
A Systematic Review on Utilizing the Acute to Chronic Workload Ratio for Injury Prevention among Professional Soccer Players


Abstract
1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Literature Search Strategy
2.3. Study Selection
2.4. Data Extraction and Management
2.5. Quality Assessment of the Studies/Risk of Bias
3. Results
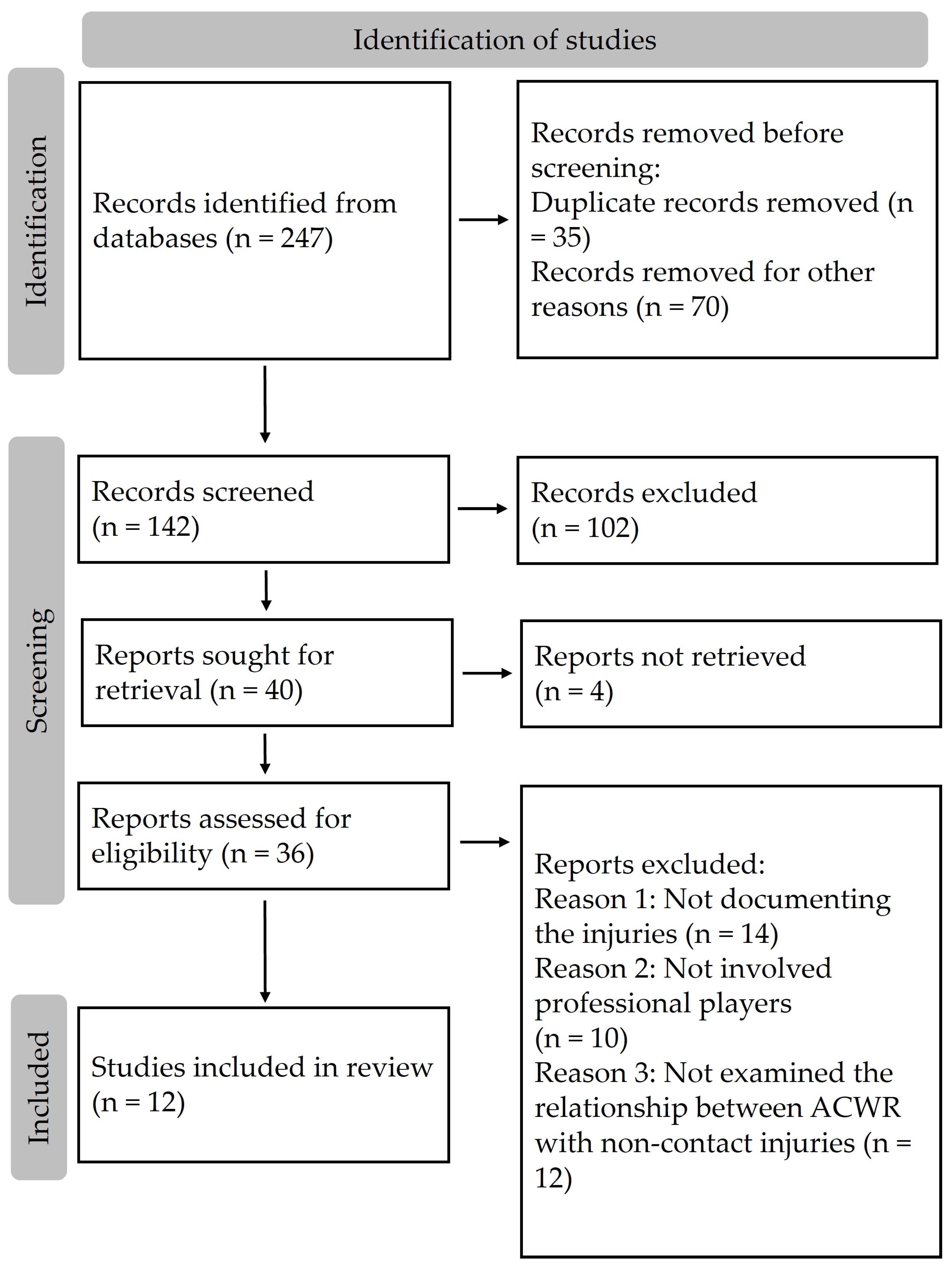
3.1. Selection of the Studies
3.2. Methodological Quality of the Studies
3.3. Characteristics of the Studies
4. Discussion
4.1. ACWR in Relation to RPE or External Variables
4.2. Most Important Variables for ACWR
4.3. Couple or Uncoupled ACWR
4.4. Duration of ACWR
4.5. Practical Applications
4.6. Study Limitations
5. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Professional FRootball. Available online: https://publications.fifa.com/en/annual-report-2021/around-fifa/professional-football-2021/ (accessed on 5 February 2024).
