Abstract
Social isolation and loneliness greatly contribute to negative health consequences in older adults. Technological solutions can be an asset in promoting social connections and healthy behaviours. This paper presents an innovative structure for an Internet of Things (IoT) platform specifically tailored for older persons. The framework utilises a supervised learning algorithm to classify users into four identified profiles to facilitate the adoption and engagement of technology. The platform incorporates wearables, such as socks and smart bands, to track physical activity, and a messaging module to encourage social interaction. The platform processes the acquired data to quantify steps and deliver tailored interventions remotely to the older adults through the AGAPE Assistant, the mHealth solution of the platform. Furthermore, the AGAPE Assistant has a user interface design for older adults, with a focus on their specific needs. Additionally, improving digital literacy among older adults is crucial for maximizing the long-term compliance and benefits of such technological solutions. On the other hand, AGAPE Monitor is a web application used by formal caregivers to configure the tailored interventions. The platform’s usability was assessed using different usability scale questionnaires, which revealed a mild level of user satisfaction and acceptance. The proposed framework is currently being deployed on more than 112 older adults across three countries: Italy, Romania, and Portugal. The proposed framework provides a holistic solution to encourage active ageing by adopting technology, implementing hybrid interventions, and promoting social interactions.
1. Introduction
Human beings are social animals whose well-being and mental and physical health depend on having strong social ties. Among all ages, including Older Adults (OAs), social isolation and loneliness are significant yet often overlooked [1]. Individuals who experience loneliness are more likely to engage in less physical exercise, which can worsen the adverse effects of loneliness on health [2]. Engaging in physical activity can contribute to maintaining fitness and good health. Further, exercise can immediately enhance the probability of engagement in beneficial social interactions, such as participating in sports groups [3].
Loneliness can be addressed by a range of interventions, which can be broadly classified into two categories: in-person/social interventions and technological interventions [4]. The social interventions involve direct face-to-face engagement with OAs, such as through workshops and group outings. On the other hand, technological interventions refer to remote interactions facilitated by digital solutions such as text and video messaging.
The acquisition of digital literacy and skills by older adults is a personalised endeavour that includes multiple layers: the level of communities’ policies and strategies to develop and implement digital health and prevent ageism, improved through appropriate learning opportunities; the level of socio-economic and health-related individual barriers and facilitators; and the level of the interaction of the older adult with teachers, trainers and with the actual technologies [5].
In this paper, we propose the Active aGeing And PErsonalised services (AGAPE) framework that combines in-person and technologically personalised interventions to promote socialisation, physical activity and digital literacy, specifically targeting OAs. The main objective of this framework is to improve the digital adoption level of the OA. We have adopted a strategy to promote physical exercise in an attempt to enhance socialisation and thereby improve individuals’ health. As mentioned beforehand, Physical Activity (PA) is a key factor in tackling loneliness. The AGAPE project incorporates remote PA monitoring using two types of wearable devices: a smart fitness band and Inertial Measurement Unit (IMU) sensors positioned on the person’s ankles. These two devices have been empirically validated as accurate methods for measuring physical activity, fall occurrences, gait, and balance [6]. However, there are several hurdles in delivering these in-person and remote interventions and wearable devices to OAs.
Firstly, most OAs have distinct prerequisites, especially in terms of embracing novel technologies and upholding a stringent level of adherence to these technologies [7]. The proposed solution should address the topic of how to create technological applications that are specifically designed for OAs with a high level of accessibility. In addition, we should explore non-intrusive solutions that seamlessly integrate into the daily routine of an OA.
The second challenge involves the implementation of a customized, tailored pathway in active ageing that takes into account the uniqueness of each OA. Combining face-to-face interventions with follow-up with remote interventions is effective for promoting PA in the long term [8]. To address this challenge, the AGAPE framework will offer a personalised and flexible method for combining in-person and remote interventions, considering the distinct requirements and preferences of each OA. The framework seeks to optimise the integration of in-person and remote interventions to enhance sustained participation in PA and enhance overall socialisation and health outcomes.
Thirdly, the challenge for creating an IoT platform for an OA is guaranteeing the seamless integration and compatibility of various IoT devices and platforms. This difficulty is crucial in establishing a unified system that can effectively gather and analyse data from diverse sources, such as fitness bands and IMU sensors [9]. Ensuring interoperability between diverse operating protocols and data formats is of utmost importance. The AGAPE Framework should possess adaptability, scalability, and the ability to integrate future technological improvements seamlessly without causing any disruptions to existing operations.
The contents of this paper are organised into the subsequent sections: Section 1 introduces our work. Section 2 describes the comprehensive methodology of the AGAPE project. Section 3 provides an in-depth description of how the framework was put into practice and presents the outcomes obtained from testing the framework. Section 4 provides a comparison between our suggested solution and other research, highlighting the limitations of our approach. Section 5 serves as the conclusion of the paper.
2. Materials and Methods
2.1. System Architecture
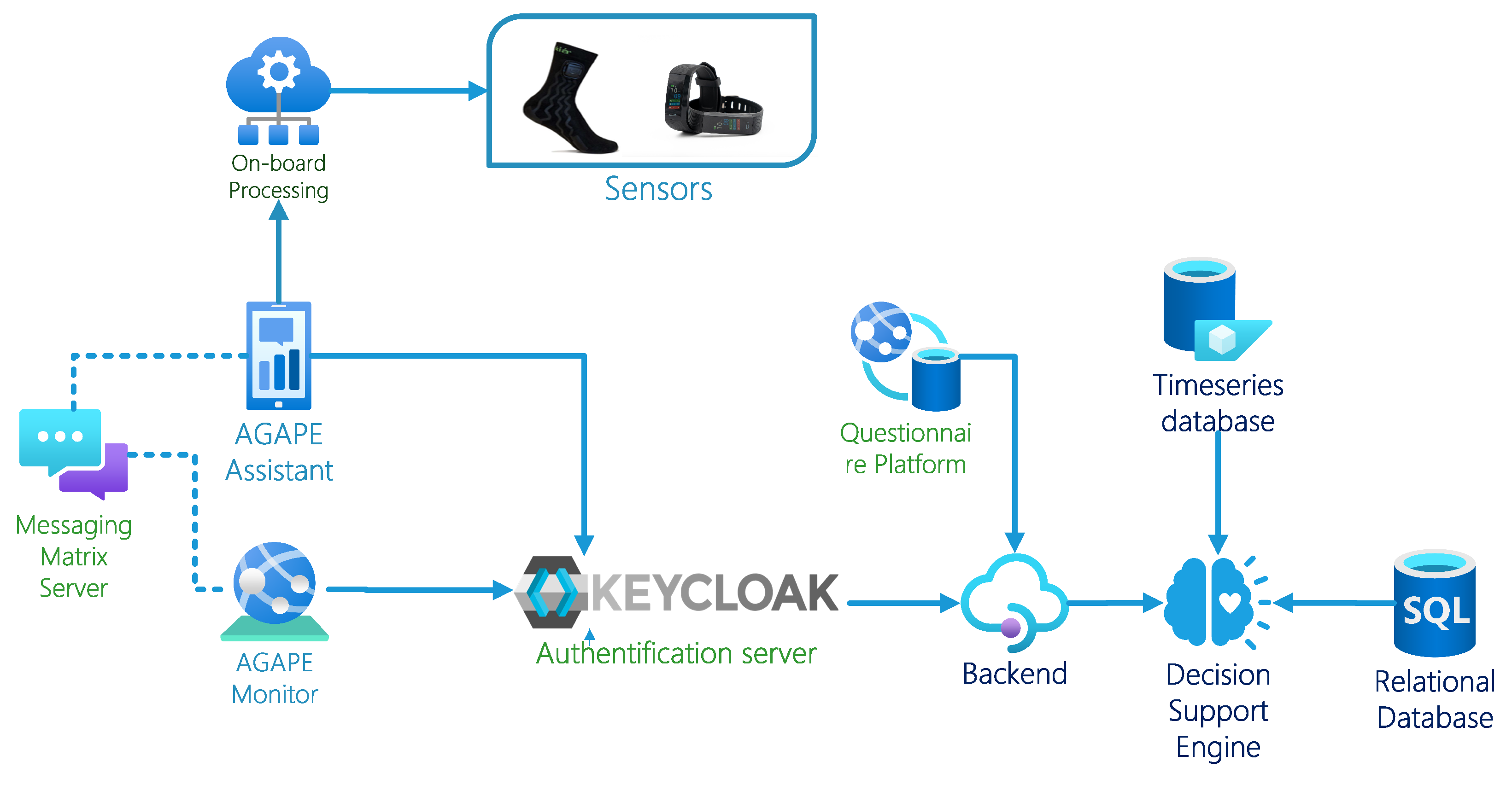
The AGAPE platform is specifically developed to effortlessly combine wearable technology, user involvement, and physical activity tracking to offer a holistic solution for promoting an active and healthy ageing process. The technological architecture of our system is depicted in Figure 1, which highlights the key components and their interconnections. The AGAPE Platform incorporates two primary stakeholders, namely:
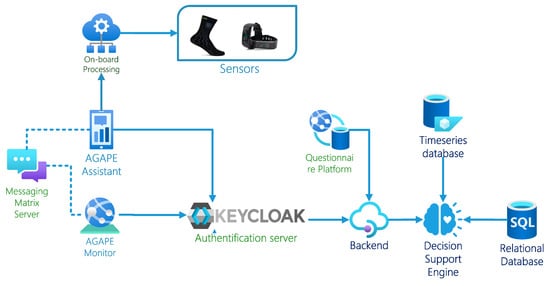
Figure 1.
AGAPE Technical Architecture.
- Older Adults: The platform is specifically designed to be used by all adults who are older than 65 years [10]. Due to the main objectives of this experimentation (feasibility of home-based use of the solution and usability testing), requiring a most objective feedback from testers, the participants were recruited from able-bodied people, with no severe physical- or cognitive-related disability nor presenting severe mood disorders.
- Formal Caregiver: They are caregivers who have undergone specific training and certification to provide professional care services to those who require assistance [11]. They work in various healthcare settings, such as hospitals, nursing homes, and assisted living facilities.
The AGAPE platform comprises the AGAPE Assistant mHealth solution for OAs. This mobile application serves as an IoT hub for all the wearables that were deployed to OAs. The AGAPE Assistant uses the smartphone’s Bluetooth to connect and retrieve the data from the wearable. The application is developed in Flutter and can be deployed on iOS and Android. The application employs a modular design pattern for the IoT Hub (BLoC [12]). The AGAPE Assistant is capable of integrating various sensors from different vendors and can seamlessly incorporate third-party Software Development Kits (SDKs).
For instance, the application has the capability to connect to IMU sensors from two suppliers and two types of fitness bands from two different manufacturers.
