
Upper Airway Collapsibility during Sleep Endoscopy with a Titratable Mandibular Advancement Simulator in Obstructive Sleep Apnea Patients

 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Procedure
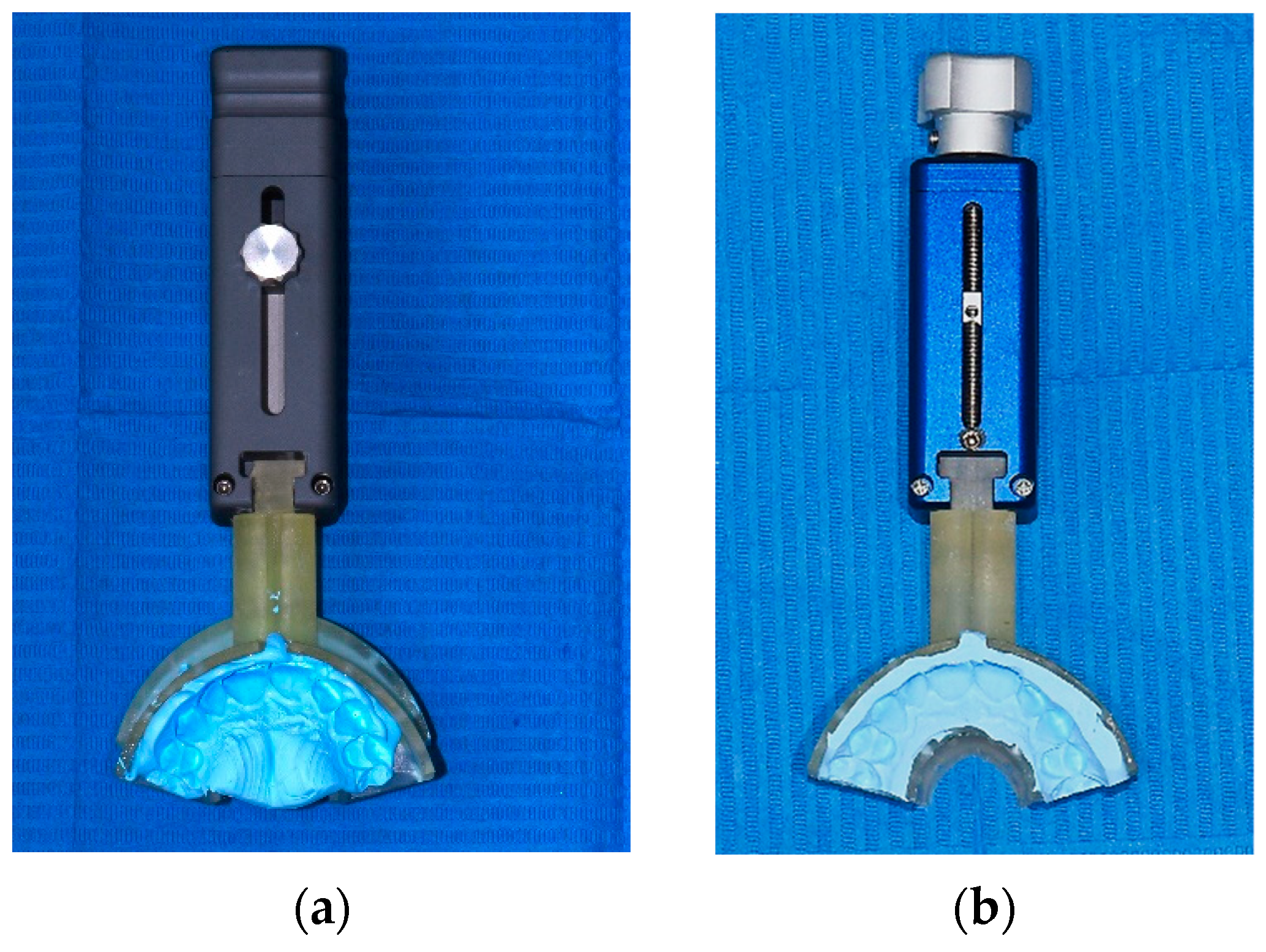
2.3. TMA Simulator Description
2.4. Statistical Analysis
3. Results
3.1. Between Group Comparison for General and Polygraphic Characteristics
3.2. Obstructive Sites without the TMA Simulator
3.3. VOTE Classification without the TMA Simulator
3.4. Obstructive Sites with TMA Simulator
3.5. VOTE Classification with TMA Simulator
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- AASM. American Academy of Sleep Medicine International Classification of Sleep Disorders; AASM: Westchester, IL, USA, 2005. [Google Scholar]
- Sateia, M.D.; Micheal, J. International Classification of Sleep Disorders—Third Edition Highlights and Modifications. Chest 2014, 146, 1384–1397. [Google Scholar] [CrossRef] [PubMed]
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; Heinzer, R.; Ip, M.S.M.; Morrell, M.J.; Nunez, C.M.; Patel, S.R.; Penzel, T.; Pépin, J.-L.; et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. Lancet Respir. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef] [PubMed]
- Heinzer, R.; Vat, S.; Marques-Vidal, P.; Marti-Soler, H.; Andries, D.; Tobback, N.; Mooser, V.; Preisig, M.; Malhotra, A.; Waeber, G.; et al. Prevalence of sleep-disordered breathing in the general population: The HypnoLaus study. Lancet Respir. Med. 2015, 3, 310–318. [Google Scholar] [CrossRef]
- Simmons, M.S.; Shapiro, C.M. The New DDS—“Dentists Diagnosing Sleep”. J. Dent. Sleep Med. 2020, 7. [Google Scholar] [CrossRef]
- Armeni, P.; Borsoi, L.; Costa, F.; Donin, G.; Gupta, A. Cost-of-Illness Study of Obstructive Sleep Apnea Syndrome (OSAS) in Italy; Università Bocconi: Milan, Italy, 2019. [Google Scholar]
- Bosi, M.; Incerti Parenti, S.; Sanna, A.; Plazzi, G.; De Vito, A.; Alessandri-Bonetti, G. Non-continuous positive airway pressure treatment options in obstructive sleep apnoea: A pathophysiological perspective. Sleep Med. Rev. 2021, 60, 101521. [Google Scholar] [CrossRef]
- Dieltjens, M.; Vanderveken, O. Oral Appliances in Obstructive Sleep Apnea. Healthcare 2019, 7, 141. [Google Scholar] [CrossRef]
- Marklund, M.; Braem, M.J.A.; Verbraecken, J. Update on oral appliance therapy. Eur. Respir. Rev. 2019, 28, 190083. [Google Scholar] [CrossRef] [PubMed]
- Mogell, K.; Blumenstock, N.; Mason, E.; Rohatgi, R.; Shah, S.; Schwartz, D. Definition of an Effective Oral Appliance for the Treatment of Obstructive Sleep Apnea and Snoring: An Update for 2019. J. Dent. Sleep Med. 2019, 6. [Google Scholar] [CrossRef]
