
Impact of Single-Session Intraoral and Extraoral Photobiomodulation on Pain Control after Extraction of Impacted Mandibular Third Molar: A Pilot Study

 ,
,  ,
,  ,
,  ,
,  ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Surgical Intervention
2.2. PBM Parameters
2.3. Follow-Up Assessment
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grossi, G.B.; Maiorana, C.; Garramone, R.A.; Borgonovo, A.; Creminelli, L.; Santoro, F. Assessing postoperative discomfort after third molar surgery: A prospective study. J. Oral Maxillofac. Surg. 2007, 65, 901–917. [Google Scholar] [CrossRef]
- Singh, A.; Pentapati, K.C.; Kodali, M.V.R.M.; Smriti, K.; Patil, V.; Chowdhary, G.L.; Gadicherla, S. Efficacy of Preemptive Dexamethasone versus Methylprednisolone in the Management of Postoperative Discomfort and Pain after Mandibular Third Molar Surgery: A Systematic Review and Meta-Analysis. Sci. World J. 2023, 2023, 7412026. [Google Scholar] [CrossRef]
- Gerbershagen, H.J.; Aduckathil, S.; van Wijck, A.J.; Peelen, L.M.; Kalkman, C.J.; Meissner, W. Pain intensity on the first day after surgery: A prospective cohort study comparing 179 surgical procedures. Anesthesiology 2013, 118, 934–944. [Google Scholar] [CrossRef]
- Merry, A.F.; Gibbs, R.D.; Edwards, J.; Ting, G.S.; Frampton, C.; Davies, E.; Anderson, B.J. Combined acetaminophen and ibuprofen for pain relief after oral surgery in adults: A randomized controlled trial. Br. J. Anaesth. 2010, 104, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Chopra, D.; Rehan, H.S.; Mehra, P.; Kakkar, A.K. A randomized, double-blind, placebo-controlled study comparing the efficacy and safety of paracetamol, serratiopeptidase, ibuprofen and betamethasone using the dental impaction pain model. Int. J. Oral Maxillofac. Surg. 2009, 38, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Maihemaiti, M.; Ainiwaer, A.; Wang, L. A clinical study of the piezosurgery, high-speed contra-angle handpiece, and the combined application of both for extraction of embedded supernumerary teeth. BMC Oral Health 2023, 23, 147. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, I.A.; Armond, A.C.V.; Falci, S.G.M. The Effectiveness of the Cold Therapy (cryotherapy) in the Management of Inflammatory Parameters after Removal of Mandibular Third Molars: A Meta-Analysis. Int. Arch. Otorhinolaryngol. 2019, 23, 221–228. [Google Scholar] [CrossRef]
