Abstract
Over the past few years, life expectancy has increased significantly. However, elderly individuals living independently often require assistance due to mobility issues, symptoms of dementia, or other health-related challenges. In these situations, high-quality elderly care systems for the aging population require innovative approaches to guarantee Quality of Service (QoS) and Quality of Experience (QoE). Traditional remote elderly care methods face several challenges, including high latency and poor service quality, which affect their transparency and stability. This paper proposes an Edge Computational Intelligence (ECI)-based haptic-driven ECI-TeleCaring system for the remote caring and monitoring of elderly people. It utilizes a Software-Defined Network (SDN) and Mobile Edge Computing (MEC) to reduce latency and enhance responsiveness. Dual Long Short-Term Memory (LSTM) models are deployed at the edge to enable real-time location-aware activity prediction to ensure QoS and QoE. The results from the simulation demonstrate that the proposed system is proficient in managing the transmission of data in real time without and with an activity recognition and location-aware model by communication latency under 2.5 ms (more than 60%) and from 11∼12 ms (60∼95%) for 10 to 1000 data packets, respectively. The results also show that the proposed system ensures a trade-off between the transparency and stability of the system from the QoS and QoE perspectives. Moreover, the proposed system serves as a testbed for implementing, investigating, and managing elder telecaring services for QoS/QoE provisioning. It facilitates real-time monitoring of the deployed technological parameters along with network delay and packet loss, and it oversees data exchange between the master domain (human operator) and slave domain (telerobot).
1. Introduction
The rapid advancements in robotics and Artificial Intelligence (AI) have significantly transformed various sectors, including healthcare [1,2]. One of the critical areas where these technologies have shown immense potential is in elder care services [3,4]. The integration of robotics into elder care aims to address the increasing demand for high-quality care, driven by the aging global population. According to the World Health Organization (WHO), the number of people aged 60 years and older is expected to double by 2050, necessitating innovative solutions to meet their care needs [5]. Robotic systems in elder care can perform a range of tasks, from physical assistance and medication management to companionship and health monitoring [6,7].
Robotic-assisted care systems have been extensively studied and developed to support individuals with various needs, ranging from physical assistance to social companionship. Early research highlighted the potential of robots like assistive mobile robots and robotic exoskeletons to enhance mobility and independence for users [8,9]. For instance, the authors in [10] proposed Lio, a mobile robot platform with a multi-functional arm designed for human–robot interaction and personal care tasks, which has been successfully deployed in healthcare facilities. Similarly, the work in [11] demonstrated that ‘Zora’, a caring robot, positively impacted client interaction and activity levels in elderly care institutions. The authors in [12] conducted a study deploying the robot platform Pepper in a care home, revealing positive engagement from residents during robot-moderated training sessions.
Despite these advancements, providing real-time elder care services presents several challenges to meet Quality of Service (QoS) and Quality of Experience (QoE) requirements [13]. The problem is particularly critical in environments where care must be provided remotely and the system must adapt to various dynamic conditions and individual needs. Traditional methods of remote care are often limited by latency, inconsistent service quality, and inadequate personalization [14]. According to the Third-Generation Partnership Project (3GPP) Release 15 report, the Ultrareliable and Low-Latency Communication (URLLC) service offers a 99.9% reliability for a data packet of size 32 bytes and focuses on 1 ms communication latency [15]. However, activity sensor data along with haptic data in emerging applications like telecaring demand a higher packet rate with reliability greater than 99.9% under 1 ms latency.
Moreover, several studies focused on integrating AI to enhance QoS and QoE in remote care settings. In [16], a telerobotic system for remote dementia care is proposed which combines a dual-arm collaborative robot with a wearable motion capture device, enabling caregivers to assist dementia patients remotely. A study in [17] conducted a randomized controlled trial to evaluate the impact of culturally competent AI in socially assistive robots, which improved emotional well-being significantly compared to usual care. The challenges of introducing care robots in Swedish elder care and identifying barriers such as technological beliefs, attitudes, and the need for knowledge and skills at various levels were explored in [18]. A comprehensive overview of social robots in therapy and healthcare is presented in [19], highlighting their potential benefits and the necessity for further research on their acceptability and perception. However, the aforementioned studies ignored the aspect of stability and transparency in elder caring teleoperation systems. In this regard, a system is essential to balance stability and transparency while meeting QoS and QoE requirements under varying communication delays and high packet rates.
In addition to these developments, recent research has explored the combination of these technologies to create more robust telemedicine and elder care systems. The study in [20] proposed an Internet of Medical Things (IoMT)-based framework for home healthcare of the elderly, combining wireless body area networks (WBANs) for continuous monitoring, deep learning, and federated learning for data processing with 5G for rapid data transmission. The framework also utilizes cloud, edge, and fog computing to support the federated learning process. However, potential challenges include ensuring seamless integration of these technologies and managing the complexity of real-time data processing and transmission in a multi-layered architecture. The authors in [21] proposed the FEEL smart home healthcare system for elderly care, utilizing federated learning, a knowledge graph, and deep learning for health monitoring and recommendations. While effective in certain areas, the study did not fully address the integration challenges of AI models and real-time data accuracy across varied environments. A spectral clustering method and MFO-Edge caching algorithm to optimize e-health IoT networks by clustering patients and connecting them to SDN edge nodes for efficient data caching was presented in [22]. While the approach improved performance in terms of data retrieval delays and cache hit rates, it did not fully address the need for real-time adaptation to dynamic network conditions and personalized caching strategies. The work in [23] proposed an SDN-based model to enable global connectivity between IoT devices and medical services, particularly for integrating Nano networks within the human body with healthcare systems. However, the study highlighted the challenge of effectively managing the integration and real-time data sharing across diverse and globally distributed IoT networks, which remains a significant hurdle in achieving seamless healthcare connectivity. Similarly, a distributed edge computing-based IoT framework combining cloud computing, edge computing, and machine learning to optimize real-time data processing in medical sensor networks was proposed in [24]. However, the study did not fully address the challenge of efficiently handling the overwhelming amount of data collected by medical sensors, which is crucial for providing timely and relevant healthcare insights.
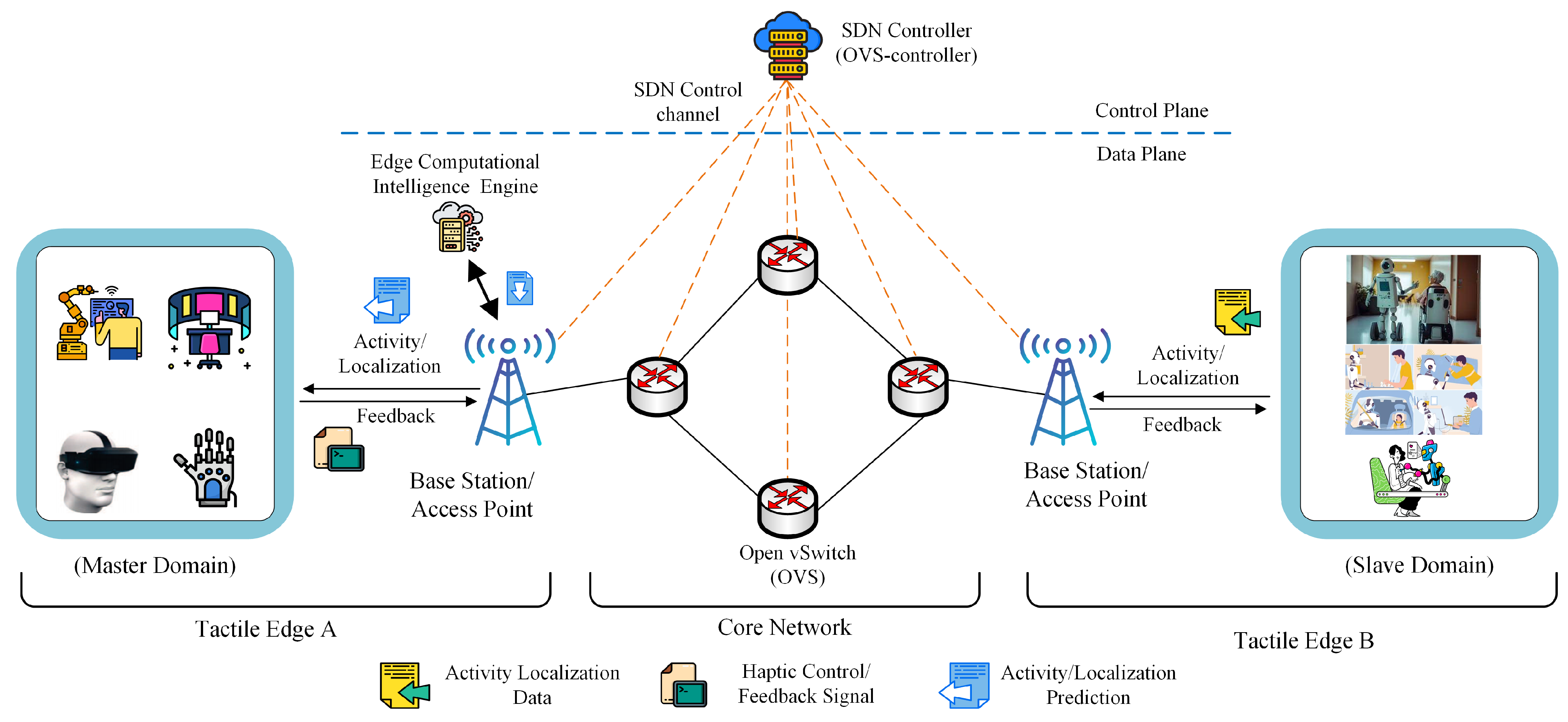
Therefore, this paper proposes an Edge Computational Intelligence (ECI)-based real-time elderly ECI-TeleCaring system to address challenges such as high latency, inconsistent service quality, inadequate personalization, and the need for stability and transparency in telecaring systems. The proposed system is specifically designed to ensure both QoS and QoE in elder care services by addressing these key challenges. To reduce latency, the system integrates Software-Defined Networking (SDN) and Mobile Edge Computing (MEC) technologies within the network domain to reduce delays and enable real-time bidirectional communication between the master and slave domains, which is critical for timely interventions in elder care. To ensure consistent service quality, a dual Long Short-Term Memory (LSTM) model is implemented at the edge for real-time remote activity prediction and critical decision making, thereby maintaining service quality even under varying conditions. The system also addresses the challenge of inadequate personalization by processing and analyzing large volumes of data at the edge, allowing it to continuously learn from and adapt to individual user needs, thereby providing a personalized care experience tailored to the specific requirements of each elderly individual. Furthermore, the proposed system is designed to enhance stability and transparency, particularly in telecaring scenarios, through edge intelligence to dynamically adapt to changing conditions and communication delays, ensuring that control signals between the master and slave domains remain stable and transparent, effectively overcoming the major shortcomings in existing telecaring systems. The proposed system consists of three main modules: the master domain, the network domain, and the slave domain, as depicted in Figure 1. A human operator on the master side uses a haptic display/device to monitor and control the slave domain. The network domain connects the master and slave domains, enabling bidirectional communication over the network. The core network of the proposed ECI-TeleCaring system includes SDN and MEC technologies to decrease network latency and support haptic-driven remote caring service. Slave domains comprise controller robots that are used for elder caring and are directly controlled and monitored by the master-domain-side human operator via control signals.
