
Effects of Toe Tube Training on Intrinsic Foot Muscle Strength and Reactive Strength Index in Runners: A Randomized Controlled Trial


Abstract
1. Introduction
2. Materials and Methods
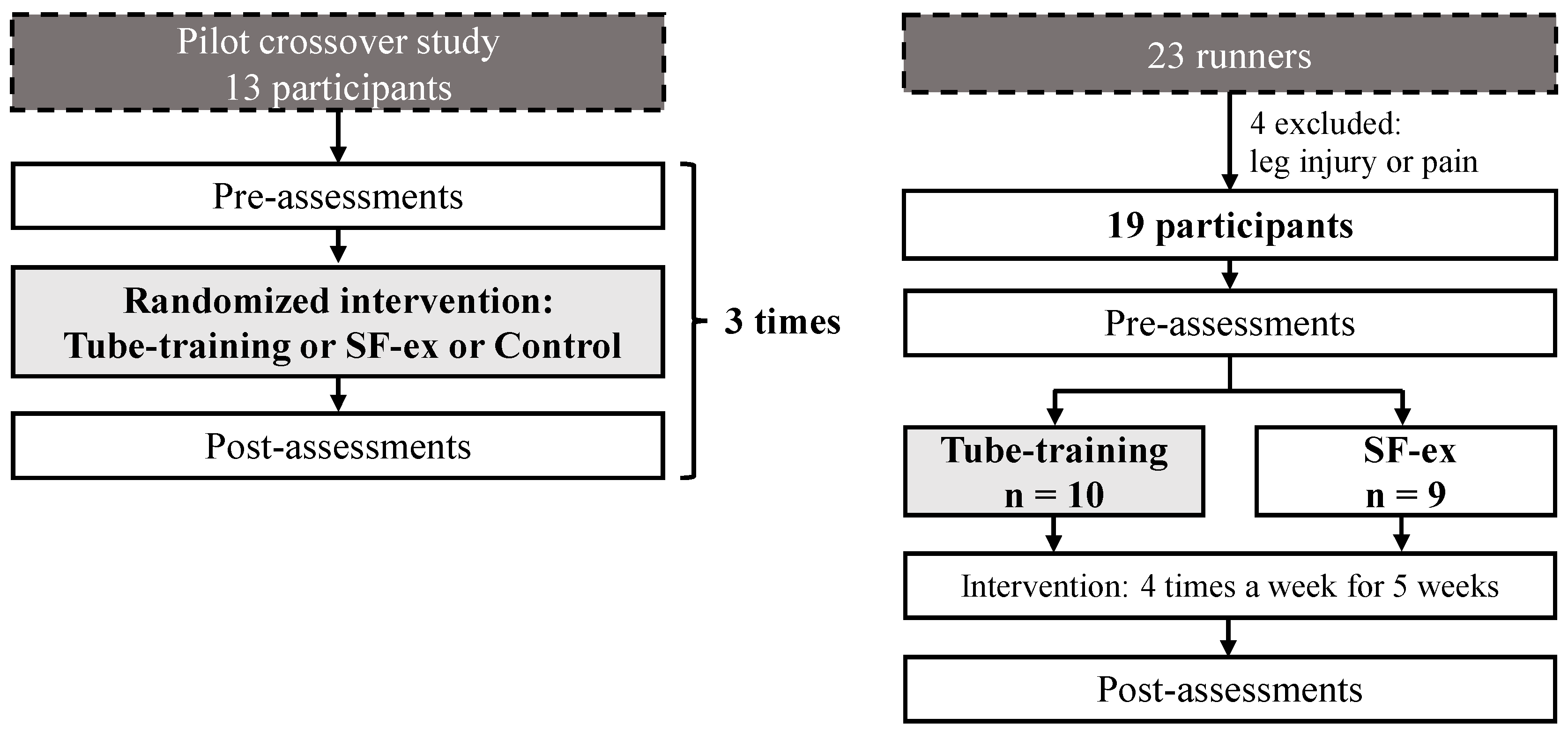
2.1. Participants
2.2. Ethics
2.3. Procedures
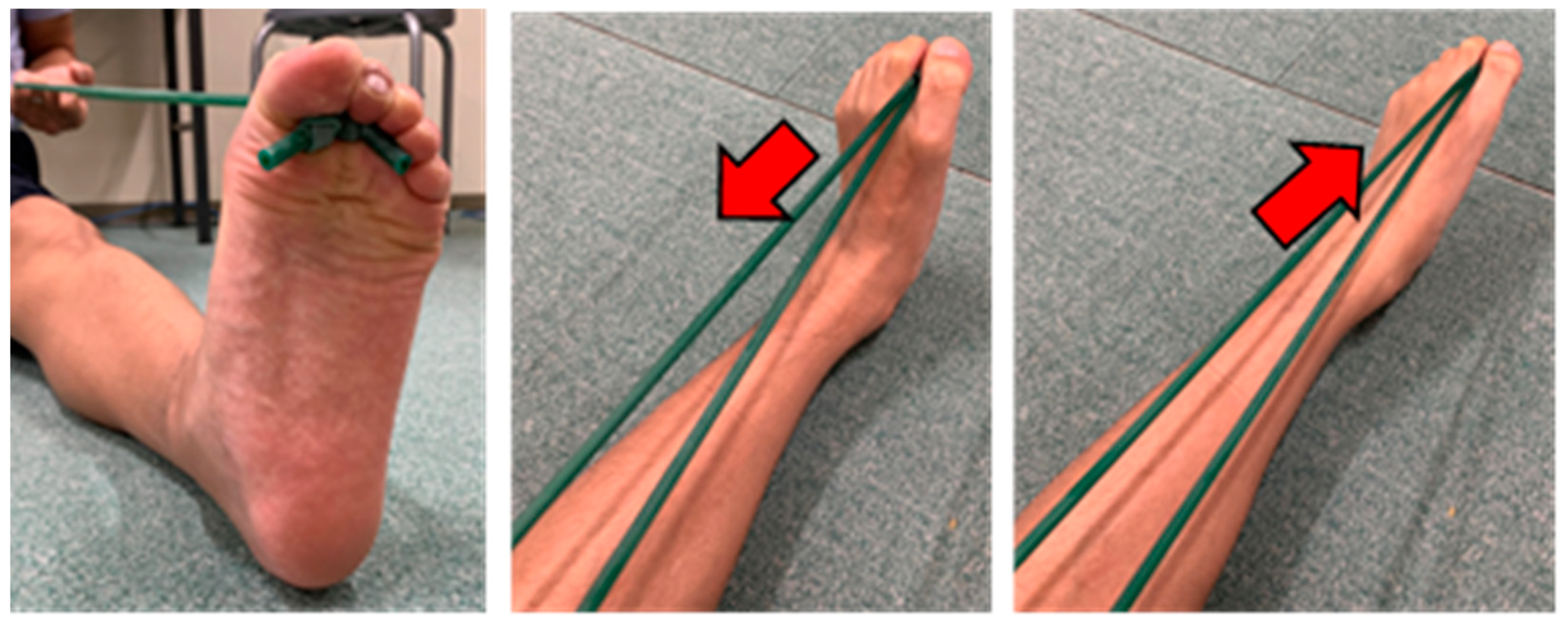
2.4. Intervention Methods
2.5. Data Collection and Analysis Methods
2.6. Statistical Analysis
3. Results
4. Discussion
4.1. Interpretation of Results
4.2. Practical Implications
4.3. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- van Gent, R.N.; Siem, D.; van Middelkoop, M.; van Os, A.G.; Bierma-Zeinstra, S.M.A.; Koes, B.W. Incidence and Determinants of Lower Extremity Running Injuries in Long Distance Runners: A Systematic Review. Br. J. Sports Med. 2007, 41, 469–480; discussion 480. [Google Scholar] [CrossRef] [PubMed]
- Kelly, L.A.; Cresswell, A.G.; Racinais, S.; Whiteley, R.; Lichtwark, G. Intrinsic Foot Muscles Have the Capacity to Control Deformation of the Longitudinal Arch. J. R. Soc. Interface 2014, 11, 20131188. [Google Scholar] [CrossRef] [PubMed]
- Lynn, S.K.; Padilla, R.A.; Tsang, K.K.W. Differences in Static- and Dynamic-Balance Task Performance after 4 Weeks of Intrinsic-Foot-Muscle Training: The Short-Foot Exercise versus the Towel-Curl Exercise. J. Sport Rehabil. 2012, 21, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Taddei, U.T.; Matias, A.B.; Ribeiro, F.I.A.; Inoue, R.S.; Bus, S.A.; Sacco, I.C.N. Effects of a Therapeutic Foot Exercise Program on Injury Incidence, Foot Functionality and Biomechanics in Long-Distance Runners: Feasibility Study for a Randomized Controlled Trial. Phys. Ther. Sport 2018, 34, 216–226. [Google Scholar] [CrossRef] [PubMed]
- Unger, C.L.; Wooden, M.J. Effect of Foot Intrinsic Muscle Strength Training on Jump Performance. J. Strength Cond. Res. 2000, 14, 373–378. [Google Scholar] [CrossRef]
- Gooding, T.M.; Feger, M.A.; Hart, J.M.; Hertel, J. Intrinsic Foot Muscle Activation During Specific Exercises: A T2 Time Magnetic Resonance Imaging Study. J. Athl. Train. 2016, 51, 644–650. [Google Scholar] [CrossRef]
- Kusagawa, Y.; Kurihara, T.; Maeo, S.; Sugiyama, T.; Kanehisa, H.; Isaka, T. Associations between the Size of Individual Plantar Intrinsic and Extrinsic Foot Muscles and Toe Flexor Strength. J. Foot Ankle Res. 2022, 15, 22. [Google Scholar] [CrossRef]
- Zhang, X.; Pauel, R.; Deschamps, K.; Jonkers, I.; Vanwanseele, B. Differences in Foot Muscle Morphology and Foot Kinematics between Symptomatic and Asymptomatic Pronated Feet. Scand. J. Med. Sci. Sports 2019, 29, 1766–1773. [Google Scholar] [CrossRef]