- Mocan, A.; Kişnişci, R.; Uçok, C. Stereophotogrammetric and clinical evaluation of morbidity after removal of lower third molars by two different surgical techniques. J. Oral Maxillofac. Surg. 1996, 54, 171–175. [Google Scholar] [CrossRef]
- Rodrigues, É.D.R.; Martins-de-Barros, A.V.; Loureiro, A.M.L.C.; Carvalho, M.V.; Vasconcelos, B. Comparison of two suture techniques on the inflammatory signs after third molars extraction-A randomized clinical trial. PLoS ONE 2023, 18, e0286413. [Google Scholar] [CrossRef]
- Tanan Karaca, G.; Duygu, G.; Er, N.; Ozgun, E. Comparative Investigation of Anti-Inflammatory Effect of Platelet-Rich Fibrin after Mandibular Wisdom Tooth Surgery: A Randomized Controlled Study. J. Clin. Med. 2023, 12, 4250. [Google Scholar] [CrossRef]
- Momeni, E.; Kazemi, F.; Sanaei-Rad, P. Extraoral low-level laser therapy can decrease pain but not edema and trismus after surgical extraction of impacted mandibular third molars: A randomized, placebo-controlled clinical trial. BMC Oral Health 2022, 22, 417. [Google Scholar] [CrossRef] [PubMed]
- Mester, E.; Mester, A.F.; Mester, A. The biomedical effects of laser application. Lasers Surg. Med. 1985, 5, 31–39. [Google Scholar] [CrossRef]
- Mohsen, A.; Tenore, G.; Rocchetti, F.; Del Vecchio, A.; Ricci, R.; Barberi, W.; Cartoni, C.; Iori, A.P.; Pippi, R.; Polimeni, A.; et al. Photo-Biomodulation as a Prevention Modality of Oral Mucositis in Patients Undergoing Allogeneic Hematopoietic Stem Cell Transplantation. Appl. Sci. 2020, 10, 7479. [Google Scholar] [CrossRef]
- Del Vecchio, A.; Tenore, G.; Luzi, M.C.; Palaia, G.; Mohsen, A.; Pergolini, D.; Romeo, U. Laser Photobiomodulation (PBM)-A Possible New Frontier for the Treatment of Oral Cancer: A Review of In Vitro and In Vivo Studies. Healthcare 2021, 9, 134. [Google Scholar] [CrossRef] [PubMed]
