

Personalized Setup Optimization Strategies to Improve Clinical Workflow in Image-Guided Pediatric Particle Therapy

 , , and
, , and
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients Population
2.2. Setup Verification Procedures in CNAO
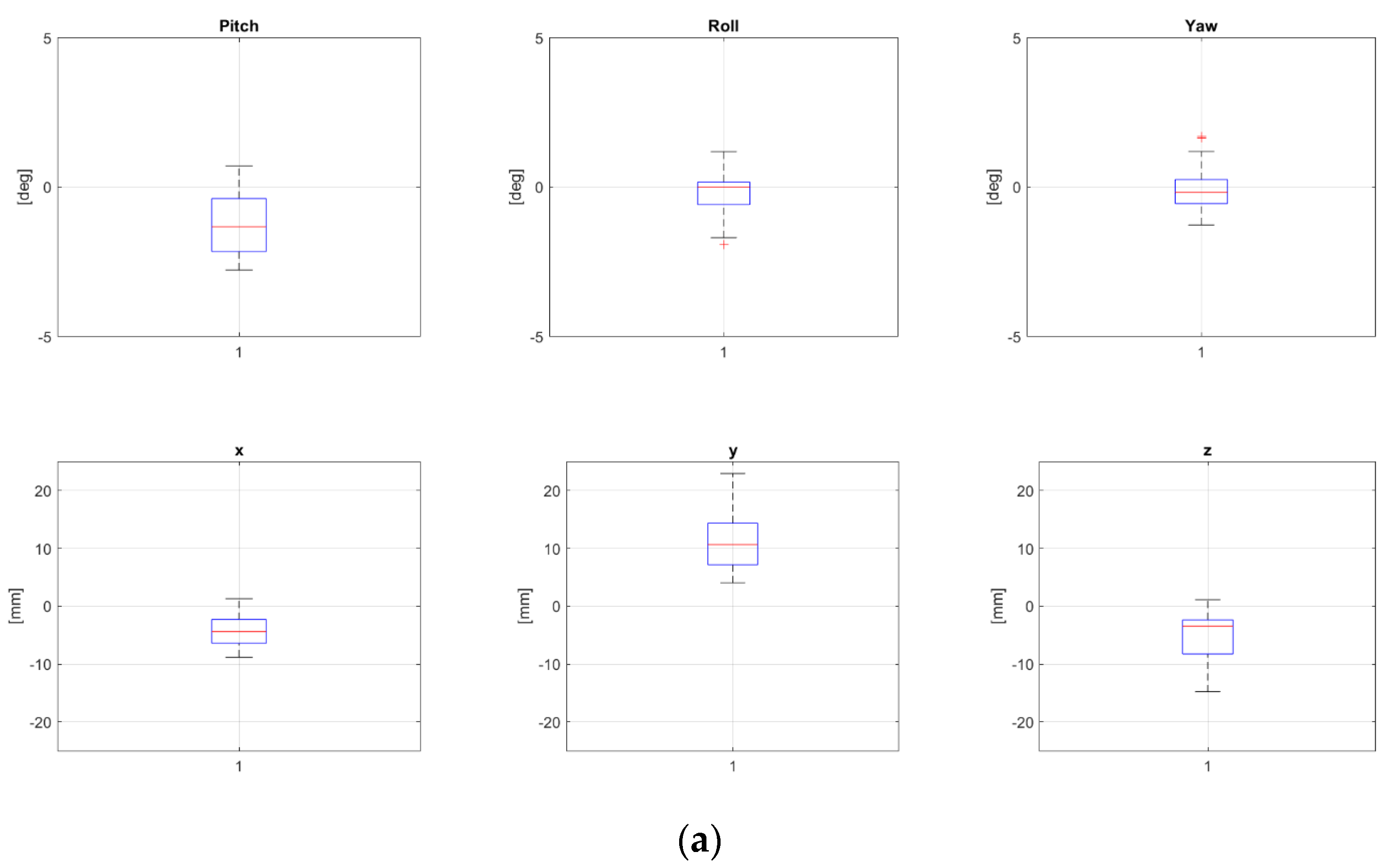
2.3. Random and Systematic Errors
2.4. Setup Data Collection
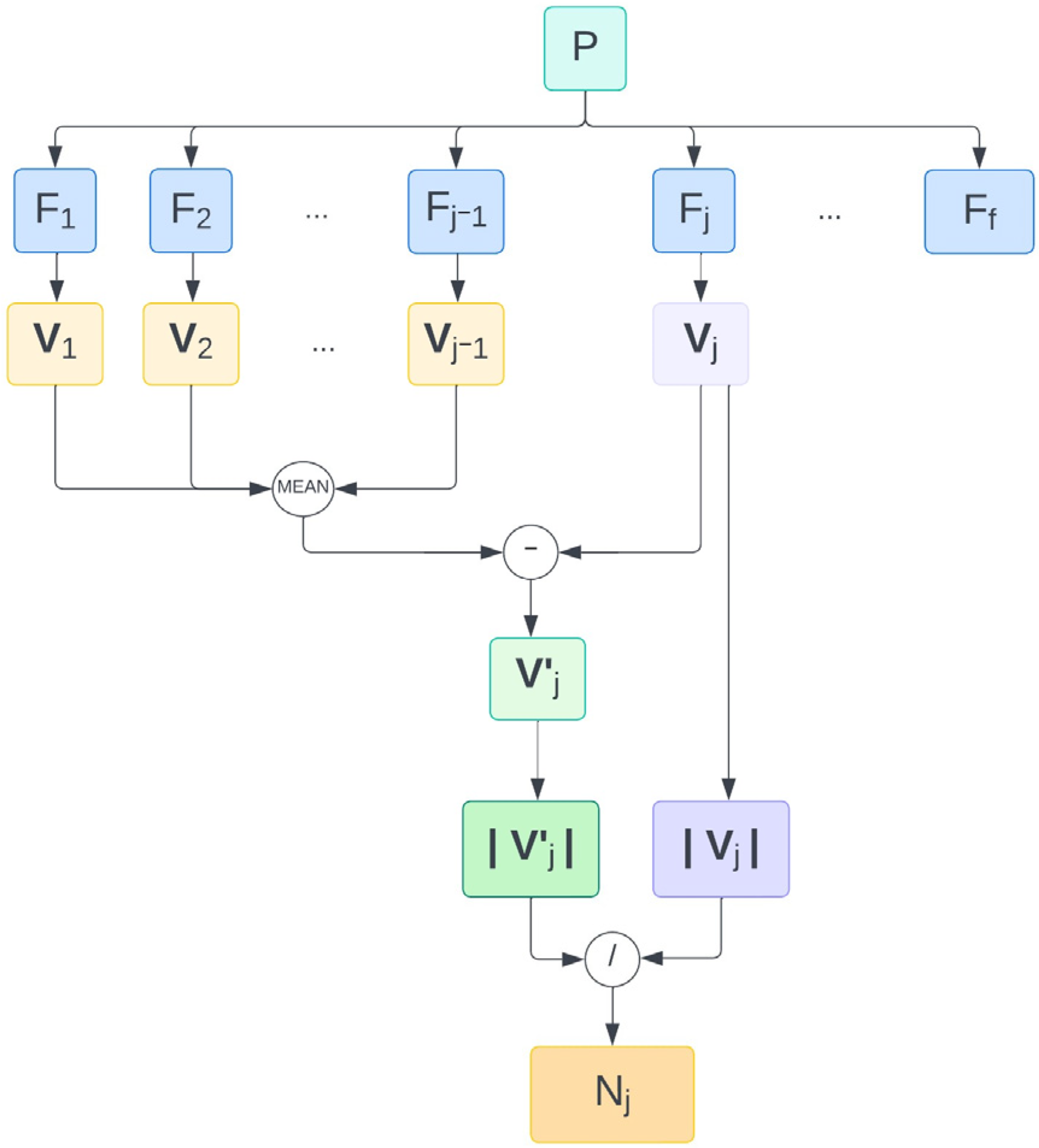
2.5. Workflow Design to Pre-Align Patient
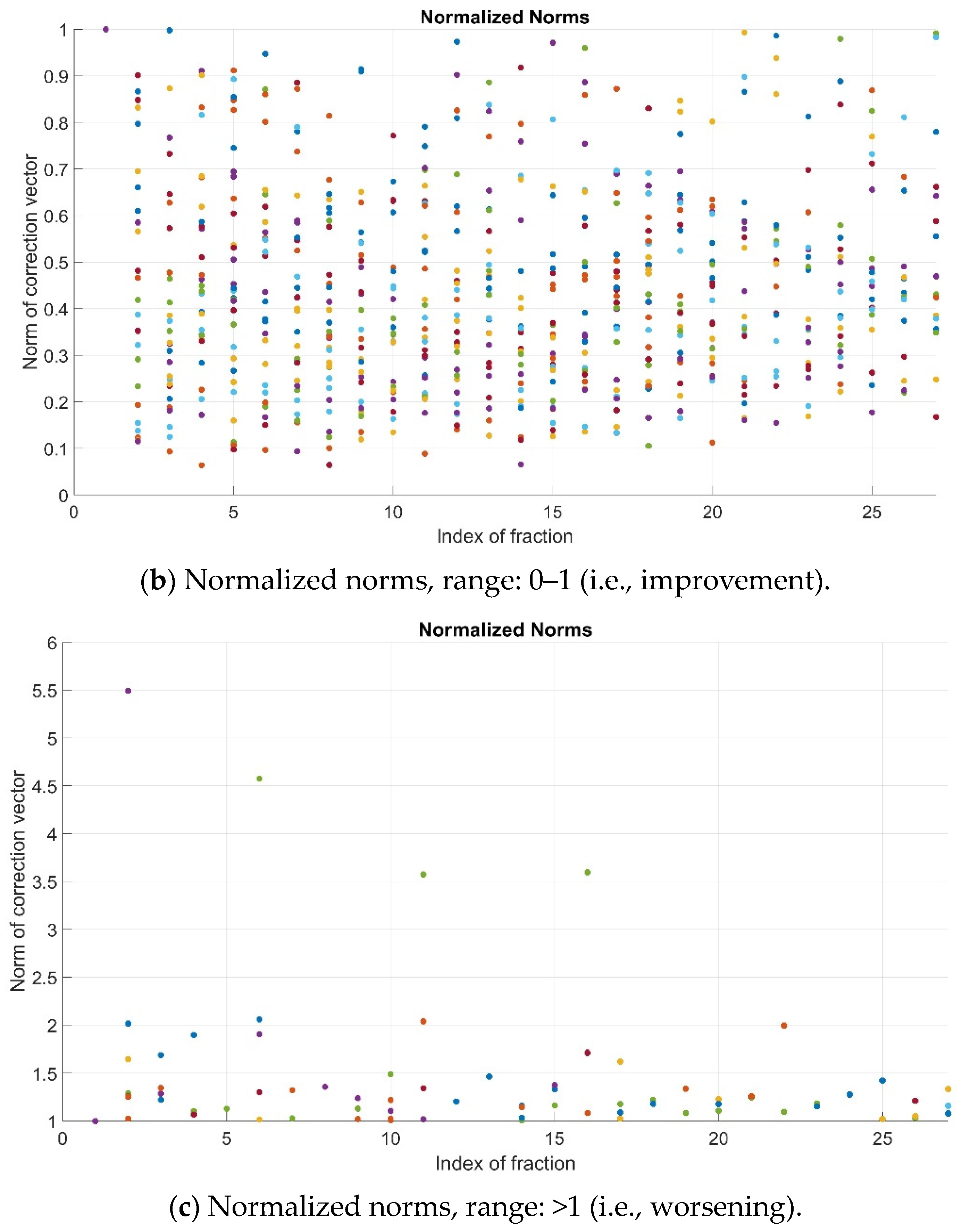
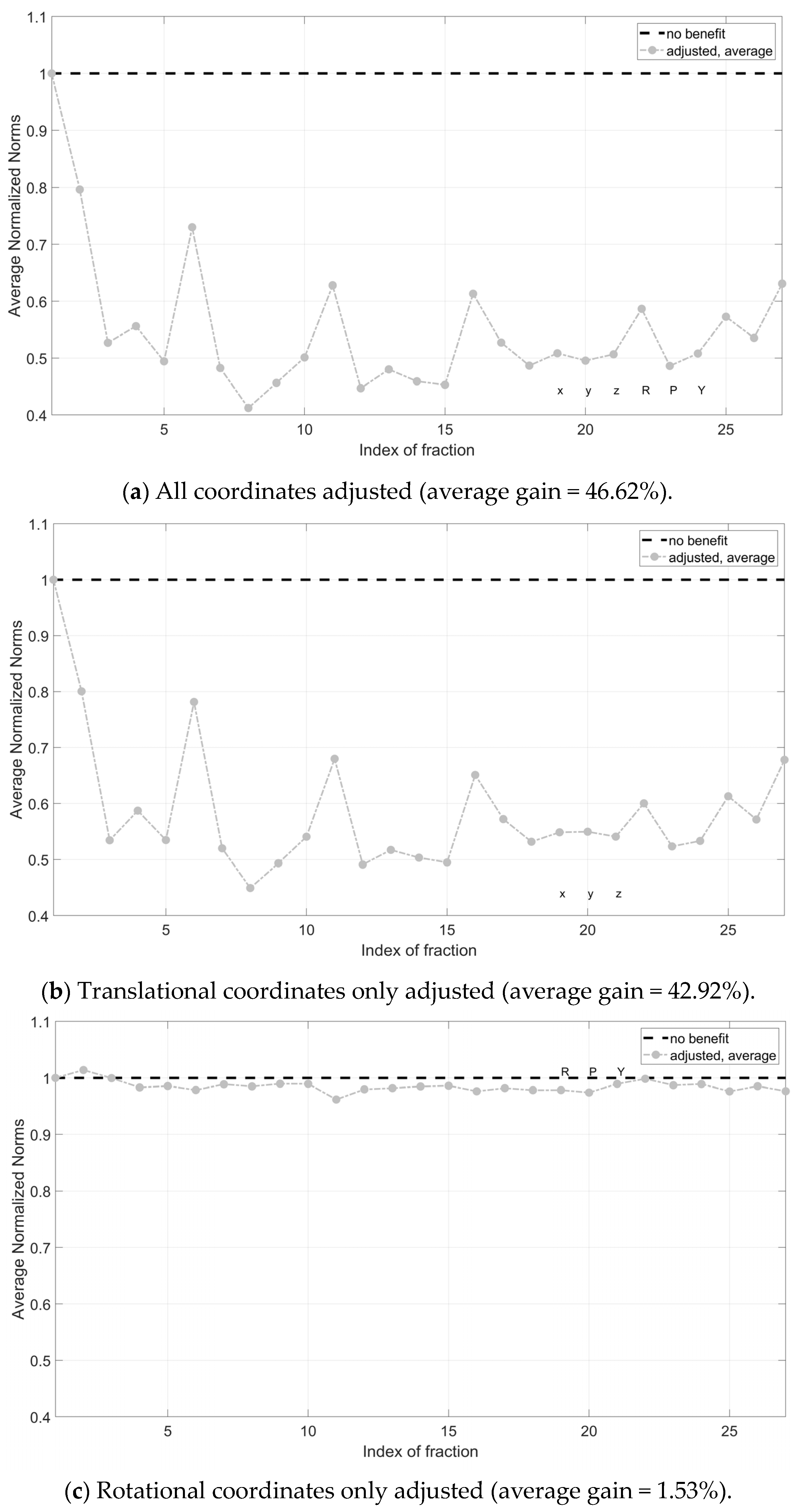
3. Results
4. Discussion
4.1. Main Findings
4.2. Comparison with Previous Investigations
4.3. Strenghts and Weaknesses
4.4. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Steliarova-Foucher, E.; Colombet, M.; Ries, L.A.G.; Moreno, F.; Dolya, A.; Bray, F.; Hesseling, P.; Shin, H.Y.; Stiller, C.A.; IICC-3 contributors. International incidence of childhood cancer, 2001–2010: A population-based registry study. Lancet Oncol. 2017, 18, 719–731, Erratum in Lancet Oncol. 2017, 18, e301. [Google Scholar] [CrossRef]
- Rombi, B.; Vennarini, S.; Vinante, L.; Ravanelli, D.; Amichetti, M. Proton radiotherapy for pediatric tumors: Review of first clinical results. Ital. J. Pediatr. 2014, 40, 74. [Google Scholar] [CrossRef]
- Sujith, B.; Yock, T.I. Proton beam therapy in pediatric oncology. Curr. Opin. Pediatr. 2019, 31, 28–34. [Google Scholar] [CrossRef]
