Abstract
Background and Objectives: Trichomonas tenax is a protozoan which participates in the human oral microflora. It is considered as a potential paradontopathogen. This microorganism is also reported in the respiratory tract. We aimed to analyze the available literature about the prevalence of Trichomonas tenax in the population affected by periodontal disease. Materials and Methods: Searching the Scopus, PubMed, and ScienceDirect databases with the keywords: “Trichomonas tenax” and “periodontal diseases” was able to identify several systematic reviews and original articles up until July 2023. All studies with patients suffering from periodontal disease, which mentioned the year of publication, the country, specified the detection methods, and included the total number of tested samples as well as the percentage of those infected with Trichomonas tenax were included. Irrelevant articles were excluded. Results: We found 137 studies, but only 64 studies about the distribution of Trichomonas tenax in patients with gum disease underwent qualitative analysis. The highest number of studies have been conducted in Iran, Poland and Iraq. Different methods have been used to detect the unicellular organism, each with a different specificity and sensitivity. Conclusions: Interest in Trichomonas tenax has grown considerably since 2000. Because of its association with periodontal disease, Trichomonas tenax’s role in the inflammatory process should not be overlooked.
1. Introduction
It has been established that the oral cavity has a large number and a rich species composition of microorganisms forming its microflora [1]. Microorganisms adhere to various surfaces (the hard and soft tissues of the teeth, and the oropharyngeal mucosa) and form biofilms [2].
Trichomonas tenax is a flagellate, anaerobic unicellular microorganism that belongs to the genus Trichomonas, of the family Trichomonadidae. It is part of the oral microflora. Its name is derived from the Greek words “trichos” meaning “hair”, “monas” meaning “simple organism” and the Latin word “tenere” meaning “hold fast” [3]. Trichomonas tenax was identified by Müller in the second half of the 18th century in solutions of tartar [4]. It was initially named Cercaria tenax and underwent several modifications until the final name, Trichomonas tenax, was accepted by K. Dobel in 1939 [5,6]. Additionally, the human organism is inhabited by two more representatives of the Trichomonadidae family—Trichomonas vaginalis and Trichomonas hominis. Their characteristics are presented in Table 1. It can be seen that Trichomonas tenax looks more like Trichomonas vaginalis than Trichomonas hominis [7]. Trichomonas tenax inhabits the oral cavity of humans, with a higher incidence in individuals with poor oral hygiene, the presence of tartar and periodontal disease, which can lead to tooth loss in adults. It is typically found between teeth, in saliva, in periodontal pockets and less commonly in tonsillar crypts [6]. There is some evidence for its presence in the duct of the submandibular salivary gland [8]. This oral protozoan is transmitted via saliva, sneezing and coughing drops, kissing or using contaminated subjects and water [9]. Cases of non-oral localizations of Trichomonas tenax have been reported, including in sputum samples, bronchoalveolar lavage, pleural punctures in patients with diseases of the lower respiratory tract, the lungs and pleura during bronchiectasis and in lung abscesses, lung cancer and pyothorax. Pulmonary trichomoniasis is believed to develop after aspiration of the microorganism from the oropharynx into the airways [10,11]. The first case of Trichomonas tenax detection in the cerebrospinal fluid of patients with polymicrobial meningitis was reported in 1976 [12]. In 1987, its presence alongside a mixed oral bacterial microflora in pus from a subhepatic abscess following perforation of a gastric ulcer was reported [13]. In 1988, the protozoan was found in the mucus of the dilated ducts of patients with fibrocystic mastopathy [14]. Trichomonas tenax has been observed in an excised lymph node alongside the causative agent of tuberculosis, Mycobacterium tuberculosis [15]. Similar to Trichomonas vaginalis, Trichomonas tenax may also cause urogenital invasions [16]. Apart from humans, it has also been found in the oral cavities of domestic animals such as cats, dogs, horses, in the cloaca of birds and in the vaginas of monkeys [17,18].

Table 1.
Comparative table showing the characteristics of Trichomonas species occurring in humans.
Trichomonas tenax has been considered as a harmless commensal for a long time. Because of its association with periodontal disease, researchers have shifted their focus to its pathogenicity factors [19]. The secretory activity of Trichomonas tenax has been studied. Ribaux et al. reported the presence of fibronectin-like molecules on the surface of this flagellated microorganism in 1983. They examined two strains of Trichomonas tenax—one isolated from patients with ulcerative gingivitis and another maintained in culture for two years. Both strains exhibited positive fluorescence with anti-fibronectin antibodies. These fibronectin-like molecules are believed to facilitate adhesion to gingival cells and connective tissue and promote phagocytosis of the bacteria [20]. Bózner and Demeš continued the studies on proteolytic activity in cell extracts and culture filtrates of Trichomonas tenax using SDS-polyacrylamide gels, identifying seven different proteolytic bands. Among them, three are SH-dependent, with molecular weights in the range of 35–36 kDa, exhibiting inhibitory sensitivity characteristic of cysteine proteinases. The remaining four bands are SH-independent, with higher molecular weights (76–270 kDa), and their inhibition sensitivity suggests that they are metalloproteinases. Bózner and Demeš then investigated the degradation of collagens I, III, IV and V by secreted extracellular proteinases from Trichomonas tenax, concluding that degradation was temperature-dependent and that type IV collagen was the most efficiently degraded. These proteinases may play a role in periodontal degradation [21]. Trichomonas tenax can produce hemolysins that destroy human, equine, and ovine erythrocytes. Two different types of hemolysins were identified. The first is protein-like, thermolabile and may be inhibited by cysteine proteinase inhibitors. The other is lipid-like, thermostable, not inhibited by proteinase inhibitors and resistant to the action of organic solvents. These hemolysins may serve as potential virulence factors [22]. Ribeiro et al. performed a study that revealed that Trichomonas tenax damages mammalian cells in vitro and behaves similarly to Trichomonas vaginalis. It phagocytoses portions of the mammalian cells, and also induces apoptosis in HeLa cells, suggesting that it behaves as a parasite [23]. In 2018, it was discovered that Trichomonas tenax lysates induce IL-8 synthesis by macrophages [19]. According to a study conducted in 2023, the protozoan exhibits toxicity to gingival cells, disrupts cell contacts, and leads to the synthesis of another inflammatory mediator (IL-6) by gingival and alveolar cells [24].
The objective of this article is to analyze the available studies on the prevalence of Trichomonas tenax in the population affected by periodontal disease.