- Del Vecchio, A.; Palaia, G.; Grassotti, B.; Tenore, G.; Ciolfi, C.; Podda, G.; Impellizzeri, A.; Mohsen, A.; Galluccio, G.; Romeo, U. Effects of laser photobiomodulation in the management of oral lichen planus: A literature review. Clin. Ter. 2021, 172, 467–483. [Google Scholar] [CrossRef] [PubMed]
- Tenore, G.; Zimbalatti, A.; Rocchetti, F.; Graniero, F.; Gaglioti, D.; Mohsen, A.; Caputo, M.; Lollobrigida, M.; Lamazza, L.; De Biase, A.; et al. Management of Medication-Related Osteonecrosis of the Jaw (MRONJ) Using Leukocyte- and Platelet-Rich Fibrin (L-PRF) and Photobiomodulation: A Retrospective Study. J. Clin. Med. 2020, 9, 3505. [Google Scholar] [CrossRef] [PubMed]
- Del Vecchio, A.; Floravanti, M.; Boccassini, A.; Gaimari, G.; Vestri, A.; Di Paolo, C.; Romeo, U. Evaluation of the efficacy of a new low-level laser therapy home protocol in the treatment of temporomandibular joint disorder-related pain: A randomized, double-blind, placebo-controlled clinical trial. Cranio 2021, 39, 141–150. [Google Scholar] [CrossRef]
- Sampaio-Filho, H.; Bussadori, S.K.; Gonçalves, M.L.L.; da Silva, D.F.T.; Borsatto, M.C.; Tortamano, I.P.; Longo, P.L.; Pavani, C.; Fernandes, K.P.S.; Mesquita-Ferrari, R.A.; et al. Low-level laser treatment applied at auriculotherapy points to reduce postoperative pain in third molar surgery: A randomized, controlled, single-blinded study. PLoS ONE 2018, 13, e0197989. [Google Scholar] [CrossRef] [PubMed]
- Kahraman, S.A.; Cetiner, S.; Strauss, R.A. The Effects of Transcutaneous and Intraoral Low-Level Laser Therapy After Extraction of Lower Third Molars: A Randomized Single Blind, Placebo Controlled Dual-Center Study. Photomed. Laser Surg. 2017, 35, 401–407. [Google Scholar] [CrossRef]
- Brignardello-Petersen, R.; Carrasco-Labra, A.; Araya, I.; Yanine, N.; Beyene, J.; Shah, P.S. Is adjuvant laser therapy effective for preventing pain, swelling, and trismus after surgical removal of impacted mandibular third molars? A systematic review and meta-analysis. J. Oral Maxillofac. Surg. 2012, 70, 1789–1801. [Google Scholar] [CrossRef]
- Dawdy, J.; Halladay, J.; Carrasco-Labra, A.; Araya, I.; Yanine, N.; Brignardello-Petersen, R. Efficacy of adjuvant laser therapy in reducing postsurgical complications after the removal of impacted mandibular third molars: A systematic review update and meta-analysis. J. Am. Dent. Assoc. 2017, 148, 887–902.e4. [Google Scholar] [CrossRef] [PubMed]