- Barnes, C.; Archer, D.T.; Hogg, B.; Bush, M.; Bradley, P.S. The evolution of physical and technical performance parameters in the English premier league. Int. J. Sports Med. 2014, 35, 1095–1100. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Gómez, M.Á.; Lorenzo, A. The evolution of physical and technical performance parameters in the Chinese Soccer Super League. Biol. Sport 2020, 37, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Nassis, G.P.; Massey, A.; Jacobsen, P.; Brito, J.; Randers, M.B.; Castagna, C.; Krustrup, P. Elite football of 2030 will not be the same as that of 2020: Preparing players, coaches, and support staff for the evolution. Scand. J. Med. Sci. Sports 2020, 3, 962–964. [Google Scholar] [CrossRef]
- Dupont, G.; Nedelec, M.; McCall, A.; McCormack, D.; Berthoin, S.; Wisløff, U. Effect of 2 soccer matches in a week on physical performance and injury rate. Am. J. Sports Med. 2010, 38, 1752–1758. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, J.; Hagglund, M.; Waldιn, M. Injury incidence and injury patterns in professional football: The UEFA injury study. Br. J. Sports Med. 2011, 45, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Pulici, L.; Certa, D.; Zago, M.; Volpi, P.; Esposito, F. Injury Burden in Professional European Football (Soccer): Systematic Review, Meta-Analysis, and Economic Considerations. Clin. J. Sport Med. 2023, 33, 450–457. [Google Scholar] [CrossRef]
- Howden’s European Football Injury Index Reveals Record Injury Cost of Over £500m for 2021/22 Season. Available online: https://www.howdengroup.com/news-and-insights/howdens-european-footbal-Injury-Index-reveals-record-injury-cost-of-over-500m-for-2021-22-season (accessed on 6 February 2024).
- Hägglund, M.; Waldén, M.; Magnusson, H.; Kristenson, K.; Bengtsson, H.; Ekstrand, J. Injuries affect team performance negatively in professional football: An 11-year follow-up of the UEFA Champions League injury study. Br. J. Sports Med. 2013, 47, 738–742. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, J.; Walden, M.; Hagglund, M. Hamstring injuries have increased by 4% annually in men’s professional football, since 2001: A 13-year longitudinal analysis of the UEFA Elite Club injury study. Br. J. Sports Med. 2016, 50, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Gabbett, T.J. The training-injury prevention paradox: Should athletes be training smarter and harder? Br. J. Sports Med. 2016, 50, 273–280. [Google Scholar] [CrossRef]
- Fousekis, A.; Fousekis, K.; Fousekis, G.; Vaitsis, N.; Terzidis, I.; Christoulas, K.; Michailidis, Y.; Mandroukas, A.; Metaxas, T. Two or Four Weeks Acute: Chronic Workload Ratio Is More Useful to Prevent Injuries in Soccer? Appl. Sci. 2023, 13, 495. [Google Scholar] [CrossRef]
- Scott, T.J.; Black, C.R.; Quinn, J.; Coutts, A.J. Validity and reliability of the session-RPE method for quantifying training in Australian football: A comparison of the CR10 and CR100 scales. J. Strength Cond. Res. 2013, 27, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Fortunati, M.; Soldini, E.; Piccoli, M.; Lakicevic, N.; Crisafulli, O.; Drid, P.; Gemeli, T.; D’antona, G. Heart rate response and contextual variables in professional rink hockey competitions. Med. Dello Sport 2023, 76, 44–57. [Google Scholar] [CrossRef]
- Hulin, B.T.; Gabbett, T.J.; Lawson, D.W.; Caputi, P.; Sampson, J.A. The acute:chronic workload ratio predicts injury: High chronic workload may decrease injury risk in elite rugby league players. Br. J. Sports Med. 2016, 50, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Blanch, P.; Gabbett, T.J. Has the athlete trained enough to return to play safely? The acute:chronic workload ratio permits clinicians to quantify a player’s risk of subsequent injury. Br. J. Sports Med. 2016, 50, 471–475. [Google Scholar] [CrossRef]