- Incerti Parenti, S.; Bortolotti, F.; Alessandri-Bonetti, G. Oral appliances for obstructive sleep apnea. J. World Fed. Orthod. 2019, 8, 3–8. [Google Scholar] [CrossRef]
- Ferguson, K.A. The role of oral appliance therapy in the treatment of obstructive sleep apnea. Clin. Chest Med. 2003, 24, 355–364. [Google Scholar] [CrossRef]
- Ramar, K.; Dort, L.C.; Katz, S.G.; Lettieri, C.J.; Harrod, C.G.; Thomas, S.M.; Chervin, R.D. Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring with Oral Appliance Therapy: An Update for 2015. J. Clin. Sleep Med. 2015, 11, 773–827. [Google Scholar] [CrossRef] [PubMed]
- Randerath, W.J.; Verbraecken, J.; Andreas, S.; Bettega, G.; Boudewyns, A.; Hamans, E.; Jalbert, F.; Paoli, J.R.; Sanner, B.; Smith, I.; et al. Non-CPAP therapies in obstructive sleep apnoea. Eur. Respir. J. 2011, 37, 1000–1028. [Google Scholar] [CrossRef] [PubMed]
- De Vito, A.; Carrasco Llatas, M.; Ravesloot, M.J.; Kotecha, B.; De Vries, N.; Hamans, E.; Maurer, J.; Bosi, M.; Blumen, M.; Heiser, C.; et al. European position paper on drug-induced sleep endoscopy: 2017 Update. Clin. Otolaryngol. 2018, 43, 1541–1552. [Google Scholar] [CrossRef] [PubMed]
- Vanderveken, O.M. Drug-induced sleep endoscopy (DISE) as a guide towards upper airway behavior and treatment outcome: The quest for a vigorous standardization of DISE. Sleep Breath. 2018, 22, 897–899. [Google Scholar] [CrossRef] [PubMed]
- Croft, C.B.; Pringle, M. Sleep nasendoscopy: A technique of assessment in snoring and obstructive sleep apnoea. Clin. Otolaryngol. Allied Sci. 1991, 16, 504–509. [Google Scholar] [CrossRef] [PubMed]
- Kezirian, E.J.; Hohenhorst, W.; de Vries, N. Drug-induced sleep endoscopy: The VOTE classification. Eur. Arch. Otorhinolaryngol. 2011, 268, 1233–1236. [Google Scholar] [CrossRef] [PubMed]
- Rabelo, F.A.; Küpper, D.S.; Sander, H.H.; Fernandes, R.M.; Valera, F.C. Polysomnographic evaluation of propofol-induced sleep in patients with respiratory sleep disorders and controls. Laryngoscope 2013, 123, 2300–2305. [Google Scholar] [CrossRef] [PubMed]
- Morrison, D.L.; Launois, S.H.; Isono, S.; Feroah, T.R.; Whitelaw, W.A.; Remmers, J.E. Pharyngeal narrowing and closing pressures in patients with obstructive sleep apnea. Am. Rev. Respir. Dis. 1993, 148, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Sanjuán, P.; Arrieta, J.J.; Sanabria, J.; Alcaraz, M.; Bosco, G.; Pérez-Martín, N.; Pérez, A.; Carrasco-Llatas, M.; Moreno-Hay, I.; Ríos-Lago, M.; et al. Optimizing Mandibular Advancement Maneuvers during Sleep Endoscopy with a Titratable Positioner: DISE-SAM Protocol. J. Clin. Med. 2022, 11, 658. [Google Scholar] [CrossRef]
