Abstract
The use of beverages containing caffeine has increased significantly in recent years due to their stimulant effects. The aim of this study was to determine the possible adverse effects of caffeine and taurine on young adults’ cardiovascular systems using linear and nonlinear parameters for this analysis. This study was carried out with 56 students from Aydın Adnan Menderes University. The participants were divided into four main groups: caffeine, taurine, caffeine + taurine, and a control. Blood pressure and electrocardiogram measurements were performed before the ingredients were consumed. After 30 and 60 min, the measurements were repeated. Linear and nonlinear analyses were performed on the heart rate variability data 60 min after consumption. Compared with taurine and the combination of caffeine + taurine, caffeine was found to have the most adverse effects on the hemodynamic parameters and the linear and nonlinear parameters of heart rate variability in the young adult participants. It was also found that the presence of taurine may have repressed the adverse effects of caffeine.
1. Introduction
Caffeine and taurine are major components of energy drinks, which have been reported to be frequently consumed by students, athletes, and individuals between the ages of 21 and 35 [1]. A clinical review on the adverse effects of energy drinks reported that more than 50% of current status reports were related to the cardiovascular system, followed by neurological problems [2]. For such reasons, it is important to investigate the beneficial and adverse effects of energy drinks and of caffeine and taurine, which are dominant in energy drinks, on young adults in particular.
Caffeine, the most dominant component of energy drinks, is a xanthine that affects GABA inhibition, phosphodiesterase modulation, and A2 adenosine receptor antagonism [3]. It stimulates the central nervous system and becomes toxic when taken in high doses [4]. Taurine, on the other hand, is a non-essential amino acid that is found in high concentrations in the brain and acts as both a neuromodulator and a neurotransmitter [5]. It is also known that taurine has beneficial effects on the cardiovascular system [6]. Although taurine administration has been shown to reduce blood pressure and has antiarrhythmic properties [7], it has been reported that higher doses of taurine reverse these benefits [8].
Studies have been conducted on caffeinated beverages, but their effects on the human body are not fully known. For example, Çalışkan et al. [9] reported in their study that caffeinated beverages have adverse effects on the cardiovascular system, and, as a result, this opinion has spread, but it has not achieved certainty. To obtain clearer and more detailed information, the cardiovascular effects of the ingredients in energy drinks should be examined separately. There are very few such studies in the literature [10,11]. For example, Bichler et al. [5] reported that they observed an increase in blood pressure 70 min after the administration of 100 mg caffeine and 1000 mg taurine capsules. Moreover, there are several studies that have investigated the effects of caffeine on exercise [12,13,14], one of which reported that when caffeine and taurine were administered together, they had an increasing effect on cardiac contractility parameters after exercise [15].
Heart rate variability (HRV) is a physiological metric that is regulated by the autonomic nervous system and is related to sympathetic and parasympathetic activity [16]. In the literature, time-domain and frequency-domain analyses, which are linear analysis methods, are generally used to examine HRV. Conventional time-domain indexes such as the standard deviation of normal-to-normal RR intervals (SDNN), the total number of adjacent RR intervals with a difference in duration greater than 50 ms (NN50), and the root-mean square of differences between adjacent normal RR intervals in a time interval (RMSSD) are the first used indexes for HRV analysis and are statistical calculations of consecutive RR intervals [17]. These parameters are usually used to identify risk stratification in cardiovascular diseases and general mortality [18]. Frequency-domain indexes are based on power spectral density analysis and estimate the absolute power in four frequency bands: ultra low frequency (ULF (≤0.003 Hz)), very low frequency (VLF (0.0033–0.04 Hz)), low frequency (LF (0.04–0.15 Hz)) and high frequency (HF (0.15–0.40 Hz)) [19]. HF and LF fluctuations reflect the variations in heart rate that are related to the respiratory cycle and baroreceptor activity during resting conditions, respectively [19]. Since HRV signals are complex and unpredictable, linear methods that focus only on sympathovagal balance assessments and first- and second-order statistics are inadequate to measure them. Nonlinear methods are extensively used to overcome this deficiency. Nonlinear measurements index the unpredictability of a time series, which results from the complexity of the mechanisms that regulate HRV, and they might provide beneficial information for the physiological interpretation of HRV [20]. Various nonlinear methods are used to analyze RR interval dynamics, such as power-law analysis, geometrical analysis, and phase space reconstruction (PSR). Since HRV depends on too many parameters, analyzing it accurately is very complicated; however, phase space reconstruction has a great advantage compared to other methods, as it can be performed when a parameter is recorded for a sufficient time interval. When HRV is reconstructed in the phase space, various nonlinear indices, such as the largest Lyapunov exponent, correlation dimension, and approximate entropy, can be calculated from the generated attractor. These nonlinear parameters can provide information about variations in the system’s complexity, which cannot be obtained using linear methods. A few studies have used PSR for analysis in different states [21,22].