To facilitate the integration of new sensors, the AGAPE Assistant analyses the raw data from the accelerometer, gyroscope and magnetometer. Hence, the analysis of these data is independent of the sensors’ supplier. To calculate the OA’s steps, we implemented the established Peak detection technique [13]. The pseudo-code for this algorithm is defined in Algorithm 1. The algorithm is flexible enough to adapt to different sensors based on the accuracy, sampling rate and position where these sensors are placed on the OA. For instance, when an IMU sampling at 50 Hz is positioned on the ankle, the filter index is configured to a value of 0.9, and the time interval between each step is established at 450 ms. The step count is used to compute the OA’s PA level on a daily basis. These data are then transmitted to the backend system for storage in a timeseries database (InfluxDB).
| Algorithm 1 Calculate Step Count Algorithm |
|
The AGAPE platform includes the AGAPE Monitor web application, which is specifically created for formal caregivers. The AGAPE Monitor functions as a Content Management System (CMS) that enables the formal carer to provide technological interventions to OAs. AGAPE Monitor and AGAPE Assistant offer text and message service that are interconnected. This service utilises the open-source Matrix Server, which simplifies the deployment of secure messaging services (end-to-end encryption). In addition, the Matrix Server employs end-to-end encryption to ensure the privacy of every user. The user authentication within the AGAPE platform is overseen by the Keycloak authentication server. Utilizing a unified authentication server enables a cohesive authentication process across multiple apps. The NodeJS backend integrates these data into a SQL relational database for organised storage and a decision support engine for OA profiling.
2.2. Workflow and Intervention Delivery
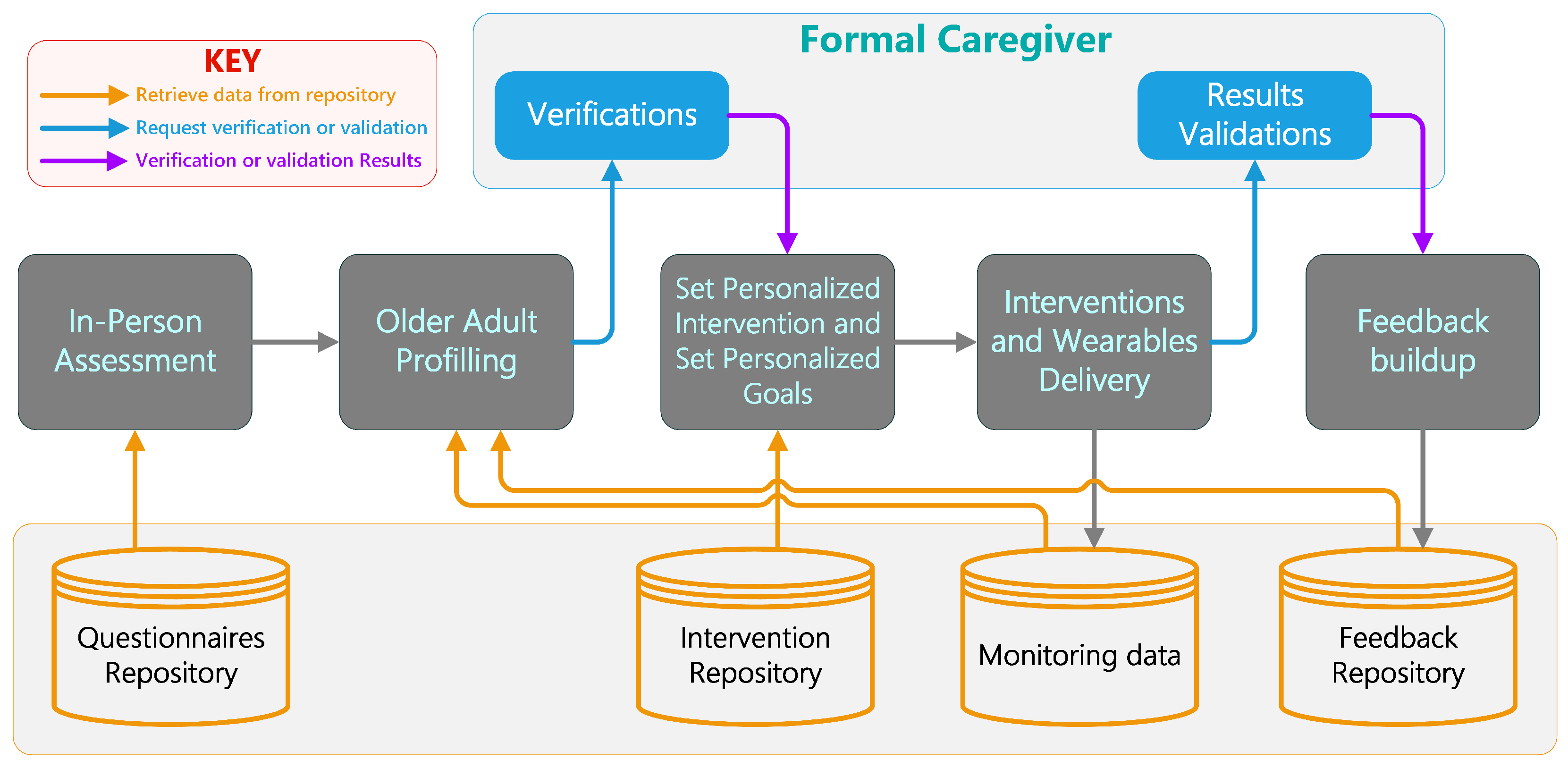
Figure 2 showcases the AGAPE workflow, a multi-step approach designed to deliver tailored care and interventions to older individuals. This is achieved through a series of evaluations, profiling, intervention implementation, and feedback for continual learning. The operational workflow of the AGAPE platform is crucial for understanding how interventions are personalised and delivered to the OA.
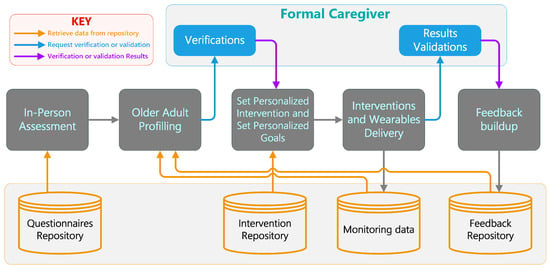
Figure 2.
AGAPE Workflow.
In-Person Assessment: The process begins with an in-person assessment, where data about the OA’s health, preferences, and needs are collected. This step is crucial for gathering baseline information to build the OA’s profile. For this assessment, we have developed a self-assessment questionnaire called the Digital Adoption questionnaire which measures the OA’s familiarity and propensity for using innovative solutions [14]. The Digital Adoption questionnaire measures users’ familiarity with and propensity towards technology use, focusing on their knowledge, confidence and daily application of technology. Its purpose is to classify users into specific adoption profiles based on their digital health literacy, guiding appropriate training. The questionnaire adapts elements from the Technology Acceptance Model (TAM) [15] and the Unified Theory of Technology Acceptance and Use (UTAUT) [16], integrating insights from Alaiad et al. (2019) [17] and Liu et al. (2022) [18] to tailor it to healthcare settings. This adaptation includes new components such as Perceived Ubiquity, Self-Efficacy, and Privacy Concerns, enhancing its relevance and accuracy in predicting technology adoption behaviour in the AGAPE context.
To measure the efficiency, usability and relevance of the platform, we also deliver three questionnaires, namely the System Usability Scale (SUS) [19] for measuring the overall usability of the AGAPE Assistant, the Technostress [20] to measure the stress experienced by the OA towards the use of technological tools like wearables and mobile applications and the Short form User Experience Questionnaire (SUEQ) [21].
Questionnaires Repository: Data from the in-person assessment are stored in a questionnaire repository. This centralised storage ensures that the information is readily accessible for analysis and reference. This repository also contains unstructured information that the Formal Caregivers provide for a specific OA. For example, a specific comorbidity that an OA possesses.
OA Profiling: Based on the initial assessment data, we combine unsupervised and supervised learning techniques on both quantitative and qualitative data, a profile of the OA is created. This profile helps in understanding the individual’s current status based on their needs, capabilities, attitudes and preferences. By categorising users into distinct profiles, AGAPE services can be tuned accordingly, and tailored interventions can be provided to the OA. Each profile is linked to a collection of interventions found in the intervention repository. To enhance the profiling approach, AGAPE utilises data on intervention consumption tracking and feedback gathered from formal carers.
Verifications: However, before delivering the interventions, the formal caregiver verifies if the assigned profile is relevant. If otherwise, the formal caregiver can modify this profile. After this verification process, the set of interventions to be delivered can be further adjusted.
Set of Personalized Intervention and Goals: After verification and using the data from the OA’s profile, personalised interventions are set along with specific, measurable goals. These interventions could range from physical exercises to cognitive activities, depending on the needs and personal preferences identified in the profiling stage. The interventions are selected from the intervention repository.
Intervention Repository: The intervention repository holds various intervention plans and strategies that can be employed. These are selected based on the OA’s profile to ensure they are well-suited to the individual’s needs.
Interventions and Wearables Delivery: The personalized interventions are then delivered to the OA, often with the support of wearable technology that can monitor various health metrics and ensure the interventions are having the desired effect.
Monitoring Data: Data from the wearable devices is continuously collected and monitored. This information is stored in a monitoring data repository for later use in the continual learning process in the OA profiling model.
Results Validations: The effectiveness of the interventions is assessed by analysing the monitoring data. This result validation helps to determine if the goals are being met and if the intervention strategies are successful.
Feedback Buildup: Based on the results of the interventions and the data collected, feedback is generated. This feedback is then used to adjust the interventions as needed, creating a feedback loop that aims to continuously improve the care provided.
2.3. Data Collected by Wearables
The wearables used in the AGAPE platform collect a range of data, including:
- Steps Count: Measures the number of steps taken daily. These data help in assessing the physical activity levels of the older adults.
- Heart Rate: Monitors heart rate variability to assess cardiovascular health. Continuous heart rate monitoring provides insights into the user’s physical condition and can detect irregularities early.
- Standing Up Frequency: Tracks how often users stand up, indicating their level of mobility and activity. Frequent standing up can be an indicator of higher activity levels and better physical health.
- Interactions with AGAPE Assistant: Logs interactions with the mobile app to monitor engagement and usability. These data are crucial for understanding how often and in what ways users are engaging with the technology.
3. Results
The AGAPE Platform is currently being deployed and tested on 112 older adults under the Active aGeing And PErsonalised service’s Ecosystem (AGAPE) project. OAs were recruited across three European regions: Bucharest (Romania), Coimbra (Portugal) and Mugello, Tuscany (Italy). The average age of the recruited OAs was 72.66 (sd = 10.39); the sub-sample within the study population was, in prevalence: married (58%), women (66%), up to secondary education level (34%), retired (90%) and living in a rural environment (54%). This section entails the main results obtained during this experiment.
3.1. Wearable Sensor Deployment
In the AGAPE Platform, wearable sensors, including Sensoria Smart Socks (https://store.sensoriafitness.com/smart-sock-v2-0-sensoria-core (accessed on 14 May 2024)), Sensoria Smartbands (https://store.sensoriafitness.com/sensoria-smart-band/ (accessed on 14 May 2024)), and 9-axis IMU straps, were deployed across all OAs. These devices played a crucial role in monitoring physical activities, such as step count and heart rate, and in assisting OAs in maintaining an active lifestyle. The first connection of the wearables with the AGAPE Assistant was assisted by the formal caregiver. After the initial training phase, the OAs were entirely capable of managing their wearable devices. This includes tasks such as reconnecting the devices to the system as needed and ensuring they are charged regularly. This level of autonomy in handling the technology is a key aspect of the AGAPE platform, facilitating ease of use and ongoing engagement for OA.
