Abstract
Tracheal, bronchus, and lung cancer (TBLC) remains a major public health concern. Knowledge about geographic patterns and time trends in TBLC could give insights to better address this problem. This study aimed to evaluate the geographic patterns and time trends in mortality due to TBLC observed in Portugal. TBLC-related deaths and population estimates (2011–2021) were derived from the Instituto Nacional de Estatística. Age-standardized mortality rates for people aged 50 or more (ASMR_50+) per 100,000 were obtained. Analyses were stratified by gender, geographic region, and level of urbanization. The time trends in ASMR_50+ were evaluated using joinpoint regression models, and the values for the annual percentage change (APC) and the respective 95% confidence interval (95% CI) were obtained. Differences in mortality due to TBLC between regions and levels of urbanization (2017–2021) were assessed through a standardized mortality ratio (SMR) and the respective 95% CI. In 2021, the ASMR_50+ per 100,000 inhabitants observed in mainland Portugal was 158.0 and 40.4 among men and women, respectively. According to the time-trend analysis, ASMR_50+ due to TBLC remained stable or described a downward trend among men, but there was an upward trend among women in suburban and urban regions. Observed deaths were significantly higher than the expected for men in urban areas (SMR = 125%; 95% CI: 121–128 and SMR = 118%; 95% CI: 115–122 in Norte and Lisboa, respectively), and women in Urban Norte (SMR = 125%; 95%CI: 119–131). Lower mortality than expected was observed among men living in Rural Norte and Rural Centro, as well as, among women living in all the rural areas. In suburban areas, the observed deaths were lower, higher, or as expected depending on the geographic region and gender. A notable upward trend in mortality due to TBLC among women was observed. The geographic patterns observed suggest the effects of deleterious environmental factors and smoking habits, deserving attention from policymakers.
1. Introduction
Tracheal, bronchus, and lung cancer (TBLC) is the third most frequent cancer and the leading cause of cancer-related deaths in Europe, where half a million new cases were diagnosed and 400,000 related deaths were reported in 2020. Over the last decade, the incidence and mortality rates of TBLC have had a decreasing trend worldwide [1,2,3]. Despite the overall decreasing trend in rates, the absolute number of new TBLC diagnoses and the related deaths have increased in most European countries, owing to the aging population [2]. Therefore, TBLC remains a major public health concern.
In Portugal, TBLC is the third most common type of cancer for both men and women. In this country, there were 5415 new TBLC diagnoses in 2020, corresponding to an incidence rate of 53 per 100,000 inhabitants and accounting for almost 10% of the global cancer burden [4]. At same time, the mortality rate due to TBLC was 47 per 100,000, corresponding to 15% of all cancer-related deaths reported in Portugal [5]. Nowadays, among the 40 European countries, Portugal presents the 18th highest crude mortality rate due to TBLC [4]. Between 1955 and 2005, Portugal witnessed an increase in TBLC mortality among women, deserving particular concern [6]. A poor survival rate for patients diagnosed with TBLC has been reported in Portugal, where the cumulative survival rate of 5 years was 10.7% and 22.9% among men and women, respectively [7]. Due to the high fatality rate of TBLC, the mortality rate could be read as a mirror of the incidence rate [8]. Therefore, research on the geographical patterns of TBLC-related deaths could give insights into the differences in the incidence of this disease.
Differences in TBLC incidence and mortality are due to known risk factors which vary across geographic areas or population groups. The main risk factor is tobacco [1,2,7,9], followed by air pollution [2,9] and occupational carcinogens [2,8,9]. The TBLC burden is higher in men than in women mainly due to differences in smoking patterns [8]. However, there has been a consistent increase in incidence rates among women, becoming nearly identical to that of men [2,9]. Between 1988 and 2008, the prevalence of smoking observed in Portugal decreased among men but there was an upward trend in such prevalence among women [10]. Meanwhile, since 2005, Portugal has been strongly committed to tobacco control and protection of citizens against involuntary exposure to tobacco smoke [11]. The efforts of the Portuguese government in decreasing smoking prevalence would have had an impact on TBLC incidence and mortality.