While there are limited studies that have used linear analysis methods to investigate the effects of energy drinks on the cardiovascular system [23,24], those using nonlinear analysis methods are even more scarce. In the literature, Caliskan and Bilgin [25] reported that energy drinks increased the complexity of the cardiovascular system, examining the electrocardiogram signals recorded from young adults using phase space reconstruction. Additionally, Yeragani et al. [26] and Papaioannou et al. [27] investigated the nonlinear dynamics of HRV and blood pressure after caffeine ingestion, respectively, while Yeragani et al. [26] and Papaioannou et al. [27] only investigated the approximate entropy when conducting nonlinear analysis of HRV and blood pressure. However, to obtain more comprehensive information about nonlinear dynamics, it is necessary to examine more varied nonlinear parameters. In the literature, no study was found in which the effects of energy drink components on the cardiovascular system were examined using both linear and nonlinear analysis methods; this study, which aims to do so, will be the first of its kind. In addition, by analyzing more nonlinear parameters such as the largest Lyapunov exponent, correlation dimension, and Hurst exponent, we aim to obtain more information about the dynamics of the cardiovascular system under the influence of caffeine and taurine. In this way, information that cannot be obtained using linear methods will be obtained using comprehensive nonlinear analysis. From another perspective, we aim to obtain more detailed and comprehensive information about the possible effects of caffeine and taurine through the dynamic and unpredictable nature of the system and about how safe these ingredients are for young adults.
2. Materials and Methods
2.1. Participants
Fifty-six volunteers (16 female (F), 40 male (M)) aged 18–24 sourced from various faculties of Aydın Adnan Menderes University participated in this study. No histories of adverse side effects or allergies related to caffeine and taurine were present. Information related to age, weight, height, body mass index, and caffeine consumption habits was obtained using an acceptance questionnaire. All participants were infrequent caffeine consumers (0–25 mg caffeine/day). The exclusion criteria included a body mass index greater than 30 kg/m2, a systemic disease, current alcoholism, and smoking. We performed an a priori power analysis to obtain the sample size. The t-test was applied for power analysis, and the actual power was found to be 0.85. We required a sample size of 14 for each group to detect the effects of caffeine and taurine on the cardiovascular system.
This was a single-blind, randomized trial. Participants were divided into four groups: caffeine (n = 14: 4 F + 10 M), taurine (n = 14: 4 F + 10 M), caffeine + taurine (n = 14: 4 F + 10 M), and control (n = 14: 4 F + 10 M), using the envelope randomization method. Opaque envelopes of the same size were chosen by the participants, and the experimental groups were formed with participants who chose envelopes containing the same group number. Informed consent was obtained from all participants.
2.2. Experimental Protocol
Participants were asked not to use caffeine-containing products, cigarettes, or alcohol 72 h before the study and not to eat or drink anything other than water 12 h before the study. Measurements were carried out at normal room temperature (20 ± 2 °C) in a partially isolated dim-light environment against external factors. The participants were told to rest for 20 min before the baseline measurements. Disposable Ag-AgCl electrodes were placed, and 5-min electrocardiogram signals were recorded from the participants in resting and supine posture. For this procedure, an ECG100C unit and BIOPAC Acknowledge acquisition software version 3.9 (Biopac System Inc., Santa Barbara, CA, USA) with a sampling frequency of 200 Hz were used. After electrocardiogram recording, systolic and diastolic blood pressure were measured manually by using a stethoscope (Littman Classic II, Saint Paul, MN, USA). Measurements were performed before consumption and 30 and 60 min after consumption. The caffeine group consumed 200 mg of caffeine + 0 mg of taurine; the taurine group consumed 0 mg of caffeine + 2500 mg of taurine; the caffeine + taurine group consumed 200 mg of caffeine + 2500 mg of taurine; and the control group consumed the same amount of water within 5 min. The doses of caffeine and taurine consumed were approximately the same as in a 20 oz energy drink. Caffeine and taurine were given in capsule form with water. The subjects were not informed about the ingredients in the capsule.
2.3. Denoising
Physiological signals are nonlinear, nonstationary, and quasi-periodic time series. However, they are very sensitive to different types of noise that can distort their morphological and spacing properties, leading to misdiagnosis and inappropriate treatment of patients. For this reason, the ECG signals obtained from the participants were subjected to various processes and cleared of noise to become understandable. In this study, a Daubechies mother wavelet ‘dB9’ at decomposition level 4 was used to remove interference noise. This mother wavelet is recommended in the literature as the most effective noise removal method for ECG signals [28]. The MATLAB Wavelet Toolbox 3.0.1 was used for the noise removal procedure.
2.4. Data Acquisition
All electrocardiogram analysis was performed according to the standards set by the Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology [20]. The HRV time series were derived from the 5-min electrocardiogram signals by using the Pan and Thompkins algorithm [29]. Consecutive RR peaks were determined, and the intervals were obtained. HRV was determined by dividing 60 by the RR interval durations.