- McKeon, P.O.; Fourchet, F. Freeing the Foot: Integrating the Foot Core System into Rehabilitation for Lower Extremity Injuries. Clin. Sports Med. 2015, 34, 347–361. [Google Scholar] [CrossRef]
- Tourillon, R.; Gojanovic, B.; Fourchet, F. How to Evaluate and Improve Foot Strength in Athletes: An Update. Front. Sport. Act. Living 2019, 1, 46. [Google Scholar] [CrossRef]
- Ooi, T.C.; Mat Ludin, A.F.; Loke, S.C.; Fiatarone Singh, M.A.; Wong, T.W.; Vytialingam, N.; Anthony Abdullah, M.M.J.; Ng, O.C.; Bahar, N.; Zainudin, N.; et al. A 16-Week Home-Based Progressive Resistance Tube Training Among Older Adults With Type-2 Diabetes Mellitus: Effect on Glycemic Control. Gerontol. Geriatr. Med. 2021, 7, 23337214211038788. [Google Scholar] [CrossRef] [PubMed]
- Makizako, H.; Nakai, Y.; Tomioka, K.; Taniguchi, Y.; Sato, N.; Wada, A.; Kiyama, R.; Tsutsumimoto, K.; Ohishi, M.; Kiuchi, Y.; et al. Effects of a Multicomponent Exercise Program in Physical Function and Muscle Mass in Sarcopenic/Pre-Sarcopenic Adults. J. Clin. Med. 2020, 9, 1386. [Google Scholar] [CrossRef] [PubMed]
- Souza, D.; Barbalho, M.; Vieira, C.A.; Martins, W.R.; Cadore, E.L.; Gentil, P. Minimal Dose Resistance Training with Elastic Tubes Promotes Functional and Cardiovascular Benefits to Older Women. Exp. Gerontol. 2019, 115, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, T.; Sakuraba, K. Strength Training for the Intrinsic Flexor Muscles of the Foot: Effects on Muscle Strength, the Foot Arch, and Dynamic Parameters before and after the Training. J. Phys. Ther. Sci. 2014, 26, 373–376. [Google Scholar] [CrossRef] [PubMed]
- Wager, J.C.; Challis, J.H. Mechanics of the Foot and Ankle Joints during Running Using a Multi-Segment Foot Model Compared with a Single-Segment Model. PLoS ONE 2024, 19, e0294691. [Google Scholar] [CrossRef]
- Krell, J.B.; Stefanyshyn, D.J. The Relationship between Extension of the Metatarsophalangeal Joint and Sprint Time for 100 m Olympic Athletes. J. Sports Sci. 2006, 24, 175–180. [Google Scholar] [CrossRef]
- Bezodis, N.E.; Salo, A.I.T.; Trewartha, G. Modeling the Stance Leg in Two-Dimensional Analyses of Sprinting: Inclusion of the MTP Joint Affects Joint Kinetics. J. Appl. Biomech. 2012, 28, 222–227. [Google Scholar] [CrossRef]
- Stefanyshyn, D.J.; Nigg, B.M. Mechanical Energy Contribution of the Metatarsophalangeal Joint to Running and Sprinting. J. Biomech. 1997, 30, 1081–1085. [Google Scholar] [CrossRef]