- Fernández-Sanjuán, P.; Alcaraz, M.; Bosco, G.; Pérez-Martín, N.; Morato, M.; Lugo, R.; Arrieta, J.J.; Sanabria, J.; Ríos-Lago, M.; Plaza, G. Modifications in Upper Airway Collapsibility during Sleep Endoscopy with a Mandibular Positioner: Study in Snorers and Obstructive Sleep Apnea Patients. J. Clin. Med. 2024, 13, 1184. [Google Scholar] [CrossRef]
- Ippolito, D.R.; Stipa, C.; Cameli, M.; Sorrenti, G.; Pelligra, I.; Alessandri-Bonetti, G. Maximum voluntary retrusion or habitual bite position for mandibular advancement assessment in the treatment of obstructive sleep apnoea patients. J. Oral Rehabil. 2020, 47, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Petri, N.; Christensen, I.J.; Svanholt, P.; Sonnesen, L.; Wildschiødtz, G.; Berg, S. Mandibular advancement device therapy for obstructive sleep apnea: A prospective study on predictors of treatment success. Sleep Med. 2019, 54, 187–194. [Google Scholar] [CrossRef] [PubMed]
- de Beeck, S.O.; Dieltjens, M.; Verbruggen, A.E.; Vroegop, A.V.; Wouters, K.; Hamans, E.; Willemen, M.; Verbraecken, J.; De Backer, W.A.; Van de Heyning, P.H.; et al. Phenotypic Labelling Using Drug-Induced Sleep Endoscopy Improves Patient Selection for Mandibular Advancement Device Outcome: A Prospective Study. J. Clin. Sleep Med. 2019, 15, 1089–1099. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, K.; Takaya, H.; Qian, J.; Petocz, P.; Ng, A.T.; Cistulli, P.A. Oral Appliance Treatment Response and Polysomnographic Phenotypes of Obstructive Sleep Apnea. J. Clin. Sleep Med. 2015, 11, 861–868. [Google Scholar] [CrossRef] [PubMed]
- Marco Pitarch, R.; Selva García, M.; Puertas Cuesta, J.; Marco Algarra, J.; Fernández Julian, E.; Fons Font, A. Effectiveness of a mandibular advancement device in obstructive sleep apnea patients: A prospective clinical trial. Eur. Arch. Otorhinolaryngol. 2018, 275, 1903–1911. [Google Scholar] [CrossRef]
- Torre, C.; Liu, S.Y.; Kushida, C.A.; Nekhendzy, V.; Huon, L.K.; Capasso, R. Impact of continuous positive airway pressure in patients with obstructive sleep apnea during drug-induced sleep endoscopy. Clin. Otolaryngol. 2017, 42, 1218–1223. [Google Scholar] [CrossRef]
- Schwab, R.J.; Pack, A.I.; Gupta, K.B.; Metzger, L.J.; Oh, E.; E Getsy, J.; A Hoffman, E.; Gefter, W.B. Upper airway and soft tissue structural changes induced by CPAP in normal subjects. Am. J. Respir. Crit. Care Med. 1996, 154 Pt 1, 1106–1116. [Google Scholar] [CrossRef] [PubMed]
- Bartolucci, M.L.; Bortolotti, F.; Raffaelli, E.; D’Antò, V.; Michelotti, A.; Alessandri Bonetti, G. The effectiveness of different mandibular advancement amounts in OSA patients: A systematic review and meta-regression analysis. Sleep Breath. 2016, 20, 911–919. [Google Scholar] [CrossRef] [PubMed]
- Masse, J.F. On the role of dentists in the diagnosis and treatment of obstructive sleep apnea: Controversy and controversy. J. Dent. Sleep Med. 2018, 5, 29–30. [Google Scholar] [CrossRef]