- Domah, F.; Shah, R.; Nurmatov, U.B.; Tagiyeva, N. The Use of Low-Level Laser Therapy to Reduce Postoperative Morbidity After Third Molar Surgery: A Systematic Review and Meta-Analysis. J. Oral Maxillofac. Surg. 2021, 79, e1–e313. [Google Scholar] [CrossRef] [PubMed]
- Duarte de Oliveira, F.J.; Brasil, G.M.L.C.; Araújo Soares, G.P.; Fernandes Paiva, D.F.; de Assis de Souza Júnior, F. Use of low-level laser therapy to reduce postoperative pain, edema, and trismus following third molar surgery: A systematic review and meta-analysis. J. Craniomaxillofac Surg. 2021, 49, 1088–1096. [Google Scholar] [CrossRef] [PubMed]
- Lacerda-Santos, J.T.; Granja, G.L.; Firmino, R.T.; Dias, R.F.; de Melo, D.P.; Granville-Garcia, A.F.; Martins, C.C. Use of Photobiomodulation to Reduce Postoperative Pain, Edema, and Trismus After Third Molar Surgery: A Systematic Review and Meta-Analysis. J. Oral Maxillofac. Surg. 2023, 81, 1135–1145. [Google Scholar] [CrossRef]
- Pell, G.J. Impacted mandibular third molars: Classification and modified techniques for removal. Dent. Digest 1933, 39, 330–338. [Google Scholar]
- Hamblin, M.R. How to Write a Good Photobiomodulation Article. Photobiomodul. Photomed. Laser Surg. 2019, 37, 325–326. [Google Scholar] [CrossRef] [PubMed]
- Majid, O.W. Submucosal dexamethasone injection improves quality of life measures after third molar surgery: A comparative study. J. Oral Maxillofac. Surg. 2011, 69, 2289–2297. [Google Scholar] [CrossRef] [PubMed]
- Savin, J.; Ogden, G.R. Third molar surgery--a preliminary report on aspects affecting quality of life in the early postoperative period. Br. J. Oral Maxillofac. Surg. 1997, 35, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.; Garg, A.; Bhagol, A.; Savarna, S.; Agarwal, S.K. Photobiomodulation Alleviates Postoperative Discomfort After Mandibular Third Molar Surgery. J. Oral Maxillofac. Surg. 2019, 77, 2412–2421. [Google Scholar] [CrossRef]