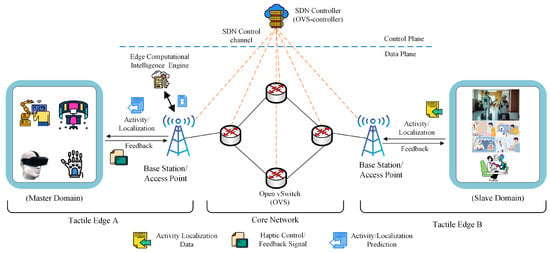
Figure 1.
An overview of the architecture design of the proposed elderly ECI-TeleCaring system.
The master domain receives the activity sensing along with haptic and audio–visual signals. The edge server on the master side predicts the activity of the caring robots and shows the performance to the human operator at the haptic display. Human operators can monitor the activity of multiple robots and, in the case of anomaly and undesirable events that degrade the Quality of Task (QoT), provide feedback to the slave domain using a haptic device or haptic data over the communication network. The proposed system employs a dual Long Short-Term Memory (LSTM) model at the edge for real-time remote activity prediction and critical decision making, significantly reducing latency and enhancing system responsiveness. The ability to process and analyze data at the edge ensures that the system can continuously learn and improve, providing a personalized care experience. The use of deep learning methods at the edge for data processing ensures that the system can handle large volumes of data, including haptic data, efficiently, providing timely responses and reducing the burden on human caregivers. Edge intelligence also facilitates the dynamic adaptation of the system to changing conditions and individual needs, thus overcoming the limitations of traditional remote care methods. The next section discusses the primary contribution of the ECI-TeleCaring system.
1.1. Research Contributions
The key contributions of this study can be summarized as follows:
- We discuss remote elder caring service, emphasizing challenges associated with high packet rate and packet size, and discuss requirements from QoS and QoE perspectives.
- A haptic-driven elderly ECI-TeleCaring system is proposed that incorporates an SDN mechanism, edge intelligence, and, particularly, Machine Learning (ML) to predict the slave-side activity at the master domain.
- In the proposed system, dual LSTM models are employed at the edge to predict the remote-side caring robot’s activity and localization in real time and display to the human operator at the master domain.
- We conducted various experiments to demonstrate that the proposed system achieves a balance between system stability and transparency while maintaining QoS and QoE requirements under unpredictable time delays and high packet rates.
- Finally, the proposed system is provided as an open-source tool along with the dataset used to facilitate further research and development in the field of remote elder telecaring services.
1.2. Paper Organization
This section discusses the organization of this paper. The rest of this paper is organized as follows. Section 2 describes the methodology and technical implementation of our proposed solution. Section 3 presents the experimental results and analysis. Finally, Section 4 concludes this paper with a summary of our findings and recommendations for future research.
2. Proposed System Methodology
This section discusses the proposed system design to provide haptic-driven elderly ECI-TeleCaring services and a testbed for existing remote elder caring systems. Firstly, we provide an overview of the proposed system, highlighting its key components: the master domain, the slave domain, the network domain, and an ECI engine. Secondly, we present a detailed discussion on the ML model, specifically, the LSTM model used to predict remote side activity and localization.
2.1. System Overview
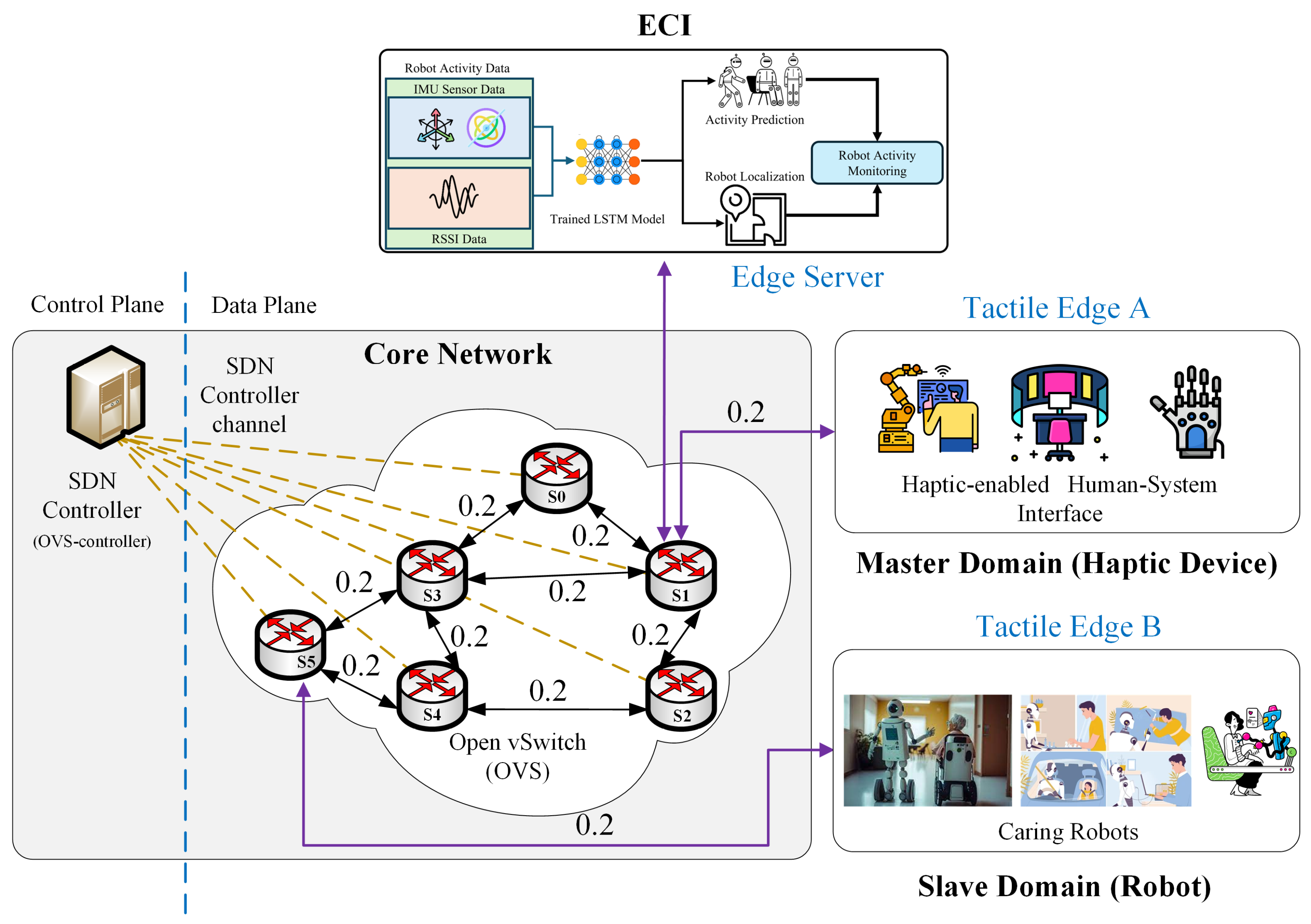
Figure 2 provides a detailed overview of the proposed haptic-driven bilateral TeleCaring system, aligned with the IEEE P1918.1 Tactile Internet standard architecture [25]. The robots on the slave side care for elder people in various environments, transmitting activity and localization data to the master side over the communication network and receiving haptic feedback. The proposed system core network consists of SDN-based technology, allowing for the separation of the control and data plane and supporting next-generation emerging applications. The SDN switch and controller communicate using OpenFlow protocol. The solid lines (black color) represent the transmission link weights in ms while the dotted lines (yellow color) represent the link between SDN-enabled switches and the controller. The SDN framework minimizes network complexity and allows for dynamic network resource sharing. Furthermore, it offers flexibility to the network by allowing operators to define virtual slices according to use cases while ensuring QoS.
