRef]
- Udagawa, N.; Koide, M.; Nakamura, M.; Nakamichi, Y.; Yamashita, T.; Uehara, S.; Kobayashi, Y.; Furuya, Y.; Yasuda, H.; Fukuda, C.; et al. Osteoclast differentiation by RANKL and OPG signaling pathways. J. Bone Min. Metab. 2021, 39, 19–26. [Google Scholar] [CrossRef]
- Liu, W.; Zhang, X. Receptor activator of nuclear factor-κB ligand (RANKL)/RANK/osteoprotegerin system in bone and other tissues (review). Mol. Med. Rep. 2015, 11, 3212–3218. [Google Scholar] [CrossRef]
- Maeda, T.; Kawane, T.; Horiuchi, N. Statins augment vascular endothelial growth factor expression in osteoblastic cells via inhibition of protein prenylation. Endocrinology 2003, 144, 681–692. [Google Scholar] [CrossRef]
- Arnez, M.F.M.; Ribeiro, L.S.N.; Barreto, G.D.; Monteiro, P.M.; Ervolino, E.; Stuani, M.B.S. RANK/RANKL/OPG Expression in Rapid Maxillary Expansion. Braz. Dent. J. 2017, 28, 296–300. [Google Scholar] [CrossRef]
- Sawada, M.; Shimizu, N. Stimulation of bone formation in the expanding mid-palatal suture by transforming growth factor-β1 in the rat. Eur. J. A/Orthod. 1996, 18, 169–179. [Google Scholar] [CrossRef]
- Saito, S.; Shimizu, N. Stimulatory effects of low-power bone regeneration in midpalatal expansion in the rat. Am. J. Orthod. Dentofac. Orthop. 1997, 111, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Sales, E.; Lima, I.; de Assis, J.T.; Gómez, W.; Pereira, W.C.; Lopes, R.T. Bone quality analysis using X-ray microtomography and microfluorescence. Appl. Radiat. Isot. 2012, 70, 1272–1276. [Google Scholar] [CrossRef] [PubMed]
- Andersen, M.L.; Costa, R.M.; Angelis, K.; Braga, L.M.G.M.; Souza, R.L.; Sebben, A.; Montenegro, M.M.V.; Silveira, L.F.; Nishioka, S.A.; Rodrigues, M.A.C.; et al. Normativas do CONCEA para a Produção, Manutenção ou Utilização Animal em atividades de Ensino ou Pesquisa Científica. Leis, Decretos, Portarias, Resoluções Normativas e Orientações técnicas. 3ª Edição. Brasília, 26 de Setembro de 2016. Available online: https://www.ceua.ufv.br/wp-content/uploads/2018/08/NORMATIVAS-DO-CONCEA-3%C2%AA-EDI%C3%87%C3%83O2.pdf (accessed on 15 March 2023).
- Kilkenny, C.; Brown, W.J.; Cuthill, I.C.; Emerson, M.; Altman, D.G. Improving bioscience research reporting: The ARRIVE guidelines for reporting animal research. Vet. Clin. Pathol. 2012, 41, 24–31. [Google Scholar] [CrossRef]
- Smith, A.J.; Clutton, R.E.; Lilley, E.; Hansen, K.E.A.; Brattelid, T. PREPARE: Guidelines for planning animal research and testing. Lab Anim. 2018, 52, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, J.R.B.; Sartoretto, S.C.; Alves, A.T.N.N.; Mourão, C.F.A.B.; Martinez-Zelaya, V.R.; Uzeda, M.J.; Granjeiro, J.M.; Montemezzi, P.; Calasans-Maia, M.D.; Calasans-Maia, J.A. In vitro In Vivo Evaluation of Nanostructured Biphasic Calcium Phosphate in Granules Putty Configurations. Int. J. Environ. Res. Public Health 2021, 18, 533. [Google Scholar] [CrossRef]
- Vieira, G.M.; Chaves, S.B.; Ferreira, V.M.M.; Freitas, K.M.S.; Amorim, R.F.B.V. The effect of simvastatin on relapse of tooth movement and bone mineral density in rats measured by a new method using microtomography. Acta Cirúrgica Bras. 2015, 30, 319–327. [Google Scholar] [CrossRef]
- Calasans-Maia, J.A.; Calasans-Maia, M.D.; Stuani, M.B.S.; Alves, A.T.N.N.; Montemezzi, P.; Mourão, C.F.A.B.; Cal-Neto, J.O.A.P.; Ruellas, A.C.O. In vivo biological evaluation of orthodontically moved incisors after replantation. Medicina 2020, 56, 421. [Google Scholar] [CrossRef]
- Bouxsein, M.L.; Boyd, S.K.; Christ, B.A.; Guldberg, R.E.; Jepsen, K.J.; Müller, R. Guidelines for assessment of bone microstructure in rodents using micro-computed tomography. J. Bone Miner. Res. 2010, 25, 1468–1486. [Google Scholar] [CrossRef]