3.2. OA Profiling
Basing our strategy on available systematic reviews collectively emphasizing the importance of tailored approaches to improve digital literacy and technology adoption among older adults, considering the diverse barriers and facilitators they face [22,23], we tried to identify a few profiles resulting from the preliminary data (112 rows) collected from the administered Digital Adoption questionnaire. Firstly, an unsupervised learning approach run on our standardized sample showed that four clusters did maximize the fit of the algorithm (silhouette score equal to 0.42). This finding is indeed coherent with what was declared by the scoping review of Wilson et al. (2021), which identified at least three distinct profiles of older adults based on their digital literacy levels [24]. Therefore, a supervised learning technique was applied, based on the four Digital Adoption profiles defined at the consortium level and adjusted by AGAPE professionals and behaviour experts, resulting in an adequate goodness of fit after further applications like cross-validation and dimensionality reduction to increase the algorithm’s robustness (accuracy of the K-Nearest Neighbour algorithm: 70%).
The Table 1 shows the profiles obtained for the experimentation. The questionnaire results are summarised based on nine different behaviour-related areas, namely

Table 1.
Profiles Identified for the AGAPE Platform.
- Effort Expectancy: Perception of the ease of using technology.
- Performance Expectancy: Expectation of the benefits and effectiveness of using technology.
- Social Influence: Influence of social factors (family, friends or trusted people) on technology adoption decisions.
- Perceived Ubiquity: Perception of the availability and prevalence of technology in daily life.
- Self-Efficacy: Confidence in one’s ability to successfully use technology.
- Privacy Concerns: Concerns about the privacy and security implications of using technology.
- Intention to Adopt: Willingness and readiness to adopt and use technology.
- Anxiety: Feelings of unease or discomfort associated with using technology.
- Facilitating Conditions: Perception of the availability of resources and support to use technology effectively.
- Attitude toward Technology: Overall disposition and feelings toward technology usage.
As stated above, for a broader understanding of the OA’s behaviour, their profiling resulting from the digital literacy questionnaire within and between the areas’ analysis is accompanied by individual sessions structured as face-to-face interviews that can ultimately allow for obtaining some valuable qualitative insights into the OA’s personal deeper needs and preferences that are not envisaged to be investigated through written assessment. This eventually allows the AGAPE framework to further tune the personalized intervention selection from the repository.
3.3. AGAPE Assistant
The AGAPE Assistant is an essential element of the AGAPE platform, providing a range of features designed to improve the social interaction and physical well-being of OAs. This smartphone application serves as a central hub for the Internet of Things (IoT), allowing for the integration of different wearable devices and providing personalised experiences based on the detected user profiles.
The integration of wearable sensors with the AGAPE Assistant application enabled efficient data collection and real-time monitoring. Over the course of the pilot testing, we observed an overall increase in physical activity among OAs, as evidenced by a significant rise in daily step counts and active minutes.
The AGAPE Assistant not only serves as an IoT hub, but it is a comprehensive mHealth solution for Active Ageing. The AGAPE Assistant provides content to OAs in order to promote health and digital literacy. This content is fully managed by the formal caregiver through the AGAPE Monitor. In Appendix A, we included the screenshot of both the AGAPE Assistant, AGAPE Monitor and SeniorPhone.
The intuitive design of the AGAPE Assistant’s user interface (UI) significantly contributes to improving the entire user experience, especially for older persons with different levels of technological proficiency. The AGAPE Assistant incorporates concepts for design and features that specifically address the needs of OAs, with a focus on accessibility, user-friendliness, and engagement.
- Simplified Navigation and Large Icons: The AGAPE Assistant features a user-friendly navigation system that includes prominently displayed icons that are easy to identify. This design decision facilitates the navigation of the programme for older folks, particularly those with little digital literacy, by providing them with a user-friendly and intuitive experience. The application features a fixed button located below the content, which has been found to be the most efficient method of navigating in an app for the OA [25].
- High Contrast and Readable Text: The app employs high-contrast colour palettes and utilises large, legible fonts to cater to users with visual impairments. This guarantees that the content is readily legible, hence minimising eye fatigue and enhancing the app’s accessibility.
- Intuitive Layout: The layout of the AGAPE Assistant is designed to be intuitive, with a clear hierarchy of information. Important functions and features are prominently displayed, reducing the cognitive load on users and making it easier for them to find what they need.
- Integration with SeniorPhone App: For users with very low digital literacy, the integration of the SeniorPhone app transforms the traditional Android launcher into a simplified, user-friendly interface. This feature includes large icons, easy navigation, high-contrast colours, and direct access to essential functions like calls, messages and emergency contacts.
The design concepts of the AGAPE Assistant are aimed at ensuring that it effectively caters to the unique requirements of OAs, thereby making it a highly beneficial tool for encouraging an active and healthy ageing process. The emphasis on accessibility, ease of use, and personalization improves user engagement and satisfaction, as evidenced by the comments received from usability evaluations.
3.3.1. Challenges and Adaptations
Throughout the implementation, several challenges were encountered, particularly in the adoption of the technology by OAs with lower digital literacy (A1 and A2) profiles. To address this, the AGAPE Assistant was adapted with a more intuitive interface, and additional training was provided to the OAs by the formal caregiver. Furthermore, the SeniorPhone App (https://seniorsphone.mobi/en/ (accessed on 14 May 2024)) provided by Senlab was integrated into the AGAPE Assitant. The SeniorPhone app transforms the traditional Android launcher into a simplified, user-friendly interface. It is designed for OAs with lower digital literacy, featuring large icons, easy navigation, high-contrast colours and direct access to essential functions like calls, messages, and emergency contacts.
3.3.2. Usability Assessment of AGAPE Assistant
The usability of the AGAPE Assistant application was evaluated using the System Usability Scale (SUS). The SUS is a reliable tool for assessing the usability of a variety of products and services, including hardware, software, mobile devices, websites, and applications. It consists of a 10-item questionnaire with five response options for respondents, from “Strongly agree” to “Strongly disagree”. The SUS provides a “usability score”, which can range from 0 to 100, with higher scores indicating better usability.
The mean SUS score is approximately 64.65. This hovers just below the commonly accepted average usability benchmark of 68, suggesting that while many users find the system reasonably usable, there is notable room for improvement. A significant aspect of the SUS data obtained is the high standard deviation. We expected this high standard deviation regarding the different OA profiles we have identified. Such variability suggests that while some users found the system highly usable (profiles B1 and B2), others struggled with certain aspects of its interface or functionality (profiles A1 and A2).
In summary, the AGAPE Assistant demonstrates a promising level of usability, but with notable variability across users. This comforts the need to provide personalised interventions, particularly for users who find the system less intuitive. The broad range of scores underscores the need for an inclusive design strategy, catering not only to users who are readily adaptable to new technologies, but also to those who may require a more guided and simplified user experience.
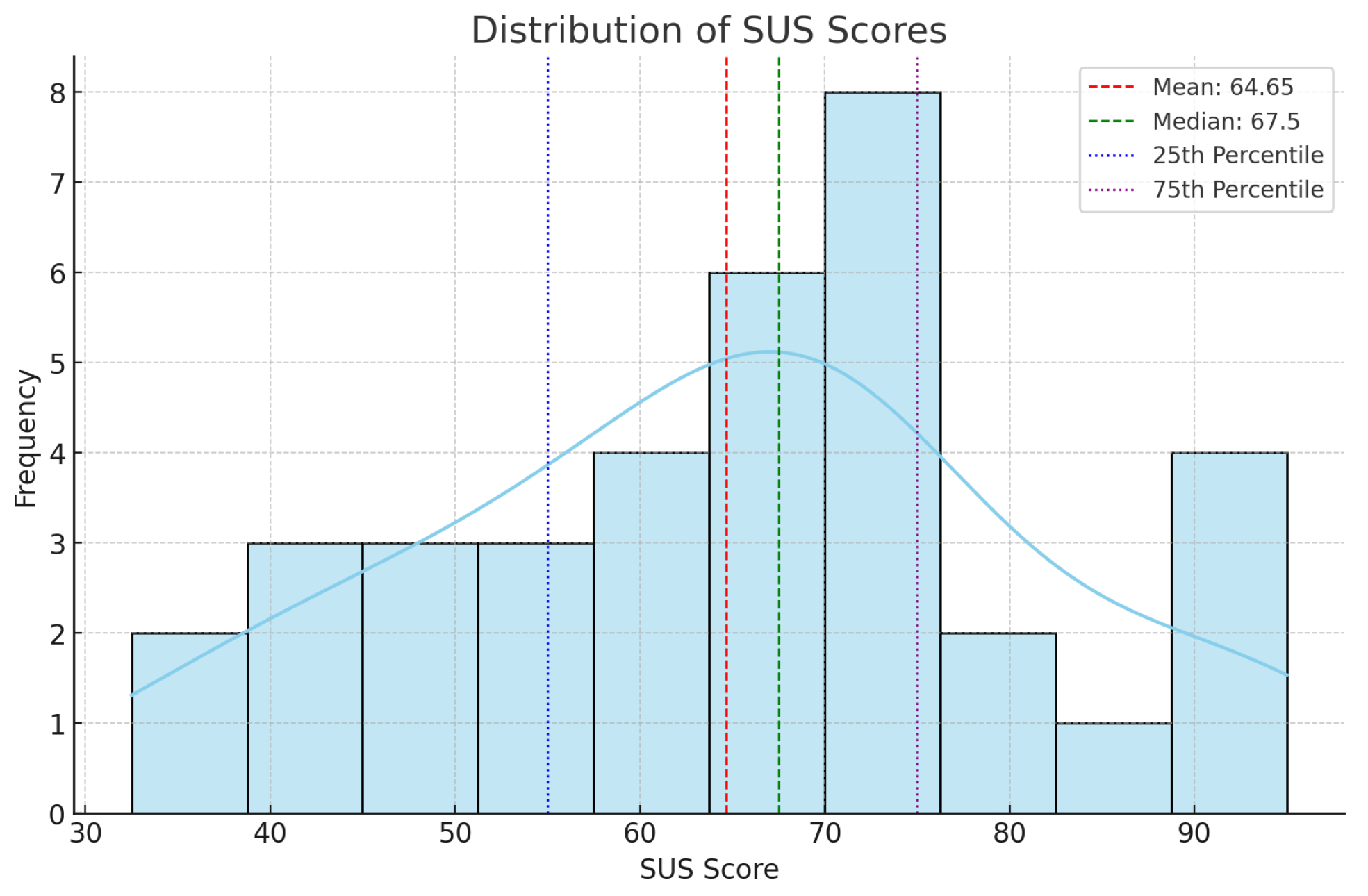
The distribution of SUS scores among the 36 OAs (Figure 3) indicate a varied response to the usability of the platform. The mean SUS score is approximately 64.65. This hovers just below the commonly accepted average usability benchmark of 68, suggesting that while many users find the system reasonably usable, there is notable room for improvement. This score reflects the system’s potential and highlights areas that could be enhanced to elevate user experience.
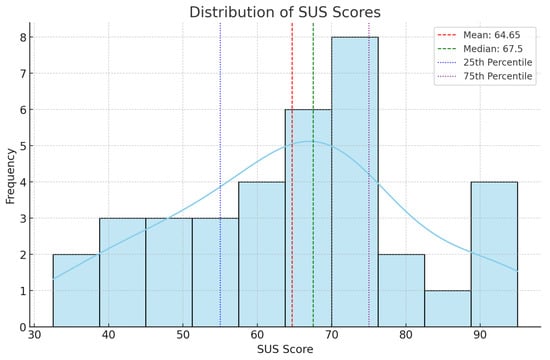
Figure 3.