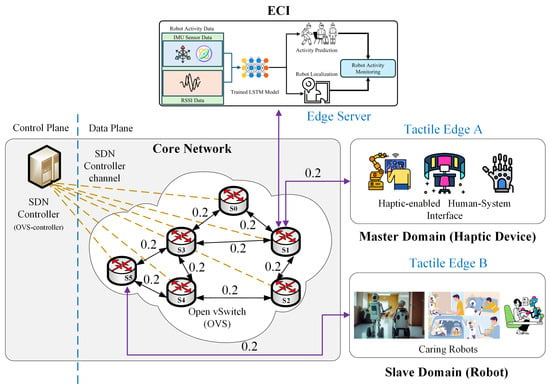
Figure 2.
An in-depth overview of the proposed ECI-TeleCaring system along with the ECI engine.
Active Queue Management techniques are employed in the proposed system that prevent buffer overflow by discarding or marking before buffer overflow, helping to deal with congestion challenges [26,27,28]. Moreover, we design a tactile support engine known as an ECI engine near the master domain following the Tactile Internet standard architecture (IEEE P1918.1), where dual-trained LSTM models are deployed for activity recognition and localization for remote-side caring robots. The edge server on the master side is responsible for activity and localization prediction of caring robots and displays the performance to the human operator via a haptic display. By processing data at the edge, critical decisions can be made in real time, significantly reducing the communication latency and enhancing the overall system’s performance with a focus on QoS and QoE provisioning for telecaring services. A human operator can monitor multiple robots simultaneously and provide feedback in case of anomalies, which is then communicated back to the slave domain over the network.
2.2. Activity Recognition and Localization
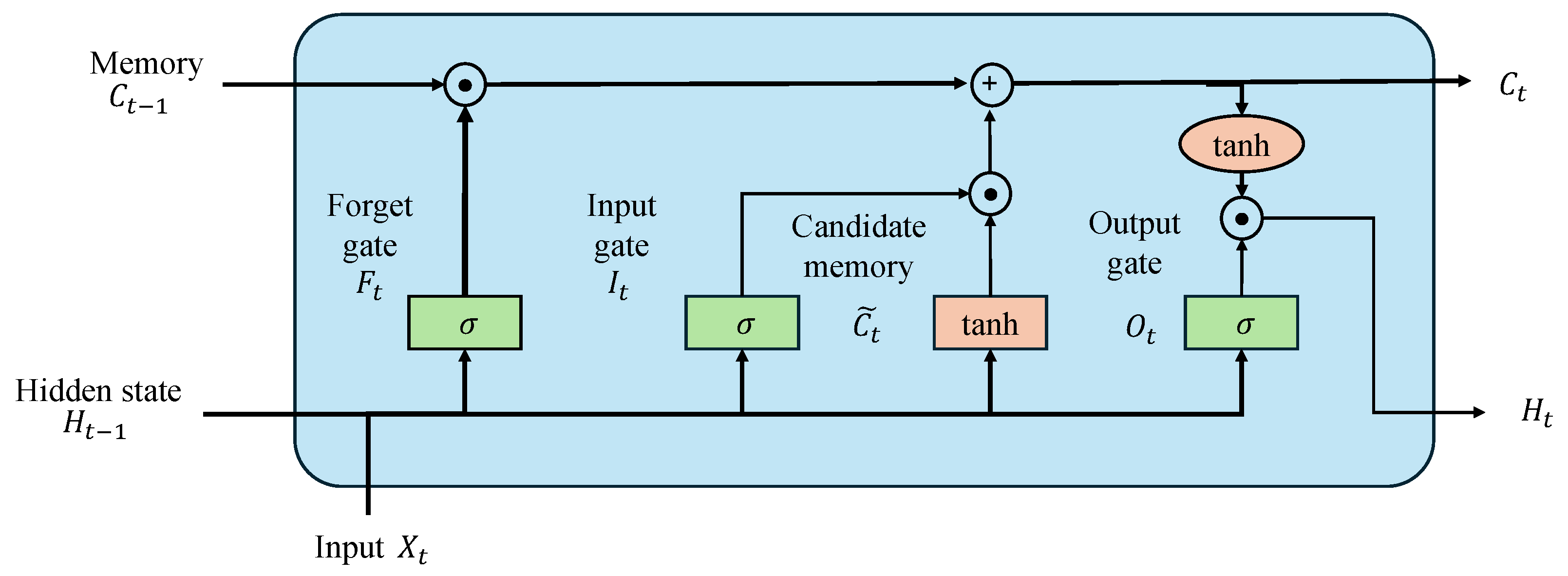
This subsection describes the proposed activity recognition and localization approach with four distinct classes and three classes, respectively, using dual LSTM networks. We implemented LSTM because it can handle temporal dependencies and because of its effectiveness in sequence prediction tasks, making it particularly suitable for activity recognition. A Long Short-Term Memory (LSTM) network, a variant of Recurrent Neural Networks (RNNs), is specifically engineered to handle time-series data. The structure of the LSTM network utilized in this research is illustrated in Figure 3.
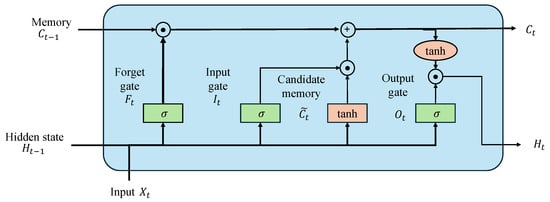
Figure 3.
Illustration of the architecture of the LSTM model employed in the proposed ECI framework for activity and localization prediction.
The network consists of an input layer, several LSTM layers, and a fully connected dense layer, culminating in a softmax output layer. The LSTM layers are tasked with capturing temporal dependencies in the data, and the dense layer translates these learned features into four distinct activity classes. The LSTM cell can be described by the following equations:
Forget gate:
where is the forget gate output, is the weight matrix, is the previous hidden state, is the current input, and is the bias term.
Input gate:
where is the input gate output, is the candidate cell state, and are the weight matrices, and and are the bias terms.
Cell state:
where is the current cell state and is the previous cell state.
Output gate:
where is the output gate output, is the current hidden state, is the weight matrix, and is the bias term. The LSTM network is trained using the cross-entropy loss function, which is suitable for multi-class classification tasks. The loss function is defined as
where N is the number of classes, is the true label, and is the predicted probability for class i. The LSTM model was trained using two datasets split into training, validation, and test sets having 70%, 15%, and 15%, respectively. The model was trained using the cross-entropy loss function and optimized with the Adam optimizer. The batch size was set to 32 and the learning rate was set to 0.0001. After training, we tested the model on the test dataset to evaluate the performance of the model using standard evaluation metrics such as accuracy, F-1 score, and recall.
3. Result and Discussion
In this section, we discuss and highlight the efficacy of the proposed elderly ECI-TeleCaring system under various simulation parametric settings. Default parameter values, simulation environment settings, and dataset collection modules used for experiments are presented in Table 1. The proposed framework is publicly available for the research community at GitHub (https://github.com/zubair1811/ECI-Elderly-TeleCaring-Monitoring-System.git, accessed on 25 July 2024) for the reproducibility of our work and to be utilized in their domain.

Table 1.
List of parameters settings, simulation environment, and dataset used in experimentation.