2. Materials and Methods
2.1. Search Strategy
Several reviews and original articles in the Scopus, PubMed and ScienceDirect databases were examined. The articles had a publication period up to July 2023. We used the “Advanced search” extension and the following keywords: “Trichomonas tenax” and “periodontal diseases”. Only full texts were included.
2.2. Inclusion and Exclusion Criteria
All studies involving individuals diagnosed with periodontal disease, with or without concomitant systemic disorders, were included. There were no geographical restrictions on selection. Other inclusion criteria included considering articles that contained information about the year of publication, country, reported detection methods, total number of samples tested, and the percentage of patients infected with the flagellate microorganism.
Duplicate articles from all three databases were excluded. In addition, articles were excluded if they were not relevant to the aims of the study, such as those involving animal studies or analyzing Trichomonas tenax in a site other than the oral cavity.
2.3. Statistical Analyses
For the statistical analyses and visual presentation of resumed studies, MS Excel 2016 software was used.
3. Results
3.1. Study Selection
We found 137 records from the Scopus, PubMed, and ScienceDirect databases that were potentially relevant. The study selection process followed the PRISMA flow diagram (Figure 1). Initially, duplicates were removed, leaving 102 articles for screening. Seventeen were excluded due to general irrelevancy based on either title or abstract, and nine were excluded due to the lack of a full text. Of the remaining seventy-six articles, twelve were further removed for various reasons, including the detection of Trichomonas tenax in animals, extraoral detection of Trichomonas tenax, and in vitro studies. Ultimately, sixty-four research papers underwent qualitative analysis.
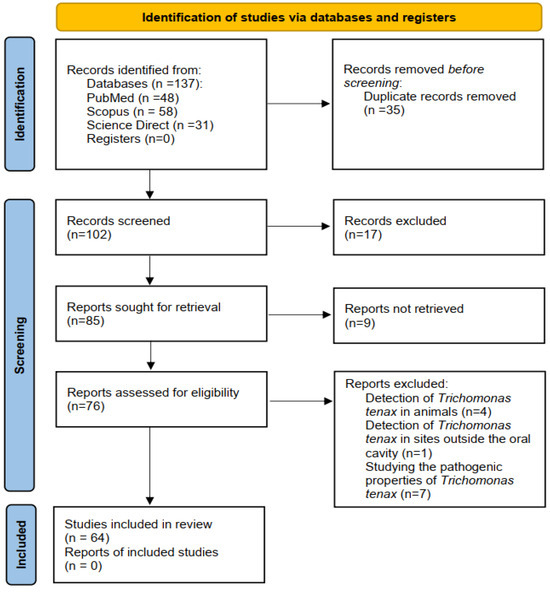
Figure 1.
PRISMA flow diagram of the study selection process.
3.2. Demonstration of Our Results
For a better demonstration of the results, tables and figures were used. We divided the Trichomonas tenax prevalence studies in patients with gum disease by continent and country. Figure 2 illustrates the distribution by continents. We were able to find the following numbers of studies:
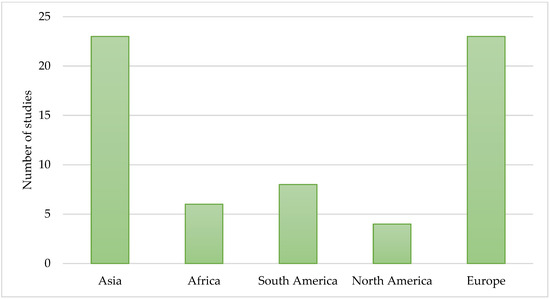
Figure 2.
Number of studies available about the prevalence of Trichomonas tenax—distribution by continents. We were able to identify the fewest studies of Trichomonas tenax prevalence in North America, and the most in Asia and Europe.
- Twenty-three studies carried out in Europe.
- Twenty-three studies carried out in Asia.
- Six studies carried out in Africa.
- Eight studies carried out in South America.
- Four studies carried out in North America.
Figure 3 shows the distribution by countries. Table 2 presents the total number of samples taken, whose number was 12,269, of which 2215 were infected with Trichomonas tenax. Table 3, Table 4, Table 5, Table 6 and Table 7 provide a detailed description of the studies, taking into account author, year of publication, country, number of samples tested, number of positive samples and detection method used. The detection methods used in the studies are those that were used to evaluate the presence of Trichomonas tenax in patients with gum disease. Their advantages and disadvantages, as well as the factors that may influence the spread of this microorganism, are mentioned in the Discussion section.
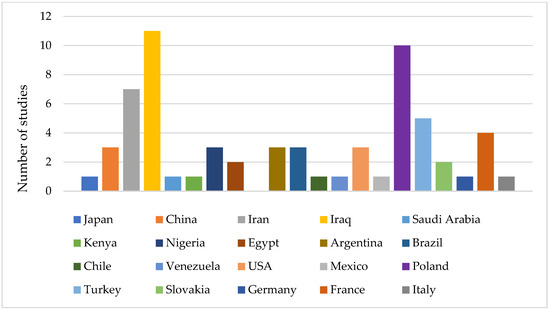
Figure 3.
Number of studies available about the prevalence of Trichomonas tenax—distribution by countries. We found the fewest studies of Trichomonas tenax prevalence in Japan, Saudi Arabia, Kenya, Chile, Venezuela, Mexico, Italy, Germany and the most in Iraq, Poland and Iran.
Table 2.
Percentage of samples infected with Trichomonas tenax.
Table 3.
Trichomonas tenax prevalence studies carried out in Europe.
Table 4.
Trichomonas tenax prevalence studies carried out in Asia.
Table 5.
Trichomonas tenax prevalence studies carried out in South America.
Table 6.
Trichomonas tenax prevalence studies carried out in North America.
Table 7.
Trichomonas tenax prevalence studies carried out in Africa.
A relatively large number of studies have been conducted in Europe, with the majority carried out in Poland. In nine of these cases, light microscopy was used as a confirmatory method. Biochemical methods were also present in one of them, and PCR was present in two of them. Five studies were carried out in the European part of Turkey, all using light microscopy and one using cultivation. In France, interest in the protozoan began in 1979, leading to four studies, two of which used PCR as a confirmatory method. Trichomonas tenax was identified by cultivation in Germany and Slovakia, and by light microscopy in Italy. We mentioned the advantages and disadvantages of each detection method in the Discussion section.