- Smith, G.; Lake, M.; Lees, A. Metatarsophalangeal Joint Function during Sprinting: A Comparison of Barefoot and Sprint Spike Shod Foot Conditions. J. Appl. Biomech. 2014, 30, 206–212. [Google Scholar] [CrossRef]
- Farris, D.J.; Kelly, L.A.; Cresswell, A.G.; Lichtwark, G.A. The Functional Importance of Human Foot Muscles for Bipedal Locomotion. Proc. Natl. Acad. Sci. USA 2019, 116, 1645–1650. [Google Scholar] [CrossRef]
- Day, E.M.; Hahn, M.E. Increased Toe-Flexor Muscle Strength Does Not Alter Metatarsophalangeal and Ankle Joint Mechanics or Running Economy. J. Sports Sci. 2019, 37, 2702–2710. [Google Scholar] [CrossRef] [PubMed]
- Okamura, K.; Fukuda, K.; Oki, S.; Ono, T.; Tanaka, S.; Kanai, S. Effects of Plantar Intrinsic Foot Muscle Strengthening Exercise on Static and Dynamic Foot Kinematics: A Pilot Randomized Controlled Single-Blind Trial in Individuals with Pes Planus. Gait Posture 2020, 75, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Mulligan, E.P.; Cook, P.G. Effect of Plantar Intrinsic Muscle Training on Medial Longitudinal Arch Morphology and Dynamic Function. Man. Ther. 2013, 18, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Borg, E.; Borg, G.; Larsson, K.; Letzter, M.; Sundblad, B.-M. An Index for Breathlessness and Leg Fatigue. Scand. J. Med. Sci. Sports 2010, 20, 644–650. [Google Scholar] [CrossRef]
- Zamunér, A.R.; Moreno, M.A.; Camargo, T.M.; Graetz, J.P.; Rebelo, A.C.S.; Tamburús, N.Y.; da Silva, E. Assessment of Subjective Perceived Exertion at the Anaerobic Threshold with the Borg CR-10 Scale. J. Sports Sci. Med. 2011, 10, 130–136. [Google Scholar]
- Hirono, T.; Ikezoe, T.; Taniguchi, M.; Nojiri, S.; Tanaka, H.; Ichihashi, N. Acute Effects of Repetitive Peripheral Magnetic Stimulation Following Low-Intensity Isometric Exercise on Muscle Swelling for Selective Muscle in Healthy Young Men. Electromagn. Biol. Med. 2021, 40, 420–427. [Google Scholar] [CrossRef]
- Hirono, T.; Ikezoe, T.; Nakamura, M.; Tanaka, H.; Umehara, J.; Ichihashi, N. Acute Effects of Low-Load Resistance Exercise with Different Rest Periods on Muscle Swelling in Healthy Young Men. J. Phys. Fit. Sport. Med. 2019, 8, 165–171. [Google Scholar] [CrossRef]
- Protopapas, K.; Perry, S.D. The Effect of a 12-Week Custom Foot Orthotic Intervention on Muscle Size and Muscle Activity of the Intrinsic Foot Muscle of Young Adults during Gait Termination. Clin. Biomech. 2020, 78, 105063. [Google Scholar] [CrossRef]