3.1. Simulation Setup
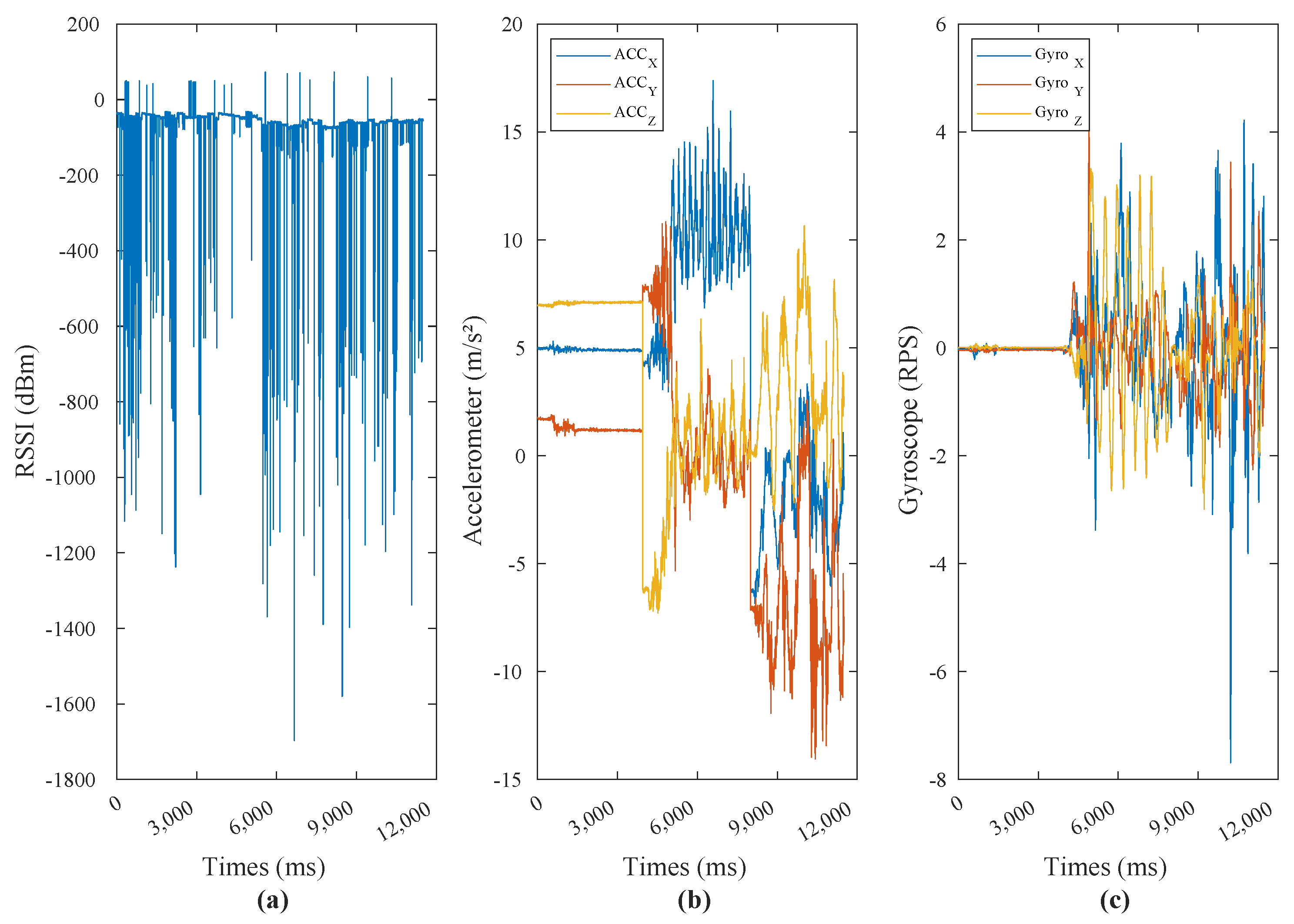
The simulation environment used for the experiment is developed in Python language on a computer with an Intel Core i7 processor, 8GB memory, and Ubuntu 20.04 (64 bit Linux) operating system. A Pytorch framework is used to program the LSTM model. To design a communication network between the master and remote sides, a Mininet emulator is utilized. The Mininet emulator is programmed in Python language and is publicly accessible for researchers at the Mininet official website (http://mininet.org/, accessed on 25 July 2024). It uses a Linux kernel to create a real network with virtualized end hosts, switches, routers, and links. It provides built-in support for SDN architecture. For our simulation experiments, we collected data using a custom-made wearable hand device equipped with an ESP32 chip for RSSI measurements and an MPU-6050 six-axis IMU sensor, as depicted in Figure 4. The dataset creation involved recording RSSI values for Wi-Fi fingerprinting (localization) and monitoring various activities with the IMU sensor. These activities included eating, being still, walking, and sitting. Data collection was performed at a high sampling rate of 50 Hz to ensure high-resolution data capture, resulting in more than 12,000 samples from male participants with a median age of 25 years. The ESP32 chip was utilized to gather RSSI values, which are crucial for determining the location of the device within an indoor environment. Meanwhile, the MPU-6050 IMU sensor provided detailed information on the user’s physical activities by measuring acceleration and angular velocity. The combination of the ESP32 and MPU-6050 sensors ensures robust and versatile data acquisition, essential for accurate analysis and application development in smart environments. In-depth details on dataset collection and the custom-made wearable hand device are provided in the Supplementary File of this paper. This dataset offers a comprehensive foundation for analyzing and modeling both localization and activity monitoring for remote patient care.
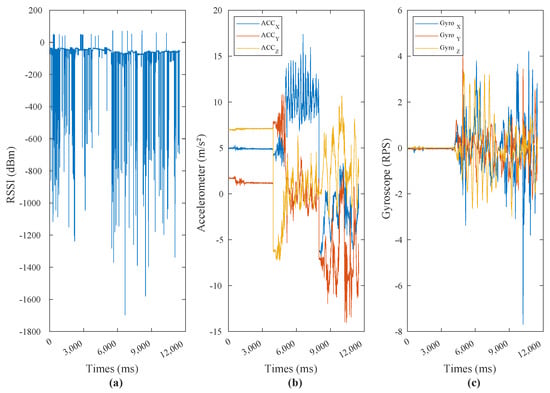
Figure 4.
Visualization of the acquired location and activity data which is used to analyze movement patterns and behavioral trends over a specified period. (a) indicates RSSI value, (b) indicates 3-axis accelerometer data, and (c) indicates 3-axis gyroscope data.
3.2. Learning Convergence of the Model
This section presents the study of the learning convergence of the models in terms of loss and accuracy, achieved by the LSTM models utilized in the proposed system for activity and localization prediction. The objective is to achieve improved convergence with a minimal number of training epochs, thereby reducing computational overhead.
The learning convergence of the LSTM model for indoor localization can be seen in Figure 5, which illustrates both loss and accuracy metrics over 300 epochs. It can be seen that the training loss continues to decline steadily, settling around 0.030, while the validation loss stabilizes near 0.035. The learning curve indicates effective learning and good generalization to unseen data. Simultaneously, the training and validation accuracy graphs show a consistent upward trend, both approaching 90%. Therefore, the convergence patterns in both loss and accuracy confirm that the model has successfully learned the indoor localization task and achieved high accuracy.
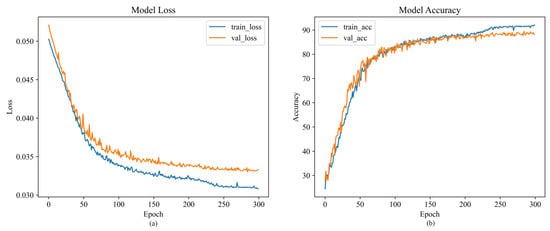
Figure 5.
The acquired training and validation loss along with respective accuracies to evaluate the learning convergence of the model for indoor localization. (a) illustrates training/validation loss over 100 epochs, and (b) illustrates training/validation accuracy over 100 epochs.
The convergence of the LSTM model for activity recognition is depicted in Figure 6, which shows both loss and accuracy over 300 epochs. Initially, the training and validation losses start above 0.05, decrease steadily, and stabilize around 0.035 towards the end. The accuracy graphs show a significant rise from around 20% at the beginning to nearly 80% by the 300th epoch for both training and validation accuracies. Therefore, the consistent improvement in both loss and accuracy metrics affirms that our model effectively learned on the activity recognition dataset.
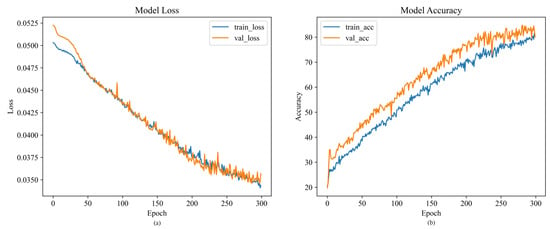
Figure 6.
Training and validation losses along with respective accuracies of the model for activity recognition. (a) illustrates training/validation loss over 100 epochs, and (b) illustrates training/validation accuracy over 100 epochs.
3.3. Latency Characterization
A haptic-driven TeleCaring system is developed to investigate the end-to-end (E2E) communication delay including the master and the slave with and without prediction model processing delay during haptic communication between the master and the slave operators in the remote elder caring application. Figure 7 and Figure 8 illustrate the analysis of the teleoperation system in terms of the E2E communication delay. The latency investigation between the robot (slave domain) and human operator (master domain) without the activity prediction model with the number of data packets (haptic, activity sensors) = 10, 100, and 1000 for the elder caring system is shown in Figure 7a–c, respectively.
