
Prediction of Lower Leg Swelling in Driving Posture


Abstract
1. Introduction
1.1. Passenger Physical Fatigue
1.2. Lower Leg Swelling
1.3. Purpose of the Study and Structure of This Paper
2. Methods
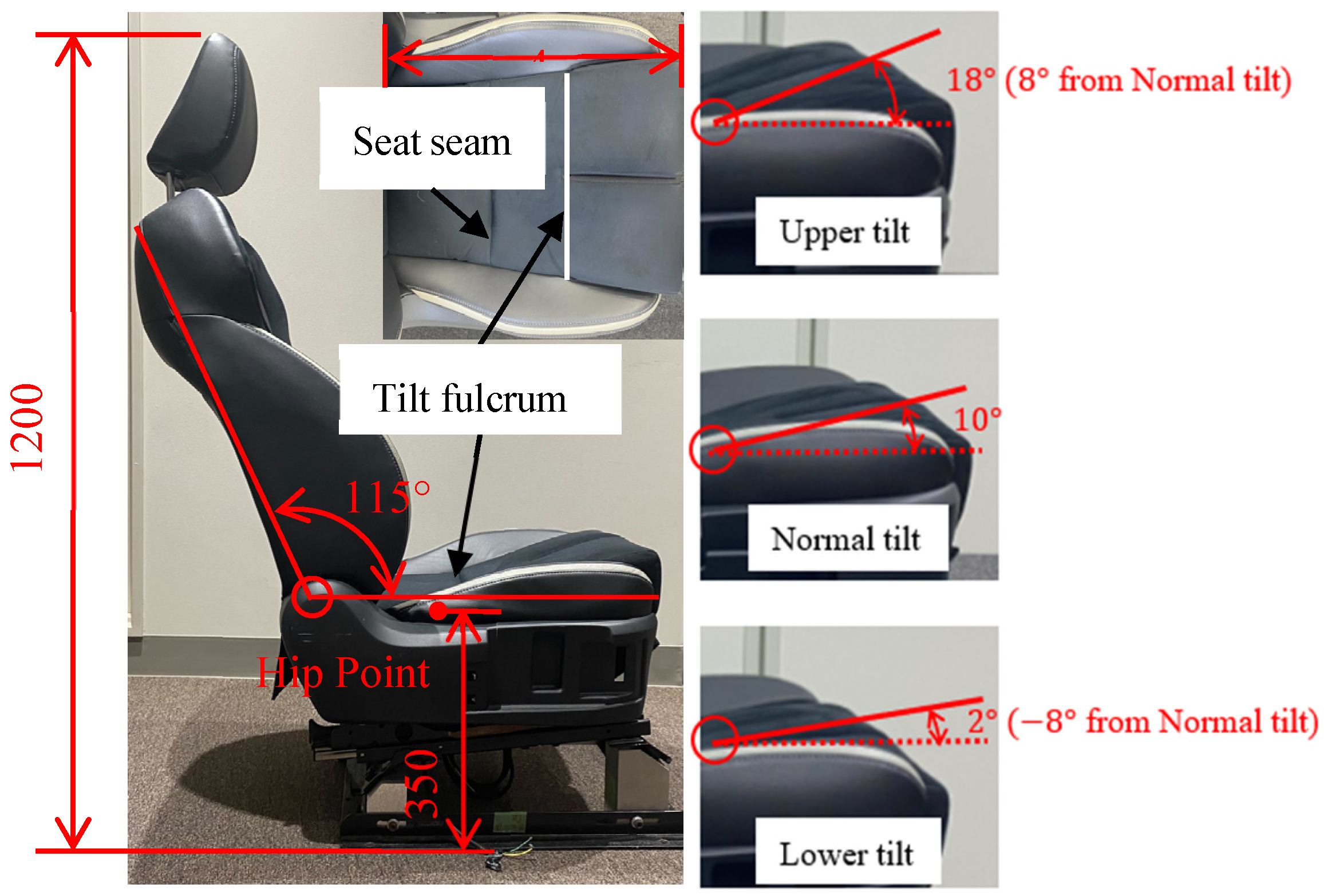
2.1. Automobile Seat
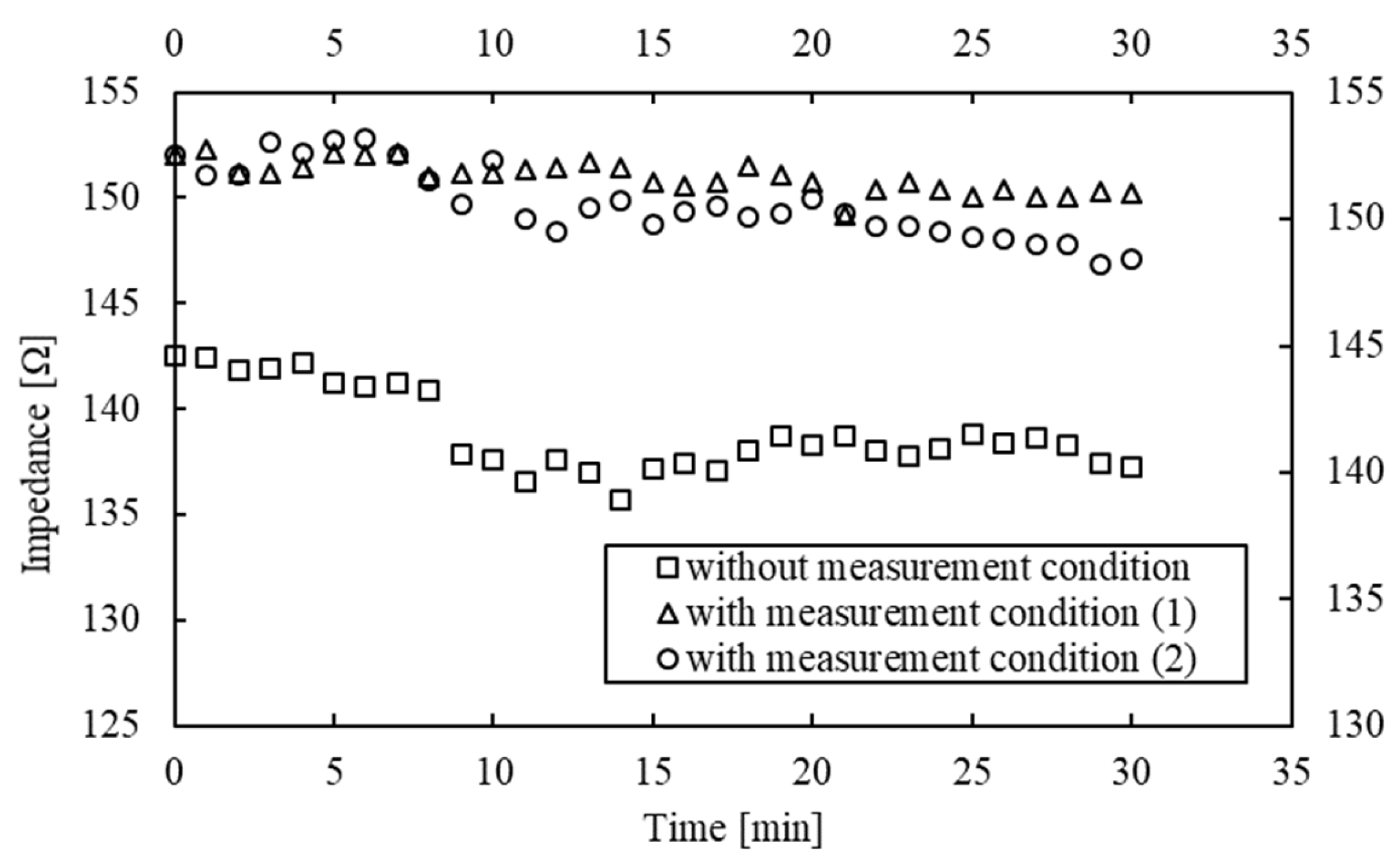
2.2. Measurement of Lower Leg Swelling
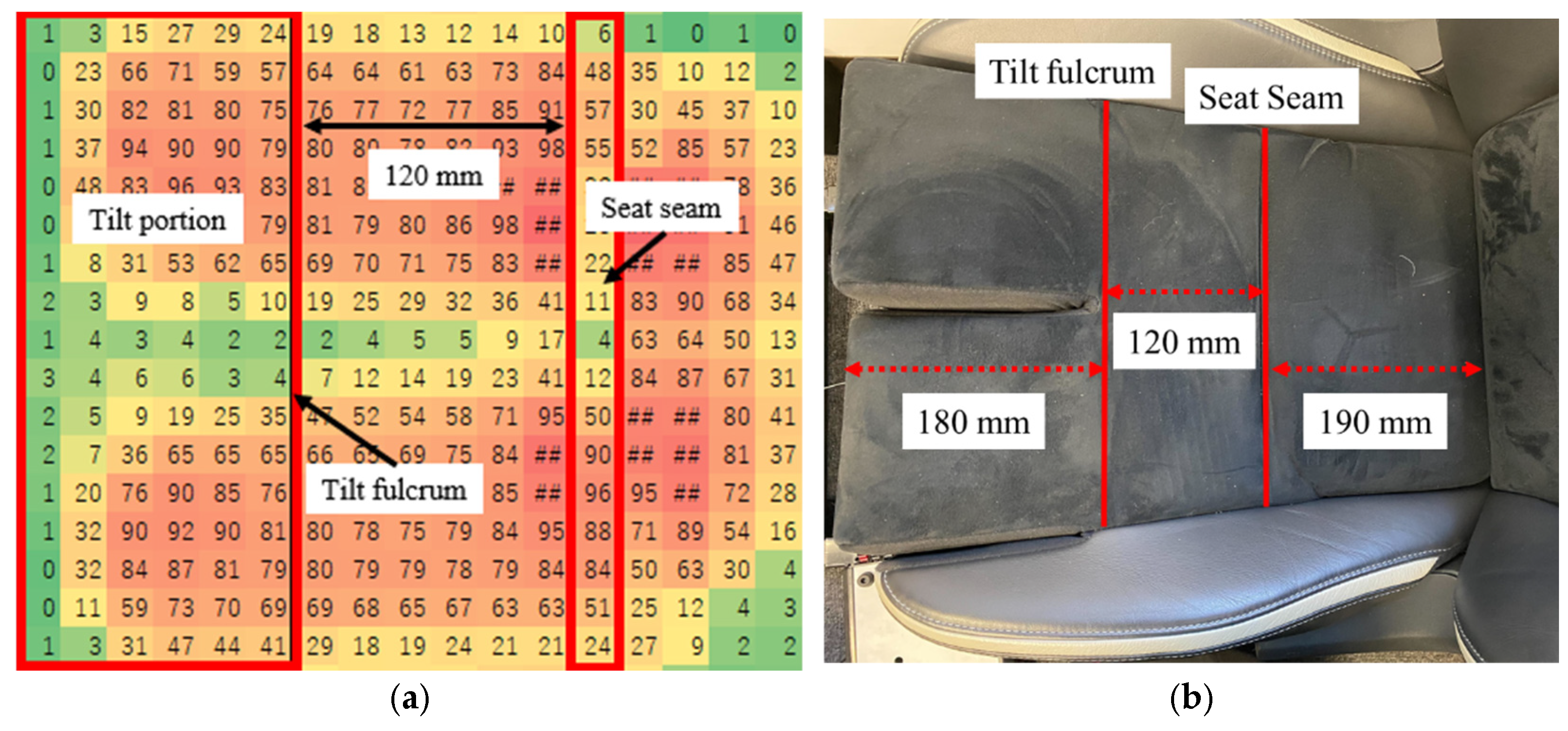
2.3. Measurement of Thigh Pressure Distribution
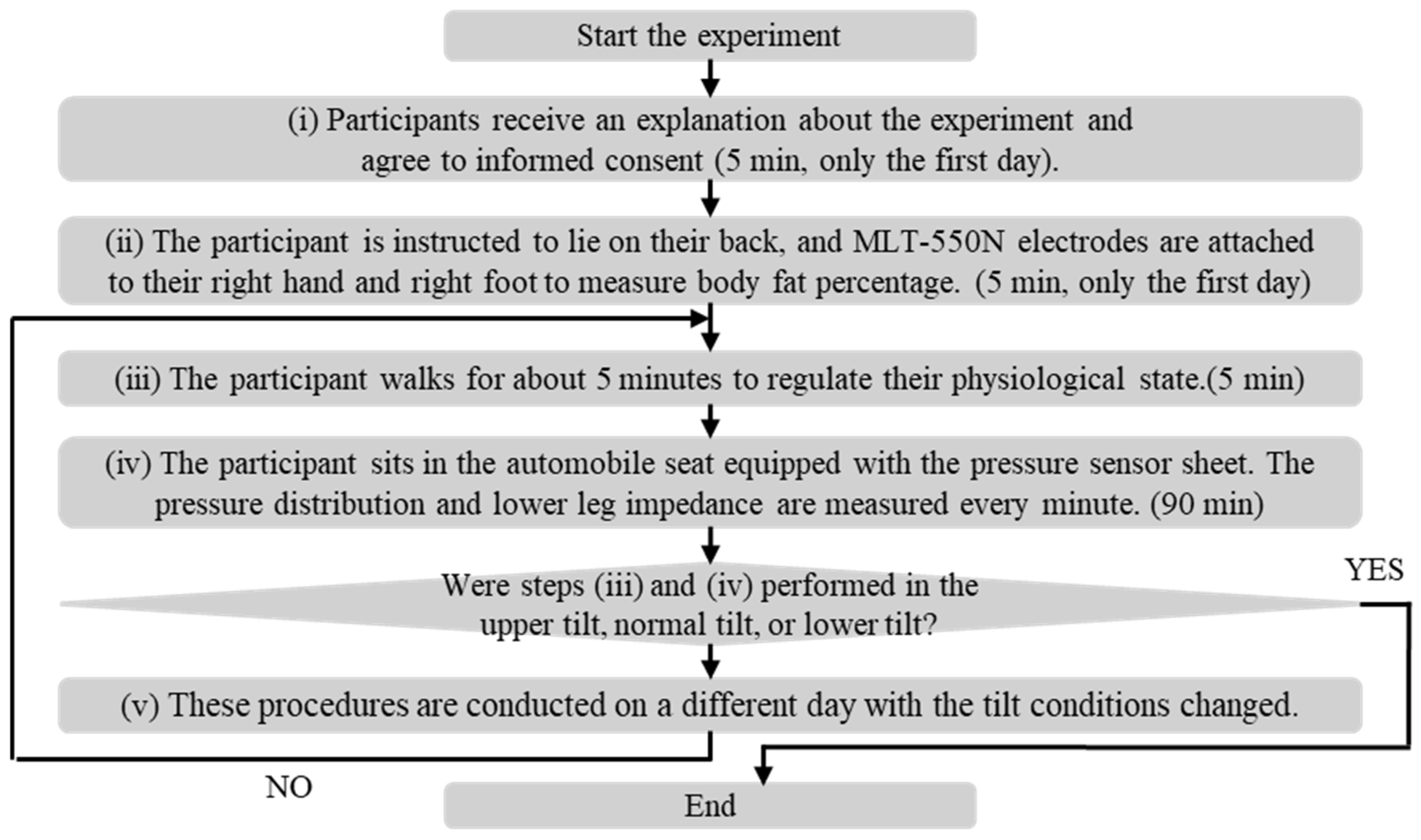
2.4. Measurement of Lower Leg Swelling and Thigh Pressure Distribution
3. Result and Discussion
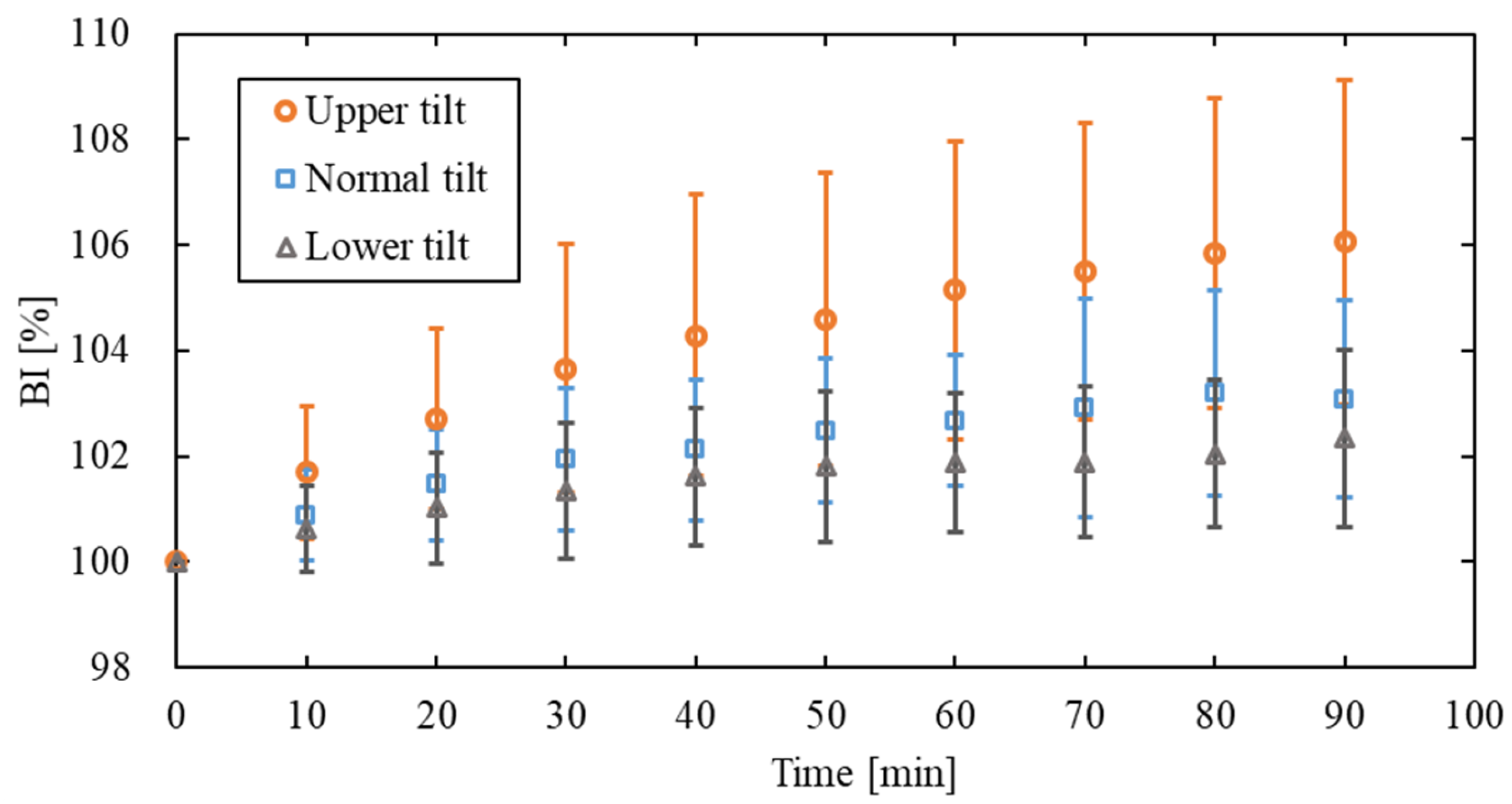
3.1. Relationship Between BI and Thigh Pressure Distribution
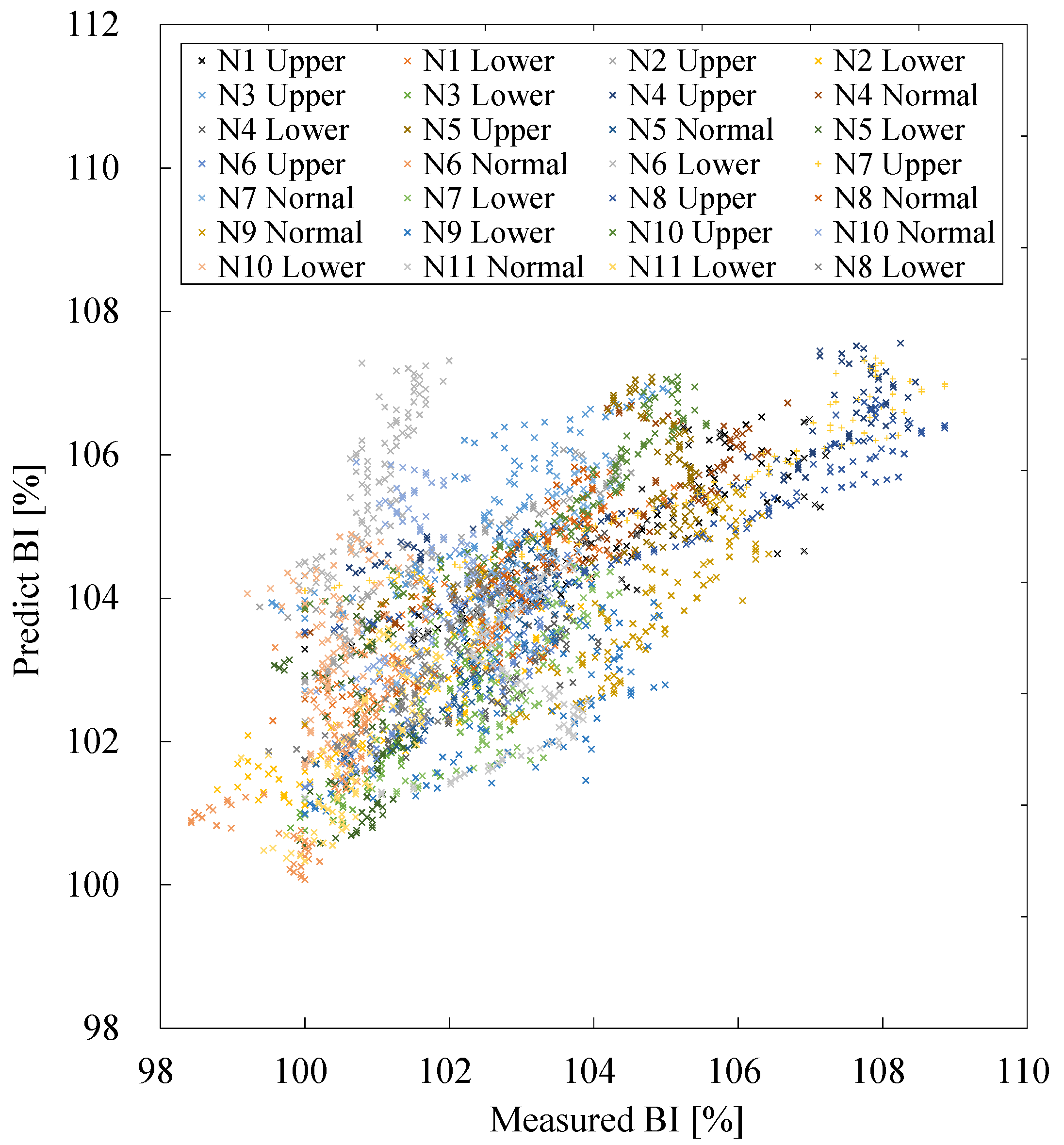
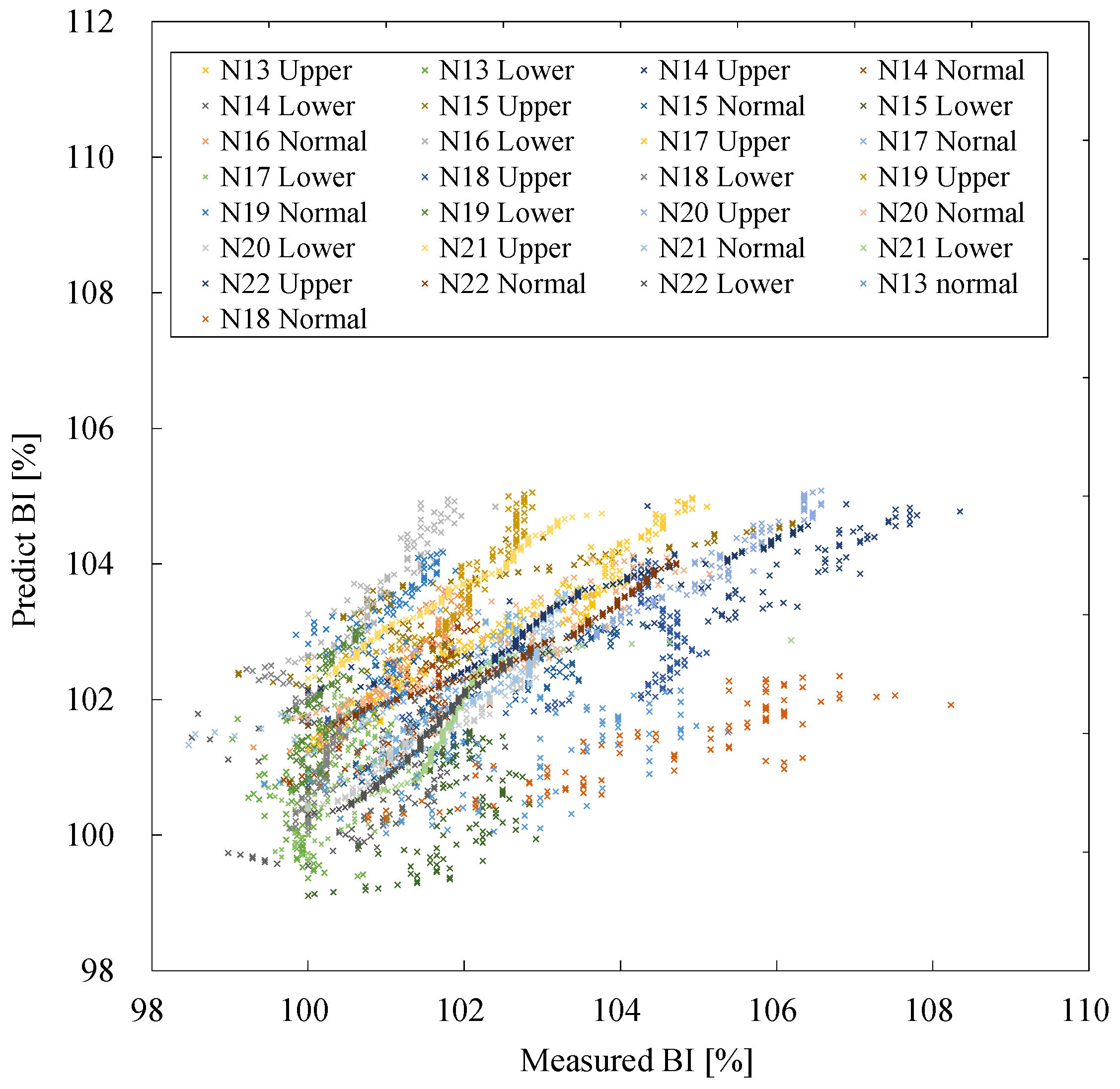
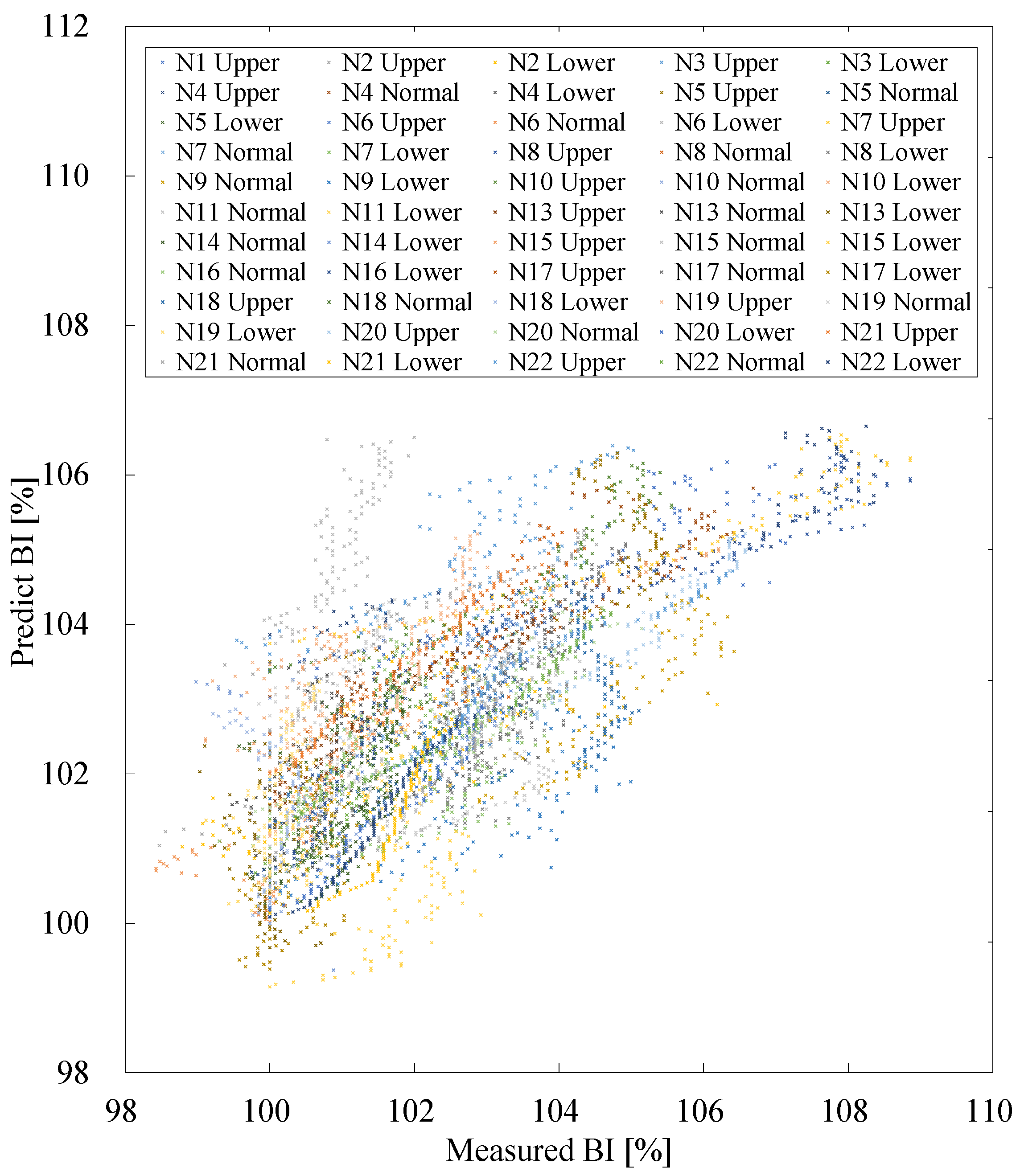
3.2. Construction of Prediction Equations for Lower Leg Swelling Relationship Between BI and Thigh Pressure Distribution
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Halin, A.; Verly, J.G.; Van Droogenbroeck, M. Survey and synthesis of state of the art in driver monitoring. Sensors 2021, 21, 5558. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Kim, H.; Kim, H.; Yang, W. A development of the self shape adjustment cushion mechanism for improving sitting comfort. Sensors 2021, 21, 7959. [Google Scholar] [CrossRef] [PubMed]
- De Looze, M.P.; Kuijt-Evers, L.F.; van Dieën, J. Sitting comfort and discomfort and the relationships with objective measures. Ergonomics 2003, 46, 985–997. [Google Scholar] [CrossRef] [PubMed]
- Kolich, M. Predicting automobile seat comfort using a neural network. Int. J. Ind. Ergon. 2004, 33, 285–293. [Google Scholar] [CrossRef]