In Asia, the majority of studies were found in Iraq. In five of them, Trichomonas tenax was identified by light microscopy. One of the studies used cultivation. Notably, half of the studies used molecular techniques for detection. In Iran, seven studies were found, half of which also employed molecular techniques. In China, two studies used light microscopy and one utilized an unknown method. In Japan and Saudi Arabia, microscopy and cultivation were used. In North America, South America and Africa the number of studies was lower compared to Asia and Europe. Light microscopy and cultivation were the main diagnostic methods used in the studies conducted in the USA and Mexico. In South America, we were able to find eight studies, with PCR being used in only one study. Most studies in Africa detected the unicellular microorganism by light microscopy or cultivation, with PCR being used in only one of them. In Australia, there was only one study that detected protozoan, but in canine samples.
4. Discussion
The relevance of the topic is supported by the fact that periodontal disease is a global societal problem, prevalent mainly in developed and developing countries, affecting both children and adults [85]. The literature emphasizes the importance of its etiology. Our review aims to enrich the knowledge that exists about the etiology of periodontal disease, since, in addition to bacteria, protozoa such as Trichomonas tenax can also be involved in the inflammatory process. After analyzing the results, we have drawn some important conclusions about the prevalence of Trichomonas tenax and identified the factors associated with its distribution, which will be the focus of the discussion.
Regarding the prevalence of Trichomonas tenax in the oral cavity, our analysis revealed that it has been detected in samples of various biological material: most commonly in dental calculus or subgingival dental plaque, and less commonly in saliva, mouthwash or gingival crevicular fluid [71]. In one study, it was found in material from decayed dental cavities, suggesting that it may be associated with caries development [60].
Most articles do not provide information about the distribution of Trichomonas tenax by sex. However, some authors reported a higher incidence of this protist in men than women [27,29,77]. In addition, it has been found more in adults. Based on the systematic review of Eslahi et al., individuals aged 46–55 years showed the highest colonization by oral trichomonads [27]. Several articles highlight the presence of the single-celled microorganism in the pediatric population [29,30,78]. According to Vráblic et al. oral protozoa occur in older children. Trichomonas tenax invasion was found to be higher in children with Down syndrome and periodontitis than in healthy children in a study by Mehr et al. [54].
Oral trichomoniasis is more commonly associated with gingivitis and periodontitis. Trichomonas tenax was found more in patients with periodontitis than with plaque-induced gingivitis [74]. It is important to emphasize that most scientists have examined Trichomonas tenax alongside Entamoeba gingivalis, another protozoan that is part of the oral microflora. Entamoeba gingivalis is typically found in the early stages of periodontitis and Trichomonas tenax is associated with the progression of periodontitis [42,64,71,75,76]. The presence of Trichomonas tenax is usually less common than that of Entamoeba gingivalis in patients with gingivitis [27]. Associations of the flagellated protozoan with respiratory diseases have also been reported [10,11].
The prevalence of periodontal disease depends on various factors including the level of socioeconomic status, sanitary conditions (areas with bad hygiene may have higher risks of contamination and an increased spread of microorganisms), certain lifestyle factors (such as smoking, diet rich in sugary or acidic foods), health education, access to dental care, the population’s immunological status and the presence of metabolic diseases such as diabetes [86]. A proportional relationship between the frequency of occurrence of Trichomonas tenax and poor oral hygiene, alcohol consumption and tobacco use has been reported by some authors [34,37,53]. Changes in oral ecology due to diabetes or reduced body resistance (HIV infection, treatment with immunosuppressants after organ transplantation) facilitate the reproduction of flagellate protozoa and the colonization of dental tissues [33,69]. Patients with masticatory system disorders, particularly those with congenital diseases, may also favor the presence of oral dysbiosis [39]. A study by Ponce de Leon et al. showed that the incidence of buccal parasites in patients with dental prostheses was greater [68]. Trichomonas tenax has also been found in peri-implantitis lesions [43].
From our analysis, it became evident that in some countries there is a notably high number of studies on the epidemiology of Trichomonas tenax. This is probably due to greater research interest in countries or regions where oral health problems, infectious and parasitic diseases are more prevalent. Previous research contributes to our understanding of why Trichomonas tenax is tested for more in Poland, Iran and Iraq. According to the study conducted by Muhammad Nazir et al., more than half of the adult populations in Poland and Iran suffer from periodontal disease. Additionally, Iran also has a high proportion of adolescents affected by it [87]. Factors such as low education, use of tobacco products and metabolic disorders can be considered as risk in Iran that lead to periodontitis and tooth loss in Iran. [88] Derikvand et al. found a significant association between parasite invasion and compromised oral hygiene in Iran [59]. An online-based survey in Iraq revealed low levels of awareness about oral health and periodontitis [89]. A similar study conducted in Poland showed an insufficient knowledge about risk factors as well as the prophylaxis of periodontal disease [90]. Unlike Iran and Iraq, Poland has another demographic characteristic: a high proportion of the population is ageing, which plays a significant role in the increased incidence of dental diseases. Declining immunity in older individuals predisposes them to the development of oral and systemic pathology [70].