- Uritani, D.; Fukumoto, T.; Matsumoto, D. Intrarater and Interrater Reliabilitiesfor a Toe Grip Dynamometer. J. Phys. Ther. Sci. 2012, 24, 639–643. [Google Scholar] [CrossRef]
- Yamashita, K.; Umezawa, J.; Nomoto, Y.; Ino, S.; Ifukube, T.; Koyama, H.; Kawasumi, M. The Role of Toe-Gap Force for the Evaluation of Falling Risk on the Elderly. In World Congress on Medical Physics and Biomedical Engineering 2006; Springer: Berlin/Heidelberg, Germany, 2007; Volume 14, pp. 405–408. ISBN 9783540368397. [Google Scholar]
- McMaster, D.T.; Gill, N.; Cronin, J.; McGuigan, M. A Brief Review of Strength and Ballistic Assessment Methodologies in Sport. Sports Med. 2014, 44, 603–623. [Google Scholar] [CrossRef]
- Yamauchi, J.; Koyama, K. Importance of Toe Flexor Strength in Vertical Jump Performance. J. Biomech. 2020, 104, 109719. [Google Scholar] [CrossRef] [PubMed]
- Balsalobre-Fernández, C.; Glaister, M.; Lockey, R.A. The Validity and Reliability of an IPhone App for Measuring Vertical Jump Performance. J. Sports Sci. 2015, 33, 1574–1579. [Google Scholar] [CrossRef] [PubMed]
- Bosco, C.; Luhtanen, P.; Komi, P.V. A Simple Method for Measurement of Mechanical Power in Jumping. Eur. J. Appl. Physiol. Occup. Physiol. 1983, 50, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Haynes, T.; Bishop, C.; Antrobus, M.; Brazier, J. The Validity and Reliability of the My Jump 2 App for Measuring the Reactive Strength Index and Drop Jump Performance. J. Sports Med. Phys. Fitness 2019, 59, 253–258. [Google Scholar] [CrossRef]
- Liu, C.; Liu, X.-N.; Wang, G.-L.; Hei, Y.; Meng, S.; Yang, L.-F.; Yuan, L.; Xie, Y. A Dual-Mediated Liposomal Drug Delivery System Targeting the Brain: Rational Construction, Integrity Evaluation across the Blood-Brain Barrier, and the Transporting Mechanism to Glioma Cells. Int. J. Nanomed. 2017, 12, 2407–2425. [Google Scholar] [CrossRef]
- Richardson, J.T.E. Eta Squared and Partial Eta Squared as Measures of Effect Size in Educational Research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 1988; ISBN 9781134742707. [Google Scholar]
- Jastifer, J.R. Intrinsic Muscles of the Foot: Anatomy, Function, Rehabilitation. Phys. Ther. Sport 2023, 61, 27–36. [Google Scholar] [CrossRef]
- Péter, A.; Hegyi, A.; Stenroth, L.; Finni, T.; Cronin, N.J. EMG and Force Production of the Flexor Hallucis Longus Muscle in Isometric Plantarflexion and the Push-off Phase of Walking. J. Biomech. 2015, 48, 3413–3419. [Google Scholar] [CrossRef]
- Zelik, K.E.; La Scaleia, V.; Ivanenko, Y.P.; Lacquaniti, F. Coordination of Intrinsic and Extrinsic Foot Muscles during Walking. Eur. J. Appl. Physiol. 2015, 115, 691–701. [Google Scholar] [CrossRef]