A body of research reported the differences in mortality rates between countries due to TBLC [2,9]; however, the differences in such rates between different geographic regions in the same country has also been considered a valuable tool. Knowledge about geographical patterns and time trends in TBLC could give insights to better allocate resources.
This study aimed to evaluate the geographic patterns and temporal trends in TBLC observed in Portugal in recent years, considering not only the geographic region but also the level of urbanization.
2. Materials and Methods
2.1. Type of Study and Data Collection
This is a descriptive ecological study based on aggregated data concerning health and vital statistics of Portuguese population. Annual data on TBLC-related deaths and population estimates in the period 2011–2021 were derived from the publicly available online database, aggregated by NUT, of the Instituto Nacional de Estatística (INE) [5]. The number of deaths and population size were tabulated by gender, by age group (five-year intervals for people aged 50 to 84, and 85 years old or more) and by the region considering the Nomenclature of Territorial Units for Statistics level 3 (NUTS III). Each NUTIII was classified according to the level of urbanization into urban, suburban, and rural areas. This classification was based on the proportion of inhabitants living in local administrative units (LAUs) that were considered thinly populated (less than 100 habitants per km2) or densely populated (≥500 habitants per km2) areas. A NUT III was classified as urban if more than 50% of residents lived in densely populated LAUs, it was classified as rural if more than 50% of residents lived in thinly populated LAUs and it was classified suburban if less than 50% of residents lived in thinly or in densely populated LAUS [12]. Then, NUTIII were aggregated in larger areas (NUT II), where the data were not available individually but were stratified according to the level of urbanization, giving the following areas: Urban Norte, Suburban Norte, Rural Norte, Suburban Centro, Rural Centro, Urban Lisboa, Rural Alentejo, and Suburban Algarve.
2.2. Statistical Analysis
Age-standardized mortality rates due to TBLC for people aged 50 or more (ASMR_50+) per 100,000 were obtained using the direct method and the European standard population (2013 revision) as reference. ASMR_50+ was separately obtained for the men and women.
The time trends in ASMR_50+ between 2011 and 2021 for each NUT and level of urbanization were separately evaluated, using joinpoint regression models, for men and women. The estimated values for the annual percent change (APC) and the respective 95% confidence interval (95%CI) were obtained by fitting a regression line to the natural logarithm of the rates, where the calendar year was the independent variable. Joinpoints were also estimated. A joinpoint is a knot at which a significant change in the time trend occurs. The segment between two consecutive joinpoints corresponds to a time trend characterized by a specific APC (the slope segment). When the APC and 95% CI limits are negative, ASMR_50+ has a significant downward trend, while positive values for the APC and 95% CI limits correspond to a significant upward trend [13]. Regression analysis was performed using the Joinpoint Regression Program, V.4.3.1.0.
The differences in mortality between regions due to TBLC, stratified by the level of urbanization, were assessed through a standardized mortality ratio (SMR) and the respective 95% CI. The SMR was obtained by dividing the number of observed deaths by the number of expected deaths, and the quotient was then multiplied by 100. Based on the gender and age-specific mortality rates reported in mainland Portugal, the expected number of deaths for the period 2017–2021 was obtained for each age group, gender, and region. The SMRs and respective 95% CI were computed based on observed and expected deaths using the WinPepi software version 11.63 (available on: http://www.brixtonhealth.com/pepi4windows.html, accessed on 14 January 2024).
3. Results
In the last year of the time series (2021), the ASMR_50+ due to TBLC per 100,000 inhabitants observed in mainland Portugal was 158.0 and 40.4 among men and women, respectively. These AMSR_50+ for 2021 presented a large variation across the areas stratified by the level of urbanization, such that higher values were observed in the urban areas (183.0 in men and 45.9 in women) while the rural areas showed lower values (131.8 and 27.9 among men and women, respectively).
Overall, the ASMR_50+ decreased among men but increased among women; however, the time trend was different between the geographic regions, as shown in Figure 1, Figure 2 and Figure 3.