- Orsini, F.; Giusti, G.; Zarantonello, L.; Costa, R.; Montagnese, S.; Rossi, R. Driving fatigue increases after the spring transition to daylight saving time in young male drivers: A pilot study. Transp. Res. Part F Traffic Psychol. Behav. 2023, 99, 83–97. [Google Scholar] [CrossRef]
- Schmidt, D.A.; Baran, E.; Thompson, A.D.; Mishra, P.; Koehler, M.J.; Shin, T.S. Technological pedagogical content knowledge (TPACK): The development and validation of an assessment instrument for preservice teachers. J. Res. Technol. Educ. 2009, 42, 123–149. [Google Scholar] [CrossRef]
- Hirao, A.; Matsuoka, Y.; Yamazaki, N. Biomechanical determinants of sitting posture. In Proceedings of the Second International Comfort Congress, Delft, The Netherlands, 29–30 August 2019; pp. 1–8. [Google Scholar]
- Al-Dirini, R.M.; Reed, M.P.; Thewlis, D. Deformation of the gluteal soft tissues during sitting. Clin. Biomech. 2015, 30, 662–668. [Google Scholar] [CrossRef]
- El Falou, W.; Duchêne, J.; Grabisch, M.; Hewson, D.; Langeron, Y.; Lino, F. Evaluation of driver discomfort during long-duration car driving. Appl. Ergon. 2003, 34, 249–255. [Google Scholar] [CrossRef]
- Behrens, M.; Mau-Moeller, A.; Bruhn, S. Effect of exercise-induced muscle damage on neuromuscular function of the quadriceps muscle. Int. J. Sports Med. 2012, 33, 600–606. [Google Scholar] [CrossRef]
- Stock, M.S.; Beck, T.W.; Defreitas, J.M. Effects of fatigue on motor unit firing rate versus recruitment threshold relationships. Muscle Nerve 2012, 45, 100–109. [Google Scholar] [CrossRef]