- García-Pinillos, F.; Lago-Fuentes, C.; Latorre-Román, P.A.; Pantoja-Vallejo, A.; Ramirez-Campillo, R. Jump-Rope Training: Improved 3-Km Time-Trial Performance in Endurance Runners via Enhanced Lower-Limb Reactivity and Foot-Arch Stiffness. Int. J. Sports Physiol. Perform. 2020, 15, 927–933. [Google Scholar] [CrossRef]
- Yamauchi, J.; Ishii, N. Relations between Force-Velocity Characteristics of the Knee-Hip Extension Movement and Vertical Jump Performance. J. Strength Cond. Res. 2007, 21, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Dowling, J.J.; Vamos, L. Identification of Kinetic and Temporal Factors Related to Vertical Jump Performance. J. Appl. Biomech. 1993, 9, 95–110. [Google Scholar] [CrossRef]
- Goldmann, J.-P.; Sanno, M.; Willwacher, S.; Heinrich, K.; Brüggemann, G.-P. The Potential of Toe Flexor Muscles to Enhance Performance. J. Sports Sci. 2013, 31, 424–433. [Google Scholar] [CrossRef]
- Yamauchi, J.; Koyama, K. Relation between the Ankle Joint Angle and the Maximum Isometric Force of the Toe Flexor Muscles. J. Biomech. 2019, 85, 1–5. [Google Scholar] [CrossRef]
- Plisky, M.S.; Rauh, M.J.; Heiderscheit, B.; Underwood, F.B.; Tank, R.T. Medial Tibial Stress Syndrome in High School Cross-Country Runners: Incidence and Risk Factors. J. Orthop. Sports Phys. Ther. 2007, 37, 40–47. [Google Scholar] [CrossRef]
- Yagi, S.; Muneta, T.; Sekiya, I. Incidence and Risk Factors for Medial Tibial Stress Syndrome and Tibial Stress Fracture in High School Runners. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 556–563. [Google Scholar] [CrossRef]
- Moen, M.H.; Tol, J.L.; Weir, A.; Steunebrink, M.; De Winter, T.C. Medial Tibial Stress Syndrome: A Critical Review. Sports Med. 2009, 39, 523–546. [Google Scholar] [CrossRef]
- Page, P.; Ellenbecker, T.S. The Scientific and Clinical Application of Elastic Resistance; Human Kinetics: Champaign, IL, USA, 2003; ISBN 0736036881. [Google Scholar]
- Edwards, A.M.; Wells, C.; Butterly, R. Concurrent Inspiratory Muscle and Cardiovascular Training Differentially Improves Both Perceptions of Effort and 5000 m Running Performance Compared with Cardiovascular Training Alone. Br. J. Sports Med. 2008, 42, 823–827. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Tube Training Group (n = 10) | SF-ex Group (n = 9) | p | |
|---|---|---|---|
| Age, years | 19.4 ± 1.2 | 20.0 ± 1.5 | 0.342 |
| Body height, cm | 170.4 ± 4.1 | 168.7 ± 0.4 | 0.394 |