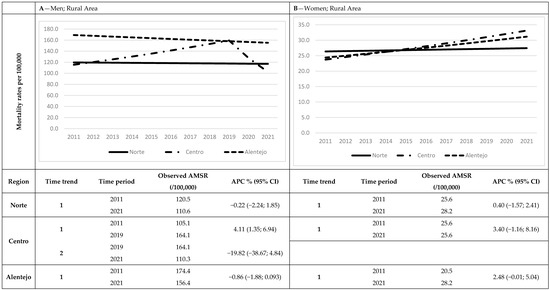
Figure 1.
Time trends in ASMR_50+ observed in rural regions, stratified by gender ((A) among men and (B) among women). Graphics display modeled values for ASMR-50+.
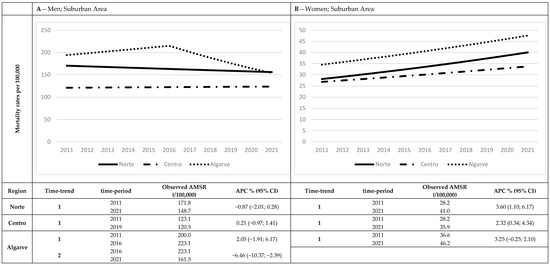
Figure 2.
Time trends in ASMR_50+ observed in suburban regions, stratified by gender ((A) among men and (B) among women). Graphics display modeled values for ASMR-50+.
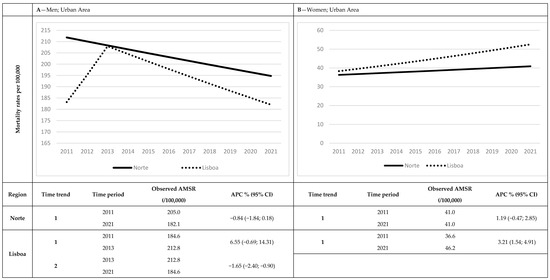
Figure 3.
Time trends in ASMR_50+ observed in urban regions, stratified by gender ((A) among men and (B) among women). Graphics display modeled values for ASMR_50+.
In the rural areas (Figure 1), there were no significant variations in AMSR_50+ among the women, regardless of the geographic region. Among men living in the rural areas, there was an upward trend in AMSR_50+ observed in Centro, between 2011 and 2019 (APC = 4.11%; 95%CI from 1.35 to 6.94), that reverted thereafter, while no significant variation in rates was observed in Norte and in Alentejo.
In the suburban areas (Figure 2), there was a significant increase in ASMR_50+ among women living in Norte (APC = 3.60%; 95% from 1.10 to 6.17) and in Centro (APC = 2.32%; 95% from 0.34 to 4.34), while no variation was observed among men living in the same regions. In Algarve, however, there was a significant decrease in AMSR_50+ among men from 2016 onwards (APC = −6.46%; 95%CI from −10.37 to −2.39), but there was no significant variation in AMSR_50+ among women.
In the urban areas (Figure 3), there was no significant variation in AMSR-50+ among men and women living in Norte. The AMSR_50+ observed in Lisboa, however, showed a significant increase in women over the whole study period (APC = 3.21%; 95% CI from 1.54 to 4.91) and a significant decrease in among men from 2013 onwards (APC = −1.65; 95% CI from −2.40 to −0.90).
Differences between geographic regions and level of urbanization were assessed through SMRs and the respective 95% CI. The results are shown separately for men (Figure 4) and women (Figure 5). The observed deaths were significantly higher than the expected for men living in Urban Norte (SMR = 125% 95% CI from 121 to 128), Urban Lisboa (SMR = 118% 95% CI from 115 to 122) and Suburban Algarve (SMR = 109% 95% CI from 102 to 117). The men living in Rural Norte (SMR = 72% 95% CI from 66 to 78), Rural Centro (SMR = 85% 95% CI from 78 to 92), and Suburban Centro (SMR = 78 95% CI from 75 to 81), however, presented a lower rate of mortality than expected (Figure 4).