2.5. Nonlinear Analysis
Phase Space Reconstruction
Electrocardiographic signals exhibit chaotic behavior, and thus, particularly nonlinear methods are required to analyze them. Takens’s phase space reconstruction technique is the most convenient as it can describe all the information of a system based on a single variable. In this study, HRV time series were reconstructed in phase space by using the calculated parameters of embedding dimension and time delay. Cao’s method [30] and the mutual information method [31] were used to calculate the embedding dimension and time delay values, respectively. The nonlinear parameters: largest Lyapunov exponent, correlation dimension, approximate entropy, and Hurst exponent, which represent the complexity and chaotic nature of the system, were extracted from the attractor. MATLAB (The Mathworks Inc., Natick, MA, USA) was used for this process. A detailed explanation was given in the study of Caliskan et al. [32].
2.6. Linear Analysis
A linear analysis of the electrocardiogram data was performed by Kubios HRV Standard (Kubios Heart Rate Variability analysis software version 3.1.0; Kupio, Finland). The time-domain parameters SDNN, RMSSD, and NN50 were analyzed. Furthermore, the frequency-domain parameters LF (0.04–0.15 Hz), HF (0.15–0.40 Hz), and LF/HF ratio were also evaluated.
2.7. Statistical Analysis
The experimental data were statistically analyzed using SPSS Statistics for Windows, Version 22.0 (SPSS Inc., Chicago, IL, USA). Distribution normalization was determined by the Shapiro–Wilk normality test. One-way variance analysis with the Bonferroni post-test was used for data with a normal distribution (>0.05), and the Kruskal–Wallis non-parametric test was used for data not distributed normally (<0.05). Two-way analyses of variance for repeated measures with the within-subject factors of time (pre, 30 min, 60 min) and group were used for the statistical evaluation. The effects of each treatment over time were analyzed by using one-way analyses of variance with the Bonferroni post-hoc test when the analyses of variance yielded a significant difference. Data were presented as the mean ± standard error of the mean. A p-value of less than 0.05 was considered to indicate statistical significance.
3. Results
Eighty-eight students were enrolled and underwent the study procedures in the second half of 2023. Fourteen volunteers had smoking habits, eight volunteers had systemic diseases, six volunteers had alcohol addiction, and four volunteers were excluded due to previous adverse reactions to caffeine. The mean age of the participants was 20.09 y/o ± 2.00 y/o, the mean height was 167.86 cm ± 3.04 cm, the mean weight was 69.62 kg ± 14.64 kg, and the mean body mass index was 23.01 ± 3.86. No significant differences were obtained between the groups among the age, height, weight, and body mass index values.
For the caffeine and caffeine + taurine groups, heart rate and systolic blood pressure increased, but no significant difference was seen in the taurine group (Table 1). The increase in heart rate and systolic blood pressure at 60 min for the caffeine group was found to be statistically significant when compared to baseline (Figure 1 and Figure 2). In addition, while the heart rate and systolic blood pressure values of the caffeine group at the 60th minute were found to be statistically significant compared to the control group (p = 0.012, p = 0.035, respectively), no difference was observed for the taurine group. Furthermore, for the treatment groups (caffeine, taurine, and caffeine + taurine groups), diastolic blood pressure did not change over time. No alterations were observed in the control group.

Table 1.
Hemodynamic and linear heart rate variability parameters of the groups. p-value refers to the differences between the groups’ pre and 60th min values.
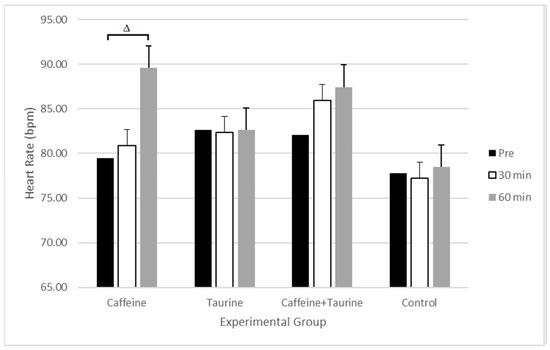
Figure 1.
Time course of changes in heart rate of experimental groups. Δ: statistically significant versus the pre value of the caffeine group (p = 0.013).
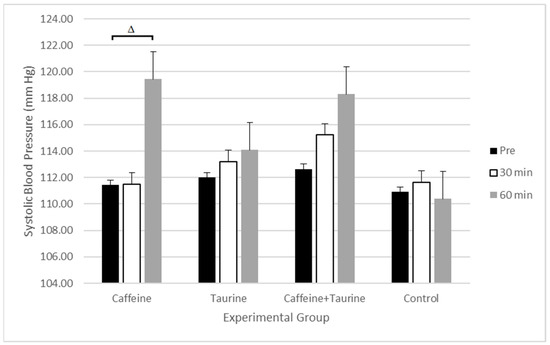
Figure 2.
Time course of changes in systolic blood pressure in experimental groups. Δ: statistically significant versus the pre value of the caffeine group (p = 0.019).