- Murray, N.B.; Gabbett, T.J.; Townshend, A.D.; Blanch, P. Calculating acute:chronic workload ratios using exponentially weighted moving averages provides a more sensitive indicator of injury likelihood than rolling averages. Br. J. Sports Med. 2017, 51, 749–754. [Google Scholar] [CrossRef] [PubMed]
- Bowen, L.; Gross, A.S. Accumulated workloads and the acute: Chronic workload ratio relate to injury risk in elite youth football players. Br. J. Sports Med. 2017, 51, 452–459. [Google Scholar] [CrossRef]
- Jaspers, A.; Kuyvenhoven, J.P. Examination of the external and internal load indicators’ association with overuse injuries in professional soccer players. J. Sci. Med. Sport 2018, 21, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Esmaeili, A.; Hopkins, W.G. The individual and combined effects of multiple factors on the risk of soft tissue non-contact injuries in elite team sport athletes. Front. Physiol. 2018, 9, 1280. [Google Scholar] [CrossRef] [PubMed]
- Delecroix, B.; McCall, A. Workload and non-contact injury incidence in elite foot- ball players competing in European leagues. Eur. J. Sport Sci. 2018, 18, 1280–1287. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Ottawa, U.O. Newcastle-Ottawa Quality Assessment Scale Cohort Studies; University of Ottawa: Ottawa, ON, Canada, 2014. [Google Scholar]
- Sons, J.W. Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Hoboken, NJ, USA, 2019. [Google Scholar]
- Bowen, L.; Gross, A.S. Spikes in acute: Chronic workload ratio (ACWR) associated with a 5–7 times greater injury rate in English Premier League football players: A comprehensive 3-year study. Br. J. Sports Med. 2020, 54, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Carbone, L.; Sampietro, M.; Cicognini, A.; García-Sillero, M.; Vargas-Molina, S. Is the Relationship between Acute and Chronic Workload a Valid Predictive Injury Tool? A Bayesian Analysis. J. Clin. Med. 2022, 11, 5945. [Google Scholar] [CrossRef] [PubMed]
- Fanchini, M.; Rampinini, E. Despite association, the acute: Chronic work load ratio does not predict non-contact injury in elite footballers. Sci. Med. Footb. 2018, 2, 108–114. [Google Scholar] [CrossRef]
- Malone, S.; Owen, A.; Newton, M.; Mendes, B.; Collins, K.D.; Gabbett, T.J. The acute:chonic workload ratio in relation to injury risk in professional soccer. J. Sci. Med. Sport 2017, 20, 561–565. [Google Scholar] [CrossRef] [PubMed]
- Mohr, P.A.; Matias, T.S.; de Lucas, R.D. Association between internal training load and muscle injuries in Brazilian professional soccer players. Biol. Sport 2023, 40, 675–679. [Google Scholar] [CrossRef] [PubMed]
- Nobari, H.; Khalili, S.M.; Zamorano, A.D.; Bowman, T.G.; Granacher, U. Workload is associated with the occurrence of non-contact injuries in professional male soccer players: A pilot study. Front. Psychol. 2022, 13, 925722. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro-Alvares, J.; Cetolin, T.; Haupenthal, A.; Baroni, B.M. Acute:chronic workload ratio of professional soccer players preceding hamstring muscle injuries: A 2-season retrospective study. Sport Sci. Health 2023. [Google Scholar] [CrossRef]
- Suarez-Arrones, L.; De Alba, B.; Röll, M.; Torreno, I.; Strütt, S.; Freyler, K.; Ritzmann, R. Player Monitoring in Professional Soccer: Spikes in Acute:Chronic Workload Are Dissociated From Injury Occurrence. Front. Sports Act. Living 2020, 2, 75. [Google Scholar] [CrossRef]