- Bjordal, J.M.; Johnson, M.I.; Iversen, V.; Aimbire, F.; Lopes-Martins, R.A. Low-level laser therapy in acute pain: A systematic review of possible mechanisms of action and clinical effects in randomized placebo-controlled trials. Photomed. Laser Surg. 2006, 24, 158–168. [Google Scholar] [CrossRef]
- Ferreira, B.; da Motta Silveira, F.M.; de Orange, F.A. Low-level laser therapy prevents severe oral mucositis in patients submitted to hematopoietic stem cell transplantation: A randomized clinical trial. Support. Care Cancer 2016, 24, 1035–1042. [Google Scholar] [CrossRef] [PubMed]
- Farhadi, F.; Eslami, H.; Majidi, A.; Fakhrzadeh, V.; Ghanizadeh, M.; KhademNeghad, S. Evaluation of adjunctive effect of low-level laser Therapy on pain, swelling and trismus after surgical removal of impacted lower third molar: A double blind randomized clinical trial. Laser Ther. 2017, 26, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Hagiwara, S.; Iwasaka, H.; Okuda, K.; Noguchi, T. GaAlAs (830 nm) low-level laser enhances peripheral endogenous opioid analgesia in rats. Lasers Surg. Med. 2007, 39, 797–802. [Google Scholar] [CrossRef] [PubMed]
- Karu, T.I.; Afanas’Eva, N.I. Cytochrome c oxidase as the primary photoacceptor upon laser exposure of cultured cells to visible and near IR-range light. Dokl. Akad. Nauk. 1995, 342, 693–695. [Google Scholar] [PubMed]
- Jawad, M.M.; Qader, S.T.A.; Zaidan, A.A.; Zaidan, B.B.; Naji, A.W.; Qader, I.T.A. An overview of laser principle, laser-tissue interaction mechanisms and laser safety precautions for medical laser users. Int. J. Pharmacol. 2011, 7, 149–160. [Google Scholar] [CrossRef]
- de Barros, D.D.; Dos Santos Barros Catão, J.S.; Ferreira, A.C.D.; Simões, T.M.S.; Almeida, R.A.C.; de Vasconcelos Catão, M.H.C. Low-level laser therapy is effective in controlling postoperative pain in lower third molar extractions: A systematic review and meta-analysis. Lasers Med. Sci. 2022, 37, 2363–2377, Erratum in Lasers Med. Sci. 2022, 37, 2379. [Google Scholar] [CrossRef]
- Cotler, H.B.; Chow, R.T.; Hamblin, M.R.; Carroll, J. The Use of Low Level Laser Therapy (LLLT) For Musculoskeletal Pain. MOJ Orthop. Rheumatol. 2015, 2, 00068. [Google Scholar] [CrossRef] [PubMed]