- Greenberger, B.A.; Yock, T.I. The role of proton therapy in pediatric malignancies: Recent advances and future directions. Semin. Oncol. 2020, 47, 8–22. [Google Scholar] [CrossRef]
- Liebl, J.; Paganetti, H.; Zhu, M.; Winey, B.A. The influence of patient positioning uncertainties in proton radiotherapy on proton range and dose distributions. Med. Phys. 2014, 41, 091711. [Google Scholar] [CrossRef]
- Ricotti, R.; Pella, A.; Tagaste, B.; Elisei, G.; Fontana, G.; Bonora, M.; Ciocca, M.; Valvo, F.; Orecchia, R.; Baroni, G. Long-time clinical experience in patient setup for several particle therapy clinical indications: Management of patient positioning and evaluation of setup reproducibility and stability. Br. J. Radiol. 2020, 93, 20190595. [Google Scholar] [CrossRef]
- Bell, K.; Licht, N.; Rübe, C.; Dzierma, Y. Image guidance and positioning accuracy in clinical practice: Influence of positioning errors and imaging dose on the real dose distribution for head and neck cancer treatment. Radiat. Oncol. 2018, 13, 190. [Google Scholar] [CrossRef]
- Qubala, A.; Schwahofer, A.; Jersemann, S.; Eskandarian, S.; Harrabi, S.; Naumann, P.; Winter, M.; Ellerbrock, M.; Shafee, J.; Abtehi, S.; et al. Optimizing the Patient Positioning Workflow of Patients with Pelvis, Limb, and Chest/Spine Tumors at an Ion-Beam Gantry based on Optical Surface Guidance. Adv. Radiat. Oncol. 2022, 8, 101105. [Google Scholar] [CrossRef]