- Doube, M.; Kłosowski, M.M.; Arganda-Carreras, I.; Cordelières, F.P.; Dougherty, R.P.; Jackson, J.S.; Schmid, B.; Hutchinson, J.R.; Shefelbine, S.J. BoneJ: Free extensible bone image analysis in ImageJ. Bone 2010, 47, 1076–1079. [Google Scholar] [CrossRef]
- Quinn, R.D.V.M. Comparing rat’s to human’s age: How old is my rat in people years? Editor. Opin./Nutr. 2005, 21, 775–777. [Google Scholar] [CrossRef] [PubMed]
- Storey, E. Tissue response to the movement of bones. Am. J. Orthod. 1973, 64, 229–247. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Yu, S.; Zhu, D.; Dai, L.; Yang, P.; Xing, X. Stimulatory effects of simvastatin on bone regeneration of the expanded suture in rats. Am. J. Transl. Res. 2020, 12, 1767–1778. [Google Scholar] [PubMed]
- Takenouchi, H.; Mayahara, K.; Arai, Y.; Karasawa, Y.; Shimizu, N. Longitudinal quantitative evaluation of the mid-palatal suture after rapid expansion using in vivo micro-CT. Arch. Oral Biol. 2014, 59, 414–423. [Google Scholar] [CrossRef] [PubMed]
- Chalisserrya, E.P.; Nama, S.Y.; Anilc, S. Simvastatin Loaded Nano Hydroxyapatite in Bone Regeneration: A Study in the Rabbit Femoral Condyle. Curr. Drug Deliv. 2019, 16, 530–537. [Google Scholar] [CrossRef]
- Mohamad, N.S.; Sinadinos, A.; Górecki, D.C.; Zioupos, P.; Tong, J. Impact of P2RX7 ablation on the morphological, mechanical and tissue properties of bones in a murine model of duchenne muscular dystrophy. J. Biomech. 2016, 49, 3444–3451. [Google Scholar] [CrossRef]
- Rocabado, J.M.R.; Kaku, M.; Nozaki, K.; Ida, K.; Kitami, M.; Aoyagi, Y.; Uoshima, K. A multi-factorial analysis of bone morphology and fracture strength of rat femur in response to ovariectomy. J. Orthop. Surg. Res. 2018, 13, 318. [Google Scholar] [CrossRef]
- Stechow, D.V.; Fish, S.; Yahalom, D.; Bab, I.; Chorev, M.; Müller, R.; Alexander, J.M. Does simvastatin stimulate bone formation in vivo? BMC Musculoskelet. Disord. 2003, 4, 8. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healthy | Control | Simvastatin | |
|---|---|---|---|
| BV | 0.649 ± 0.011 | 0.577 ± 0.020 | 0.616 ± 0.011 |
| TV | 0.728 | 0.728 | 0.728 |
| BV/TV | 0.892 ± 0.016 * | 0.788 ± 0.021 ** | 0.847 ± 0.017 *** |
| EV | 0.078 ± 0.011 | 0.150 ± 0.020 | 0.111 ± 0.011 |
| %BV/TV | 89.260 | 78.88 | 84.700 |
| Healthy | Control | Simvastatin | |
|---|---|---|---|
| Ct.Ar (mm2) | 0.735 ± 0.064 * | 0.686 ± 0.023 ** | 0.715 ± 0.006 |
| Ct.Ar/Tt.Ar(%) | 90.800 ± 0.774 * | 84.580 ± 2.511 ** | 88.040 ± 0.602 *** |
| Ct.Th (mm3) | 0.906 ± 0.044 * | 0.649 ± 0.009 ** | 0.818 ± 0.066 *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nascimento, J.R.B.; Lima, I.; Sartoretto, S.C.; Neves Novellino Alves, A.T.; Sorrentino de Freitas Farias dos Santos, C.M.; Lopes, R.T.; Javid, K.; Deylami, I.; Mourão, C.F.; Diuana Calasans-Maia, M.; et al. The Impact of Systemic Simvastatin on Bone Remodeling Following Rapid Maxillary Expansion: An In Vivo Study. Appl. Sci. 2024, 14, 430. https://doi.org/10.3390/app14010430
Nascimento JRB, Lima I, Sartoretto SC, Neves Novellino Alves AT, Sorrentino de Freitas Farias dos Santos CM, Lopes RT, Javid K, Deylami I, Mourão CF, Diuana Calasans-Maia M, et al. The Impact of Systemic Simvastatin on Bone Remodeling Following Rapid Maxillary Expansion: An In Vivo Study. Applied Sciences. 2024; 14(1):430. https://doi.org/10.3390/app14010430
Chicago/Turabian StyleNascimento, Jhonathan Raphaell Barros, Isabela Lima, Suelen Cristina Sartoretto, Adriana Terezinha Neves Novellino Alves, Caio Márcio Sorrentino de Freitas Farias dos Santos, Ricardo Tadeu Lopes, Kayvon Javid, Ilia Deylami, Carlos Fernando Mourão, Monica Diuana Calasans-Maia, and et al. 2024. "The Impact of Systemic Simvastatin on Bone Remodeling Following Rapid Maxillary Expansion: An In Vivo Study" Applied Sciences 14, no. 1: 430. https://doi.org/10.3390/app14010430