- Davidson, K.L.; Hubley-Kozey, C.L. Trunk muscle responses to demands of an exercise progression to improve dynamic spinal stability. Arch. Phys. Med. Rehabil. 2005, 86, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Levick, J.R.; Michel, C.C. Microvascular fluid exchange and the revised starling principle. Cardiovasc. Res. 2010, 87, 198–210. [Google Scholar] [CrossRef] [PubMed]
- Chester, M.R.; Rys, M.J.; Konz, S.A. Leg swelling, comfort and fatigue when sitting, standing, and sit/standing. Int. J. Ind. Ergon. 2002, 29, 289–296. [Google Scholar] [CrossRef]
- Hayes, S.; Cornish, B.; Newman, B. Comparison of methods to diagnose lymphoedema among breast cancer survivors: 6-month follow-up. Breast Cancer Res. Treat. 2005, 89, 221–226. [Google Scholar] [CrossRef]
- Lukaski, H.C. Methods for the assessment of human body composition: Traditional and new. Am. J. Clin. Nutr. 1987, 46, 537–556. [Google Scholar] [CrossRef]
- Fujita, D.; Mori, A.; Cleminson, T.; Kada, M.; Fukuda, J.; Kobara, K.; Osaka, H.; Watanabe, S. Using seating techniques as a preventative measure against lower limb edema -The effect of combining tilt angle and reclining mechanisms on wheelchairs. J. Phys. Ther. Sci. 2010, 22, 437–441. [Google Scholar] [CrossRef]
- Battini, D.; Berti, N.; Finco, S.; Guidolin, M.; Reggiani, M.; Tagliapietra, L. WEM-Platform: A Real-Time Platform for Full-Body Ergonomic Assessment and Feedback in Manufacturing and Logistics Systems. Comput. Ind. Eng. 2022, 164, 107881. [Google Scholar] [CrossRef]