Additionally, we will discuss an issue that is critical to the positivity of the samples, namely the methods of detection. It is important to note that not all methods exhibit the same sensitivity and specificity. The limitations of the methods must be considered together with other factors, such as a limited number of samples, a small number of participants, and a lack of standardized protocols, which may account for the differences in the obtained results. Different methodologies have been used over the years to find Trichomonas tenax. The detection methods were unspecified in two studies and biochemical methods were used in one. We observed that many scientists have identified Trichomonas tenax through microscopic examination, with or without pre-staining, by visualizing pear-shaped or elliptical cells with several flagella [91]. Microscopic examination was the primary detection method in forty studies, with thirty-nine using light microscopy and one employing phase-contrast microscopy. The advantage of microscopy is the easy and quick visualization of trichomonads. Cultivation allows for the isolation and identification of Trichomonas tenax. We were able to find fourteen reports that detect the unicellular organism through cultivation in an axenic culture medium known as Diamond’s medium, which was established in the second half of the 20th century [92]. However, we acknowledge the limitations of both of these methods, namely limited specificity and low sensitivity. Cultivation is also time-consuming. There is a high probability that the results may not be completely accurate in studies that have used these two methods because of their shortcomings. Furthermore, it is possible that the samples may have been contaminated with Trichomonas hominis or Trichomonas vaginalis, whose morphologies are particularly similar, as discussed in Table 1, causing false-positive results. As discussed earlier, most studies have examined Trichomonas tenax and Entamoeba gingivalis together. Diagnosis may be complicated by the tendency of Trichomonas tenax to form amoeba-like forms that may be overlooked by light microscopy [81]. These forms are visually similar to those of Entamoeba gingivalis and may lead to the misinterpretation of results. It should be noted that in some studies light microscopy and cultivation are complemented by Polymerase chain reaction (PCR), which increases diagnostic accuracy and reliability. PCR can detect the DNA of microorganisms even at very low concentrations, which is difficult or impossible with light microscopy. Molecular techniques are the only method used in some studies. These techniques have a high sensitivity and specificity and can be used for strain discrimination. The high sensitivity of PCR is highlighted in some studies, where it was able to detect the nucleic acid of the protozoan in samples that had previously been found to be negative by light microscopy [48,81]. The shortcomings of molecular techniques include the need for advanced laboratory skills and specialized equipment, as well as the possibility of contamination and false-positive results. We established that PCR was used in 15 studies. Some of the Trichomonas tenax genes, such as the beta-tubulin gene, 18S rRNA gene, rpb1 gene, have been analyzed by PCR [42,74,93]. Loop-mediated isothermal amplification (LAMP) is a relatively new method that requires a shorter run time and is more sensitive than PCR [94,95]. There was only one study in which LAMP was employed to detect Trichomonas tenax, but this used canine oral samples and the specific detection of ITS (internal transcribed spacers) and the 5.8S rRNA gene [96]. We observed that gaps currently exist in immunological diagnosis. Advances in diagnostic techniques and tools may contribute to increasing the number of epidemiological studies on Trichomonas tenax.
Despite these findings, there is still insufficient information regarding the distribution of Trichomonas tenax and there is a need for future research on its prevalence. Conducting more epidemiological studies could prove to be useful in understanding its prevalence as well as the social disparities among affected populations. Furthermore, future research may focus on the pathogenesis and impact of this microorganism on oral health, its genetics and biology and its relationship with other microorganisms in the oral cavity. The development of more sensitive and specific methods for the diagnosis of Trichomonas tenax may facilitate a more accurate determination of its presence in the human mouth. Improved methods could help not only in the diagnosis of existing disease, but also in the screening of people with dental calculus. Because of its advantages, we may recommend the LAMP method as an efficient screening method in the future. Another critical area for potential future research is exploring the influence of the immune system on Trichomonas tenax and the potential development of immunological diagnostic methods. We may propose Trichomonas tenax to be a candidate for inclusion in the mandatory diagnostic panel for periodontitis. Its elimination will improve the prognosis of gum disease in these patients. In this context, studies on drug resistance and the impact of different toothpastes may be important. The involvement of Trichomonas tenax in the etiopathogenesis of dental caries requires further research.
5. Conclusions