- Ma, Y.; Yu, M.; Gao, X. The effect of gradually increased mandibular advancement on the efficacy of an oral appliance in the treatment of obstructive sleep apnea. J. Clin. Sleep Med. 2020, 16, 1369–1376. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|---|
| V | NO OBSTRUCTION | Partial Antero-Posterior | Complete Antero Posterior | Partial Latero-lateral | Complete Latero-lateral | Partial Circular | Complete Circular | - | - | - |
| O | NO OBSTRUCTION | Partial Latero-lateral | Complete Latero-lateral | - | - | - | - | - | - | - |
| T | NO OBSTRUCTION | Partial Antero Posterior | Complete Antero Posterior | - | - | - | - | - | - | - |
| E | NO OBSTRUCTION | Secondary Partial Antero Posterior | Secondary Complete Antero Posterior | Secondary Partial Latero-lateral | Secondary Complete Latero-lateral | Primary Partial Antero Posterior | Primary Complete Antero Posterior | Primary Partial Latero-lateral | Primary Complete Latero-lateral | Arytenoids And Glottis |
| Males [n (%)] | 307 (91.6%) | |
| Age (years) [mean ± SD] | 49.98 ± 9.88 | |
| BMI (kg/m2) [mean ± SD] | 28.49 ± 3.48 | |
| AHI (ev/h) [mean ± SD] | 34.14 ± 18.61 | |
| OSAS mild (5 ≤ AHI < 15) [n (%)] | 54 (16.1%) | |
| OSAS moderate (15 ≤ AHI < 30) [n (%)] | 101 (30.2%) | |
| OSAS severe (AHI ≥ 30) [n (%)] | 180 (53.7%) | |
| Non-Responders [Mean ± SD] | Responders [Mean ± SD] | Difference (CI) | p (t-Test) | |
|---|---|---|---|---|
| Age (years) | 48.77 ± 9.86 | 50.76 ± 9.83 | −1.99 (−4.23; 0.25) | 0.082 |
| BMI (kg/m2) | 29.14 ± 3.81 | 28.09 ± 3.21 | 1.05 (0.29; 1.82) | 0.007 |
| Non-Responders [Mean ± SD] | Responders [Mean ± SD] | Difference (CI) | p (t-Test) | |
|---|---|---|---|---|
| AHI (ev/h) | 39.50 ± 19.65 | 30.82 ± 17.16 | 8.68 (4.66; 12.71) | <0.001 |
| AHIsup (ev/h) | 51.43 ± 21.51 | 46.58 ± 21.01 | 4.85 (0.03; 9.67) | 0.049 |
| AHInonsup (ev/h) | 25.71 ± 23.92 | 16.12 ± 17.68 | 9.59 (4.86; 14.32) | <0.001 |
| ODI (ev/h) | 39.69 ± 21.13 | 30.98 ± 19.66 | 8.71 (4.12; 13.30) | <0.001 |
| Satmed (%) | 92.89 ± 2.34 | 93.31 ± 1.84 | −0.43 (−0.90; 0.04) | 0.075 |
| Satmin (%) | 76.91 ± 8.19 | 79.20 ± 8.29 | −2.28 (−4.19; −0.37) | 0.019 |
| CT90 (%) | 14.51 ± 17.08 | 9.36 ± 11.25 | 5.15 (2.00; 8.30) | 0.001 |
| VOTE Classification | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | p | ||
| V | ||||||||||||
| Non Resp. | 5 (3.9%) | 2 (1.6%) | 18 (14.1%) | 3 (2.3%) | 34 (26.6%) | 0 (0.0%) | 66 (51.6%) | 0.008 | ||||
| Resp. | 5 (2.4%) | 13 (6.3%) | 53 (25.6%) | 5 (2.4%) | 62 (30.0%) | 1 (0.5%) | 68 (32.9%) | |||||
| O | ||||||||||||
| Non Resp. | 14 (10.9%) | 5 (3.9%) | 109 (85.2%) | 0.003 | ||||||||
| Resp. | 41 (19.8%) | 23 (11.1%) | 143 (69.1%) | |||||||||