For the time-domain analysis, in the caffeine and caffeine + taurine groups, the RMSSD and NN50 increased and SDNN decreased. The alteration in these parameters for the caffeine group was found to be statistically significant when compared to the control group’s values at 60 min (p = 0.021, p = 0.048, and p = 0.016, respectively). Furthermore, an increase in the HF frequency-domain parameter was observed in the treatment groups, while the LF and LF/HF frequency-domain parameters tended to decrease over time. However, these reductions were not statistically significant when compared to the baseline values and the control group’s values. No changes were observed for the taurine and control groups’ time and frequency-domain parameters.
The time course of the changes in the largest Lyapunov exponent and approximate entropy are presented in Figure 3 and Figure 4. All nonlinear parameters were increased in the caffeine group, and these increments were statistically significant for the largest Lyapunov exponent and approximate entropy at 60 min (Table 2). Also, the caffeine group’s largest Lyapunov exponent values at 60 min were found to be statistically significant when compared to those for the control group (p = 0.013). For the taurine group, there was a slight reduction in the correlation dimension, but no significant alterations were observed for the other nonlinear parameters. Furthermore, for the caffeine + taurine group, all nonlinear parameters were higher than the pre values; however, a statistically significant increase was only observed for the largest Lyapunov exponent value at 60 min. No significant changes in the nonlinear parameters were observed for the control group over time.
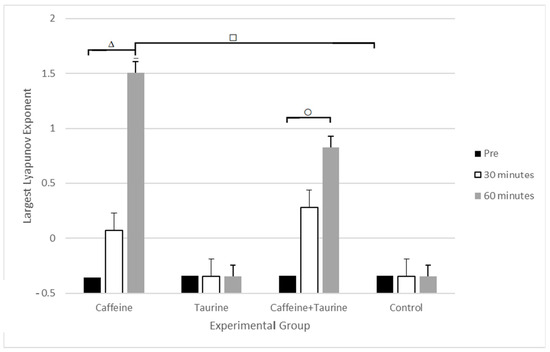
Figure 3.
Time course of changes in the largest Lyapunov exponent of experimental groups. Δ: statistically significant versus the pre value of the caffeine group (p = 0.009); ○: statistically significant versus the pre value of the caffeine + taurine group (p = 0.021); □: statistically significant versus the pre value of the control group (p = 0.013).
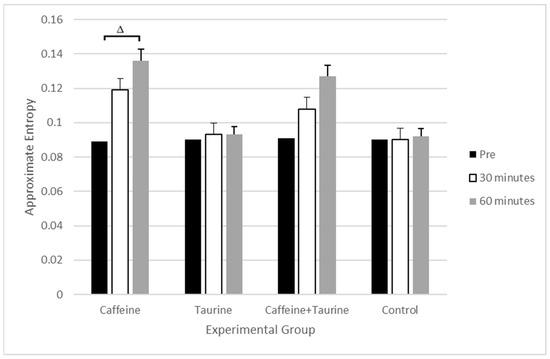
Figure 4.
Time course of changes in the approximate entropy of experimental groups. Δ: statistically significant versus the pre value of the caffeine group (p = 0.035).
Table 2.
Nonlinear heart rate variability parameters of the groups. p-value refers to the differences between the pre and 60th min values of the groups.
4. Discussion
This study was performed to evaluate the effects of caffeine and taurine components on the cardiovascular systems of young adults and to analyze HRV both linearly and nonlinearly. As a principal finding, compared with taurine and the combination of caffeine + taurine, caffeine was found to have the most negative effects on the cardiovascular system. It was also found that caffeine had adverse effects on the linear and nonlinear parameters of HRV. However, the presence of taurine may have repressed the adverse effects of caffeine.
Caffeine and taurine are accepted as the major ingredients of energy drinks that cause improvements in neurocognitive performance and positive ergogenic effects [10]. It was reported that high doses of caffeine are characterized by multiple cardiac comorbidities, including atrial fibrillation, palpitations, and tremors [7]. In addition, a transient increase in blood pressure and heart rate occurs due to the release of adrenaline after the consumption of caffeine [33]. Furthermore, low doses of taurine demonstrated cardioprotective actions such as decreasing platelet aggregation, reducing blood pressure, and having antiarrhythmic properties [7]. However, it was suggested that for higher doses of taurine, these beneficial effects were overridden [8].