Interest in Trichomonas tenax has significantly increased since 2000. Numerous studies have identified it in oral specimens from patients with periodontal disease, most commonly tartar or dental plaque, using a variety of methods. Studies have shown that there is a proportional relationship between its prevalence and poor personal hygiene and some behavioral factors. It occurs in older children and more frequently in adults with periodontitis than gingivitis. It may be a marker associated with the severity of periodontal disease. We found the largest number of studies detecting Trichomonas tenax in patients with gum disease in Iran, Iraq and Poland, where oral health problems are common. Consequently, Trichomonas tenax’s role in the inflammatory process should not be overlooked, and therefore, this single-celled microorganism should be discussed in the diagnosis and treatment of patients with periodontal disease. Its eradication from the oral cavity can mitigate the risk of aspiration into the lungs and subsequent complications. For future research, it would be beneficial for researchers to focus on the epidemiology, the mechanisms of dental tissue damage and the immunological diagnosis, treatment and prevention of Trichomonas tenax.
Author Contributions
Writing—original draft, methodology, review and editing S.S. and T.D.; writing— supervision, conceptualization, review and editing O.T. and G.Y. All authors have read and agreed to the published version of the manuscript.
Funding
The European Union-Next Generation EU, through the National Recovery and Resilience Plan of the Republic of Bulgaria, project No. BG-RRP-2.004-0009-C02, supported this work.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Willis, J.R.; Gabaldón, T. The human oral microbiome in health and disease: From sequences to ecosystems. Microorganisms 2020, 8, 308. [Google Scholar] [CrossRef]
- Zaura, E.; Nicu, E.A.; Krom, B.P.; Keijser, B.J.F. Acquiring and maintaining a normal oral microbiome: Current perspective. Front. Cell. Infect. Microbiol. 2014, 4, 85. [Google Scholar] [CrossRef]
- Mehlhorn, H. Human Parasites: Diagnosis, Treatment, Prevention; Springer: New York, NY, USA, 2016. [Google Scholar]
- Hamadto, H.H.A.; El Hayawan, I.A.H.; Abdallah, K.F.; Abd El-Maboud, A.I.; Mohammed, O.I.; Omar, G.H.E. Relation between Trichomonas tenax and pulmonary diseases. Egypt J. Med. Sci. 2014, 35, 633–652. [Google Scholar]
- Dobell, C. The common flagellate of the human mouth, Trichomonas tenax (O.F.M.): Its discovery and its nomenclature. Parasitology 1939, 31, 138–146. [Google Scholar] [CrossRef]
- Honigberg, B.M.; Lee, J.J. Structure and division of Trichomonas tenax (O. F. Müller). Am. J. Epidemiol. 1959, 69, 177–201. [Google Scholar] [CrossRef]
- Wenrich, D.H. Comparative morphology of the trichomonad flagellates of man. Am. J. Trop. Med. Hyg. 1944, 24, 39–51. [Google Scholar] [CrossRef]
- Duboucher, C.; Mogenet, M.; Périé, G. Salivary trichomoniasis. A case report of infestation of a submaxillary gland by Trichomonas tenax. Arch. Pathol. Lab. Med. 1995, 119, 277–279. [Google Scholar]
- Mallat, H.; Podglajen, I.; Lavarde, V.; Mainardi, J.L.; Frappier, J.; Cornet, M. Molecular characterization of Trichomonas tenax causing pulmonary infection. J. Clin. Microbiol. 2004, 42, 3886–3887. [Google Scholar] [CrossRef]
- Hersh, S.M. Pulmonary trichomoniasis and Trichomonas tenax. J. Med. Microbiol. 1985, 20, 1–10. [Google Scholar] [CrossRef]
- Wu, Y.; Ye, Y.; Yang, Y.; Yang, W.; Lin, J.; Cao, K. Pyopneumothorax from coinfection by Trichomonas tenax and Geotrichum capitatum in a child from China: A case report. BMC Infect. Dis. 2021, 21, 842. [Google Scholar] [CrossRef]
- Masur, H.; Hook, E.; Armstrong, D. A Trichomonas species in a mixed microbial meningitis. JAMA 1976, 236, 1978–1979. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, E.B.; Friis-Møller, A.; Friis, J. Trichomonas species in a subhepatic abscess. Eur. J. Clin. Microbiol. 1987, 6, 296–297. [Google Scholar] [CrossRef] [PubMed]
- Krvavac, S. Trichomoniasis of the breast diseased by fibrocystic mastopathy: Pathogenic rather than saprophytic relationship (Trichomonas in fibrocystic mastopathy process). Med. Arh. 1998, 52, 143–145. [Google Scholar] [PubMed]
- Duboucher, C.; Farto-Bensasson, F.; Chéron, M.; Peltier, J.Y.; Beaufils, F.; Périé, G. Lymph node infection by Trichomonas tenax: Report of a case with co-infection by Mycobacterium tuberculosis. Hum. Pathol. 2000, 31, 1317–1321. [Google Scholar] [CrossRef] [PubMed]
- Brosh-Nissimov, T.; Hindiyeh, M.; Azar, R.; Smollan, G.; Belausov, N.; Mandelboim, M.; Rahav, G.; Keller, N.; Gefen-Halevi, S. A false-positive Trichomonas vaginalis result due to Trichomonas tenax presence in clinical specimens may reveal a possible T. tenax urogenital infection. Clin. Microbiol. Infect. 2019, 25, 123–124. [Google Scholar] [CrossRef] [PubMed]
- Kellerová, P.; Tachezy, J. Zoonotic Trichomonas tenax and a new trichomonad species, Trichomonas brixi n. sp., from the oral cavities of dogs and cats. Int. J. Parasitol. 2017, 47, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Hegner, R.; Ratcliffe, H. Trichomonads from the Vagina of the Monkey, from the Mouth of the Cat and Man, and from the Intestine of the Monkey, Opossum and Prairie-Dog. J. Parasitol. 1927, 14, 27. [Google Scholar] [CrossRef]
- Bisson, C.; Dridi, S.M.; Machouart, M. Assessment of the role of Trichomonas tenax in the etiopathogenesis of human periodontitis: A systematic review. PLoS ONE 2019, 14, e0226266. [Google Scholar] [CrossRef]
- Ribaux, C.L.; Magloire, H.; Joffre, A.; Morrier, J.J. Immunohistochemical localization of fibronectin-like protein on the cell surface of the oral flagelatte Trichomonas tenax. J. Biol. Buccale 1983, 11, 41–51. [Google Scholar]
- Bózner, P.; Demeš, P. Cell-associated and extracellular proteolytic activity of an oral flagellate, Trichomonas tenax. Arch. Oral Biol. 1991, 36, 77–83. [Google Scholar] [CrossRef]