- Bell, K.; Heitfeld, M.; Licht, N.; Rübe, C.; Dzierma, Y. Influence of daily imaging on plan quality and normal tissue toxicity for prostate cancer radiotherapy. Radiat. Oncol. 2017, 12, 7. [Google Scholar] [CrossRef]
- Dzierma, Y.; Mikulla, K.; Richter, P.; Bell, K.; Melchior, P.; Nuesken, F.; Rübe, C. Imaging dose and secondary cancer risk in image-guided radiotherapy of pediatric patients. Radiat. Oncol. 2018, 13, 168. [Google Scholar] [CrossRef]
- Stock, M.; Georg, D.; Ableitinger, A.; Zechner, A.; Utz, A.; Mumot, M.; Kragl, G.; Hopfgartner, J.; Gora, J.; Böhlen, T.; et al. The technological basis for adaptive ion beam therapy at MedAustron: Status and outlook. Z. Med. Phys. 2018, 28, 196–210. [Google Scholar] [CrossRef]
- Collings, E.W.; Lu, L.; Gupta, N.; Sumption, M.D. Accelerators, Gantries, Magnets and Imaging Systems for Particle Beam Therapy: Recent Status and Prospects for Improvement. Front. Oncol. 2022, 11, 737837. [Google Scholar] [CrossRef]
- Wall, V.; Marignol, L.; ElBeltagi, N. Image-Guided Radiotherapy in Paediatrics: A Survey of International Patterns of Practice. J. Med. Imaging Radiat. Sci. 2018, 49, 265–269. [Google Scholar] [CrossRef]
- Brock, K.K.; Mutic, S.; McNutt, T.R.; Li, H.; Kessler, M.L. Use of image registration and fusion algorithms and techniques in radiotherapy: Report of the AAPM Radiation Therapy Committee Task Group No. 132. Med. Phys. 2017, 44, e43–e76. [Google Scholar] [CrossRef]