SUS Score Distribution.
A significant aspect of the SUS data is the high standard deviation of about 16.67. We expected this high standard deviation regarding the different OA profiles we have identified. Such variability suggests that while some users found the system highly usable (profiles B1 and B2), others struggled with certain aspects of its interface or functionality (profiles A1 and A2). This range of user experience, from a low of 32.5 to a high of 95, further emphasises the disparity in usability perceptions.
3.3.3. Technostress Assessment towards Wearables and AGAPE Assistant
The level of technostress experienced by the OA when using the AGAPE Assistant application was evaluated using a dedicated Technostress questionnaire. This tool assesses the stress induced by interacting with technological tools such as wearables and mobile applications. The questionnaire is structured to capture the various dimensions of technostress, offering insights into the participants’ comfort and anxiety levels while using new technologies.
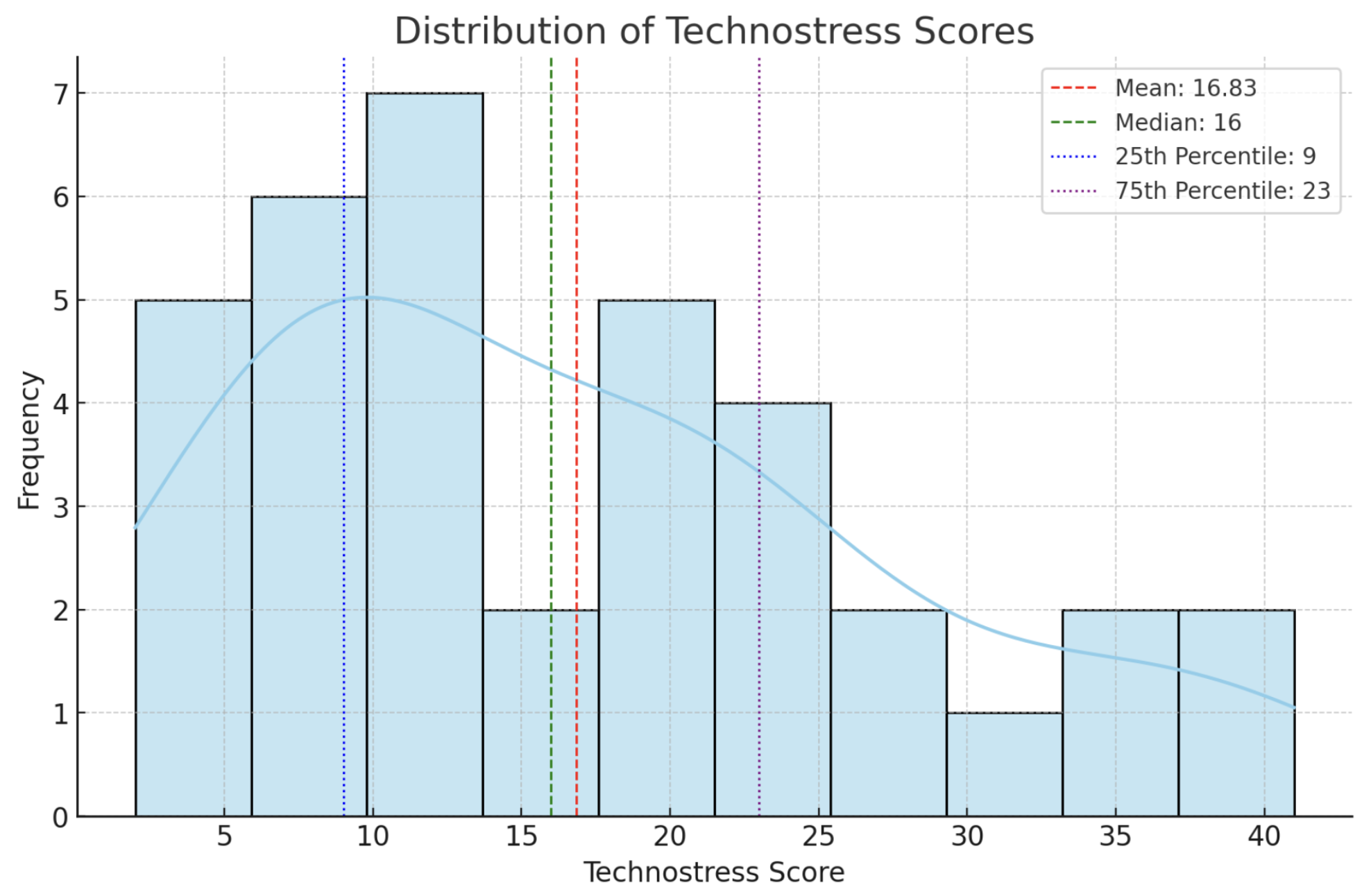
The average technostress score is approximately 16.83, which lies in the lower spectrum, indicating a generally moderate level of stress. However, this average masks the broad range of individual experiences. The standard deviation shows a high variability in the technostress scores. It highlights that while a portion of the participants are relatively comfortable and less stressed with the use of technology (lower scores), others experience higher levels of technostress.
The analysis of the technostress scores (Figure 4) among the OAs in our study reveals a diverse range of experiences with technology-induced stress. The average technostress score is approximately 16.83, which lies in the lower spectrum, indicating a generally moderate level of stress. However, this average masks the broad range of individual experiences.
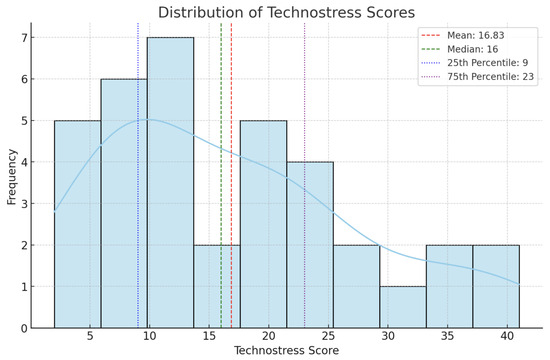
Figure 4.
Technostress Score Distribution.
The standard deviation of about 10.64 points to a high variability in the technostress scores. This wide range of experiences, from a low of 2 to a high of 41, emphasizes the different levels of comfort and anxiety that technology can induce in OAs. It highlights that while a portion of the participants are relatively comfortable and less stressed with the use of technology (lower scores), others experience higher levels of technostress.
A detailed analysis of the SUS and Technostress results for each pilot has been presented and discussed in the paper “Developing an ecosystem of advanced digital services for healthy ageing by a co-creation methodology: preliminary results of the AGAPE project”. The paper is currently “under review” in the PLOS ONE Journal.
3.3.4. Heuristic Evaluation
In order to provide an optimal user–interface interaction, the technology has to comply with a series of rules aimed at enhancing the usability of the product [26]. Various qualitative feedbacks were collected from the OAs. They appreciated the fact that the metaphors used in the solution match the real-world ones, the fact that the solution shows consistency, and that navigating and understanding it requires recognition rather than forcing users to recall the meanings of the icons and tasks to be performed, as well as the meaning of the data shown in apps. Aesthetics and the minimalist design of the AGAPE Assistant are appreciated, as is the fact that the solution promotes learning by doing and helps users adopt new methods of self-management and digital health. The aspects related to the visibility of the system status, user control, in-app documentation, helping the user track actions, making more relevant information visible, simplifying interactions through simple gestures and user motivation are also appreciated, even if they require improvements to optimise user experience. The aspects inquired were included in the interviews after consulting the heuristic principles of digital design for complex systems and the design of digital tools destined to be used by OAs.
3.3.5. Short form User Experience Questionnaire (SUEQ)
The user experience was also evaluated on a qualitative basis using the short form of the User Experience Questionnaire [21]. The SUEQ covers both classical usability aspects and user experience aspects on the following key topics, scaled from −3 (most negative answer) to +3 (most positive answer):
- Obstructive vs. Supportive: This dimension assesses whether users perceive the technology as hindering or facilitating their tasks and activities. Higher scores indicate a more supportive experience, suggesting that users find the technology helpful rather than obstructive.
- Complicated vs. Easy: This dimension gauges the perceived complexity of the technology. Higher scores indicate that users find the technology easy to use and understand, while lower scores suggest a more complicated interface or system.
- Inefficient vs. Efficient: This dimension evaluates the perceived efficiency of the technology in assisting users with their goals. Higher scores indicate that users perceive the technology as effective and efficient in supporting their activities.
- Confusing vs. Clear: This dimension assesses the clarity and comprehensibility of the technology. Higher scores indicate that users find the technology clear and easy to follow, while lower scores suggest confusion or ambiguity in its usage.
- Boring vs. Exciting: This dimension measures the level of engagement and excitement elicited by the technology. Higher scores suggest that users find the technology engaging and stimulating, while lower scores indicate a lack of interest or excitement.
- Not interesting vs. Interesting: This dimension further evaluates the level of interest sparked by the technology. Higher scores indicate that users find the technology interesting and engaging, while lower scores suggest a lack of interest or novelty.
- Conventional vs. Inventive: This dimension assesses whether users perceive the technology as conventional or innovative. Higher scores suggest that users perceive the technology as innovative and inventive, offering new and creative solutions to their needs.
- Usual vs. Leading Edge: This dimension evaluates whether users perceive the technology as standard or cutting-edge. Higher scores indicate that users perceive the technology as advanced and at the forefront of its field.
Upon analysing the SUEQ scores, it is evident that there is a range of responses among the OAs. The scores vary from 33 to 51, with a mean score of 39.21. This variability suggests that individuals may have different perceptions and experiences with integrated technologies and a personalised care approach.
Further examination of the individual SUEQ items reveals specific areas of satisfaction and potential areas for improvement. For instance, items related to usefulness (1, 3, 6) and usability (2, 4, 5) of the technology received relatively high scores, indicating that participants found the system easy to use and valuable in enhancing their daily lives. However, aspects such as aesthetics and content received slightly lower scores, suggesting room for enhancement in the design and information provided by the technology.
Overall, the final SUEQ scores suggest a generally positive perception of the integrated IoT and wearable technologies for personalized elderly care. However, there are opportunities for refinement to better meet the needs and preferences of older adults. Addressing these areas of improvement can lead to a more satisfying and effective solution for promoting active and healthy aging among older adults.
3.4. AGAPE Monitor
3.4.1. Real-Time Monitoring and Analysis
The AGAPE Monitor provides caregivers real-time access to the data collected from the wearable sensors worn by OAs. The data are on the edge of the OA’s smartphone, and then the processed data are ingested by the Node-Red Server to the AGAPE back-end. This feature allows for immediate responses to any significant changes in the physical activity or health status of the OA, thereby enhancing the level of care and attention provided. The AGAPE Monitor also includes profiles of OAs, including their digital technology use profile mentioned before.
3.4.2. Personalised Care Planning
The AGAPE Monitor’s data analysis capabilities extend to the personalisation of care plans. By leveraging the data collected from the wearable sensors, caregivers can tailor their interventions to the specific needs and health statuses of each OA, considering also their digital technology use profiles. Throughout the PA promotion interventions, the formal carers have the ability to establish individualised daily step count objectives for each OA. The AGAPE Assistant app will be updated automatically.
In addition, the formal carer has the ability to oversee all the information that is uploaded to the AGAPE Assistant. To enhance the health literacy of an OA, the carer can choose and share targeted digital information, such as photographs and videos, with the AGAPE Assistant.