- Nagao, E.; Yamamoto, A.; Igarashi, T.; Goto, N.; Sasa, R. Two distinct hemolysins in Trichomonas tenax ATCC 30207. Oral Microbiol. Immunol. 2000, 15, 355–359. [Google Scholar] [CrossRef]
- Ribeiro, L.C.; Santos, C.; Benchimol, M. Is Trichomonas tenax a parasite or a commensal? Protist 2015, 166, 196–210. [Google Scholar] [CrossRef]
- Hong, Z.B.; Lai, Y.T.; Chen, C.H.; Chen, Y.J.; Chen, C.C.; Lin, W.C. Trichomonas tenax induces barrier defects and modulates the inflammatory cytotoxicity of gingival and pulmonary epithelial cells. Parasite 2023, 30, 7. [Google Scholar] [CrossRef]
- Feki, A.; Molet, B.; Haag, R.; Kremer, M. Protozoa of the human oral cavity (Epidemiological correlations and pathogenic possibilities. J. Biol. Buccale 1981, 9, 155–161. [Google Scholar] [PubMed]
- Ferrara, A.; Conca, R.; Grassi, L.; de Carneri, I. [Possible pathogenic role of Trichomonas tenax in chronic periodontitis]. Ann. Ist Super. Sanita 1986, 22, 253–255. [Google Scholar]
- Eslahi, A.V.; Olfatifar, M.; Abdoli, A.; Houshmand, E.; Johkool, M.G.; Zarabadipour, M.; Abadi, P.A.; Ghorbani, A.; Mirzadeh, M.; Badri, M. The neglected role of Trichomonas tenax in oral diseases: A systematic review and meta-analysis. Acta Parasitol. 2021, 66, 715–732. [Google Scholar] [CrossRef] [PubMed]
- Kurnatowska, A.; Kurnatowska, A. Difficulties in the diagnosis of Trichomonas infection complicated by mycosis of the oral cavity. Wiad. Parazytol. 1990, 36, 237–243. [Google Scholar]
- Vráblic, J.; Tomová, S.; Catár, G.; Randová, L.; Suttová, S. Morphology and diagnosis of Entamoeba gingivalis and Trichomonas tenax and their occurrence in children and adolescents. Bratisl. Lek. Listy 1991, 92, 241–246. [Google Scholar]
- Vráblic, J.; Tomová, S.; Catár, G. Occurrence of the protozoa, Entamoeba gingivalis and Trichomonas tenax in the mouths of children and adolescents with hyperplastic gingivitis caused by phenytoin. Bratisl. Lek. Listy 1992, 93, 136–140. [Google Scholar]
- Kurnatowska, A.J.; Kurnatowski, P. Trichomonosis of the oral cavity complicated by mycosis. Parassitologia 1998, 40, 339–342. [Google Scholar]
- Pardi, G.; Perrone, M.; de Ilja, M.; Incidencia, R. De Trichomonas Tenax en pacientes con periodontitis marginal crónica. Acta Odontol. Venez. 2002, 40, 152–159. [Google Scholar]
- Piekarczyk, J.; Fiedor, P.; Chomicz, L.; Szubinska, D.; Starościak, B.; Piekarczyk, B.; Zawadzki, P.; Zebrowska, J.; Dudziński, T. Oral cavity as a potential source of infections in recipients with diabetes mellitus. Transplant. Proc. 2003, 35, 2207–2208. [Google Scholar] [CrossRef] [PubMed]
- Kurnatowska, A.J.; Dudko, A.; Kurnatowski, P. Invasion of Trichomonas tenax in patients with periodontal diseases. Wiad. Parazytol. 2004, 50, 397–403. [Google Scholar] [PubMed]
- Turkowicz, M.; Tomaszewska, D.; Cielecka, D. Molecular Diagnosis of oral cavity Trichomonas infections in HIV Patients. Wiad. Parazytol. 2004, 50, 181–186. [Google Scholar] [PubMed]
- Abualqomsaan, M.; Töz, S.O.; Yolasiğmaz, A.; Turgay, N. The investigation of Entamoeba gingivalis and Trichomonas tenax in a group of patients with periodontal disease. Turkiye Parazitol. Derg. 2010, 34, 91–94. [Google Scholar] [PubMed]
- Gedik, R.; Özçelik, S.; Malatyali, E.; Gedik, T. Ağız ve Diş Sağlığı Île Entamoeba Gingivalis ve Trichomonas Tenax varlığı arasındaki ilişkinin araştırılması. Turkiye Parazitol. Derg. 2010, 34, 155–159. [Google Scholar]
- Yazar, S.; Çetinkaya, Ü.; Hamamcı, B.; Alkan, A.; Şişman, Y.; Esen, Ç.; Kolay, M. Investigation of Entamoeba gingivalis and Trichomonas tenax in periodontitis or gingivitis patients in kayseri. Turkiye Parazitol. Derg. 2016, 40, 17–21. [Google Scholar] [CrossRef]
- Zawadzki, P.J.; Perkowski, K.; Starościak, B.; Dybicz, M.; Baltaza, W.; Pionkowski, K.; Chomicz, L. Evaluation of selected oral cavity microbiota—Risk factors of management complications in patients with masticatory system disorders. Ann. Parasitol. 2016, 62, 71–76. [Google Scholar] [CrossRef]
- Zawadzki, P.J.; Perkowski, K.; Padzik, M.; Mierzwińska-Nastalska, E.; Szaflik, J.P.; Conn, D.B.; Chomicz, L. Examination of oral microbiota diversity in adults and older adults as an approach to prevent spread of risk factors for human infections. BioMed Res. Int. 2017, 2017, 8106491. [Google Scholar] [CrossRef]
- Dubar, M.; Zaffino, M.L.; Remen, T.; Thilly, N.; Cunat, L.; Machouart, M.C.; Bisson, C. Protozoans in subgingival biofilm: Clinical and bacterial associated factors and impact of scaling and root planing treatment. J. Oral Microbiol. 2020, 12, 1693222. [Google Scholar] [CrossRef]
- Benabdelkader, S.; Andreani, J.; Gillet, A.; Terrer, E.; Pignoly, M.; Chaudet, H.; Aboudharam, G.; La Scola, B. Specific clones of Trichomonas tenax are associated with periodontitis. PLoS ONE 2019, 14, e0213338. [Google Scholar] [CrossRef]
- Arpag, O.F.; Kaya, O.M. Presence of Trichomonas tenax and Entamoeba gingivalis in peri-implantitis lesions. Quintessence Int. 2020, 51, 212–218. [Google Scholar] [CrossRef]
- Sato, M.; Hayashi, A.; Kato, M.; Nitta, H.; Namikawa, I.; Shiraki, M.; Katsutani, Y.; Iwayama, S.; Hirata, K.; Kimura, K. Occurrence of oral trichomonads (Trichomonas tenax) in subgingival plaque materials. Nihon Shishubyo Gakkai Kaishi 1985, 27, 407–415. [Google Scholar] [CrossRef][Green Version]
- Li, Z. A survey of Entamoeba gingivalis and Trichomonas buccalis in Xian. Zhonghua Kou Qiang Yi Xue Za Zhi 1988, 23, 307–309. [Google Scholar] [PubMed]
- Mahdi, N.K.; Al-Saeed, A.T. Trichomonas tenax in Basrah, Iraq. J. Pak. Med. Assoc. 1993, 43, 261–262. [Google Scholar] [PubMed]
- Xiufeng, G.; Qionglian, L.; Qiya, F. The survey and analysis of 427 persons with infestation of Entamoeba gingivalis and Trichomonas buccalis in Haikou City. J. Hainan Med. Coll. 2003, 9, 90–92. [Google Scholar]