Consistent with the effects of caffeine, Hartley et al. [34] reported a significant increase in both systolic blood pressure and diastolic blood pressure 60 min after the intake of a 250 mg caffeine capsule, while Papaioannou et al. [27] reported an increase in blood pressure values 60 min after the ingestion of 240 mg caffeine. These were in line with our results. This increase in blood pressure may be because of sympathetic over-activation, antagonism of adenosine receptors, and increased norepinephrine release [35]. Furthermore, Geethavani et al. [36] reported a significant increase in the heart rate related to caffeine intake after 60 min. We also found a significant elevation in heart rate values in the caffeine group 60 min after ingestion. On the other hand, in our study, we did not observe any changes in systolic blood pressure, diastolic blood pressure, or heart rate in the taurine group. Contrary to our results, it has been reported in the literature that the ingestion of taurine doses below the 10 g/day safe limit [37] reduces blood pressure and heart rate [7]. Since peak plasma concentrations of taurine occur at 60 min to 150 min after ingestion [38], the reason why no change was observed may be the duration of our study. On the other hand, for the caffeine + taurine group, the heart rate values increased in line with the study of Jeffries et al. [11], which reported a large increase in heart rate one hour after the ingestion of a combination of caffeine + taurine at rest. Increases in the systolic blood pressure and diastolic blood pressure values of the caffeine + taurine group were also found in our study; the increase was smaller in the caffeine + taurine group than in the caffeine group. This is because taurine may have a reducing effect on blood pressure and heart rate variability due to inducing vasodilation and its hypotonic effect. Caffeine consumption has been reported to increase vasoconstriction and the release of norepinephrine, which causes a high heart rate and blood pressure [39]. However, taurine has the opposite effect of caffeine by suppressing norepinephrine, increasing norepinephrine turnover, and reducing angiotensin II-mediated vasoconstriction [40]. In this case, the increased release of norepinephrine due to the presence of caffeine may have shown a taurine suppressive effect, therefore reducing the negative effects caused by caffeine, such as increases in heart rate and blood pressure [7]. Therefore, taurine may have repressed the effect of caffeine. This suggestion is in agreement with the report published by the European Union’s SCF, which noted that “if there are any interactions between caffeine and taurine, taurine might reduce the cardiovascular effects of caffeine” [7].
SDNN, LF, and LF/HF are related to heart responsiveness and are thought to be mediated by interactions between sympathetic and parasympathetic nerve activities. Their reduction is reported to be associated with an increased risk of sudden arrhythmic death. In particular, SDNN values below 50 ms are classified as unhealthy, while healthy values are between 50 and 100 ms [41]. In our study, we found a reduction in these parameters for the caffeine and caffeine + taurine groups, in line with the study of Nelson et al. [42], which reported a decrease in SDNN and LF values after the consumption of 473 mL of energy drink, and with Caliskan and Bilgin’s study [43], which reported a decrease in LF and LF/HF parameters after the same amount of energy drink was consumed. However, several studies have reported that these parameters increased or did not change over time [24,44]. This may be because, in our study, the effects of caffeine and taurine were examined separately instead of using energy drinks. Furthermore, we evaluated the RMSSD, NN50, and HF parameters, which are related to cardiac parasympathetic function, and found that these parameters increased in the caffeine and caffeine + taurine groups. Our results agreed with studies reporting increased RMSSD and HF values after the consumption of varying amounts of energy drinks or caffeine capsules [23,44]. Furthermore, the increases in heart rate, RMSSD, NN50, and HF can be explained by the dominance of parasympathetic influence mediated via the release of acetylcholine by the vagus nerve. Since there are no studies investigating the acute effects of taurine on the cardiovascular system, we cannot make comparisons with our results in this regard.
The oscillations of the heart have chaotic behavior. Therefore, nonlinear analysis of the cardiovascular system is gaining importance. It was reported that the cardiovascular system demonstrated increased complexity and chaotic behavior in several disease states [45]. There are very few studies in the literature investigating the effects of caffeine or energy drinks on the cardiovascular system using nonlinear analysis methods. In fact, no studies on the effects of taurine or a combination of taurine + caffeine have been conducted in this manner before our own study. We observed increases in the caffeine and caffeine + taurine groups’ largest Lyapunov exponent, correlation dimension, approximate entropy, and Hurst exponent values at 60 min. These results are in line with studies that have reported increased Lyapunov exponent and correlation dimension values 60 min after participants consumed energy drinks or coffee [25] and increased approximate entropy values after 5 mg/kg caffeine intake when compared to the control group [26]. Since no studies have evaluated the Hurst exponent after caffeine or taurine consumption in the literature, there is no opportunity to compare the results we obtained. The nonlinear parameters largest Lyapunov exponent, correlation dimension, approximate entropy, and Hurst exponent indicate the complexity and chaotic dynamics of the system. The increased values of these parameters are related to pathological phenomena. Therefore, our results support the suggestion that caffeine and beverages containing caffeine and taurine have adverse effects on the cardiovascular system and may induce heart-related diseases.
The central nervous system controls the heart from beat-to-beat through the vagus nerve and modulates heart rate. HRV is one of the major predictors utilized in a wide spectrum of cardiological and non-cardiological diseases. A high heart rate can cause tachycardia and also sudden cardiac death [22]. In this case, serious clinical conditions and heart failure symptoms such as mild dizziness, fainting with chest discomfort, severe chest pain, and shortness of breath may occur [46]. In addition, high blood pressure is an important risk factor for heart failure, atrial fibrillation, chronic kidney disease, heart valve diseases, aortic syndromes, and dementia, in addition to coronary heart disease and stroke [47]. Even though the doses used in our study were within the safe range (a single dose of 200 mg caffeine and 6 g/taurine per person per day) determined by the European Food Safety Authority (EFSA) [34,48], the high heart rate and blood pressure seen in our results showed that caffeine had negative effects on the cardiovascular system. Therefore, it was concluded that caffeine intake at this dose may be harmful.