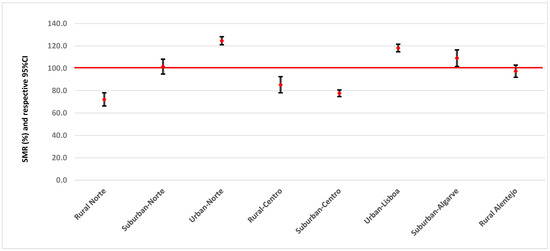
Figure 4.
Standardized mortality ratio and respective 95% CI by region and level of urbanization among men. Red line means no differences between observed and expected values.
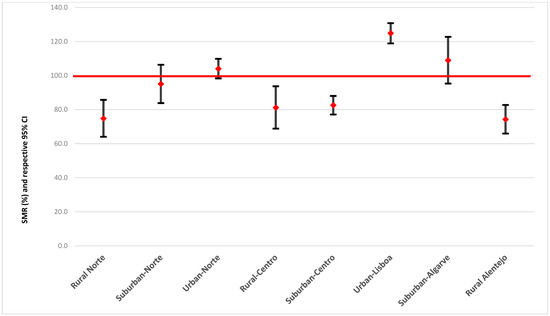
Figure 5.
Standardized mortality ratio and respective 95% CI by region and level of urbanization among women. Red line means no differences between observed and expected values.
Among women, only those living in Urban Lisboa presented significantly higher deaths than expected (SMR = 125% 95% CI from 119 to 131). The observed deaths were significantly lower than expected for women living in all rural regions.
4. Discussion
In Portugal, over the last decade, ASMRs due to TBLC has remained stable or presented a downward trend among men, while the rates observed among women have shown an upward trend in suburban and urban regions. Among men, the ASMR_50+ due to TBLC are threefold higher than among women. Also, there are differences in ASMR_50+, not only by level of urbanization but also by geographic area.
According to our results, the temporal trends in ASMR-50+ due to TBLC have described quite a similar pattern across the geographic regions with a downward trend among men and an upward trend among women, regardless of the level of urbanization. However, our stratified analysis highlight differences in ASMR_50+ due to TBLC, not only according to the level of urbanization, but also according to the geographic region. A body of research has reported differences in the risk of TBLC between countries [14] and between geographic regions in the same country [15,16,17,18,19], including in Portugal [20]. In line with the previous research [19], our results showed that ASMR_50+ due to TBLC was higher than expected in urban and lower than in rural areas, although there are some differences between geographic regions with the same level of urbanization. A higher risk of death due to TBLC in the urban areas mirrors the impact of air pollution on the occurrence of respiratory diseases [21]. Urbanization and concomitant industrialization are linked to an increased emission of pollutants due to fossil fuel combustion and motorized traffic, and the air concentration of these pollutants has been correlated with the risk of death due to respiratory diseases [21], namely TBLC [21,22,23], and it can partially explain why the risk of death due to TBLC that we observed was higher in urban and lower in rural areas. However, we cannot exclude the effect of other factors underlying the differences in ASMR_50+ due to TBLC between the rural and urban areas, particularly tobacco use, the leading cause of death due to TBLC [2]. According to data from 2014 [5], when compared with rural areas, the prevalence of smoking in urban areas in Northern Portugal was 50% higher among men (29% vs. 18%) and almost fourfold higher among women (13% vs. 4%), and these differences appeared to be shaped by the values of the SMR, particularly among men. Also, considering only the rural areas, there were differences in the prevalence of smoking across geographic regions such that Norte presented the lowest and Alentejo had the highest prevalence, either among men (18% in Norte and 28% in Alentejo) or women (4% in Norte and 10% in Alentejo) [5]. The differences in the SMRs that we had observed across the rural geographic regions were in line, but only in men, with the differences in smoking prevalence between the areas. In turn, the suburban regions appeared as heterogenous areas where the effect of the geographic region was much more evident than in rural or urban areas. We observed that the ASMR_50+ among the suburban population was higher than expected in Algarve, lower than expected in Centro, and as expected in Norte. In many countries around the world, suburban populations are more likely to have unfavorable lifestyles [24,25], including smoking behaviors [25]. However, the suburban areas in Portugal are hybrid regions, which allow people to live in closer high-density cities, but share a higher or lower amount of healthy features with the rural areas. In some Portuguese municipalities, mainly in suburban settings, there have been huge, targeted efforts to improve the levels of environmental quality and to promote healthy lifestyles, including the use of non-motorized vehicles and the prevention of smoking [26]. The differences in the ASMR_50+ due to TBLC, according to the geographic region, that we observed in the suburban areas can be partially explained by the differences in the frequency of unhealthy lifestyles. The prevalence of smoking in suburban areas was higher in Algarve (33% and 24% among men and women, respectively) than in Norte (26% and 8% among men and women, respectively) or in Centro (27% and 8% among men and women, respectively). Also, there has been reported large disparity across the Portuguese regions with regard to the environmental quality and the suburban area in Algarve presented the second worst indicator of environmental quality [5].