- de Boer, H.C.; Heijmen, B.J. eNAL: An extension of the NAL setup correction protocol for effective use of weekly follow-up measurements. Int. J. Radiat. Oncol. Biol. Phys. 2007, 67, 1586–1595. [Google Scholar] [CrossRef]
- Kukolowicz, P.; Mietelska, M.; Kiprian, D. Effectiveness of the No action level protocol for head & neck patients—Time considerations. Rep. Pr. Oncol. Radiother. 2020, 25, 828–831. [Google Scholar] [CrossRef]
- Johnson, P.B.; Jackson, A.; Saki, M.; Feldman, E.; Bradley, J. Patient posture correction and alignment using mixed reality visualization and the HoloLens 2. Med. Phys. 2022, 49, 15–22. [Google Scholar] [CrossRef]
- Pella, A.; Riboldi, M.; Tagaste, B.; Bianculli, D.; Desplanques, M.; Fontana, G.; Cerveri, P.; Seregni, M.; Fattori, G.; Orecchia, R.; et al. Commissioning and quality assurance of an integrated system for patient positioning and setup verification in particle therapy. Technol. Cancer Res. Treat. 2014, 13, 303–314. [Google Scholar] [CrossRef]
- Desplanques, M.; Tagaste, B.; Fontana, G.; Pella, A.; Riboldi, M.; Fattori, G.; Donno, A. A comparative study between the imaging system the optical tracking system in proton therapy at, C.N.A.O. J. Radiat. Res. 2013, 54 (Suppl. 1), i129–i135. [Google Scholar] [CrossRef]