This study possessed some limitations. The first limitation is the relatively small number of participants. A study with a larger sample size may contribute to a more accurate generalization of the results. Furthermore, studies with larger and more diverse sample sizes are being planned. In our study, short-term electrocardiogram recording was performed because there was a “stationarity” problem in long-term ECG recordings [20]. However, we did not consider the VLF parameter. Because of this, VLF values are considered dubious in short-term recordings [20]. If the duration of the recording increases, the long-term effects of caffeine and taurine on the cardiovascular system, such as their effects on VLF, can be evaluated, and the results can be extended. Moreover, energy drinks contain other ingredients such as glucuronolactone, sugar, ginkgo, and ginseng herbal flavors. It may be possible that these other components affect the cardiovascular system alone or synergistically with caffeine and taurine. The acute effects of other components were not evaluated in our study, which is an important limitation. In addition, the effects of higher doses of caffeine and taurine were not evaluated due to this being unethical and unsafe. Finally, the peak plasma concentration of taurine occurs at 60–150 min [49], but in our study we performed measurements at 30 min and 60 min after consumption. Therefore, the possible effects of taurine may not have been fully observed.
5. Conclusions
This study, which investigated the acute effects of caffeine and taurine components on the cardiovascular systems of young adults and analyzed HRV both linearly and nonlinearly, found that caffeine had the most negative effects on the cardiovascular system in young adults when compared to taurine and a combination of caffeine + taurine. It was also found that caffeine significantly increased heart rate and systolic blood pressure, which are important hemodynamic parameters. Furthermore, as a result of nonlinear analysis, it was found that caffeine consumption increased the complexity of the cardiovascular system in young adults. Accordingly, it had adverse effects on the linear and nonlinear parameters of HRV. It was also found that the presence of taurine may have repressed the adverse effects of caffeine. To validate and expand these findings, further studies with larger and more diverse sample sizes to investigate the possible acute effects of other energy drink ingredients over longer periods of time are being planned.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Medical Ethics Committee of Aydın Adnan Menderes University (Protocol number: 2022/15, 10 February 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
Acknowledgments
We thank the students for their participation in this study.
Conflicts of Interest
The author declares no conflicts of interest.
References
- Miller, K.E. Energy drinks, race, and problem behaviors among college students. J. Adolesc. Health 2008, 43, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Ali, F.; Rehman, H.; Babayan, Z.; Stapleton, D.; Joshi, D.D. Energy drinks and their adverse health effects: A systematic review of the current evidence. Postgrad. Med. 2015, 127, 308–322. [Google Scholar] [CrossRef]
- Higgins, J.P.; Tuttle, T.D.; Higgins, C.L. Energy beverages: Content and safety. Mayo Clin. Proc. 2010, 85, 1033–1041. [Google Scholar] [CrossRef] [PubMed]
- Kerrigan, S.; Lindsey, T. Fatal caffeine overdose: Two case reports. Forensic Sci. Int. 2005, 153, 67–69. [Google Scholar] [CrossRef]
- Bichler, A.; Swenson, A.; Harris, M.A. A combination of caffeine and taurine has no effect on short term memory but induces changes in heart rate and mean arterial blood pressure. Amino Acids 2006, 31, 471–476. [Google Scholar] [CrossRef]
- Wu, G. Important roles of dietary taurine, creatine, carnosine, anserine and 4-hydroxyproline in human nutrition and health. Amino Acids 2020, 52, 329–360. [Google Scholar] [CrossRef]
- Schaffer, S.W.; Shimada, K.; Jong, C.J.; Ito, T.; Azuma, J.; Takahashi, K. Effect of taurine and potential interactions with caffeine on cardiovascular function. Amino Acids 2014, 46, 1147–1157. [Google Scholar] [CrossRef]
- Ellermann, C.; Hakenes, T.; Wolfes, J.; Wegner, F.K.; Willy, K.; Leitz, P.; Rath, P.; Eckardt, L.; Frommeyer, G. Cardiovascular risk of energy drinks: Caffeine and taurine facilitate ventricular arrhythmias in a sensitive whole-heart model. J. Cardiovasc. Electrophysiol. 2022, 33, 1290–1297. [Google Scholar] [CrossRef]