Gender differences in the temporal trends that we observed were in line with the previous research about global trends of ASMRs due to TBLC. Indeed, an overall decline in mortality rates due to TBLC has been reported but with opposite trends in men (downward trend) and women (upward trend) [1,2]. The global temporal trends in mortality follow the temporal trends in TBLC incidence, with a dramatic increase in the number of new cases diagnosed among women, particularly in Southern Europe, [3] the region to which Portugal belongs. Specifically, in Portugal, between 1998 and 2011, there was an increase in TBLC incidence for both men and women, but the annual percentage change was much more evident among women compared to men [11]. Such gender-specific differences in the incidence of TBLC have grown over time. In turn, the incidence of TBLC is mainly determined by the prevalence of cigarette smoking [1,9,14,27]. Therefore, smoking patterns over time drive trends of ASMRs due to TBLC [2,14]. Although there are large differences across geographic areas and between men and women, over 50% of the new cases of TBLC reported in Portugal have been attributed to tobacco smoking [11]. Several European countries reported the increasing prevalence of smoking among women while the prevalence describes a downward trend among men [28]. This pattern has also been reported in Portugal from 1988 to 2008, where smoking prevalence increased by four times among women aged between 30 and 50 years [10]. Also, between 1990 and 2015, the prevalence of daily smokers observed in Portugal increased by 1.3% per year among women but decreased by 1.0% per year among men [28]. The gender-specific differences in the variation in smoking prevalence over time most likely explain the differences between women and men with regard to the temporal trends of ASMR_50+ due to TBLC that we observed. However, previous research conducted in Portugal has reported a slightly higher proportion of TBLC stage I at diagnosis among women in comparison with men, most likely due to earlier detection of TBLC among women, which can improve prognosis and increase survival [20].
5. Conclusions
In summary, our findings indicate that ASMR-50+ due to TBLC described a moderate decline among men but a notable upward trend among women in urban and suburban areas. Also, there were variations in mortality due to TBLC not only by geographic regions but also by the level of urbanization. Both the urban areas (Norte and Lisboa) as well the suburban area in Algarve presented higher mortality rates than expected. These temporal and geographic patterns could be driven by deleterious environmental and smoking habits, and they deserve particular attention from policymakers.
Author Contributions
Conceptualization, C.T. and A.N.; methodology, C.T.; software, C.T.; validation, C.T., A.F.A. and A.N.; formal analysis, C.T.; investigation, A.O., C.F. and J.C.; resources, A.O., C.F. and J.C.; data curation, A.O., C.F. and J.C.; writing—original draft preparation, C.T.; writing—review and editing, A.F.A.; visualization, A.F.A.; supervision, A.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was based on aggregated data, publicly available from Instituto Naciaonal de Estatística online database. Therefore, this research did not require ethical approval.
Informed Consent Statement
This study was based on aggregated data publicly available from Instituto Naciaonal de Estatística and informed consent statement wasn’t applicable.