- Fattori, G.; Riboldi, M.; Pella, A.; Peroni, M.; Cerveri, P.; Desplanques, M.; Fontana, G.; Tagaste, B.; Valvo, F.; Orecchia, R.; et al. Image guided particle therapy in CNAO room 2: Implementation and clinical validation. Phys. Med. 2015, 31, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Ciocca, M.; Mirandola, A.; Molinelli, S.; Russo, S.; Mastella, E.; Vai, A.; Mairani, A.; Magro, G.; Pella, A.; Donetti, M.; et al. Commissioning of the 4-D treatment delivery system for organ motion management in synchrotron-based scanning ion beams. Phys. Med. 2016, 32, 1667–1671. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| P | R | Age | S | N | Pitch | Roll | Yaw | X | Y | Z | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | M | SD | M | SD | M | SD | |||||
| 1 | 2 | 19 | EC | - | −0.48 | 0.32 | 0.28 | 0.88 | 0.24 | 0.73 | −3.77 | 2.49 | 4.73 | 3.49 | −1.39 | 1.48 |
| 2 | 2 | 9 | C | - | −0.35 | 0.47 | 0.27 | 0.76 | 0.08 | 0.55 | −2.93 | 0.96 | −0.50 | 0.59 | 1.34 | 0.61 |
| 3 | 1–3 | 4 | C | - | −1.54 | 0.66 | −1.32 | 0.46 | −0.40 | 0.38 | 0.32 | 0.64 | 0.52 | 0.70 | −2.82 | 1.33 |
| 4 | 1–3 | 23 | C | - | 1.07 | 0.94 | 0.51 | 0.50 | 0.89 | 0.54 | 0.24 | 0.97 | 3.70 | 0.73 | −4.75 | 0.49 |
| 5 | 1–3 | 13 | C | - | −0.36 | 1.27 | −0.82 | 1.24 | 0.23 | 0.51 | 0.39 | 2.01 | −0.33 | 1.86 | −0.85 | 1.55 |