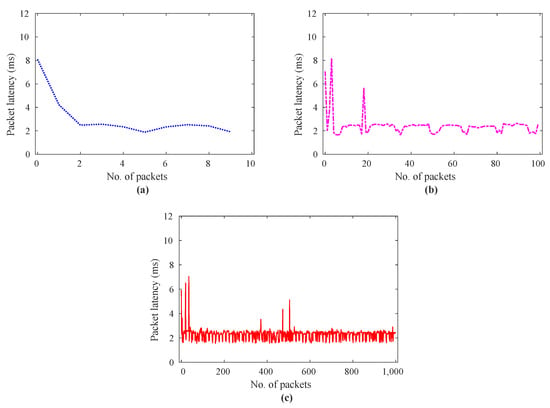
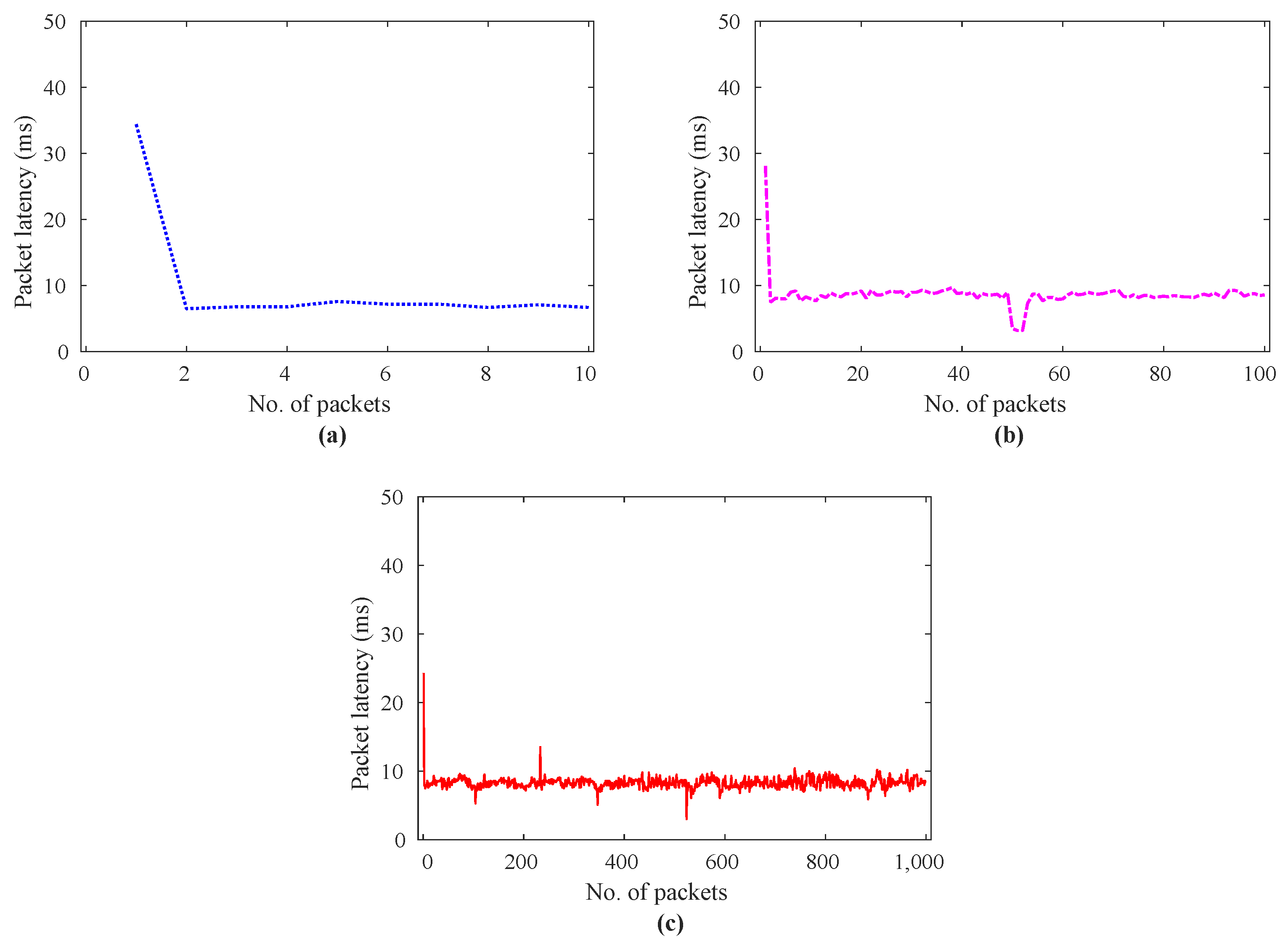
Figure 7.
Data packet latency analysis for real-time remote elder caring human–robot communication without edge-enabled activity and localization prediction model; (a) data packets = 10, (b) data packets = 100, (c) data packets = 1000.
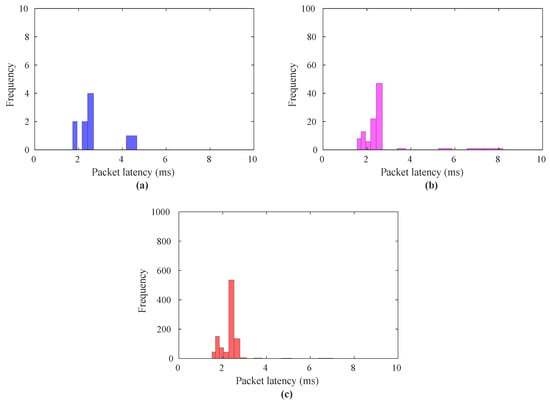
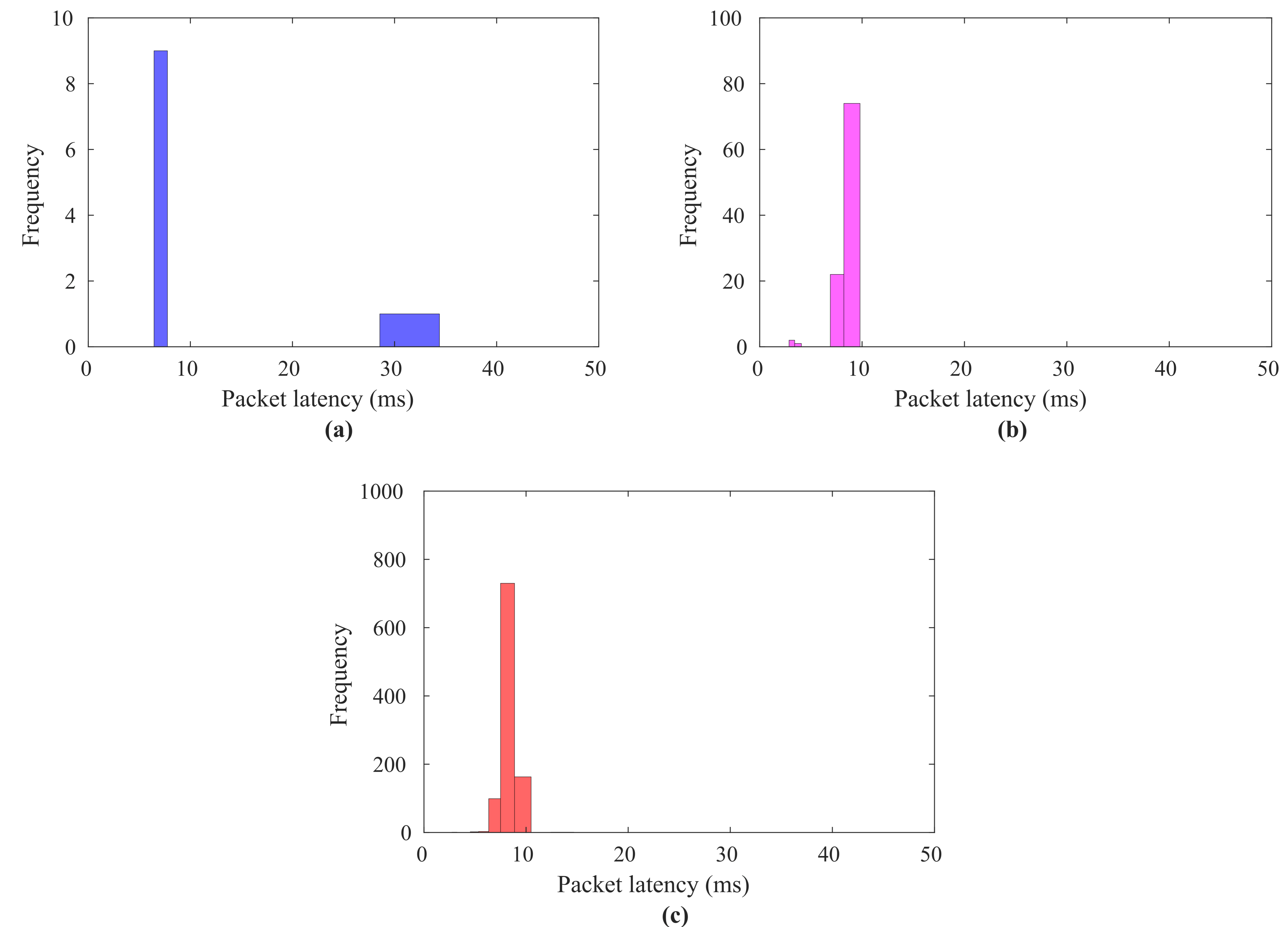
Figure 8.
Data packet latency analysis in terms of a histogram for real-time remote elder caring human–robot communication without edge-enabled activity and localization prediction model; (a) data packets = 10, (b) data packets = 100, (c) data packets = 1000.
These results show that there is a trend for E2E latency to reduce from 8.18 to 1.55 ms as the number of data packets increases. When there is only one data packet, as depicted in Figure 7a, the packet delay tends to be close to 8 ms, whereas Figure 7b,c depict a packet delay of less than 7 ms. To investigate this communication delay analysis in depth, Figure 8 explains the findings as a histogram of the packet delay. The latencies shown in Figure 8 show the most frequent occurrence of the data packets, contrasting with Figure 7.
Similar to Figure 7a–c, the experimental results in Figure 8a–c demonstrate a decrease in E2E packet latencies, with most of the latencies falling between 1 and 4 ms. Figure 8a indicates the frequency of the number of the packet under 2.5 ms is around 40%.
Figure 8b,c demonstrate that the latencies of the data (haptic, activity sensors) traffic decrease, which indicates the occurrence of the number of the data packets with latency under 2.5 ms is around 60%. It can be clearly seen from Figure 8a–c that the maximum data packet falls between 1 and 3 ms, which is one of the strict requirements for Internet of Senses (IoS) services. This demonstrates how the proposed framework would be able to offer elder remote caring service while adhering to QoS/QoE requirements (1–50 ms). However, the challenge is when we implement an activity and localization prediction model at the edge server on the master domain side to guide the human operator in the case of an anomaly and wrong activity on the remote side. So, the human operator controls the remote robot to perform the desired task accurately, with a focus on ensuring high QoT. In this regard, Figure 9 illustrates the analysis of the remote elder caring system with a prediction model in terms of the E2E round-trip delay.