3.4.3. Communication and Social Engagement
The platform also enhances the social engagement of an OA. Through its messaging and video calling functionalities, the AGAPE Monitor encourages regular interaction between the OA and their caregivers, promoting social connectivity, which is vital in combating loneliness and isolation among OA.
3.4.4. Outcome Reporting
The AGAPE Monitor generates detailed reports on the health progression and activity levels of OAs. These reports are crucial for evaluating the effectiveness of the interventions and for making informed decisions on future care strategies and can be shared with other healthcare experts. They offer a comprehensive view of the impact that wearable technology and personalised interventions have on the well being of an OA.
3.5. Main Findings
The identification of four distinct profiles among OAs underscores the diversity in digital literacy and attitudes towards technology within this demographic. This diversity necessitates tailored approaches to technology adoption and engagement. Our findings reveal that while some OAs are highly adept at integrating new technologies into their lives, others exhibit apprehension and require more guidance and simplified user experiences.
The System Usability Scale (SUS) and Technostress assessments highlighted significant variability in the OA’s experiences with the AGAPE platform. While the average scores indicated reasonable usability and moderate levels of technostress, the wide range of individual responses pointed to the necessity for personalised interventions. This finding is particularly relevant for users who experience higher levels of technostress or find the system less intuitive.
This study demonstrated that with appropriate training and the introduction of user-friendly applications like the SeniorPhone App, OAs with lower digital literacy can successfully manage and benefit from wearable technologies. This suggests that the barriers to technology adoption in the OA population can be mitigated with targeted support and user-centric design.
4. State of Art and Discussion
Assistive technologies, also known as gerontotechnologies, encompass methods, devices, systems, and IoT-based solutions designed to empower older users to live independently, perform daily activities, and engage in self-care [27]. These technologies include alarms, reminders, sensor-based monitoring and feedback capabilities, and remote communication tools. They assist users as needed, providing support to detect, monitor, and report vital signs and activity patterns, help prevent hazards, and assist in performing complex tasks safely [28].
Smart assistive solutions can bridge the digital divide between older users and younger generations by providing relevant health information, suggesting activity adjustments, and empowering users to share information with family, caregivers, and peers easily [29].
Mobile health, including wearable devices, mobile monitoring systems, and telemedicine, is gaining importance in healthcare for the aging population. Wearable technologies enable continuous monitoring of health parameters such as heart rate, oxygen levels, body temperature, and physical activity, providing significant benefits for early detection and management of chronic conditions [30,31]. Wearables and mobile health technologies facilitate “aging in place” programs, allowing older adults to remain in their home environment while being remotely monitored, thus supporting independence and reducing healthcare costs [32].
4.1. Related Work
The recent advancements in IoT platforms for older persons’ care, as highlighted in studies such as Iranpak et al. [30] and Liu et al. [31], underscore the importance of integrating wearable sensor technologies for real-time health monitoring. Their approaches address challenges posed by isolation and reduced communication among older people, which align with the objectives of the AGAPE platform.
Awadalla et al. [33] emphasize the potential of wearable devices and smartphone applications to enhance the quality of life for older adults by enabling the continuous monitoring of vital health parameters. However, the AGAPE framework extends this concept by incorporating a user-profiling system based on questionnaire responses to tailor the technological experience and interventions. This personalized approach is crucial given the variability in digital literacy and attitudes towards technology among older adults.
Stavrotheodoros et al. [34] highlight the potential of smart-home IoT infrastructure to foster independent living. Their work aligns with the AGAPE framework in utilizing a range of sensors and devices for health and activity monitoring in a non-intrusive manner. Both approaches recognize the significance of the seamless integration of these technologies into daily living environments.
Lorusso et al. [35] conducted a pre-validation of technologies aimed at enhancing both health management and socialization in older adults. The AGAPE platform emphasizes holistic interventions tailored to individual needs and profiles, enhancing usability and ensuring broader and more effective adoption of technology for active ageing.
Baig et al. [36] performed a systematic review on wearable sensors and IoT-based monitoring applications for older adults. The review emphasizes the importance of wearable technology for activity monitoring and independent living. The AGAPE platform’s integration of wearable sensors such as Sensoria Smart Socks aligns with these findings, offering detailed monitoring of physical activity.
Rojo-Perez et al. [37] identified five distinct profiles of active ageing in older adults in Spain. These profiles range from moderate activity with low physical but moderate social and political engagement to profiles characterized by high participation in cognitive and educational activities. This broader perspective can enrich the AGAPE platform’s approach, offering insights into how digital technology interventions could be tailored to the diverse needs and lifestyles of older adults.
Michèle et al. [38] present a comprehensive analysis of older adults’ engagement in social and leisure activities, creating distinct profiles based on their participation patterns. This nuanced understanding of older adults’ lifestyle choices offers valuable parallels to the AGAPE platform, which tailors its technological solutions to suit various user profiles.
Morrow-Howell et al. [39] defined five distinct activity profiles among older adults, ranging from low to high activity and including working and physically active categories. Integrating aspects from physical activity levels could enhance the AGAPE profiling strategy, leading to more tailored and effective interventions.
Cristiano et al. [40] discuss the importance of a user-centred design in developing IoT platforms for elderly care. Their findings align with AGAPE’s approach of involving end-users in the design process to ensure the technology meets their needs and preferences. However, Cristiano’s work emphasizes the broader user acceptance and usability aspects, while AGAPE incorporates these considerations into a more structured profiling and intervention system.
The PHArA-ON project by D’Onofrio et al. [41] also explores integrating multiple technologies, such as AI, robotics, and wearable sensors, to support healthy and active ageing. While both PHArA-ON and AGAPE aim to enhance the quality of life for older adults, PHArA-ON’s approach is broader, incorporating social inclusion and cognitive stimulation through diverse technologies. AGAPE, on the other hand, focuses on the specific needs of older adults through personalized interventions and profiling, which might provide more targeted and effective solutions for individuals with varying levels of digital literacy.
Liu et al. [42] developed an IoT-based health promotion system for seniors that includes three subsystems: physiological information, context awareness service, and elderly nutrition and health promotion. Unlike AGAPE, which focuses heavily on digital literacy and personalized interventions based on user profiles, Liu’s system integrates health promotion modules directly addressing diet and exercise. AGAPE could benefit from this comprehensive approach by incorporating similar nutritional and exercise recommendations, thus enhancing the overall health promotion aspect.
Nebeker et al. [43] investigated the use of mHealth devices to promote independent physical activity among older adults. Their study emphasized participant perceptions of privacy, data management, and usability. While their mHealth intervention successfully increased physical activity, they identified challenges related to device usability and privacy concerns.
The vINCI project, detailed by Spinsante et al. (2023) [44], includes wearable sensors, RGB-depth cameras, and smart insoles, within a cloud-based microservices architecture. This project emphasizes personalized user profiles created through machine learning models analysing health-related quality of life data, similar to AGAPE’s user profiling based on digital literacy and technology adoption. However, vINCI employs blockchain technology for secure data management, an advanced security measure that AGAPE might consider adopting. Both projects prioritize promoting social interactions and physical activity, but vINCI’s comprehensive monitoring through RGB-depth cameras offers a more detailed activity tracking capability compared to AGAPE’s wearable sensors.
Lin et al. [45] explored the adoption of mobile and wearable technology for physical activity among older adults. The study revealed a stage-wise model of technology adoption, emphasizing the importance of awareness, attitudes, appraisals, and initial use in determining long-term adoption. The findings underscored the need for age-specific interventions and highlighted barriers such as established habits and lack of understanding of technology’s benefits, which align with the challenges identified in the AGAPE framework. However, unlike the AGAPE project, Lin’s study primarily focused on the initial phases of technology adoption without integrating a comprehensive intervention strategy to sustain engagement.
Chaparro et al. [46] introduced the SHAPES smart mirror approach, which uses a smart mirror and associated wearable devices to monitor health metrics and promote physical activity among older adults. While the smart mirror provided real-time feedback and motivation, the study pointed out challenges in user interface design and data integration, similar to those addressed by the AGAPE platform. However, the SHAPES approach focused more on the technological interface rather than a holistic intervention framework that includes personalized care and social interaction.
Hvalic-Touzery et al. [47] examined the benefits of wearable activity trackers for older adults, noting improvements in physical activity levels and health outcomes. The study emphasized the role of continuous monitoring and feedback in encouraging activity. While this aligns with the AGAPE platform’s use of wearables for physical activity tracking, Hvalic-Touzery’s research did not incorporate a multi-stakeholder approach involving formal caregivers for personalized intervention planning, which is a distinctive feature of the AGAPE framework.
Talukder et al. [48] propose a model that examines both enablers and inhibitors affecting the continued use intention of wearable health technologies (WHTs) among the elderly. Their findings highlight social value, emotional and epistemic values, and device quality as significant enablers, while inertia and technology anxiety act as inhibitors. The study reveals that emotional value, though a strong predictor, is often under-stimulated in current WHTs, suggesting a need for designs that evoke positive emotions. This emphasises our approach to personalize interventions and user engagement through tailored content and simplified interfaces to mitigate anxiety and enhance continuous use.
4.2. Discussion
The comparative analysis in Table 2 illustrates that the AGAPE platform distinguishes itself from other solutions by providing a comprehensive approach that includes health monitoring, activity tracking, social interaction, personalization, and user profiling. While many solutions focus on one or two aspects, AGAPE’s integrated framework offers a holistic approach to addressing the needs of older adults.
Table 2.
Comparative Analysis of AGAPE and Other Solutions.
Spinsante et al. [44] share similar advantages with the AGAPE platform. Their project also emphasizes personalized user profiles created through machine learning models analysing health-related quality-of-life data. Both platforms prioritize promoting social interactions and physical activity. However, the vINCI project by Spinsante et al. employs advanced technologies such as RGB-depth cameras and blockchain for secure data management. These advanced features provide a more detailed activity tracking capability and enhanced data security. On the other hand, AGAPE’s use of more cost-effective and simpler technologies may offer advantages in terms of accessibility and ease of deployment.
Despite its strengths, the AGAPE platform faces several challenges. One significant challenge is the variability in digital literacy among older adults. While the platform attempts to personalize interventions based on user profiles, the initial learning curve and technology adoption can be daunting for some users. Additionally, ensuring data privacy and security remains a critical concern, especially when integrating multiple IoT devices and platforms. Although the platform emphasizes usability and a user-centred design, continuous feedback and iterative improvements are necessary to cater to the diverse needs of the older population.
The AGAPE framework comprises smart socks and IMU sensors positioned on the ankle. The OAs encountered challenges in wearing these sensors on a regular basis, particularly with the socks in warm and hot weather conditions. The OAs perceived the ankle-mounted IMU sensors to be unfashionable. We are investigating alternative solutions, such as placing an IMU sensor beneath a t-shirt to be more discreet. The step count algorithm requires adjustment to accommodate the sensor’s changing position.
In conclusion, while the AGAPE platform offers a robust and comprehensive solution for promoting active and healthy aging, it must address challenges related to digital literacy, data privacy, and continuous user engagement to maximize its effectiveness and user satisfaction. By learning from the strengths of other solutions such as Spinsante et al.’s project, AGAPE can further enhance its platform to provide even more effective and secure care for older adults.