- Jimenez, J.F.; Maire, J.L. ErgoTwin: A Digital Twin Model for Monitoring the Postural Risks on Industrial Workers. In Service Oriented, Holonic and Multi-Agent Manufacturing Systems for Industry of the Future. SOHOMA 2023; Borangiu, T., Trentesaux, D., Leitão, P., Berrah, L., Jimenez, J.F., Eds.; Studies in Computational Intelligence; Springer: Cham, Switzerland, 2024; Volume 1136, pp. 345–360. [Google Scholar] [CrossRef]
- Quan, Q.; Gao, Y.; Bai, Y.; Jin, Z. Multi-modal Fusion in Ergonomic Health: Bridging Visual and Pressure for Sitting Posture Detection. CCF Trans. Pervasive Comp. Interact. 2024. [Google Scholar] [CrossRef]
- Kapoor, R.; Jaiswal, A.; Makedon, F. Light-Weight Seated Posture Guidance System with Machine Learning and Computer Vision. In Proceedings of the 15th International Conference on Pervasive Technologies Related to Assistive Environments (PETRA ‘22), Corfu, Greece, 29 June–1 July 2022; Association for Computing Machinery: New York, NY, USA, 2022; pp. 595–600. [Google Scholar] [CrossRef]
- Lloyd, D.G.; Saxby, D.J.; Pizzolato, C.; Worsey, M.; Diamond, L.E.; Palipana, D.; Bourne, M.; de Sousa, A.C.; Mannan, M.M.N.; Nasseri, A.; et al. Maintaining Soldier Musculoskeletal Health Using Personalised Digital Humans, Wearables and/or Computer Vision. J. Sci. Med. Sport 2023, 26 (Suppl. S1), S30–S39. [Google Scholar] [CrossRef]
- Benjaminse, A.; Nijmeijer, E.M.; Gokeler, A.; Di Paolo, S. Application of Machine Learning Methods to Investigate Joint Load in Agility on the Football Field: Creating the Model, Part I. Sensors 2024, 24, 3652. [Google Scholar] [CrossRef]
- Deurenberg, P. International consensus conference on impedance in body composition. Age Nutr. 1994, 5, 142–145. [Google Scholar]