Data Availability Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Huang, J.; Deng, Y.; Tin, M.S.; Lok, V.; Ngai, C.H.; Zhang, L.; Lucero-Prisno, D.E.; Xu, W.; Zheng, Z.-J.; Elcarte, E.; et al. Distribution, Risk Factors, and Temporal Trends for Lung Cancer Incidence and Mortality: A Global Analysis. Chest 2022, 161, 1101–1111. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Zhao, P.; Zhou, L.; Xiang, D.; Hu, J.; Liu, Y.; Ruan, J.; Ye, X.; Zheng, Y.; Yao, J.; et al. Epidemiological trends of tracheal, bronchus, and lung cancer at the global, regional, and national levels: A population-based study. J. Hematol. Oncol. 2020, 13, 98. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Luo, G.; Etxeberria, J.; Hao, Y. Global Patterns and Trends in Lung Cancer Incidence: A Population-Based Study. J. Thorac. Oncol. 2021, 16, 933–944. [Google Scholar] [CrossRef]
- World Health Organization. International Agency for Research on Cancer—Global Cancer Observatory. Cancer Today. 2020. Available online: http://gco.iarc.fr/ (accessed on 29 December 2021).
- Instituto Nacional de Estatística. Available online: https://www.ine.pt/ (accessed on 29 December 2021).
- Alves, L.; Bastos, J.; Lunet, N. Trends in lung cancer mortality in Portugal (1955–2005). Rev. Port. Pneumol. 2009, 15, 575–587. [Google Scholar] [CrossRef] [PubMed]
- Guerreiro, T.; Forjaz, G.; Antunes, L.; Bastos, J.; Mayer, A.; Aguiar, P.; Araújo, A.; Nunes, C. Lung cancer survival and sex-specific patterns in Portugal: A population-based analysis. Pulmonology 2021, 29, S70–S79. [Google Scholar] [CrossRef]
- Schabath, M.B.; Cote, M.L. Cancer Progress and Priorities: Lung Cancer. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1563–1579. [Google Scholar] [CrossRef]
- Barta, J.A.; Powell, C.A.; Wisnivesky, J.P. Global Epidemiology of Lung Cancer. Ann. Glob. Health 2019, 85, 8. [Google Scholar] [CrossRef] [PubMed]
- Carreira, H.; Pereira, M.; Azevedo, A.; Lunet, N. Trends in the prevalence of smoking in Portugal: A systematic review. BMC Public Health 2012, 12, 958. [Google Scholar] [CrossRef]
- Forjaz, G.; Bastos, J.; Castro, C.; Mayer, A.; Noone, A.-M.; Chen, H.-S.; Mariotto, A.B. Regional differences in tobacco smoking and lung cancer in Portugal in 2018: A population-based analysis using nationwide incidence and mortality data. BMJ Open 2020, 10, e038937. [Google Scholar] [CrossRef]
- Dijkstra, L.; Poelman, H. A Harmonised Definition of Cities and Rural Areas: The New Degree of Urbanisation; European Commission: Brussels, Belgium, 2014. [Google Scholar]
- Kim, H.-J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Sharma, R. Mapping of global, regional and national incidence, mortality and mortality-to-incidence ratio of lung cancer in 2020 and 2050. Int. J. Clin. Oncol. 2022, 27, 665–675. [Google Scholar] [CrossRef]
- Hagedoorn, P.; Vandenheede, H.; Willaert, D.; Vanthomme, K.; Gadeyne, S. Regional Inequalities in Lung Cancer Mortality in Belgium at the Beginning of the 21st Century: The Contribution of Individual and Area-Level Socioeconomic Status and Industrial Exposure. PLoS ONE 2016, 11, e0147099. [Google Scholar] [CrossRef]
- Mokdad, A.H.; Dwyer-Lindgren, L.; Fitzmaurice, C.; Stubbs, R.W.; Bertozzi-Villa, A.; Morozoff, C.; Charara, R.; Allen, C.; Naghavi, M.; Murray, C.J.L. Trends and Patterns of Disparities in Cancer Mortality Among US Counties, 1980–2014. JAMA 2017, 317, 388–406. [Google Scholar] [CrossRef]