- Athari, A.; Soghandi, L.; Haghighi, A.; Kazemi, B. Prevalence of oral trichomoniasis in patients with periodontitis and gingivitis using pcr and direct smear. Iran. J. Public Health 2007, 36, 33–37. [Google Scholar]
- Kadir, M.; Al-Mashhadani, A.; Dim, S.T.; Chapook, G.O. Prevalence of Trichomonas tenax and Entamoeba gingivalis among patients attending dental clinics in Kirkuk City. J. Tech. 2007, 20, 36–40. [Google Scholar]
- Zhihua, Z. Investigation on the infection of Trichomonas tenax. J. Shanxi Med. Coll. Contin. Educ. 2009, 144, 1417–1425. [Google Scholar]
- Ghabanchi, J.; Zibaei, M.; Afkar, M.D.; Sarbazie, A.H. Prevalence of oral Entamoeba gingivalis and Trichomonas tenax in patients with periodontal disease and healthy population in Shiraz, Southern Iran. Indian J. Dent. Res. 2010, 21, 89–91. [Google Scholar] [CrossRef]
- Ibrahim, S.; Abbas, R. Evaluation of Entamoeba gingivalis and Trichomonas tenax in patients with periodontitis and gingivitis and its correlation with some risk factors. J. Baghdad Coll. Dent. 2012, 24, 158–162. [Google Scholar]
- Shahab Hamad, S.; Huseein Mohammad, S.; Kader, M.A. Relationship between the dental health and prevalence’s Trichomonas tenax and Entamoeba gingivalis among patients attending dental clinics in Kirkuk. J. Univ. Babylon 2012, 20, 1441–1447. [Google Scholar]
- Mehr, A.K.; Zarandi, A.; Anush, K. Prevalence of oral Trichomonas tenax in periodontal lesions of Down syndrome in Tabriz, Iran. J. Clin. Diagn. Res. 2015, 9, ZC88–ZC90. [Google Scholar] [CrossRef]
- Jabuk, S.I.; Rafla’a, S.H.; Hussien, Z.M.A.; Najam, H.M.; Naji, N.M. Isolation and identification of bacteria and parasite from teeth caries and periodontal. Adv. Environ. Biol. 2015, 9, 50–53. [Google Scholar]
- Al-Khayat, F.A.A.-M. The Prevalence of oral protozoa Trichomonas tenax in some patients with gingivitis. J. Baghdad Coll. Dent. 2016, 28, 179–182. [Google Scholar] [CrossRef]
- Khafari Ghosheh, M.; Khalili, B.; Kheri, S.; Shataghi, A.; Heidari Sorshjani, S. With gingivitis and periodontitis referring Resalat Dental clinic, Chaleshtor in 2015. Armaghane Danesh 2017, 22, 220–229. [Google Scholar]
- Ismail, K.A.; Jastaniyyah, M.A.; Al-Nemari, N.A.; Al-Ghamdi, H.M.; Al-Hamed, R.A. Detection of Trichomonas tenax (T. tenax) in bad oral hygiene Saudi patients in Taif City. Int. Educ. Appl. Sci. Res. J. 2017, 2, 4–6. [Google Scholar]
- Derikv, N.; Mahmoudv, H.; Sepahv, A.; Baharv, P.; Kiafar, M.M.; Chiniforush, N.; Ghasemi, S.S. Frequency and associated risk factors of Entamoeba gingivalis and Trichomonas tenax among patients with periodontitis in Western Iran. J. Res. Med. Dent. Sci. 2018, 6, 99–103. [Google Scholar]
- Mahmoudvand, H.; Sepahvand, A.; Niazi, M.; Momeninejad, N.; Sepahvand, S.M.; Behzadian, M. Prevalence and risk factors of oral cavity protozoa (Entamoeba gingivalis and Trichomonas tenax) among patients with dental cavity caries. J. Res. Med. Dent. Sci. 2018, 6, 42–46. [Google Scholar]
- Abdulhaleem, S.H.; Sulbi, I.M.; Almammuri, A.H. Study the distribution of oral Trichomonas Tenax at Almukadissa City/IRAQ. Indian J. Public Health Res. Dev. 2018, 9, 951–954. [Google Scholar] [CrossRef]
- Jaffer, N.; Al-Noori, A.; Salih, A.; Zuhdi, S. Molecular detection of oral Trichomonas tenax among individuals attending dental care units using PCR in Duhok City–Kurdistan region. J. Duhok Univ. 2019, 22, 195–202. [Google Scholar] [CrossRef]
- Hassan, F.; Al-Dulaimi, A.; Abed, A.; Alajeely, A.; Ail, Y.M. Incidence of Entamoeba gingivalis and Trichomonas tenax in periodontitis and gingivitis patients who attended to private clinics in Babylon Province. Med.-Leg. Update 2020, 20, 906–910. [Google Scholar] [CrossRef]
- Yaseen, A.; Mahafzah, A.; Dababseh, D.; Taim, D.; Hamdan, A.A.; Al-Fraihat, E.; Hassona, Y.; ¸Sahin, G.Ö.; Santi-Rocca, J.; Sallam, M. Oral colonization by Entamoeba gingivalis and Trichomonas tenax: A PCR-based study in health, gingivitis, and periodontitis. Front. Cell. Infect. Microbiol. 2021, 11, 782805. [Google Scholar] [CrossRef]
- Sharifi, M.; Jahanimoghadam, F.; Babaei, Z.; Mohammadi, M.A.; Sharifi, F.; Hatami, N.; Danesh, M.; Poureslami, P.; Poureslami, H. Prevalence and associated-factors for Entamoeba gingivalis in adolescents in Southeastern Iran by culture and PCR, 2017. Iran. J. Public Health 2020, 49, 351–359. [Google Scholar] [CrossRef]
- Hala Nadhim, K.; Nadham Kadham, M. Incidence of Tricomonas Tenax in diseased mouth. Int. J. Oral Dent. Health 2023, 7, 198–200. [Google Scholar] [CrossRef]
- Zdero, M.; Ponce de León, P.; Vasconi, M.D.; Nocito, I.; Lucca, A. Entamoeba gingivalis y Trichomonas tenax: Hallazgo en poblaciones humanas con y sin patología bucal. Acta Bioquim. Clin. Latinoam. 1999, 33, 359–365. [Google Scholar]
- Ponce De León, P.; Zdero, M.; Vasconi, M.D.; Nocito, I.; Lucca, A.; Perez, B. Relation between buccal protozoa and pH and salivary IgA in patients with dental prosthesis. Rev. Inst. Med. Trop. Sao Paulo 2001, 43, 241–242. [Google Scholar] [CrossRef] [PubMed]
- Nocito Mendoza, I.; Vasconi Correas, M.D.; Ponce de León Horianski, P.; Zdero Pandzich, M. Entamoeba gingivalis y Trichomonas tenax en pacientes diabéticos. Rev. Cuba. Ortod. Odontopediatr. 2003, 8, 13–23. [Google Scholar]
- Mabel, E.; Osorio, A.; Maldonado Ibáñez, A.B.; Maldonado Ibáñez, C.; María, A.; Mora, B.; Parra, J.; Urdaneta, Y.; Urdaneta, M. Entamoeba gingivalis and Trichomonas tenax in the oral cavity of patients from the Integral Adult Clinic of the faculty of Odontology, Maracaibo, Venezuela. Rev. Soc. Venez. Microbiol. 2009, 29, 122–127. [Google Scholar]