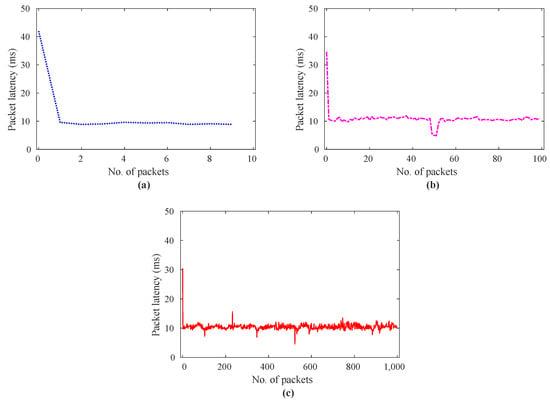
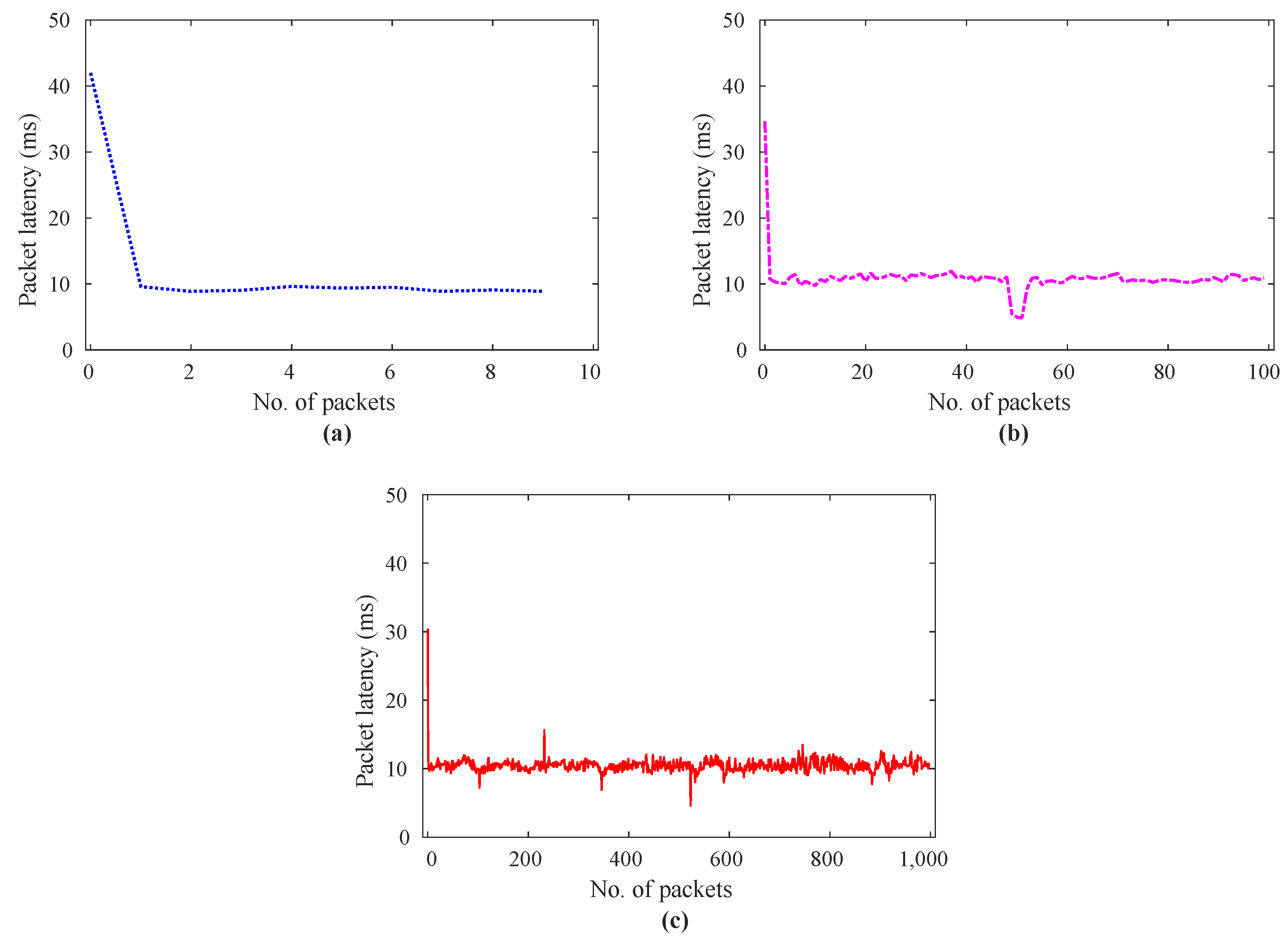
Figure 9.
Data packet latency analysis for real-time remote elder caring human–robot communication with edge-enabled activity prediction and localization model; (a) data packets = 10, (b) data packets = 100, (c) data packets = 1000.
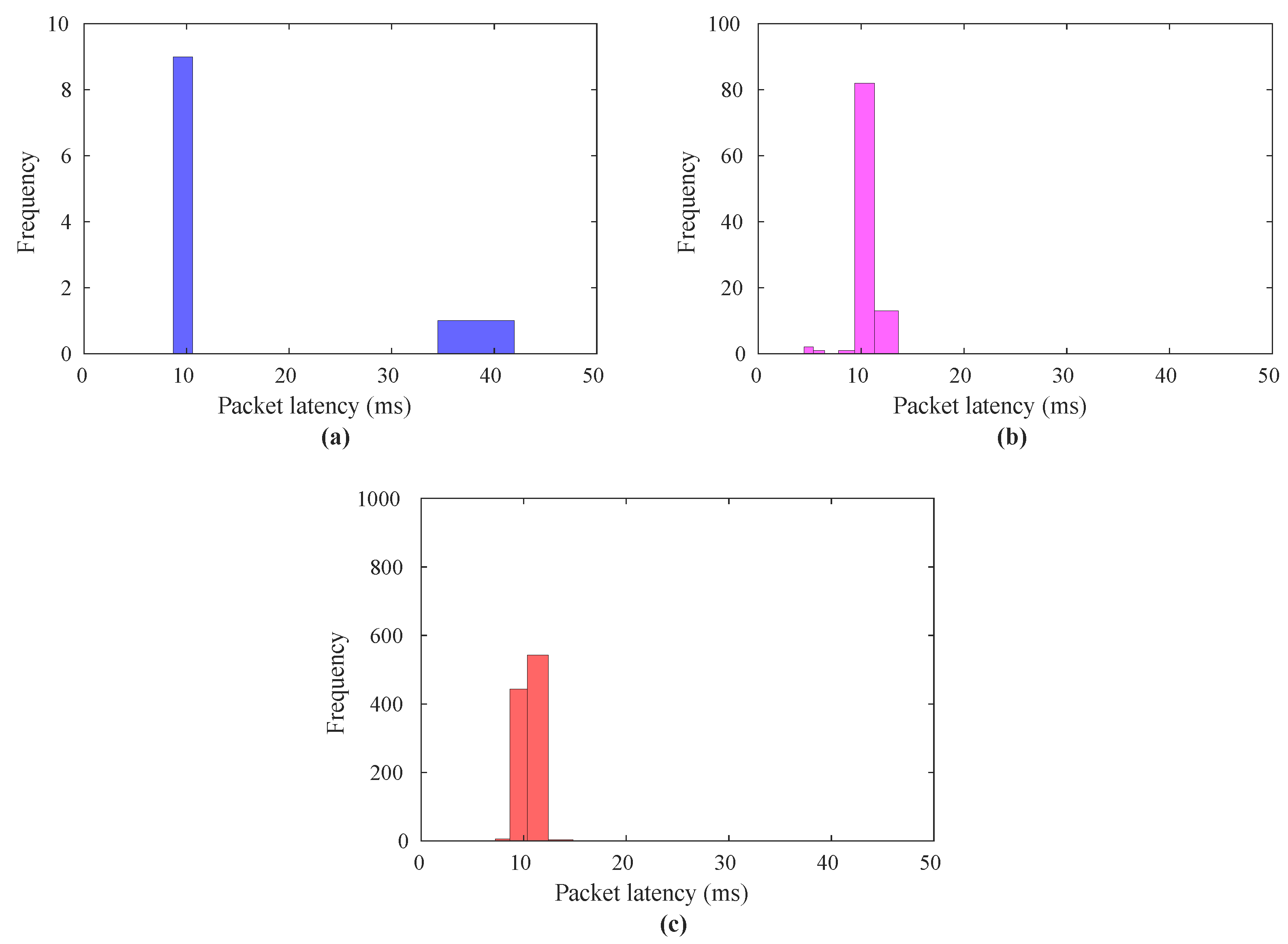
Figure 9a–c depicts the latency investigation between the robot (slave domain) and human operator (master domain) with the integration of the activity and localization prediction model in the ECI engine with the number of data packets ranging from 10 to 1000, respectively. These results also show that the network communication latency tends to decrease as the number of packets increases from 10 to 1000. The latency value in Figure 9a, where the number of packets is 10, lies between 41.97 and 9 ms. The packet latency approaches 42 ms when the number of data packets is 1, in contrast to Figure 9b,c, where packet delay is less than 35 ms. Figure 10a–c depict the histogram of the packet latencies to demonstrate the in-depth analysis. Figure 10a–c indicate that most of the latency of the packet lies between 9 and 14 ms, and the frequency of the number of packets under 11 ms is more than 60%. Figure 10a shows that the occurrence of the number of the data packets with latency under 12 ms is 95%. Similarly, Figure 10b,c show that the total number of the packets with latency under 12 ms is 100%. In Figure 9a–c, communication latency between master and slave with packets =10,100, and 1000 are 41.9–9, 35–11, and 31–10, respectively, compared to Figure 7a–c, where the value of latency lies between 8 and 2 ms. This investigation shows how the processing time of the prediction model causes E2E delays in data transmission.