- Fikáčková, H.; Navrátilová, B.; Dylevský, I.; Navrátil, L.; Jirman, R. Assessment of the effect of non invasive laser on the process of healing of an extraction wound by infrared thermography: Preliminary study. J. Appl. Biomed. 2003, 1, 175–180. [Google Scholar] [CrossRef]
- Sampaio-Filho, H.; Sotto-Ramos, J.; Pinto, E.H.; Cabral, M.R.; Longo, P.L.; Tortamano, I.P.; Marcos, R.L.; Silva, D.F.; Pavani, C.; Horliana, A.C. Evaluation of low-level laser at auriculotherapy points to reduce postoperative pain in inferior third molar surgery: Study protocol for a randomized controlled trial. Trials 2016, 17, 432. [Google Scholar] [CrossRef]
- Yüksek, M.N.; Eroğlu, C.N. Clinical evaluation of single and repeated sessions of photobiomodulation with two different therapeutic wavelengths for reducing postoperative sequelae after impacted mandibular third molar surgery: A randomized, double-blind clinical study. J. Appl. Oral. Sci. 2021, 29, e20210383. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Extraoral | Intraoral |
|---|---|---|
| Manufacturer | Eltech K-Laser | |
| Model identifier | K-Laser Blu Dental | |
| Number emitters | Three wavelengths | |
| Wavelength and bandwidth | 445 nm, 660 nm, and 970 nm | |
| Pulse mode | 4 Hz | |
| Beam spot size at target | ~5 cm2 | ~2 cm2 |
| Exposure duration | 3 min | 3 min (1 min for each point) |
| Number of points irradiated | One point at the mandibular angle “masseter insertion” | Three points surrounding the surgical wound (buccal, lingual, and distal) |
| Area irradiated | ~5 cm2 | ~6 cm2 |
| Application technique | Without movement in a contact mode | Point by point in a defocused mode |
| Total irradiation energy | 99 J | 36 J |
| Number and frequency of treatment sessions | Single session immediately after surgical intervention | |
| Variable | Test Group (TG) n = 11 | Control Group (CG) n = 11 | Total n = 22 | Fisher’s Exact Test | p-Value |
|---|---|---|---|---|---|
| Gender: n (%) | |||||
| Female | 8 (72.73) | 4 (36.36) | 12 (54.55) | 2.93 | 0.198 |
| Male | 3 (27.27) | 7 (63.63) | 10 (45.45) | ||
| Extracted Tooth: n (%) | |||||
| 4.8 | 1 (9.09) | 5 (45.45) | 6 (27.27) | 3.67 | 0.194 |
| 3.8 | 10 (90.91) | 6 (54.55) | 16 (72.73) | ||
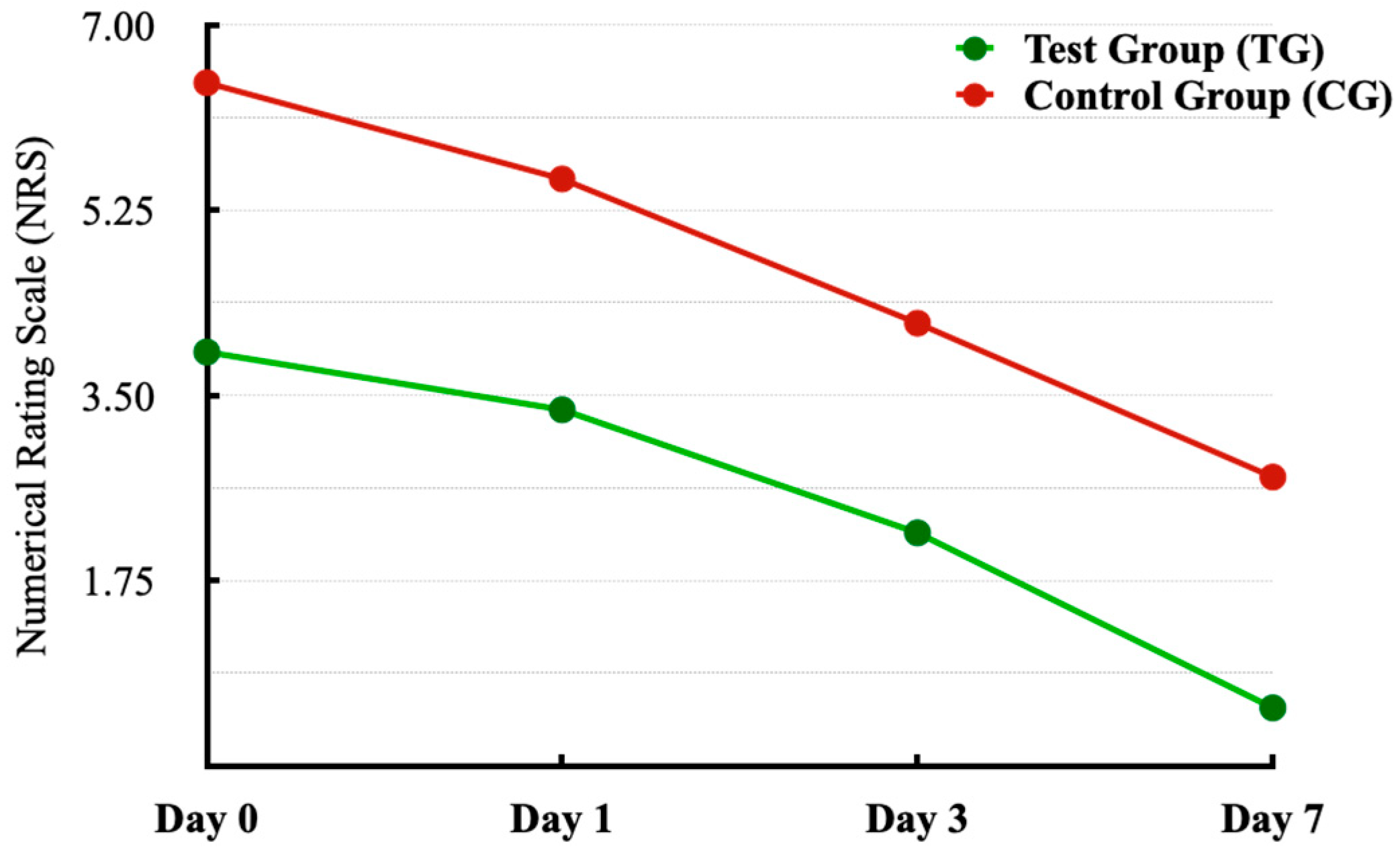