- Deurenberg, P.; Deurenberg-Yap, M.; Schouten, F.J. Validity of total and segmental impedance measurements for prediction of body composition across ethnic population groups. Eur. J. Clin. Nutr. 2002, 56, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Lukaski, H.C.; Johnson, P.E.; Bolonchuk, W.W.; Lykken, G.I. Assessment of fat-free mass using bioelectrical impedance measurements of the human body. Am. J. Clin. Nutr. 1985, 41, 810–817. [Google Scholar] [CrossRef]
- Nishimura, M.; Kato, T.; Onodera, S. Evaluation Methods for the Measurement of Lower Leg Edema in Healthy Young Adults. Yonago Acta Med. 2020, 63, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Hachiya, T.; Blaber, A.P.; Saito, M. Near-infrared spectroscopy provides an index of blood flow and vasoconstriction in calf skeletal muscle during lower body negative pressure. Acta Physiol. 2008, 193, 117–127. [Google Scholar] [CrossRef]
- Yamaguchi, H.; Yoshida, H.; Kamijo, M.; Fujimaki, G.; Naruse, T. Effect of footrest angle on decrement of leg swelling while sitting. Int. J. Affect. Eng. 2014, 13, 197–203. [Google Scholar] [CrossRef]
- Kato, Z.; Okubo, T. Syogakusya no Tame no Seitai Kinou no Hakarikata 2.0 [How to Measure Biological Functions for Beginning Students 2.0]; Nihon Syuppan Service: Tokyo, Japan, 2006. (In Japanese) [Google Scholar]
- Seo, A.; Kondo, Y.; Yoshinaca, F. A portable apparatus for monitoring leg swelling by bioelectrical impedance measurement. J. Occup. Health 1997, 39, 150–151. [Google Scholar] [CrossRef]