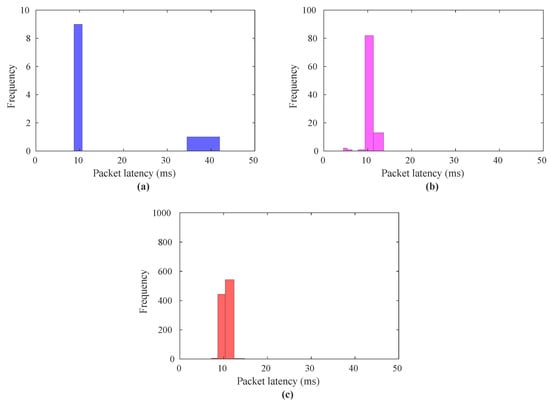
Figure 10.
Data packet latency analysis in terms of a histogram for real-time remote elder caring human–robot communication with edge-enabled activity and localization prediction model; (a) data packets = 10, (b) data packets = 100, (c) data packets = 1000.
To investigate the effect of the activity and localization prediction model processing for overall service latency, in-depth latency analysis was performed to capture prediction model processing and is depicted in Figure 11a–c. Similar to Figure 9a–c, the result in Figure 11a–c illustrates the edge-enabled prediction model processing time over the communication network, which is responsible for the extra delay in overall application delay. The result in Figure 11a–c also illustrates that the model processing time reduces for an increase in the number of data packets. It is clear from the histogram results in Figure 12a–c that the latency is more concentrated between 7 and 10 ms. It is noteworthy that as the number of data packets increases, along with a higher sampling rate, the proposed model exhibits lower processing time while meeting the application latency requirement. Moreover, we created complex network scenarios with varying parametric settings to evaluate the system’s performance. In these scenarios, different numbers of external hosts, ranging from 0 to 15, were connected near both the master and slave sides. During telecaring operations, these hosts also communicated with each other, simulating real-time dense network conditions. Detailed results from the experiments involving these dense networks are presented in the Supplementary File of this paper, and latency analysis is presented in Table 2, while a summary of the system’s reliability and stability is provided in Table 3.
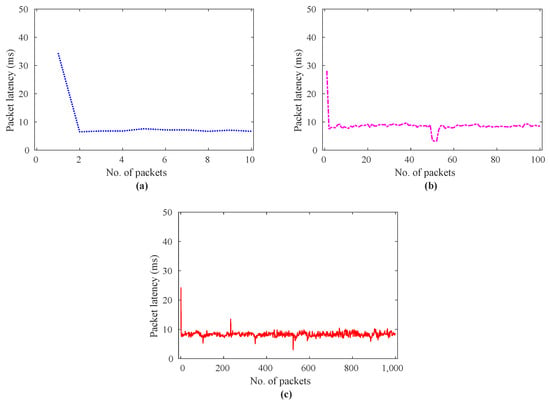
Figure 11.
Data packet latency analysis for edge-enabled activity and localization prediction model processing time; (a) data packets = 10, (b) data packets = 100, (c) data packets = 1000.
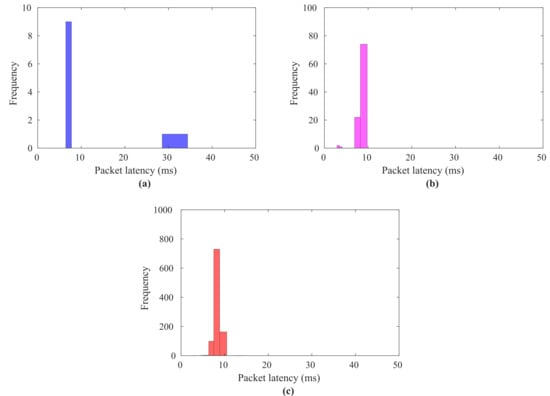
Figure 12.
Data packet latency analysis in terms of a histogram for edge-enabled activity and localization prediction model processing time; (a) data packets = 10, (b) data packets = 100, (c) data packets = 1000.
Table 2.
Summary of the results with complex network scenarios under different parametric settings.
Table 3.
Summary of the reliability characterization for haptic, activity, and localization sensors data transmission for real-time remote elder caring service with latency cutoff between 11∼15 ms.
Table 3 shows a comprehensive reliability analysis for the transmission of haptic, activity, and localization sensor data transmission between the remote robot and the master domain. The reliability of the data traffic is estimated based on its delayed/dropped and out-of-order packets. It can be seen from Table 1 that the percentage of delayed/lost packets drops from 33% to 18.50% (33 to 185 data packets), and the percentage of out-of-order sending packets drops from 16.16% to 8.50% with data packets 100 to 1000 when the number of external hosts = 0. The reason behind more delayed/ dropped data packets with packets = 100 than packets = 10 is that initially, ML models learn the hidden pattern from the data. Therefore, after learning the pattern, it takes less processing time with packets = 1000. Similarly, when considering data packets without ML models, the percentage of delayed or dropped packets remains at 0% and there are no out-of-order sending packets across the range of 10 to 1000 data packets. Similarly, the percentage of delayed/lost packets increases with the increase in the number of external hosts = 5, 10, and 15. This is due to the congestion in the communication network during external host communication. In this regard, in the future, we will use ML methods to estimate the network congestion level and select optimal network coding techniques to decrease the percentage of delayed/lost packets. On there other hand, the percentage of out-of-order data packets is high at the number of packets = 10, while it decreases with the higher number of packets. This indicates the system performance is also good with external hosts, having fewer out-of-order packets. A detailed analysis of the results in terms of data packet latency investigation and a histogram analysis are presented in the Supplementary File of this paper.
In this study, we developed an ECI-TeleCaring system to tackle critical issues such as reducing latency, providing personalized care, and ensuring system stability. Compared to existing telecare systems, our approach offers several key improvements. For example, the work in [29] focused on data privacy and scalability using blockchain and MEC, while our system emphasizes real-time interaction and adapts to the specific needs of each patient. Similarly, work in [30] designed a system that reduces latency and manages bandwidth efficiently but mainly supports video consultations and preliminary diagnoses. Our proposed system integrates AI at the edge to provide dynamic, personalized care that enhances both the quality and experience of elder care services. Other existing systems also have limitations that our ECI-based system overcomes. For instance, the authors in [31] improved healthcare access in remote areas by connecting urban and rural services but did not focus on real-time, personalized care, which is a key feature of our system. The study [32] enhanced telecare by managing uncertainties in patient data but did not fully address the need for stability and responsiveness in teleoperations. The work in [33] monitored health indicators like sleep and water usage to improve elderly care but lacked the AI-driven adaptability and personalization that our system provides.
4. Conclusions
This study proposed an Edge Computational Intelligence-based remote elderly care system called ECI-TeleCaring to improve the quality and efficiency of elderly care services. The proposed ECI-TeleCaring system utilizes SDN and MEC to tackle the challenges of high latency, inconsistent service quality, and inadequate personalized service in traditional caring services. Experimental evaluation demonstrates significant improvements in stability and responsiveness. The end-to-end communication delay decreases from 8.18 ms to 1.55 ms with the increase in number of data packets. Moreover, after deploying the activity and localization prediction model at the edge, the system maintains QoS and QoE requirements, resulting in 60∼95% data packets centered around 11∼12 ms for data packets ranging from 10 to 1000, respectively. We observed that the packet latency for most data packets is between 1 and 4 ms without the prediction model and between 9 and 14 ms with the prediction model. Experimental results also indicate a reliability improvement from 33% to 18.50% in delayed or dropped packets with the increase in number of data packets from 100 to 1000. In the future, one of our main goals is to optimize the system architecture further. We plan to undertake this by exploring other AI algorithms, such as reinforcement learning, for the SDN controller. This will help the system adapt better by estimating network congestion in real time and taking steps to reduce transmission delays, jitter, and packet loss, which are common issues in communication networks. We also want to improve the accuracy of our predictive models by using recent machine learning techniques and working with larger, more diverse datasets. Another key area of future work is to carry out extensive field experiments in different care settings. These experiments are important for testing how well the system performs and how reliable it is in real-world conditions, especially in elder care. Additionally, we plan to expand the proposed ECI-TeleCaring system’s functionality by adding more telecare services, such as better health monitoring features and improved user interfaces.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/app14188486/s1.
Author Contributions
Methodology, A.S.M.S.S. and M.Z.I.; software and coding, M.Z.I. and A.S.M.S.S.; experimentation and formal analysis, M.Z.I. and A.S.M.S.S.; writing—original draft preparation, M.Z.I. and A.S.M.S.S.; writing—review and editing, M.Z.I. and A.S.M.S.S.; supervision, H.S.K.; funding acquisition, M.Z.I. and H.S.K. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the National Research Foundation of Korea (NRF) Grant by the Korean Government through MSIT under Grant 2022R1F1A1063662 and the Strengthening R & D Capability Program of Sejong University.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The activity and localization datasets used in this work are made available online with open access for academic research use. The dataset is available online at https://github.com/zubair1811/ECI-Elderly-TeleCaring-Monitoring-System/tree/main/Activity-Localization-Dataset (accessed on 25 July 2024), and the simulation experiment results files are available at https://github.com/zubair1811/ECI-Elderly-TeleCaring-Monitoring-System.git (accessed on 25 July 2024).