- Albuquerque Júnior, R.L.C.; de Melo, C.M.; de Santana, W.A.; Ribeiro, J.L.; Silva, F.A. Incidence of Entamoeba gingivalis and Trichomonas tenax in samples of dental biofilm and saliva from patients with periodontal disease. RGO Rev. Gaúcha Odontol. 2011, 59, 35–40. [Google Scholar]
- Bernaola-Paredes, E.; Guillén-Oneeglio, A.; Gutiérrez-Romero, F. Aislamiento de Trichomonas tenax en pacientes con periodontitis crónica al medio de cultivo de tioglicolato modificado. Kiru 2012, 9, 95–106. [Google Scholar]
- Norberg, C.M.B.M. Entamoeba Gingivalis (Gros, 1849) and Trichomonas Tenax (Muller, 1773) oral infections in patients from Baixada Fluminense, Province of Rio de Janeiro, Brazil. Sci. J. Public Health 2014, 2, 288–292. [Google Scholar] [CrossRef]
- Bracamonte-Wolf, C.; Orrego, P.R.; Muñoz, C.; Herrera, D.; Bravo, J.; Gonzalez, J.; Varela, H.; Catalán, A.; Araya, J.E. Observational cross-sectional study of Trichomonas tenax in patients with periodontal disease attending a Chilean university dental clinic. BMC Oral Health 2019, 19, 207. [Google Scholar] [CrossRef]
- Hinshaw, H.C. Correlation of protozoan infections of human mouth with extent of certain lesions in pyorrhea alveolaris. Exp. Biol. Med. 1926, 24, 71–73. [Google Scholar] [CrossRef]
- Beatman, L.H. Studies on Trichomonas buccalis. J. Dent. Res. 1933, 13, 339–347. [Google Scholar] [CrossRef]
- Wantland, W.W.; Lauer, D. Correlation of some oral hygiene variables with age, sex, and incidence of oral protozoa. J. Dent. Res. 1970, 49, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Cuevas, R.F.; de la Barquera Ramos, M.A.S.; Contreras, C.C.; Hernández-Sierra, F. Prevalencia y asociación epidemiológica de los protozoarios orales Entamoeba Gingivalis y Trichomonas Tenax en niños mexicanos. Revista ADM 2008, 65, 259–262. [Google Scholar]
- Chunge, R.N.; Manji, F.; Amwayi, P. Oral protozoa in a Kenyan population. East Afr. Med. J. 1988, 65, 203–207. [Google Scholar] [PubMed]
- Ozumba, U.; Ozumba, N.; Ndiokwelu, E. Oral protozoa in a Nigeria population. Afr. J. Clin. Exp. Microbiol. 2004, 5, 15–19. [Google Scholar] [CrossRef]
- El-Sayed, N.M.; Meabed, E.M.H. Detection of Trichomonas tenax in patients with periodontitis using microscopy and culture compared to PCR. Egypt. J. Med. Sci. 2008, 29, 537–550. [Google Scholar]
- Onyido, A.E.; Amadi, E.S.; Olofin, I.; Onwumma, A.A.; Okoh, I.C.; Chikwendu, C.I. Prevalence of Entamoeba gingivalis and Trichomonas tenax among dental patients attending Federal School of Dental Technology and Therapy clinic, Enugu, Nigeria. Nat. Sci. 2011, 9, 59–62. [Google Scholar]
- El Sibaei, M.M.; Abdel-Fattah, N.S.; Ahmed, S.A.; Abou-Seri, H.M. Growth kinetics, antigen profiling, and proteinase activity of Egyptian Trichomonas tenax isolates derived from patients having oral infections. Exp. Parasitol. 2012, 130, 416–422. [Google Scholar] [CrossRef]
- Christiana Ani, O.; Agbo, E.E.; Nnamonu, E.I.; Onyeidu, S.O.; Onyeidu, B.U.; Okwerekwu, N.J. Rising profile of oral cavity protozoa amongst dental patients in South Eastern Nigeria. Int. J. Health Life Sci. 2020, 6, 34–42. [Google Scholar] [CrossRef]
- Nazir, M.A. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int. J. Health Sci. 2017, 11, 72–80. [Google Scholar]
- Kanmaz, M.; Kanmaz, B.; Buduneli, N. Periodontal treatment outcomes in smokers: A narrative review. Tob. Induced Dis. 2021, 19, 77. [Google Scholar] [CrossRef] [PubMed]
- Nazir, M.; Al-Ansari, A.; Al-Khalifa, K.; Alhareky, M.; Gaffar, B.; Almas, K. Global prevalence of periodontal disease and lack of its surveillance. Sci. World J. 2020, 2020, 2146160. [Google Scholar] [CrossRef] [PubMed]
- Khazaei, S.; H Keshteli, A.; Feizi, A.; Savabi, O.; Adibi, P. Epidemiology and risk factors of tooth loss among Iranian adults: Findings from a large community-based study. BioMed Res. Int. 2013, 2013, 786462. [Google Scholar] [CrossRef]
- Abdulbaqi, H.R.; Abdulkareem, A.A.; Alshami, M.L.; Milward, M.R. The oral health and periodontal diseases awareness and knowledge in the Iraqi population: Online-based survey. Clin. Exp. Dent. Res. 2020, 6, 519–528. [Google Scholar] [CrossRef]
- Dolińska, E.; Milewski, R.; Pietruska, M.J.; Gumińska, K.; Prysak, N.; Tarasewicz, T.; Janica, M.; Pietruska, M. Periodontitis-related knowledge and its relationship with oral health behavior among adult patients seeking professional periodontal care. J. Clin. Med. 2022, 11, 1517. [Google Scholar] [CrossRef]
- Matthew, M.A.; Yang, N.; Ketzis, J.; Mukaratirwa, S.; Yao, C. Trichomonas tenax: A neglected protozoan infection in the oral cavities of humans and dogs—A scoping review. Trop. Med. Infect. Dis. 2023, 8, 60. [Google Scholar] [CrossRef]
- Diamond, L.S.; Bartgis, I.L. Axenic cultivation of Trichomonas tenax, the oral flagellate of man I. Establishment of cultures. J. Protozool. 1962, 9, 442–444. [Google Scholar] [CrossRef] [PubMed]
- Kikuta, N.; Yamamoto, A.; Fukura, K.; Goto, N. Specific and sensitive detection of Trichomonas tenax by the polymerase chain reaction. Lett. Appl. Microbiol. 1997, 24, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Garg, N.; Ahmad, F.J.; Kar, S. Recent advances in loop-mediated isothermal amplification (LAMP) for rapid and efficient detection of pathogens. Curr. Res. Microb. Sci. 2022, 3, 100120. [Google Scholar] [CrossRef] [PubMed]
- Lenkowski, M.; Nijakowski, K.; Kaczmarek, M.; Surdacka, A. The loop-mediated isothermal amplification technique in periodontal diagnostics: A systematic review. J. Clin. Med. 2021, 10, 1189. [Google Scholar] [CrossRef]
- Matthew, M.A.; Christie, J.; Yang, N.; Yao, C. A loop-mediated isothermal amplification (LAMP) assay specific to Trichomonas tenax is suitable for use at point-of-care. Microorganisms 2022, 10, 594. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).