| 6 | 1–3 | 18 | C | - | 0.09 | 0.34 | 0.68 | 0.47 | 0.19 | 0.34 | 1.36 | 0.72 | 1.53 | 0.95 | −3.41 | 0.27 |
| 7 | 1–3 | 12 | C | - | 0.20 | 1.08 | −0.11 | 0.55 | −0.16 | 0.47 | −1.31 | 1.37 | −1.05 | 0.94 | −3.98 | 0.45 |
| 8 | 2 | 17 | EC | - | −1.22 | 1.05 | −0.26 | 0.69 | −0.03 | 0.73 | −4.19 | 3.02 | 10.90 | 4.61 | −4.84 | 4.03 |
| 9 | 1–3 | 15 | C | - | 0.36 | 0.63 | 0.33 | 0.48 | 0.09 | 0.30 | 1.49 | 1.56 | 2.64 | 2.00 | −3.36 | 0.93 |
| 10 | 2 | 2 | EC | Y | −0.19 | 0.49 | 0.05 | 0.39 | 0.28 | 0.43 | −2.80 | 1.33 | 2.26 | 2.12 | −2.81 | 0.86 |
| 11 | 1–3 | 24 | C | - | −0.46 | 0.65 | 0.22 | 0.55 | 0.48 | 0.58 | 1.12 | 0.69 | 0.20 | 0.49 | −3.60 | 1.61 |
| 12 | 1–3 | 28 | C | - | −0.24 | 0.57 | 0.25 | 0.32 | 0.48 | 0.28 | 0.89 | 0.94 | 0.17 | 0.69 | −3.66 | 0.93 |
| 13 | 1–3 | 13 | C | - | −1.23 | 0.86 | −1.67 | 0.53 | 0.68 | 0.65 | −0.46 | 1.30 | −2.58 | 0.78 | −5.50 | 0.45 |
| 14 | 2 | 2 | EC | Y | −1.29 | 0.82 | −0.15 | 0.59 | −0.32 | 0.61 | −2.70 | 1.24 | 2.47 | 1.67 | −4.01 | 1.69 |
| 15 | 2 | 14 | C | - | 0.07 | 0.59 | 0.09 | 0.58 | 0.08 | 0.46 | −1.78 | 1.35 | −0.73 | 1.21 | 1.54 | 1.05 |
| 16 | 1–3 | 8 | C | - | 0.23 | 0.36 | 0.27 | 0.46 | 0.49 | 0.32 | 1.52 | 1.03 | 0.91 | 0.79 | −4.31 | 1.23 |
| 17 | 1–3 | 13 | C | - | −1.17 | 0.73 | 0.07 | 0.18 | −0.50 | 0.54 | −0.74 | 0.57 | 0.14 | 1.10 | −4.19 | 0.31 |
| 18 | 1–3 | 2 | C | Y | 0.14 | 0.30 | 0.40 | 0.42 | 0.18 | 0.40 | −0.54 | 1.54 | 0.95 | 1.30 | −3.13 | 3.37 |