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| URLLC | Ultrareliable and Low-Latency Communication |
| QoS | Quality of Service |
| QoE | Quality of Experience |
| QoT | Quality of Task |
| E2E | End to end |
| SDN | Software-Defined Network |
| MEC | Mobile Edge Computing |
| ECI | Edge Computational Intelligence |
References
- Ali, O.; Abdelbaki, W.; Shrestha, A.; Elbasi, E.; Alryalat, M.A.A.; Dwivedi, Y.K. A systematic literature review of artificial intelligence in the healthcare sector: Benefits, challenges, methodologies, and functionalities. J. Innov. Knowl. 2023, 8, 100333. [Google Scholar] [CrossRef]
- Boo, S.; Oh, H. Perceptions of registered nurses on facilitators and barriers of implementing the AI-IoT-based healthcare pilot project for older adults during the COVID-19 pandemic in South Korea. Front. Public Health 2023, 11, 1234626. [Google Scholar] [CrossRef] [PubMed]
- Alowais, S.A.; Alghamdi, S.S.; Alsuhebany, N.; Alqahtani, T.; Alshaya, A.I.; Almohareb, S.N.; Aldairem, A.; Alrashed, M.; Bin Saleh, K.; Badreldin, H.A.; et al. Revolutionizing healthcare: The role of artificial intelligence in clinical practice. BMC Med. Educ. 2023, 23, 689. [Google Scholar] [CrossRef]
- Cingolani, M.; Scendoni, R.; Fedeli, P.; Cembrani, F. Artificial intelligence and digital medicine for integrated home care services in Italy: Opportunities and limits. Front. Public Health 2023, 10, 1095001. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ageing and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 25 July 2024).
- Sawik, B.; Tobis, S.; Baum, E.; Suwalska, A.; Kropińska, S.; Stachnik, K.; Pérez-Bernabeu, E.; Cildoz, M.; Agustin, A.; Wieczorowska-Tobis, K. Robots for Elderly Care: Review, Multi-Criteria Optimization Model and Qualitative Case Study. Healthcare 2023, 11, 1286. [Google Scholar] [CrossRef]
- Padhan, S.; Mohapatra, A.; Ramasamy, S.K.; Agrawal, S. Artificial intelligence (AI) and robotics in elderly healthcare: Enabling independence and quality of life. Cureus 2023, 15, e42905. [Google Scholar] [CrossRef]
- Goeldner, M.; Herstatt, C.; Tietze, F. The emergence of care robotics—A patent and publication analysis. Technol. Forecast. Soc. Change 2015, 92, 115–131. [Google Scholar] [CrossRef]
- Brose, S.W.; Weber, D.J.; Salatin, B.A.; Grindle, G.G.; Wang, H.; Vazquez, J.J.; Cooper, R.A. The role of assistive robotics in the lives of persons with disability. Am. J. Phys. Med. Rehabil. 2010, 89, 509–521. [Google Scholar] [CrossRef]
- Mišeikis, J.; Caroni, P.; Duchamp, P.; Gasser, A.; Marko, R.; Mišeikienė, N.; Zwilling, F.; De Castelbajac, C.; Eicher, L.; Früh, M.; et al. Lio—A personal robot assistant for human-robot interaction and care applications. IEEE Robot. Autom. Lett. 2020, 5, 5339–5346. [Google Scholar] [CrossRef]
- Melkas, H.; Hennala, L.; Pekkarinen, S.; Kyrki, V. Impacts of robot implementation on care personnel and clients in elderly-care institutions. Int. J. Med. Inform. 2020, 134, 104041. [Google Scholar] [CrossRef]
- Carros, F.; Meurer, J.; Löffler, D.; Unbehaun, D.; Matthies, S.; Koch, I.; Wieching, R.; Randall, D.; Hassenzahl, M.; Wulf, V. Exploring human-robot interaction with the elderly: Results from a ten-week case study in a care home. In Proceedings of the 2020 CHI Conference on Human Factors in Computing Systems, Honolulu, HI, USA, 25–30 April 2020; pp. 1–12. [Google Scholar]
- Mello, R.C.; Ribeiro, M.R.; Frizera-Neto, A. Implementing cloud robotics for practical applications. Springer Tracts Adv. Robot. 2023, 10, 1–24. [Google Scholar]
- Ashok, K.; Gopikrishnan, S. Statistical analysis of remote health monitoring based IoT security models & deployments from a pragmatic perspective. IEEE Access 2023, 11, 2621–2651. [Google Scholar]
- Le, T.K.; Salim, U.; Kaltenberger, F. An overview of physical layer design for ultra-reliable low-latency communications in 3GPP releases 15, 16, and 17. IEEE Access 2020, 9, 433–444. [Google Scholar] [CrossRef]
- Lv, H.; Yang, G.; Zhou, H.; Huang, X.; Yang, H.; Pang, Z. Teleoperation of collaborative robot for remote dementia care in home environments. IEEE J. Transl. Eng. Health Med. 2020, 8, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulos, C.; Castro, N.; Nigath, A.; Davidson, R.; Faulkes, N.; Menicatti, R.; Khaliq, A.A.; Recchiuto, C.; Battistuzzi, L.; Randhawa, G.; et al. The CARESSES randomised controlled trial: Exploring the health-related impact of culturally competent artificial intelligence embedded into socially assistive robots and tested in older adult care homes. Int. J. Soc. Robot. 2022, 14, 245–256. [Google Scholar] [CrossRef]
- Johansson-Pajala, R.M.; Gustafsson, C. Significant challenges when introducing care robots in Swedish elder care. Disabil. Rehabil. Assist. Technol. 2022, 17, 166–176. [Google Scholar] [CrossRef]
- Cifuentes, C.A.; Pinto, M.J.; Céspedes, N.; Múnera, M. Social robots in therapy and care. Curr. Robot. Rep. 2020, 1, 59–74. [Google Scholar] [CrossRef]
- Zhang, C.; Su, L. An IoMT Framework Integrating 5G and Wireless Body Area Networks for Home Healthcare. In Proceedings of the 2024 3rd International Conference on Networks, Communications and Information Technology, Xi’an, China, 7–9 June 2024; pp. 166–171. [Google Scholar]
- Ghosh, S.; Ghosh, S.K. Feel: Federated learning framework for elderly healthcare using edge-iomt. IEEE Trans. Comput. Soc. Syst. 2023, 10, 1800–1809. [Google Scholar] [CrossRef]
- Jazaeri, S.S.; Asghari, P.; Jabbehdari, S.; Javadi, H.H.S. Composition of caching and classification in edge computing based on quality optimization for SDN-based IoT healthcare solutions. J. Supercomput. 2023, 79, 17619–17669. [Google Scholar] [CrossRef]
- Ahmed, A.S.; Salah, H.A. Development a Software Defined Network (SDN) with Internet of Things (IoT) Security for Medical Issues. J. AI-Qadisiyah Comput. Sci. Math. 2023, 15, 98. [Google Scholar] [CrossRef]
- Alnaim, A.K.; Alwakeel, A.M. Machine-learning-based IoT–edge computing healthcare solutions. Electronics 2023, 12, 1027. [Google Scholar] [CrossRef]
- Hoeiland-Joergensen, T.; McKenney, P.; Taht, D.; Gettys, J.; Dumazet, E. The Flow Queue Codel Packet Scheduler and Active Queue Management Algorithm. RFC 8290, January 2018. Available online: https:///tools.ietf.org/html/rfc8290 (accessed on 25 July 2024).
- Holland, O.; Steinbach, E.; Prasad, R.V.; Liu, Q.; Dawy, Z.; Aijaz, A.; Pappas, N.; Chandra, K.; Rao, V.S.; Oteafy, S.; et al. The IEEE 1918.1 “tactile internet” standards working group and its standards. Proc. IEEE 2019, 107, 256–279. [Google Scholar] [CrossRef]
- Malik, T.S.; Tanveer, J.; Anwar, S.; Mufti, M.R.; Afzal, H.; Kim, A. An Efficient and Secure Fog Based Routing Mechanism in IoT Network. Mathematics 2023, 11, 3652. [Google Scholar] [CrossRef]
- Hosseinzadeh, M.; Tanveer, J.; Masoud Rahmani, A.; Yousefpoor, E.; Sadegh Yousefpoor, M.; Khan, F.; Haider, A. A cluster-tree-based secure routing protocol using dragonfly algorithm (DA) in the Internet of Things (IoT) for smart agriculture. Mathematics 2022, 11, 80. [Google Scholar] [CrossRef]
- Hewa, T.; Braeken, A.; Ylianttila, M.; Liyanage, M. Multi-access edge computing and blockchain-based secure telehealth system connected with 5G and IoT. In Proceedings of the GLOBECOM 2020–2020 IEEE Global Communications Conference, Taipei, Taiwan, 7–11 December 2020; pp. 1–6. [Google Scholar]
- Dilibal, Ç. Development of edge-IoMT computing architecture for smart healthcare monitoring platform. In Proceedings of the 2020 4th International Symposium on Multidisciplinary Studies and Innovative Technologies (ISMSIT), Istanbul, Turkey, 22–24 October 2020; pp. 1–4. [Google Scholar]
- Humayun, M.; Almufareh, M.F.; Al-Quayed, F.; Alateyah, S.A.; Alatiyyah, M. Improving Healthcare Facilities in Remote Areas Using Cutting-Edge Technologies. Appl. Sci. 2023, 13, 6479. [Google Scholar] [CrossRef]
- Kordestani, H.; Mojarad, R.; Chibani, A.; Barkaoui, K.; Amirat, Y.; Zahran, W. Extended Hapicare: A telecare system with probabilistic diagnosis and self-adaptive treatment. Expert Syst. Appl. 2021, 186, 115749. [Google Scholar] [CrossRef]
- Tang, Z.; Jiang, L.; Zhu, X.; Huang, M. An Internet of Things-Based Home Telehealth System for Smart Healthcare by Monitoring Sleep and Water Usage: A Preliminary Study. Electronics 2023, 12, 3652. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).