- Deurenberg, P.; Weststrate, J.A.; Paymans, I.; van der Kooy, K. Factors affecting bioelectrical impedance measurements in humans. Eur. J. Clin. Nutr. 1988, 42, 1017–1022. [Google Scholar]
- Clanton, T.O.; Solcher, B.W. Chronic leg pain in the athlete. Clin. Sports Med. 1994, 13, 743–759. [Google Scholar] [CrossRef]
- Miyoshi, S.; Hiroshige, Y.; Kamikubo, T.; Yamaguchi, E.; Yoshioka, T.; Shirakawa, T. Relationships between medial tibial stress syndrome and physical functions in long-distance runners. Rigakuryoho Kagaku 2020, 35, 355–359. [Google Scholar] [CrossRef]
- Newman, P.; Adams, R.; Waddington, G. Two simple clinical tests for predicting onset of medial tibial stress syndrome: Shin palpation test and shin oedema test. Br. J. Sports Med. 2012, 46, 861–864. [Google Scholar] [CrossRef] [PubMed]
- Kitamura, T.; Kato, T.; Sato, K.; Matsuoka, Y. Optimization of public seat functions to assure a comfortable sitting posture in diverse conditions. Glob. J. Res. Eng. 2013, 13, 9–17. [Google Scholar]
- Hitos, K.; Cannon, M.; Cannon, S.; Garth, S.; Fletcher, J.P. Effect of leg exercises on popliteal venous blood flow during prolonged immobility of seated subjects: Implications for prevention of travel-related deep vein thrombosis. J. Thromb. Haemost. 2007, 5, 1890–1895. [Google Scholar] [CrossRef]
- Stachenfeld, N.S.; Taylor, H.S. Effects of estrogen and progesterone administration on extracellular fluid. J. Appl. Physiol. 2004, 96, 1011–1018. [Google Scholar] [CrossRef]
- Stachenfeld, N.S.; Taylor, H.S. Progesterone increases plasma volume independent of estradiol. J. Appl. Physiol. 2005, 98, 1991–1997. [Google Scholar] [CrossRef]