| Body weight, kg | 54.5 ± 3.2 | 53.6 ± 2.6 | 0.439 |
| BMI, kg/m2 | 18.8 ± 0.5 | 18.8 ± 1.0 | 0.948 |
| Toe grip strength, kgf | 19.4 ± 4.3 | 20.1 ± 4.9 | 0.715 |
| Toe gap strength, kgf | 3.2 ± 0.9 | 3.7 ± 1.1 | 0.306 |
| RSI | 2.3 ± 0.3 | 2.4 ± 0.4 | 0.625 |
| Between-Group Differences | |||||||
|---|---|---|---|---|---|---|---|
| Main Effect by Time | Interaction | ||||||
| F-Value | p | Partial η2 | F-Value | p | Partial η2 | ||
| Toe grip strength | Tube training | 25.64 | <0.001 ** | 0.60 | 0.270 | 0.610 | 0.02 |
| SF-ex | |||||||
| Toe grip strength | Tube training | 11.26 | 0.004 ** | 0.40 | 0.656 | 0.429 | 0.04 |
| SF-ex | |||||||
| RSI | Tube training | 4.81 | 0.042 * | 0.22 | 0.670 | 0.424 | 0.04 |
| SF-ex | |||||||
| Within-Group Differences | ||||||
|---|---|---|---|---|---|---|
| Pre-Intervention | Post-Intervention | Difference [95% CI] | p | Cohen’s d [95% CI] | ||
| Toe grip strength | Tube training | 19.4 ± 4.3 | 23.3 ± 3.6 | 3.98 [1.91, 6.05] | 0.002 ** | 1.37 [0.48, 2.24] |
| SF-ex | 20.1 ± 4.9 | 23.4 ± 4.4 | 3.24 [0.69, 5.80] | 0.019 * | 0.98 [0.15, 1.76] | |
| Toe gap strength | Tube training | 3.2 ± 0.9 | 3.8 ± 0.9 | 0.60 [0.29, 0.91] | 0.002 ** | 1.37 [0.48, 2.24] |
| SF-ex | 3.7 ± 1.1 | 4.1 ± 1.2 | 0.37 [−0.24, 0.97] | 0.200 | 0.46 [−0.24, 1.14] | |
| RSI | Tube training | 2.33 ± 0.31 | 2.55 ± 0.39 | 0.22 [0.01, 0.44] | 0.046 * | 0.73 [0.01, 1.42] |
| SF-ex | 2.41 ± 0.44 | 2.51 ± 0.62 | 0.10 [−0.16, 0.36] | 0.396 | 0.30 [−0.38, 0.96] | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakai, Y.; Takeshita, Y. Effects of Toe Tube Training on Intrinsic Foot Muscle Strength and Reactive Strength Index in Runners: A Randomized Controlled Trial. Appl. Sci. 2024, 14, 10514. https://doi.org/10.3390/app142210514
Nakai Y, Takeshita Y. Effects of Toe Tube Training on Intrinsic Foot Muscle Strength and Reactive Strength Index in Runners: A Randomized Controlled Trial. Applied Sciences. 2024; 14(22):10514. https://doi.org/10.3390/app142210514
Chicago/Turabian StyleNakai, Yuki, and Yasufumi Takeshita. 2024. "Effects of Toe Tube Training on Intrinsic Foot Muscle Strength and Reactive Strength Index in Runners: A Randomized Controlled Trial" Applied Sciences 14, no. 22: 10514. https://doi.org/10.3390/app142210514
APA StyleNakai, Y., & Takeshita, Y. (2024). Effects of Toe Tube Training on Intrinsic Foot Muscle Strength and Reactive Strength Index in Runners: A Randomized Controlled Trial. Applied Sciences, 14(22), 10514. https://doi.org/10.3390/app142210514