- Tiernan, C.; Comyns, T.; Lyons, M.; Nevill, A.M.; Warrington, G. The Association Between Training Load Indices and Injuries in Elite Soccer Players. J. Strength Cond. Res. 2022, 36, 3143–3150. [Google Scholar] [CrossRef]
- Impellizzeri, F.M.; Rampinini, E.; Coutts, A.J.; Sassi, A.L.D.O.; Marcora, S.M. Use of RPE-based training load in soccer. Med. Sci. Sports Exerc. 2004, 36, 1042–1047. [Google Scholar] [CrossRef]

{kind=link}
| Study | NOS Score | |||
|---|---|---|---|---|
| Selection | Comparability | Outcome | Total Score | |
| Bowen et al., 2020 [25] | 3 | 2 | 2 | 7, G |
| Carbone et al., 2022 [26] | 3 | 1 | 2 | 6, G |
| Delecroix et al., 2018 [21] | 2 | 1 | 2 | 5, F |
| Fanchini et al., 2018 [27] | 2 | 1 | 1 | 4, P |
| Fousekis et al., 2023 [12] | 3 | 1 | 2 | 6, G |
| Jasper et al., 2018 [19] | 4 | 1 | 0 | 5, P |
| Malone et al., 2017 [28] | 3 | 1 | 2 | 6, G |
| Mohr et al., 2023 [29] | 3 | 1 | 2 | 6, G |
| Nobari et al., 2022 [30] | 2 | 1 | 1 | 4, P |
| Ribeiro-Alvarez et al., 2023 [31] | 3 | 1 | 2 | 6, G |
| Suarez-Arrones et al., 2020 [32] | 3 | 1 | 1 | 5, P |
| Tiernan et al., 2022 [33] | 3 | 1 | 2 | 6, G |
| Study | Year | Sample Size | Duration | Variables | Number of Injuries | Kind of ACWR | Results/Conclusions |
|---|---|---|---|---|---|---|---|
| Bowen et al. [25] | 2020 | 33 | 3 seasons | TD, LID, HSD, SD, ACC, DEC | 91 | Coupled 1:4 | The highest risk of non-contact injuries occurred when there was a low chronic exposure to decelerations (<1731) and the ACWR exceeded 2.0. Similarly, the risk of non-contact injuries was 5–6 times greater for accelerations and low-intensity distance when chronic workloads were classified as low and when the ACWR surpassed 2.0, compared to instances where the ACWR was below this threshold. When considering all chronic workloads, an ACWR exceeding 2.0 was linked to a significant but comparatively lower injury risk for the same metrics, including total distance. |
| Carbone et al. [26] | 2022 | 35 | >6 months | RPE | 30 | Coupled 1:4 and ACWR randomly generated | The likelihood of experiencing an injury, whether conditioned by ACWR or a randomly generated ACWR, remained consistent across all estimated quantiles, and the distinctions between them lacked statistical significance. Conclusions drawn indicate that the ACWR ratio, when employing internal load monitoring, does not demonstrate superior predictive capabilities compared to a synthetic ACWR generated with a random denominator for assessing the probability of injury. It is advised not to rely solely on ACWR in isolation for analyzing the causal relationship between load and injury. |
| Delecroix et al. [21] | 2018 | 130 | 1 season | RPE | 237 | Coupled 1:2, 1:3, 1:4 | The occurrence of injuries was elevated when the A/C ratios for 4-week and 2-week periods were below 0.85. Similarly, increased injury incidence was observed when the 2-week A/C ratio deviated from the 0.85–1.25 range. Nevertheless, the presence of low sensitivity and/or specificity values, along with minimal changes in the probability of injury, suggested that workload, when considered in isolation, is not a reliable predictor of injuries. None of the A/C workload combinations proved suitable for accurately predicting injuries. |
| Fanchini et al. [27] | 2018 | 34 | 3 seasons | RPE | 90 | Coupled 1:2, 1:3, 1:4 | Considering these results, even when acute/chronic ratios are very high (based on the current sample), predicting injuries seems improbable. Although there was an association between acute/chronic markers, their predictive capability was limited. |