| 19 | 1–3 | 7 | C | Y | 1.52 | 0.85 | −0.62 | 0.75 | 0.34 | 0.46 | 1.21 | 0.78 | 2.01 | 1.41 | −3.60 | 1.53 |
| 20 | 1–3 | 16 | C | - | −0.28 | 0.66 | 0.05 | 0.55 | 0.16 | 0.44 | 0.58 | 1.05 | 0.75 | 1.39 | −3.43 | 0.46 |
| 21 | 1–3 | 8 | C | - | 0.91 | 0.58 | 1.09 | 0.39 | 1.25 | 0.40 | 1.86 | 0.54 | 1.66 | 1.06 | −5.09 | 0.31 |
| 22 | 1–3 | 22 | C | - | 0.53 | 0.58 | 0.28 | 0.43 | −0.32 | 0.29 | 0.13 | 2.57 | 2.57 | 1.93 | −3.93 | 0.89 |
| 23 | 2 | 3 | EC | Y | −0.43 | 0.74 | −0.41 | 0.91 | −0.10 | 0.56 | −2.58 | 1.26 | 0.21 | 2.79 | −3.19 | 1.35 |
| 24 | 2 | 17 | EC | - | −0.82 | 0.66 | −0.51 | 0.66 | −0.34 | 0.60 | −4.61 | 1.89 | 5.51 | 7.41 | −5.96 | 2.07 |
| 25 | 1–3 | 14 | C | - | 0.44 | 0.72 | 0.50 | 0.40 | 0.56 | 0.41 | 0.66 | 1.37 | 1.11 | 1.29 | −2.49 | 0.57 |
| 26 | 1–3 | 22 | C | - | 0.14 | 0.26 | 0.24 | 0.31 | 0.86 | 0.22 | −0.79 | 0.65 | 2.06 | 0.85 | −2.29 | 0.22 |
| 27 | 1–3 | 16 | C | - | −0.27 | 0.38 | 0.27 | 0.40 | 0.13 | 0.24 | −0.12 | 1.25 | −1.22 | 0.92 | −2.40 | 0.66 |
| 28 | 2 | 15 | EC | - | −0.61 | 0.69 | −0.44 | 1.00 | 0.07 | 1.05 | 0.17 | 1.55 | 2.47 | 2.70 | −3.99 | 1.31 |
| 29 | 1–3 | 14 | C | - | 0.03 | 0.82 | −0.56 | 0.83 | −0.03 | 0.30 | 3.18 | 1.88 | 1.36 | 3.10 | −1.60 | 1.16 |
| 30 | 2 | 14 | EC | - | −0.08 | 0.66 | 0.05 | 0.40 | 0.37 | 0.74 | −2.72 | 1.14 | 0.80 | 2.64 | −1.00 | 0.95 |