- Caliskan, S.G.; Kilic, M.A.; Bilgin, M.D. Acute effects of energy drink on hemodynamic and electrophysiologic parameters in habitual and non-habitual caffeine consumers. Clin. Nutr. ESPEN 2021, 42, 333–338. [Google Scholar] [CrossRef]
- Doerner, J.M.; Kuetting, D.L.; Luetkens, J.A.; Naehle, C.P.; Dabir, D.; Homsi, R.; Nadal, J.; Schild, H.H.; Thomas, D.K. Caffeine and taurine containing energy drink increases left ventricular contractility in healthy volunteers. Int. J. Cardiovasc. Imaging 2015, 31, 595–601. [Google Scholar] [CrossRef]
- Jeffries, O.; Hill, J.; Patterson, S.D.; Waldron, M. Energy drink doses of caffeine and taurine have a null or negative effect on sprint performance. J. Strength Cond. Res. 2020, 34, 3475–3481. [Google Scholar] [CrossRef]
- Benjamim, C.J.R.; Kliszczewicz, B.; Garner, D.M.; Cavalcante, T.C.F.; da Silva, A.A.M.; Santana, M.D.R.; Valenti, V.E. Is caffeine recommended before exercise? A systematic review to investigate its impact on cardiac autonomic control via heart rate and its variability. J. Am. Coll. Nutr. 2020, 39, 563–573. [Google Scholar] [CrossRef]
- Porto, A.A.; Benjamim, C.J.R.; Gonzaga, L.A.; Luciano de Almeida, M.; Bueno Júnior, C.R.; Garner, D.M.; Valenti, V.E. Caffeine intake and its influences on heart rate variability recovery in healthy active adults after exercise: A systematic review and meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 1071–1082. [Google Scholar] [CrossRef]
- Porto, A.A.; Benjamim, C.J.R.; Gonzaga, L.A.; Garner, D.M.; Valenti, V.E. Acute effects of energy drink on heart rate variability recovery after exercise: A systematic review and meta-analysis. Sci. Sports 2022, 8067, 109–216. [Google Scholar] [CrossRef]
- Baum, M.; Weiβ, M. The influence of a taurine containing drink on cardiac parameters before and after exercise measured by echocardiography. Amino Acids 2001, 20, 75–82. [Google Scholar] [CrossRef]
- Hasty, F.; García, G.; Dávila, C.H.; Wittels, S.H.; Hendricks, S.; Chong, S. Heart rate variability as a possible predictive marker for acute inflammatory response in COVID-19 patients. Mil. Med. 2020, 186, e34–e38. [Google Scholar] [CrossRef]
- Germán-Salló, Z.; Germán-Salló, M. Non-linear methods in HRV analysis. Proc. Technol. 2016, 22, 645–651. [Google Scholar] [CrossRef]
- Ernst, G.; Watne, L.O.; Rostrup, M.; Neerland, B.E. Delirium in patients with hip fracture is associated with increased heart rate variability. Aging Clin. Exp. Res. 2020, 32, 2311–2318. [Google Scholar] [CrossRef]
- Shaffer, F.; Ginsberg, J.P. An overview of heart rate variability metrics and norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef]
- Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef]
- Nejadgohli, I.; Moradi, M.H.; Abdolali, F. Using phase space reconstruction for patient independent heartbeat classification in comparison with some benchmark methods. Comput. Biol. Med. 2011, 41, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Koulaouzidis, G.; Das, S.; Cappielo, G.; Mazomenos, E.B.; Maharatna, K.; Puddu, P.E.; Morgan, J.M. Prompt and accurate diagnosis of ventricular arrhythmias with a novel index based on phase space reconstruction of ECG. Int. J. Cardiol. 2015, 182, 38–43. [Google Scholar] [CrossRef]
- Wiklund, U.; Karlsson, M.; Oström, M.; Messner, T. Influence of energy drinks and alcohol on post-exercise heart rate recovery and heart rate variability. Clin. Physiol. Funct. Imaging 2009, 29, 74–80. [Google Scholar] [CrossRef]
- An, S.M.; Park, J.S.; Kim, S.H. Effect of energy drink dose on exercise capacity, heart recovery and heart rate variability after high-intensity exercise. J. Exerc. Nutr. Biochem. 2014, 18, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Caliskan, S.G.; Bilgin, M.D. Non-linear analysis of heart rate variability for evaluating the acute effects of caffeinated beverages in young adults. Cardiol. Young 2020, 30, 1018–1023. [Google Scholar] [CrossRef] [PubMed]
- Yaregani, V.K.; Krishnan, S.; Engels, H.J.; Gretebeck, R. Effects of caffeine on linear and nonlinear measures of heart rate variability before and after exercise. Depress. Anxiety 2005, 21, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Papaioannou, T.G.; Vlachopoulos, C.; Ioakeimidis, N.; Alexopoulos, N.; Stefanadis, C. Nonlinear dynamics of blood pressure variability after caffeine consumption. Clin. Med. Res. 2006, 4, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Seljuq, U.; Himayun, F.; Rasheed, H. Selection of an optimal mother wavelet basis function for ECG signal denoising. In Proceedings of the 17th IEEE International Multi Topic Conference, Karachi, Pakistan, 8–10 December 2014; pp. 26–30. [Google Scholar]