- Murcia, N.; Mohafid, A.; Cardin, O. Non-intrusive musculoskeletal disorders risk assessment towards an integration in human operators’ digital twins. IFAC-PapersOnLine 2023, 56, 5667–5672. [Google Scholar] [CrossRef]
- Hirao, A.; Uchida, H.; Kato, T. Analysis of musculoskeletal loads during prolonged sitting in the desk work. In Advances in Digital Human Modeling. DHM 2023; Scataglini, S., Harih, G., Saeys, W., Truijen, S., Eds.; Lecture Notes in Networks and Systems; Springer: Cham, Switzerland, 2023; Volume 744. [Google Scholar] [CrossRef]
- Pizoń, J.; Gola, A. Human–Machine Relationship—Perspective and Future Roadmap for Industry 5.0 Solutions. Machines 2023, 11, 203. [Google Scholar] [CrossRef]
- Paul, G.; Wang, X.; Yang, J. An Introduction to the Special Issue on Digital Human Modeling (DHM) in Ergonomics 4.0. IISE Trans. Occup. Ergon. Hum. Factors 2021, 9, 107–110. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
|
Participant Number | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sex | Male | ||||||||||
| Height [mm] | 1820 | 1770 | 1760 | 1720 | 1730 | 1830 | 1720 | 1730 | 1700 | 1690 | 1770 |
| Weight [kg] | 63 | 63 | 63 | 65 | 58 | 58 | 61 | 69 | 55 | 62 | 62 |
| BMI [kg/m2] | 18.9 | 20.1 | 20.3 | 22.0 | 19.4 | 17.3 | 20.8 | 22.8 | 19.0 | 21.7 | 19.8 |
| Body fat [%] | 18.4 | 14.2 | 21.6 | 16.7 | 18.8 | 11.5 | 19.9 | 29.0 | 13.3 | 20.9 | 17.0 |
| Participant Number | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 |
| Sex | Female | ||||||||||
| Height [mm] | 1600 | 1670 | 1560 | 1610 | 1540 | 1520 | 1600 | 1550 | 1540 | 1520 | 1530 |