| Numeric Rating Scale (NRS): average (SD 1) | t-test | p-value | |||
| Day 0 | 3.91 (2.34) | 6.45 (2.46) | 5.18 (2.68) | −2.48 | 0.022 |
| Day 1 | 3.36 (2.54) | 5.55 (2.30) | 4.45 (2.61) | −2.11 | 0.047 |
| Day 3 | 2.59 (2.25) | 4.18 (2.75) | 3.39 (2.58) | −1.49 | 0.153 |
| Day 7 | 0.55 (1.21) | 2.73 (2.69) | 1.64 (2.32) | −2.45 | 0.028 |
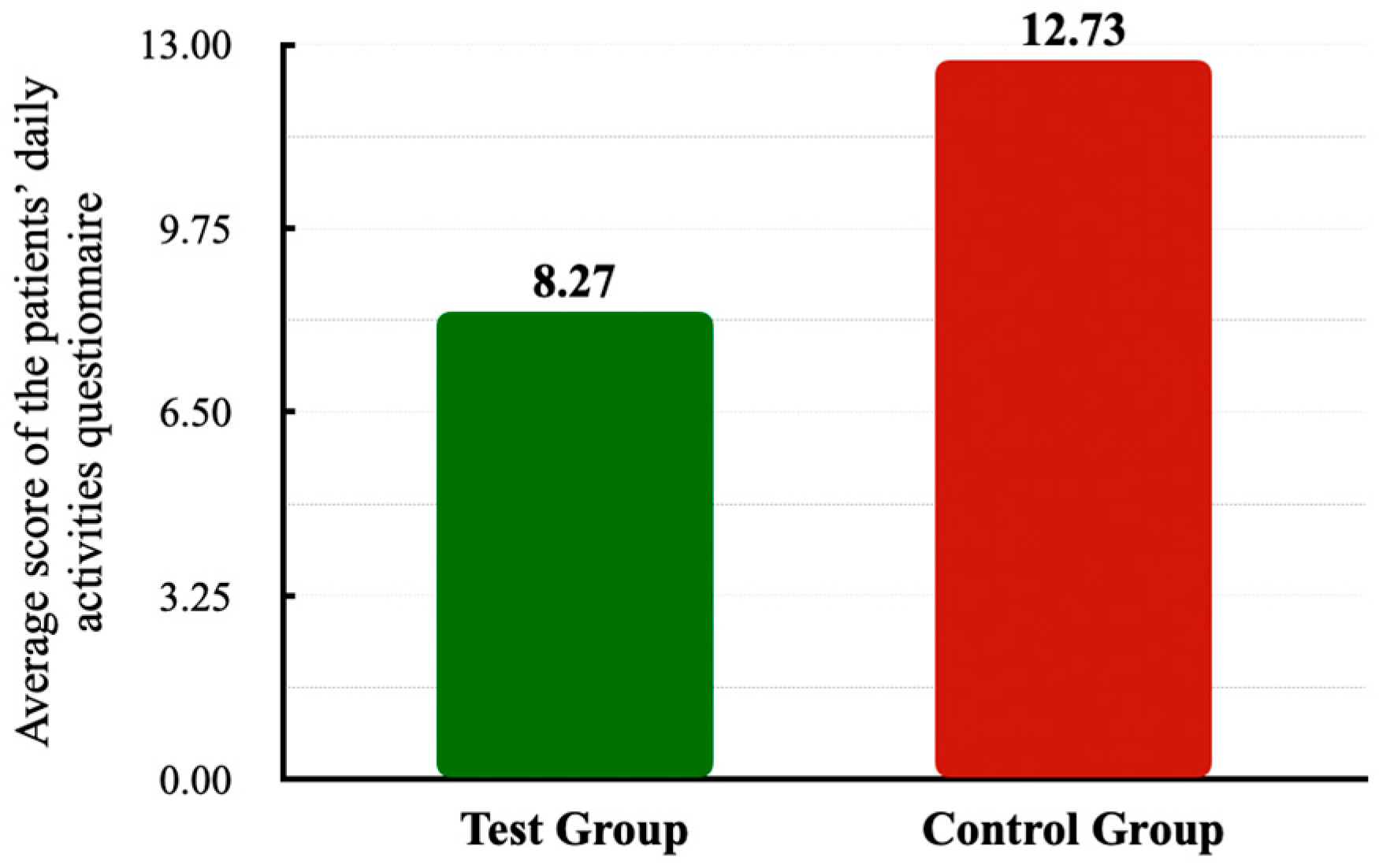
| Patients’ Daily Activities Questionnaire: average (SD) | 8.27 (7.36) | 12.72 (8.57) | 10.5 (8.12) | −1.31 | 0.206 |
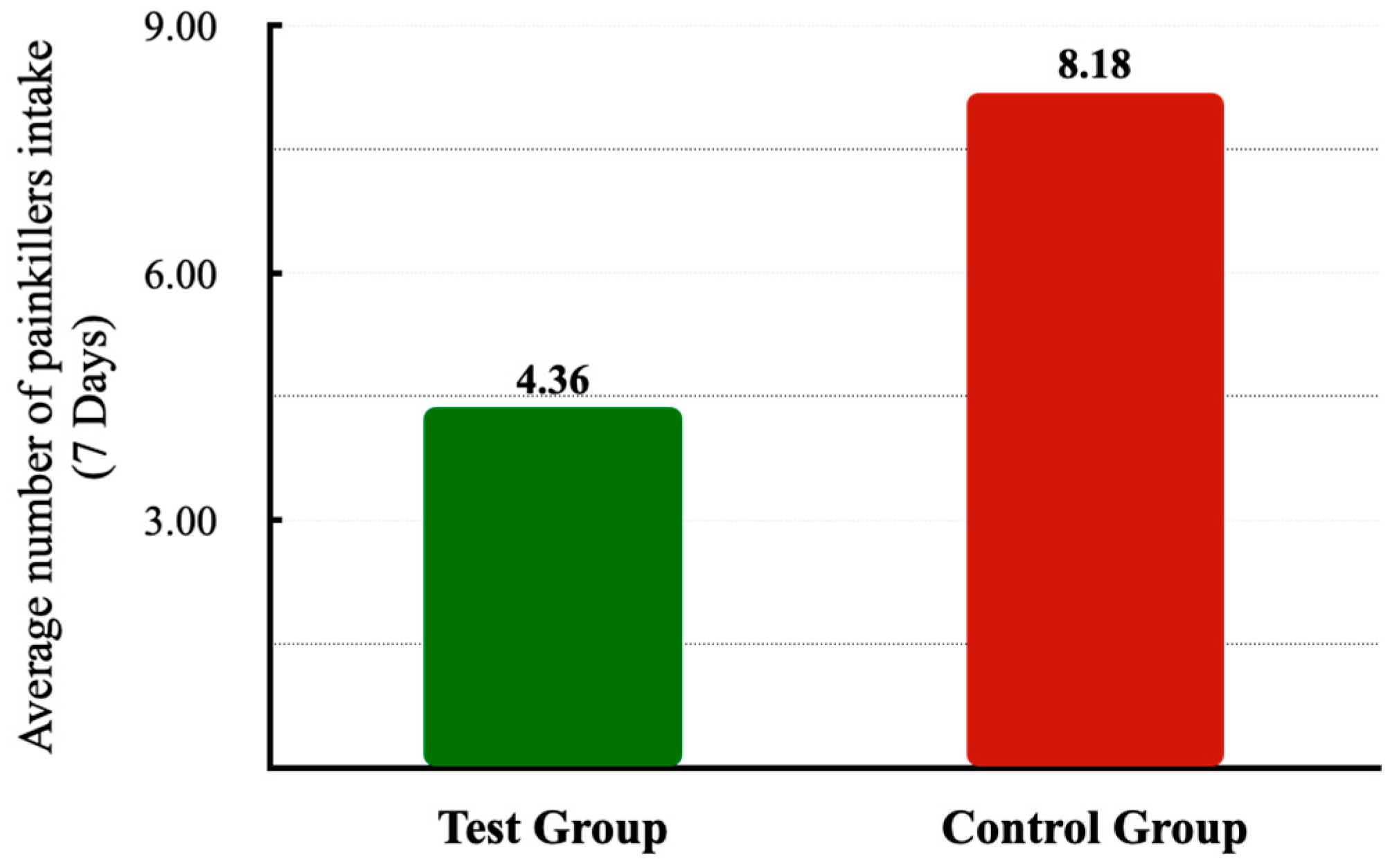
| Painkiller Intake: average (SD) | 4.36 (3.14) | 8.18 (5.34) | 6.27 (4.70) | −2.04 | 0.054 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tenore, G.; Mohsen, A.; Pergolini, D.; Le Rose, M.; Del Vecchio, A.; Palaia, G.; Rocchetti, F.; Fantozzi, P.J.; Podda, G.M.; Romeo, U. Impact of Single-Session Intraoral and Extraoral Photobiomodulation on Pain Control after Extraction of Impacted Mandibular Third Molar: A Pilot Study. Appl. Sci. 2024, 14, 3268. https://doi.org/10.3390/app14083268
Tenore G, Mohsen A, Pergolini D, Le Rose M, Del Vecchio A, Palaia G, Rocchetti F, Fantozzi PJ, Podda GM, Romeo U. Impact of Single-Session Intraoral and Extraoral Photobiomodulation on Pain Control after Extraction of Impacted Mandibular Third Molar: A Pilot Study. Applied Sciences. 2024; 14(8):3268. https://doi.org/10.3390/app14083268
Chicago/Turabian StyleTenore, Gianluca, Ahmed Mohsen, Daniele Pergolini, Michele Le Rose, Alessandro Del Vecchio, Gaspare Palaia, Federica Rocchetti, Paolo Junior Fantozzi, Gian Marco Podda, and Umberto Romeo. 2024. "Impact of Single-Session Intraoral and Extraoral Photobiomodulation on Pain Control after Extraction of Impacted Mandibular Third Molar: A Pilot Study" Applied Sciences 14, no. 8: 3268. https://doi.org/10.3390/app14083268
APA StyleTenore, G., Mohsen, A., Pergolini, D., Le Rose, M., Del Vecchio, A., Palaia, G., Rocchetti, F., Fantozzi, P. J., Podda, G. M., & Romeo, U. (2024). Impact of Single-Session Intraoral and Extraoral Photobiomodulation on Pain Control after Extraction of Impacted Mandibular Third Molar: A Pilot Study. Applied Sciences, 14(8), 3268. https://doi.org/10.3390/app14083268