- Pan, J.; Thompkins, W.J. A real-time QRS detection algorithm. IEEE Trans. Biomed. Eng. 1985, 32, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Cao, L. Practical method for determining the minimum embedding dimension of a scalar time series. Physics D 1997, 110, 43–50. [Google Scholar] [CrossRef]
- Fraser, A.M.; Swinney, H.L. Independent coordinates for strange attractors from mutual information. Phys. Rev. A 1986, 33, 1134–1140. [Google Scholar] [CrossRef]
- Caliskan, S.G.; Polatli, M.; Bilgin, M.D. Nonlinear analysis of heart rate variability of healthy subjects and patients with chronic obstructive pulmonary disease. J. Med. Eng. Technol. 2018, 42, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Artalejo, F.; López-García, E. coffee consumption and cardiovascular disease: A condensed review of epidemiological evidence and mechanisms. J. Agric. Food Chem. 2018, 66, 5257–5263. [Google Scholar] [CrossRef] [PubMed]
- Hartley, T.R.; Sung, B.H.; Pincomb, G.A.; Whitsett, T.L.; Wilson, M.F.; Lovallo, W.R. Hypertension risk status and effect of caffeine on blood pressure. Hypertension 2000, 36, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Chei, C.L.; Loh, J.K.; Soh, A.; Yuan, J.M.; Koh, W.P. Coffee, tea, caffeine, and risk of hypertension: The Singapore Chinese Health Study. Eur. J. Nutr. 2018, 57, 1333–1342. [Google Scholar] [CrossRef] [PubMed]
- Geethavani, G.; Rameswarudu, M.; Rameshwari, R.R. Effect of caffeine on heart rate and blood pressure. Int. J. Sci. Res. 2014, 4, 1–2. [Google Scholar]
- EFSA Panel on Additives and Products or Substances used in Animal Feed (FEEDAP); Scientific opinion on the safety and efficacy of taurine as a feed additive for all animal species. EFSA J. 2012, 10, 2736. [CrossRef]
- Ghandforoush-Sattari, M.; Mashayekhi, S.; Krishna, C.V.; Thompson, J.P.; Routledge, P.A. Pharmacokinetics of oral taurine in healthy volunteers. J. Amino Acids 2010, 2010, 346237. [Google Scholar] [CrossRef]
- Palatini, P.; Ceolotto, G.; Ragazzo, F.; Dorigatti, F.; Saladini, F.; Papparella, I.; Mos, L.; Zanta, G.; Santonastaso, M. CYP1A2 genotype modifies the association between coffee intake and the risk of hypertension. J. Hypertens. 2009, 27, 1594–1601. [Google Scholar] [CrossRef] [PubMed]
- Hano, T.; Kasano, M.; Tomari, H.; Iwane, N. Taurine suppresses pressor response through the inhibition of sympathetic nerve activity and the improvement in baro-reflex sensitivity of spontaneously hypertensive rats. Adv. Exp. Med. Biol. 2009, 643, 57–63. [Google Scholar] [CrossRef]
- Kleiger, R.E.; Miller, J.P.; Bigger, J.T.; Moss, A.J. Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. Am. J. Cardiol. 1987, 59, 256–262. [Google Scholar] [CrossRef]
- Nelson, M.T.; Biltz, G.R.; Dengel, D.R. Cardiovascular and ride time-to-exhaustion effects of an energy drink. J. Int. Soc. Sports Nutr. 2014, 11, 2. [Google Scholar] [CrossRef] [PubMed]
- Çalışkan, Ş.G.; Bilgin, M.D. Acute effects of caffeinated beverages on electrocardiographic and hemodynamic parameters in young adults. Cukurova Med. J. 2022, 47, 972–980. [Google Scholar] [CrossRef]
- Flueck, J.L.; Schaufelberger, F.; Lienert, M.; Schäfer Olstad, D.; Wilhelm, M.; Perret, C. Acute effects of caffeine on heart rate variability, blood pressure and tidal volume in paraplegic and tetraplegic compared to able-bodied individuals: A randomized, blinded trial. PLoS ONE 2016, 11, e0165034. [Google Scholar] [CrossRef] [PubMed]
- Vaillancourt, D.E.; Newell, K.M. Changing complexity in human behavior and physiology through aging and disease. Neurobiol. Aging 2002, 23, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Sarıkaya, S.; Akyol, L.; Şahin, Ş.; Ede, H.; Börekçi, E.; Keser Yılmaz, Y.; Bolat, A.; Erbay, A.R. Clinical approach to patients with supraventricular tachycardia. Bozok Tıp Derg. 2013, 3, 51–58. [Google Scholar]
- Fuchs, F.D.; Whelton, P.K. High blood pressure and cardiovascular disease. Hypertension 2020, 75, 285–292. [Google Scholar] [CrossRef]
- EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies). Scientific Opinion on the safety of caffeine. EFSA J. 2015, 13, 4102. [Google Scholar] [CrossRef]
- Arnaud, M.J.; Welsch, C. Theophylline and Caffeine Metabolism in Man; Friedr. Vieweg and Sons: Zurich, Switzerland, 1982. [Google Scholar]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).