| 31 | 1–3 | 8 | C | - | −0.14 | 0.19 | 0.32 | 0.16 | 0.50 | 0.22 | 1.06 | 0.36 | 2.31 | 0.70 | −1.44 | 0.33 |
| 32 | 1–3 | 11 | C | - | 0.04 | 0.38 | 0.21 | 0.27 | 0.54 | 0.19 | 0.77 | 0.33 | 0.92 | 0.81 | −4.50 | 0.26 |
| MA | 0.53 | 0.63 | 0.42 | 0.55 | 0.36 | 0.47 | 1.53 | 1.26 | 1.91 | 1.72 | 3.26 | 1.08 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pepa, M.; Pella, A.; Sellaro, G.; Galante, F.; Mirandola, A.; Ghirelli, A.; Vennarini, S.; Colombo, F.; Imparato, S.; Iannalfi, A.; et al. Personalized Setup Optimization Strategies to Improve Clinical Workflow in Image-Guided Pediatric Particle Therapy. Appl. Sci. 2024, 14, 4658. https://doi.org/10.3390/app14114658
Pepa M, Pella A, Sellaro G, Galante F, Mirandola A, Ghirelli A, Vennarini S, Colombo F, Imparato S, Iannalfi A, et al. Personalized Setup Optimization Strategies to Improve Clinical Workflow in Image-Guided Pediatric Particle Therapy. Applied Sciences. 2024; 14(11):4658. https://doi.org/10.3390/app14114658
Chicago/Turabian StylePepa, Matteo, Andrea Pella, Giulia Sellaro, Federica Galante, Alfredo Mirandola, Angelica Ghirelli, Sabina Vennarini, Francesca Colombo, Sara Imparato, Alberto Iannalfi, and et al. 2024. "Personalized Setup Optimization Strategies to Improve Clinical Workflow in Image-Guided Pediatric Particle Therapy" Applied Sciences 14, no. 11: 4658. https://doi.org/10.3390/app14114658