5. Conclusions
The AGAPE platform, currently in an ongoing pilot involving 112 OAs across three European regions, has demonstrated its potential in advancing active ageing through the use of IoT and wearable technologies. This paper’s distinction is in discovering four distinct profiles among OAs that highlight the diverse technological needs and preferences within this demographic. These profiles, ranging from very low to high digital literacy, highlight the necessity of tailoring innovative solutions to individual user profiles for maximum effectiveness.
However, the results obtained from the System Usability Scale (SUS) and Technostress assessments indicate areas for improvement. The mean SUS score of 64.65, just below the average usability benchmark of 68, along with a high standard deviation of 16.67, suggests significant variability in the platform’s usability among different users. Similarly, the technostress scores, averaging at 16.83 with a standard deviation of 10.64, reveal a range of comfort levels with technology among the participants. These findings highlight the need for ongoing refinement of the AGAPE platform, particularly in enhancing its usability and reducing technostress for users with lower digital literacy.
To further enhance the AGAPE framework, several future directions can be pursued; The AGAPE ecosystem should focus on creating a more intuitive and user-friendly interface, with the aim of making technological advancements accessible and beneficial to a broader range of users. Efforts to mitigate Technostress through personalised training and support can also enhance user experience and acceptance. By addressing these areas, the AGAPE solutions have the potential to become an integral tool in the realm of older age care, promoting active ageing and enriching the lives of OA through technology. This study sets the foundation for such advancements, paving the way for more inclusive and effective active ageing solutions.
The AGAPE ecosystem can incorporate the HL7 FHIR data standards to seamlessly interface with existing Electronic Health Record systems [49]. This would facilitate the effortless exchange of health data across carers and healthcare providers. The integration would enable a comprehensive approach to patient care, enhancing the ability to provide real-time updates and fostering better coordination among many stakeholders engaged in the care of OAs.
The integration of advanced data analytics and artificial intelligence can augment the decision-making capabilities of the AGAPE platform. Forecasting the level of PA in an OA can assist in recognising potential risks and offering timely interventions, hence enhancing health outcomes for senior individuals. In addition, advanced algorithms can be implemented to classify the various PAs performed by the OA. For instance, identify the activities of an individual as either running, walking, or sleeping.
By consistently updating and broadening the selection of wearable devices that are compatible with the AGAPE Assistant, OA will be able to stay up-to-date with the most recent technological advancements. For example, utilising a chest-mounted heart rate sensor can result in more precise heart rate measurements compared to a sensor worn on the wrist. Additionally, this will offer enhanced health monitoring functionalities.
Engaging in partnerships with local community organisations and influential figures can facilitate the comprehension of the distinct requirements and preferences of various demographic cohorts. This participation can help promote the adoption and acceptance of the AGAPE ecosystem within these communities. For example, the AGAPE ecosystem is currently undergoing testing in three different countries, but we have intentions to expand this testing to additional countries.
Author Contributions
Conceptualization, J.S.J., I.C. and F.A.; methodology, J.S.J.; software, J.S.J., F.A., D.N. and J.L.; validation, E.T., F.C. and D.K.; formal analysis, J.S.J. and C.P.; investigation, I.C., C.P., B.F. and A.P.; data curation, I.C., C.P. and A.P.; writing—original draft preparation, J.S.J., F.A. and I.C.; writing—review and editing, I.C., B.F. and F.C.; supervision, E.T., F.C., M.B. and D.K.; project administration, E.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by European Commission grant number AAL-2021-8-124-CP and FNR grant number 16457409.
Institutional Review Board Statement
The AGAPE research activities involving human participants have been approved by the ethical organisms in Italy (Approval of the Comitato Etico Nazionale per la Sperimentazione Clinica della Regione Toscana n.23452spe/31 May 2023), Portugal (Approved by Regional Health Administration of the Center, Portugal (January 2023), obtained on 20 April 2023) and Romania (Approval of the Institutional Ethical Commission of Elias University Hospital in Bucharest, letter 11002-6/10.02.2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy.
Conflicts of Interest
Francesco Agnoloni, Jure Lampe and Elena Tamburini was employed by the company SenLab d.o.o and Medea S.r.l. The remaining authors declare that the re-search was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| OA | Older Adult |
| IoT | Internet of Things |
| AGAPE | Connected Health and Social Engagement Framework for Technology Adoption |
| IMU | Inertial Measurement Unit |
Appendix A
Figure A1 shows the AGAPE Assistant mobile application running on an Android device in the front. The AGAPE Assistant is linked to the Sensoria Smart Socks, which record the number of steps taken and the frequency of standing up. The AGAPE Monitor web application displays real-time data transferred from the AGAPE Assistant to the AGAPE Monitor. The AGAPE Monitor includes a radar chart that displays the evaluation subjects used to construct the OA profile. Figure A2 shows the connection screen of the AGAPE Assistant app to connect the different sensors, and finally, Figure A3 shows the SeniorPhone app and the integration with AGAPE Assistant.
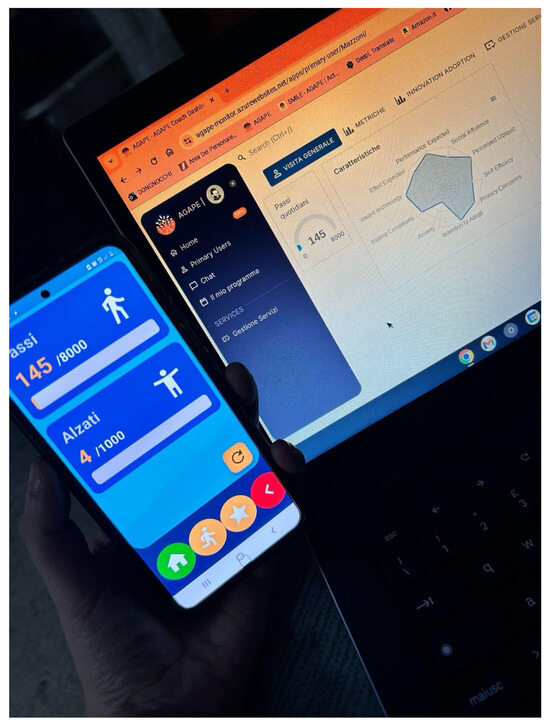
Figure A1.
The AGAPE Assistant connected to the wearable and transferring the data in real-time to the AGAPE Monitor.
Figure A1.
The AGAPE Assistant connected to the wearable and transferring the data in real-time to the AGAPE Monitor.
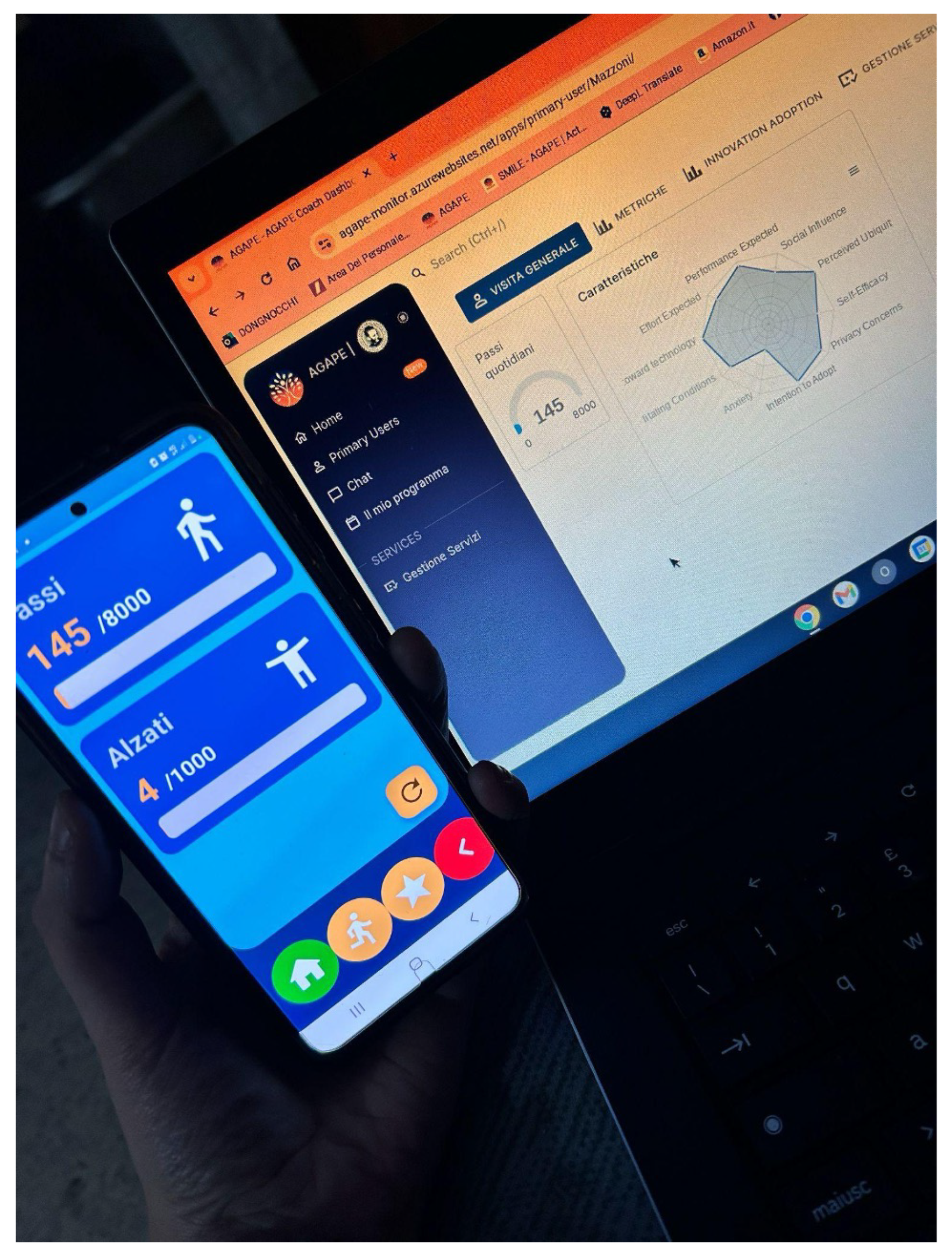
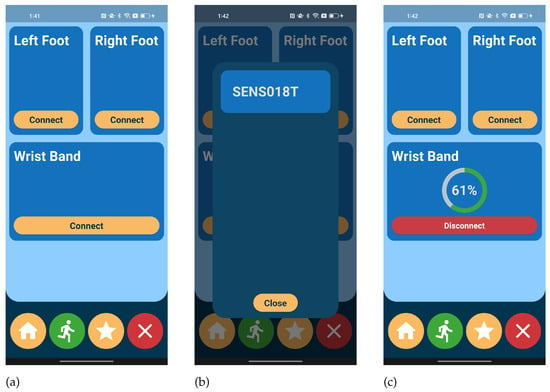
Figure A2.
Screenshots of the AGAPE Assistant mHealth: (a) The Sensor connection screen for multiple sensor connection, (b) the Device Scanning screen that shows nearby sensors available to be connected by Bluetooth, (c) A wristband connected showing the battery level of the band.
Figure A2.
Screenshots of the AGAPE Assistant mHealth: (a) The Sensor connection screen for multiple sensor connection, (b) the Device Scanning screen that shows nearby sensors available to be connected by Bluetooth, (c) A wristband connected showing the battery level of the band.