| T | ||||||||||||
| Non Resp. | 60 (46.9%) | 24 (18.8%) | 44 (34.4%) | 0.103 | ||||||||
| Resp. | 86 (41.5%) | 27 (13.0%) | 94 (45.4%) | |||||||||
| E | ||||||||||||
| Non Resp. | 83 (64.8%) | 8 (6.3%) | 22 (17.2%) | 1 (0.8%) | 5 (3.9%) | 0 (0.0%) | 5 (3.9%) | 0 (0.0%) | 4 (3.1%) | 0 (0.0%) | 0.186 | |
| Resp. | 123 (59.4%) | 16 (7.7%) | 48 (23.2%) | 1 (0.5%) | 4 (1.9%) | 2 (1.0%) | 11 (5.3%) | 1 (0.5%) | 0 (0.0%) | 1 (0.5%) | ||
| VOTE Classification | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | p | ||
| V | ||||||||||||
| Non Resp. | 11 (8.6%) | 23 (18.0%) | 22 (17.2%) | 16 (12.5%) | 26 (20.3%) | 2 (1.6%) | 28 (21.9%) | <0.001 | ||||
| Resp. | 86 (41.5%) | 61 (29.5%) | 14 (6.8%) | 23 (11.1%) | 7 (3.4%) | 6 (2.9%) | 10 (4.8%) | |||||
| O | ||||||||||||
| Non Resp. | 32 (25.0%) | 35 (27.3%) | 61 (47.7%) | <0.001 | ||||||||
| Resp. | 141 (68.1%) | 55 (26.6%) | 11 (5.3%) | |||||||||
| T | ||||||||||||
| Non Resp. | 92 (71.9%) | 24 (18.8%) | 12 (9.4%) | 0.008 | ||||||||
| Resp. | 162 (78.3%) | 41 (19.8%) | 4 (1.9%) | |||||||||
| E | ||||||||||||
| Non Resp. | 98 (76.6%) | 10 (7.8%) | 4 (3.1%) | 2 (1.6%) | 1 (0.8%) | 4 (3.1%) | 5 (3.9%) | 2 (1.6%) | 2 (1.6%) | 0 (0.0%) | 0.005 | |
| Resp. | 190 (91.8%) | 6 (2.9%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 5 (2.4%) | 3 (1.4%) | 2 (1.0%) | 0 (0.0%) | 1 (0.5%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cameli, M.; Stipa, C.; Pelligra, I.; Ippolito, D.R.; Sorrenti, G.; Alessandri-Bonetti, G.; Incerti Parenti, S. Upper Airway Collapsibility during Sleep Endoscopy with a Titratable Mandibular Advancement Simulator in Obstructive Sleep Apnea Patients. Appl. Sci. 2024, 14, 4710. https://doi.org/10.3390/app14114710
Cameli M, Stipa C, Pelligra I, Ippolito DR, Sorrenti G, Alessandri-Bonetti G, Incerti Parenti S. Upper Airway Collapsibility during Sleep Endoscopy with a Titratable Mandibular Advancement Simulator in Obstructive Sleep Apnea Patients. Applied Sciences. 2024; 14(11):4710. https://doi.org/10.3390/app14114710
Chicago/Turabian StyleCameli, Matteo, Chiara Stipa, Irene Pelligra, Daniela Rita Ippolito, Giovanni Sorrenti, Giulio Alessandri-Bonetti, and Serena Incerti Parenti. 2024. "Upper Airway Collapsibility during Sleep Endoscopy with a Titratable Mandibular Advancement Simulator in Obstructive Sleep Apnea Patients" Applied Sciences 14, no. 11: 4710. https://doi.org/10.3390/app14114710
APA StyleCameli, M., Stipa, C., Pelligra, I., Ippolito, D. R., Sorrenti, G., Alessandri-Bonetti, G., & Incerti Parenti, S. (2024). Upper Airway Collapsibility during Sleep Endoscopy with a Titratable Mandibular Advancement Simulator in Obstructive Sleep Apnea Patients. Applied Sciences, 14(11), 4710. https://doi.org/10.3390/app14114710