- Lei, L.; Huang, A.; Cai, W.; Liang, L.; Wang, Y.; Liu, F.; Peng, J. Spatial and Temporal Analysis of Lung Cancer in Shenzhen, 2008–2018. Int. J. Environ. Res. Public Health 2020, 18, 26. [Google Scholar] [CrossRef] [PubMed]
- Ou, J.Y.; Fowler, B.; Ding, Q.; Kirchhoff, A.C.; Pappas, L.; Boucher, K.; Akerley, W.; Wu, Y.; Kaphingst, K.; Harding, G.; et al. A statewide investigation of geographic lung cancer incidence patterns and radon exposure in a low-smoking population. BMC Cancer 2018, 18, 115. [Google Scholar] [CrossRef] [PubMed]
- Redondo-Sánchez, D.; Fernández-Navarro, P.; Rodríguez-Barranco, M.; Nuñez, O.; Petrova, D.; García-Torrecillas, J.M.; Jiménez-Moleón, J.J.; Sánchez, M.-J. Socio-economic inequalities in lung cancer mortality in Spain: A nation-wide study using area-based deprivation. Int. J. Equity Health 2023, 22, 145. [Google Scholar] [CrossRef]
- Guerreiro, T.; Antunes, L.; Bastos, J.; Mayer, A.; Forjaz, G.; Araujo, A.; Nunes, C. Lung Cancer: A Nationwide Study to Characterize Sex Differences, Incidence, and Spatial Patterns in Portugal. In Vivo 2020, 34, 2711–2719. [Google Scholar] [CrossRef] [PubMed]
- Brunekreef, B.; Strak, M.; Chen, J.; Andersen, Z.J.; Atkinson, R.; Bauwelinck, M.; Bellander, T.; Boutron, M.C.; Brandt, J.; Carey, I.; et al. Mortality and Morbidity Effects of Long-Term Exposure to Low-Level PM2.5, BC, NO2, and O3: An Analysis of European Cohorts in the ELAPSE Project. Res. Rep. Health Eff. Inst. 2021, 2021, 208. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9476567/pdf/hei-2021-208.pdf (accessed on 20 January 2024).
- Cardoso, D.; Painho, M.; Roquette, R. A geographically weighted regression approach to investigate air pollution effect on lung cancer: A case study in Portugal. Geospat. Health 2019, 14, 35–45. [Google Scholar] [CrossRef]
- Arif, I.; Adams, M.D.; Johnson, M.T. A meta-analysis of the carcinogenic effects of particulate matter and polycyclic aromatic hydrocarbons. Environ. Pollut. 2024, 351, 123941. [Google Scholar] [CrossRef]
- Khayat, S.; Dolatian, M.; Navidian, A.; Mahmoodi, Z.; Sharifi, N.; Kasaeian, A. Lifestyles in suburban populations: A systematic review. Electron. Physician 2017, 9, 4791–4800. [Google Scholar] [CrossRef] [PubMed]
- Mantey, D.S.; Omega-Njemnobi, O.; Hunt, E.T.; Lanza, K.; Cristol, B.; Kelder, S.H. Home Smoke-Free Policies as Children Age: Urban, Rural, and Suburban Differences. Nicotine Tob. Res. 2022, 24, 1985–1993. [Google Scholar] [CrossRef] [PubMed]
- Torres, M.; Silva, L.T.; Santos, L.; Mendes, J.F. Saúde e bem-estar em meio urbano: Das políticas à prática. Rev. Port. Saúde Pública 2013, 31, 95–107. [Google Scholar] [CrossRef][Green Version]
- National Center for Chronic Disease Prevention and Health Promotion (US) Office on Smoking and Health. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General; Centers for Disease Control and Prevention (US): Atlanta, GA, USA, 2014. Available online: https://www.ncbi.nlm.nih.gov/books/NBK179276/ (accessed on 20 January 2024).
- Reitsma, M.B.; Fullman, N.; Ng, M.; Salama, J.S.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abera, S.F.; Abraham, B.; Abyu, G.Y.; et al. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990–2015: A systematic analysis from the Global Burden of Disease Study 2015. Lancet 2017, 389, 1885–1906. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).