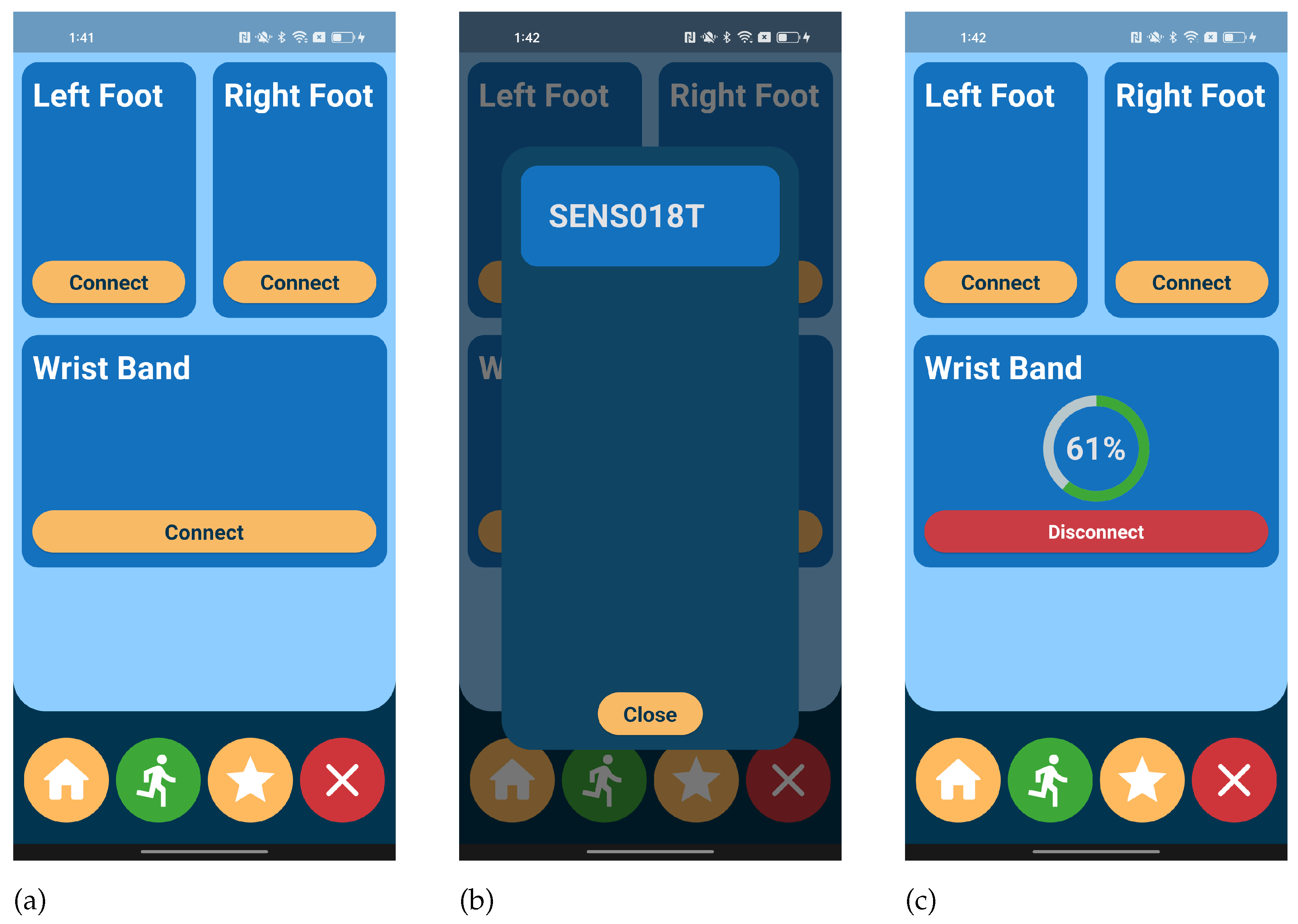

Figure A3.
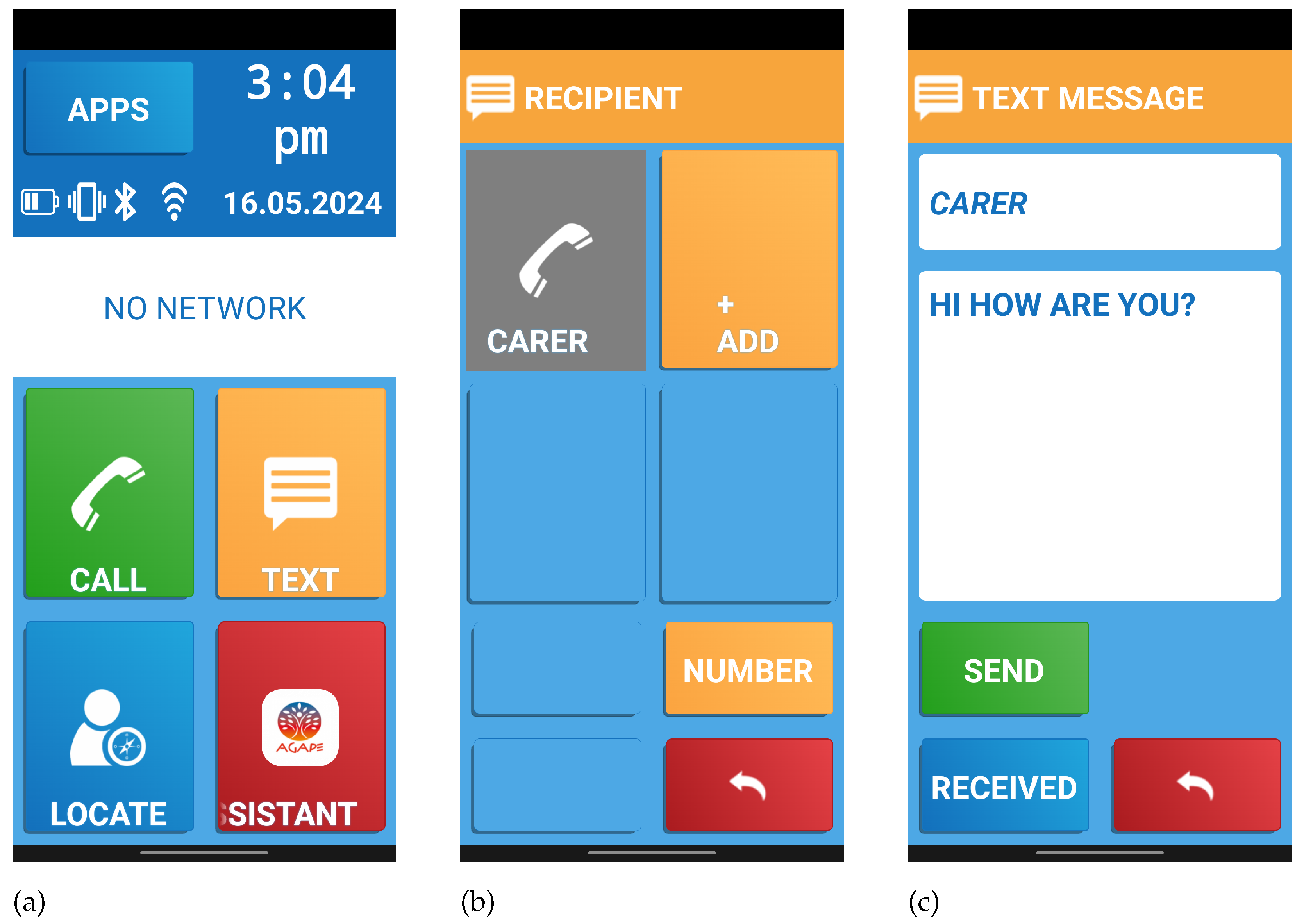
Screenshots of SeniorPhone: (a) Homepage of SeniorPhone that automatically integrates the AGAPE Assistant icon, (b) Simple contact list to contact the carer inn a pre-built contact list, (c) Simple message composition screen though text messaging.
Figure A3.
Screenshots of SeniorPhone: (a) Homepage of SeniorPhone that automatically integrates the AGAPE Assistant icon, (b) Simple contact list to contact the carer inn a pre-built contact list, (c) Simple message composition screen though text messaging.
Appendix B
The Table A1 provides a sample of the data collected from one of the participants using the AGAPE platform. These data include step count, heart rate, and the number of interactions with the AGAPE Assistant. This table illustrates the type of data collected daily, which is used to monitor the physical activity and health status of the participants.
Table A1.
Sample Data Collected from AGAPE Platform.
Table A1.
Sample Data Collected from AGAPE Platform.
| Date | Steps | Heart Rate (bpm) | Standing Up Frequency | Interactions with AGAPE Assistant |
|---|---|---|---|---|
| 1 April 2023 | 5678 | 72 | 8 | 15 |
| 2 April 2023 | 6210 | 75 | 10 | 18 |
| 3 April 2023 | 4832 | 70 | 7 | 12 |
| 4 April 2023 | 7350 | 78 | 12 | 20 |
| 5 April 2023 | 4980 | 74 | 9 | 16 |
References
- Social Isolation and Loneliness. 2024. Available online: https://www.who.int/teams/social-determinants-of-health/demographic-change-and-healthy-ageing/social-isolation-and-loneliness (accessed on 18 March 2024).
- Ahn, J.; Falk, E.B.; Kang, Y. Relationships between physical activity and loneliness: A systematic review of intervention studies. Curr. Res. Behav. Sci. 2024, 6, 100141. [Google Scholar] [CrossRef]
- Basterfield, L.; Burn, N.L.; Galna, B.; Karoblyte, G.; Weston, K.L. The association between physical fitness, sports club participation and body mass index on health-related quality of life in primary school children from a socioeconomically deprived area of England. Prev. Med. Rep. 2021, 24, 101557. [Google Scholar] [CrossRef]
- Masi, C.M.; Chen, H.Y.; Hawkley, L.C.; Cacioppo, J.T. A meta-analysis of interventions to reduce loneliness. Pers. Soc. Psychol. Rev. 2011, 15, 219–266. [Google Scholar] [CrossRef]
- Karna, E.; Aavikko, L.; Rohner, R.; Gallistl, V.; Pihlainen, K.; Muller, C.; Ehlers, A.; Bevilacqua, R.; Strano, S.; Maranesi, E.; et al. A Multilevel Model of Older Adults’ Appropriation of ICT and Acquisition of Digital Literacy. Int. J. Environ. Res. Public Health 2022, 19, 15714. [Google Scholar] [CrossRef]
- Kristoffersson, A.; Lindén, M. A Systematic Review of Wearable Sensors for Monitoring Physical Activity. Sensors 2022, 22, 573. [Google Scholar] [CrossRef]
- Fang, Y.M.; Chang, C.C. Users’ psychological perception and perceived readability of wearable devices for elderly people. Behav. Inf. Technol. 2016, 35, 225–232. [Google Scholar] [CrossRef]
- Yamatsu, K.; Narazaki, K. Feasibility of the Remote Physical Activity Follow-Up Intervention after the Face-to-Face Program for Healthy Middle-Aged Adults: A Randomized Trial Using ICT and Mobile Technology. Int. J. Environ. Res. Public Health 2022, 19, 4922. [Google Scholar] [CrossRef]
- Kumar, K.; Kumar, A.; Kumar, N.; Mohammed, M.A.; Al-Waisy, A.S.; Jaber, M.M.; Shah, R.; Al-Andoli, M.N. Dimensions of Internet of Things: Technological Taxonomy Architecture Applications and Open Challenges—A Systematic Review. Wirel. Commun. Mob. Comput. 2022, 2022, 9148373. [Google Scholar] [CrossRef]
- Orimo, H. Reviewing the definition of elderly. Nihon Ronen Igakkai Zasshi 2006, 43, 27–34. [Google Scholar] [CrossRef]
- 4 Different Types of Caregivers. Available online: https://www.nautilusshc.com/blog/4-types-of-caregivers (accessed on 20 March 2024).