| Fousekis et al. [12] | 2022 | 35 | 1 season | TD, HSD, SD, ACC, DEC | 9 | Coupled 1:2, 1:4 | In this study, both models assessing ACWR4 and ACWR2 provide insights into the potential likelihood of non-contact injuries in professional soccer players. The ACWR2 model appears to be a more sensitive indicator, as the differences were more pronounced across a greater number of examined variables. The findings suggest that ACWR is associated with the subsequent occurrence of injuries, but the threshold for ACWR can vary. This variability is primarily influenced by evaluating the load of the last two weeks in comparison to the load of the four weeks preceding the injury. |
| Jaspers et al. [19] | 2018 | 35 | 2 seasons | TD, HSD, ACC, DEC, RPE | 64 | Coupled 1:4 | An elevated ratio for HSD (>1.18) led to an increased risk of injury, while lower injury risks were observed when comparing moderate ratios for ACC (0.87–1.12), DEC (0.86–1.12), and RPE x duration (0.85–1.12) to low ratios. |
| Malone et al. [28] | 2017 | 48 | 1 season | RPE | 75 | Coupled 1:4 | Nevertheless, players who maintained comparable in-season acute/chronic workload ratios ranging from >1.00 to <1.25 exhibited a further diminished risk of injury. |
| Mohr et al. [29] | 2023 | 32 | 2 seasons | RPE | 33 | Coupled 1:4 | There was no association between ACWR and injury occurrence. |
| Nobari et al. [30] | 2022 | 21 | 1 season | Training load marker (BL) from GPS and accelerometer | 21 | ACWR = Awn/(Awn − 1 + Awn − 2 + Awn − 3) × 0.333 | ACWR appears to be a good indicator for estimating the injury risk. |
| Ribeiro-Alvares et al. [31] | 2023 | 48 | 2 seasons | TD, HSD, SD | 20 | Uncoupled 1:3 | Considering that three-quarters of hamstring injuries in professional soccer players were preceded by ACWR values below 1.5 across all GPS metrics, it is advisable for medical and coaching staff to exercise caution when relying solely on the ACWR ‘danger zone’ as the primary metric to assess player availability for training or matches. |
| Suarez-Arrones et al. [32] | 2020 | 15 | 10 weeks | TD, HSD, SD | 1 | Uncoupled 1:4 | The current study indicated that spikes in the ACWR did not correlate with subsequent injury incidents among professional soccer players. |
| Tiernan et al. [33] | 2022 | 15 | 1 season | RPE | 21 | Uncoupled 1:4 and exponentially weighted moving averages (EWMA) ACWR | A rise in ACWR by 0.1, surpassing 1.0, elevated the likelihood of a non-contact injury occurring five days later, with 62% of injuries taking place if ACWR was above 1.20. Moreover, this study revealed that five days preceding an injury (contact or non-contact), a player faced a 30% heightened risk of a non-contact injury and a 26% increased risk of a contact injury if the EWMA ACWR increased by 0.1, surpassing 0.97. The findings suggest that EWMA ACWR might be a more sensitive measure for identifying players at a higher risk of injury compared to ACWR. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michailidis, Y. A Systematic Review on Utilizing the Acute to Chronic Workload Ratio for Injury Prevention among Professional Soccer Players. Appl. Sci. 2024, 14, 4449. https://doi.org/10.3390/app14114449
Michailidis Y. A Systematic Review on Utilizing the Acute to Chronic Workload Ratio for Injury Prevention among Professional Soccer Players. Applied Sciences. 2024; 14(11):4449. https://doi.org/10.3390/app14114449
Chicago/Turabian StyleMichailidis, Yiannis. 2024. "A Systematic Review on Utilizing the Acute to Chronic Workload Ratio for Injury Prevention among Professional Soccer Players" Applied Sciences 14, no. 11: 4449. https://doi.org/10.3390/app14114449
APA StyleMichailidis, Y. (2024). A Systematic Review on Utilizing the Acute to Chronic Workload Ratio for Injury Prevention among Professional Soccer Players. Applied Sciences, 14(11), 4449. https://doi.org/10.3390/app14114449