| Weight [kg] | 53 | 52 | 45 | 50 | 45 | 45 | 50 | 43 | 44 | 49 | 40 |
| BMI [kg/m2] | 20.7 | 18.6 | 18.5 | 19.3 | 19.0 | 19.5 | 19.5 | 17.9 | 18.6 | 21.2 | 17.1 |
| Body fat [%] | 27.6 | 12.7 | 20.2 | 16.8 | 15.3 | 12.9 | 17.1 | 18.8 | 17.6 | 17.9 | 11.6 |
| Data | Independent Variables | Non-Standardized Coefficient | Standardized Coefficient | Variance Inflation Factor |
|---|---|---|---|---|
| Male | 0.036 | 0.468 | 1.000 | |
| 0.002 | 0.552 | 1.130 | ||
| −8.373 | −0.184 | 1.203 | ||
| ) | −0.027 | −0.064 | 1.320 | |
| Constant | 111.415 | ― | ― | |
| Female | 0.027 | 0.439 | 1.000 | |
| 0.002 | 0.527 | 1.002 | ||
| −7.202 | −0.204 | 1.016 | ||
| ) | 0.010 | 0.017 | 1.018 | |
| Constant | 107.867 | ― | ― | |
| All | 0.031 | 0.439 | 1.000 | |
| 0.002 | 0.659 | 1.421 | ||
| −3.405 | −0.184 | 1.264 | ||
| ) | 0.001 | 0.002 | 1.150 | |
| Constant | 101.950 | ― |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kajitani, F.; Kato, T.; Hirao, A. Prediction of Lower Leg Swelling in Driving Posture. Appl. Sci. 2024, 14, 11788. https://doi.org/10.3390/app142411788
Kajitani F, Kato T, Hirao A. Prediction of Lower Leg Swelling in Driving Posture. Applied Sciences. 2024; 14(24):11788. https://doi.org/10.3390/app142411788
Chicago/Turabian StyleKajitani, Fuka, Takeo Kato, and Akinari Hirao. 2024. "Prediction of Lower Leg Swelling in Driving Posture" Applied Sciences 14, no. 24: 11788. https://doi.org/10.3390/app142411788
APA StyleKajitani, F., Kato, T., & Hirao, A. (2024). Prediction of Lower Leg Swelling in Driving Posture. Applied Sciences, 14(24), 11788. https://doi.org/10.3390/app142411788