- Bloc State Management Library. 2024. Available online: https://bloclibrary.dev (accessed on 20 March 2024).
- Yang, X.; Huang, B. An accurate step detection algorithm using unconstrained smartphones. In Proceedings of the 27th Chinese Control and Decision Conference (2015 CCDC), Qingdao, China, 23–25 May 2015; pp. 5682–5687. [Google Scholar] [CrossRef]
- Nugent, C.; Cleland, I.; Nugent, L.; Estevez, M.E.; Lendinez, A.M.; Craig, D.; Agnoloni, F.; Tamburini, E. Using Generative AI to Assist with Technology Adoption Assessment. In International Conference on Ubiquitous Computing and Ambient Intelligence; Springer: Cham, Switzerland, 2023; pp. 202–207. [Google Scholar]
- Davis, F.D. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989, 13, 319–340. [Google Scholar] [CrossRef]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User acceptance of information technology: Toward a unified view. MIS Q. 2003, 13, 425–478. [Google Scholar] [CrossRef]
- Alaiad, A.; Alsharo, M.; Alnsour, Y. The determinants of m-health adoption in developing countries: An empirical investigation. Appl. Clin. Inform. 2019, 10, 820–840. [Google Scholar] [CrossRef]
- Liu, Y.; Lu, X.; Zhao, G.; Li, C.; Shi, J. Adoption of mobile health services using the unified theory of acceptance and use of technology model: Self-efficacy and privacy concerns. Front. Psychol. 2022, 13, 944976. [Google Scholar] [CrossRef]
- Brooke, J. SUS: A quick and dirty usability scale. Usability Eval. Ind. 1995, 189, 4–7. [Google Scholar]
- Ragu-Nathan, T.S.; Tarafdar, M.; Ragu-Nathan, B.S.; Tu, Q. The Consequences of Technostress for End Users in Organizations: Conceptual Development and Empirical Validation. Inf. Syst. Res. 2008, 19, 417–433. [Google Scholar] [CrossRef]
- Schrepp, M.; Hinderks, A.; Thomaschewski, J. Applying the User Experience Questionnaire (UEQ) in Different Evaluation Scenarios. In Design, User Experience, and Usability. Theories, Methods, and Tools for Designing the User Experience; Marcus, A., Ed.; Springer: Cham, Switzerland, 2014; pp. 383–392. [Google Scholar]
- Oh, S.S.; Kim, K.A.; Kim, M.; Oh, J.; Chu, S.H.; Choi, J. Measurement of digital literacy among older adults: Systematic review. J. Med. Internet Res. 2021, 23, e26145. [Google Scholar] [CrossRef] [PubMed]
- Xie, L.; Zhang, S.; Xin, M.; Zhu, M.; Lu, W.; Mo, P.K.H. Electronic health literacy and health-related outcomes among older adults: A systematic review. Prev. Med. 2022, 157, 106997. [Google Scholar] [CrossRef]
- Wilson, J.; Heinsch, M.; Betts, D.; Booth, D.; Kay-Lambkin, F. Barriers and facilitators to the use of e-health by older adults: A scoping review. BMC Public Health 2021, 21, 1556. [Google Scholar] [CrossRef]
- Rivas, A.; Antoun, C.; Feuer, S.; Mathew, T.; Nichols, E.; Olmsted-Hawala, E.; Wang, L. Comparison of Three Navigation Button Designs in Mobile Survey for Older Adults. Surv. Pract. 2022, 15, 1–14. [Google Scholar] [CrossRef]
- Nielsen, J.; Molich, R. Heuristic evaluation of user interfaces. In Proceedings of the CHI ’90: Conference on Human Factors in Computing, Seattle, WA, USA, 1–5 April 1990; pp. 249–256. [Google Scholar] [CrossRef]
- Blackman, S.; Matlo, C.; Bobrovitskiy, C.; Waldoch, A.; Fang, M.L.; Jackson, P.; Mihailidis, A.; Nygård, L.; Astell, A.; Sixsmith, A. Ambient Assisted Living Technologies for Aging Well: A Scoping Review. J. Intell. Syst. 2016, 25, 55–69. [Google Scholar] [CrossRef]
- Alexandru, A.; Ianculescu, M. Enabling Assistive Technologies to Shape the Future of the Intensive Senior-Centred Care: A Case Study Approach. Stud. Inform. Control 2017, 26, 343–352. [Google Scholar] [CrossRef]
- Nunes, F.; Verdezoto, N.; Fitzpatrick, G.; Kyng, M.; Grönvall, E.; Storni, C. Self-Care Technologies in HCI. ACM Trans. Comput.-Hum. Interact. 2015, 22, 1–45. [Google Scholar] [CrossRef]
- Iranpak, S.; Shahbahrami, A.; Shakeri, H. Remote patient monitoring and classifying using the internet of things platform combined with cloud computing. J. Big Data 2021, 8, 120. [Google Scholar] [CrossRef]
- Liu, Q.; Sun, S.; Yuan, X.; Zhang, Y. Ambient backscatter communication-based smart 5G IoT network. EURASIP J. Wirel. Commun. Netw. 2021, 2021, 34. [Google Scholar] [CrossRef]
- Malwade, S.; Abdul, S.S.; Uddin, M.; Nursetyo, A.A.; Fernandez-Luque, L.; Zhu, X.; Cilliers, L.; Wong, C.P.; Bamidis, P.; Li, Y.C. Mobile and wearable technologies in healthcare for the ageing population. Comput. Methods Programs Biomed. 2018, 161, 233–237. [Google Scholar] [CrossRef]
- Awadalla, M.; Kausar, F.; Ahshan, R. Developing an IoT Platform for the Elderly Health Care. Int. J. Adv. Comput. Sci. Appl. 2021, 12. [Google Scholar] [CrossRef]
- Stavrotheodoros, S.; Kaklanis, N.; Votis, K.; Tzovaras, D. A Smart-Home IoT Infrastructure for the Support of Independent Living of Older Adults. In IFIP Advances in Information and Communication Technology; Springer: Cham, Switzerland, 2018; pp. 238–249. [Google Scholar] [CrossRef]
- Lorusso, L.; Mosmondor, M.; Grguric, A.; Toccafondi, L.; D’Onofrio, G.; Russo, S.; Lampe, J.; Pihl, T.; Mayer, N.; Vignani, G.; et al. Design and Evaluation of Personalized Services to Foster Active Aging: The Experience of Technology Pre-Validation in Italian Pilots. Sensors 2023, 23, 797. [Google Scholar] [CrossRef]
- Baig, M.M.; Afifi, S.; GholamHosseini, H.; Mirza, F. A Systematic Review of Wearable Sensors and IoT-Based Monitoring Applications for Older Adults - a Focus on Ageing Population and Independent Living. J. Med. Syst. 2019, 43, 233. [Google Scholar] [CrossRef] [PubMed]
- Rojo-Perez, F.; Rodriguez-Rodriguez, V.; Molina-Martinez, M.A.; Fernandez-Mayoralas, G.; Sanchez-Gonzalez, D.; Rojo-Abuin, J.M.; Ayala, A.; Rodriguez-Blazquez, C.; Calderon-Larranaga, A.; Ribeiro, O.; et al. Active ageing profiles among older adults in Spain: A Multivariate analysis based on SHARE study. PLoS ONE 2022, 17, e0272549. [Google Scholar] [CrossRef]
- Michele, J.; Guillaume, M.; Alain, T.; Nathalie, B.; Claude, F.; Kamel, G. Social and leisure activity profiles and well-being among the older adults: A longitudinal study. Aging Ment. Health 2019, 23, 77–83. [Google Scholar] [CrossRef]
- Morrow-Howell, N.; Putnam, M.; Lee, Y.S.; Greenfield, J.C.; Inoue, M.; Chen, H. An investigation of activity profiles of older adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2014, 69, 809–821. [Google Scholar] [CrossRef] [PubMed]
- Cristiano, A.; Musteata, S.; De Silvestri, S.; Bellandi, V.; Ceravolo, P.; Cesari, M.; Azzolino, D.; Sanna, A.; Trojaniello, D. Older Adults’ and Clinicians’ Perspectives on a Smart Health Platform for the Aging Population: Design and Evaluation Study. JMIR Aging 2022, 5, e29623. [Google Scholar] [CrossRef] [PubMed]
- D’Onofrio, G.; Fiorini, L.; Toccafondi, L.; Rovini, E.; Russo, S.; Ciccone, F.; Giuliani, F.; Sancarlo, D.; Cavallo, F. Pilots for Healthy and Active Ageing (PHArA-ON) Project: Definition of New Technological Solutions for Older People in Italian Pilot Sites Based on Elicited User Needs. Sensors 2021, 22, 163. [Google Scholar] [CrossRef]
- Liu, C.H.; Tu, J.F. Development of an IoT-Based Health Promotion System for Seniors. Sustainability 2020, 12, 8946. [Google Scholar] [CrossRef]
- Nebeker, C.; Zlatar, Z.Z. Learning From Older Adults to Promote Independent Physical Activity Using Mobile Health (mHealth). Front. Public Health 2021, 9, 703910. [Google Scholar] [CrossRef]
- Spinsante, S.; Poli, A.; Mongay Batalla, J.; Krawiec, P.; Dobre, C.; Bǎjenaru, L.; Mavromoustakis, C.X.; Costantinou, C.S.; Molan, G.; Herghelegiu, A.M.; et al. Clinically-validated technologies for assisted living. J. Ambient. Intell. Humaniz. Comput. 2023, 14, 2095–2116. [Google Scholar] [CrossRef]
- Lin, S.H. Adoption of Mobile and Wearable Technology for Older Adults’ Physical Activity: A Preliminary Model. J. Consum. Health Internet 2023, 27, 139–155. [Google Scholar] [CrossRef]
- Chaparro, J.D.; Ruiz, J.F.B.; Romero, M.J.S.; Peño, C.B.; Irurtia, L.U.; Perea, M.G.; Garcia, X.D.T.; Molina, F.J.V.; Grigoleit, S.; Lopez, J.C. The SHAPES Smart Mirror Approach for Independent Living, Healthy and Active Ageing. Sensors 2021, 21, 7938. [Google Scholar] [CrossRef]
- Hvalič-Touzery, S.; Šetinc, M.; Dolničar, V. Benefits of a Wearable Activity Tracker with Safety Features for Older Adults: An Intervention Study. Int. J. Environ. Res. Public Health 2022, 19, 15723. [Google Scholar] [CrossRef]
- Talukder, M.S.; Laato, S.; Islam, A.K.M.N.; Bao, Y. Continued use intention of wearable health technologies among the elderly: An enablers and inhibitors perspective. Int. Res. 2021, 31, 1611–1640. [Google Scholar] [CrossRef]
- Index—FHIR v5.0.0. 2024. Available online: http://hl7.org/fhir (accessed on 17 May 2024).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).