
Scapular Motor Control and Upper Limb Movement Quality in Subjects with and without Chronic Shoulder Pain: A Cross-Sectional Study

 , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Instrumentation
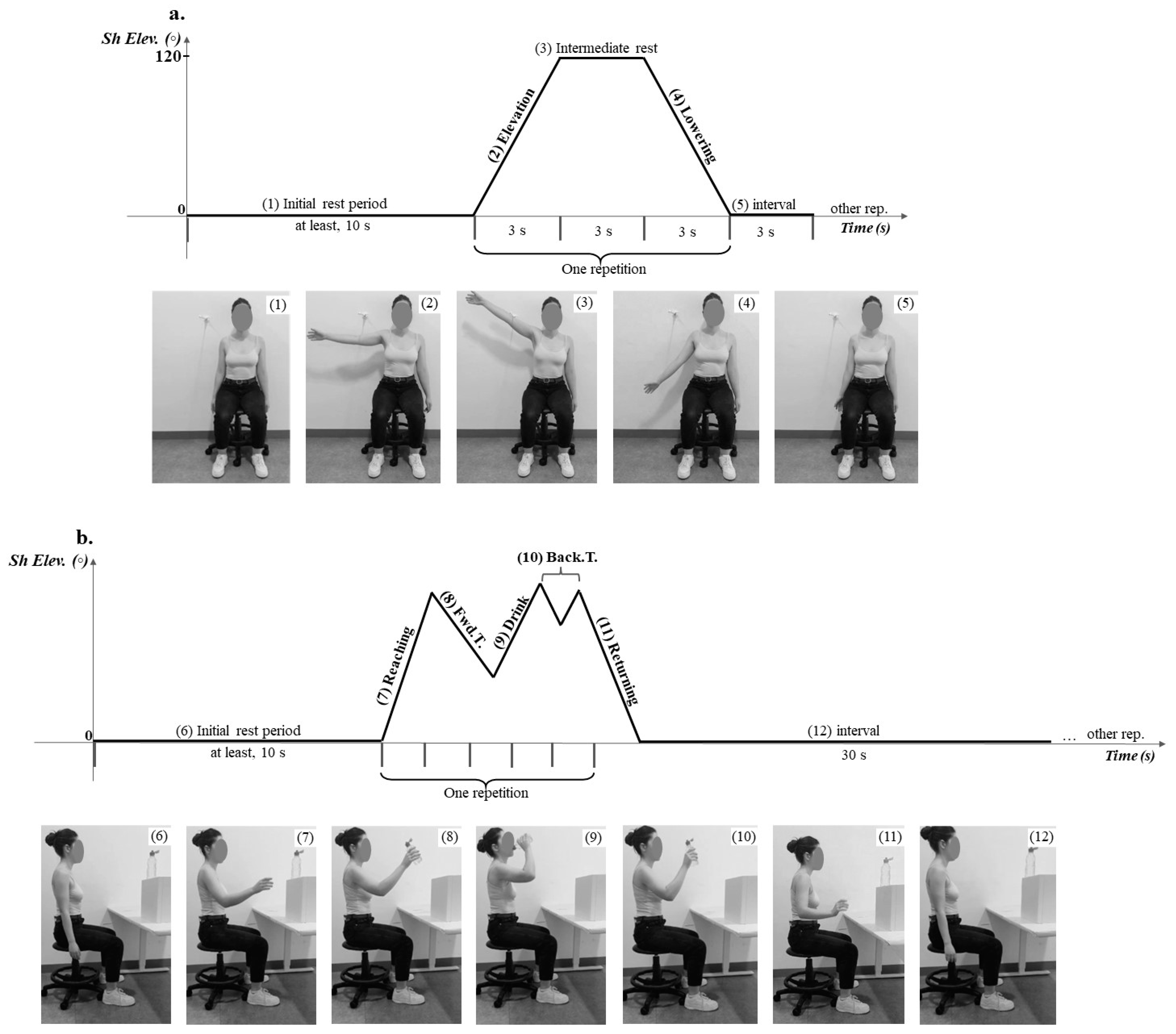
2.3. Procedures
2.3.1. Data Processing
2.3.2. Statistical Analysis
3. Results
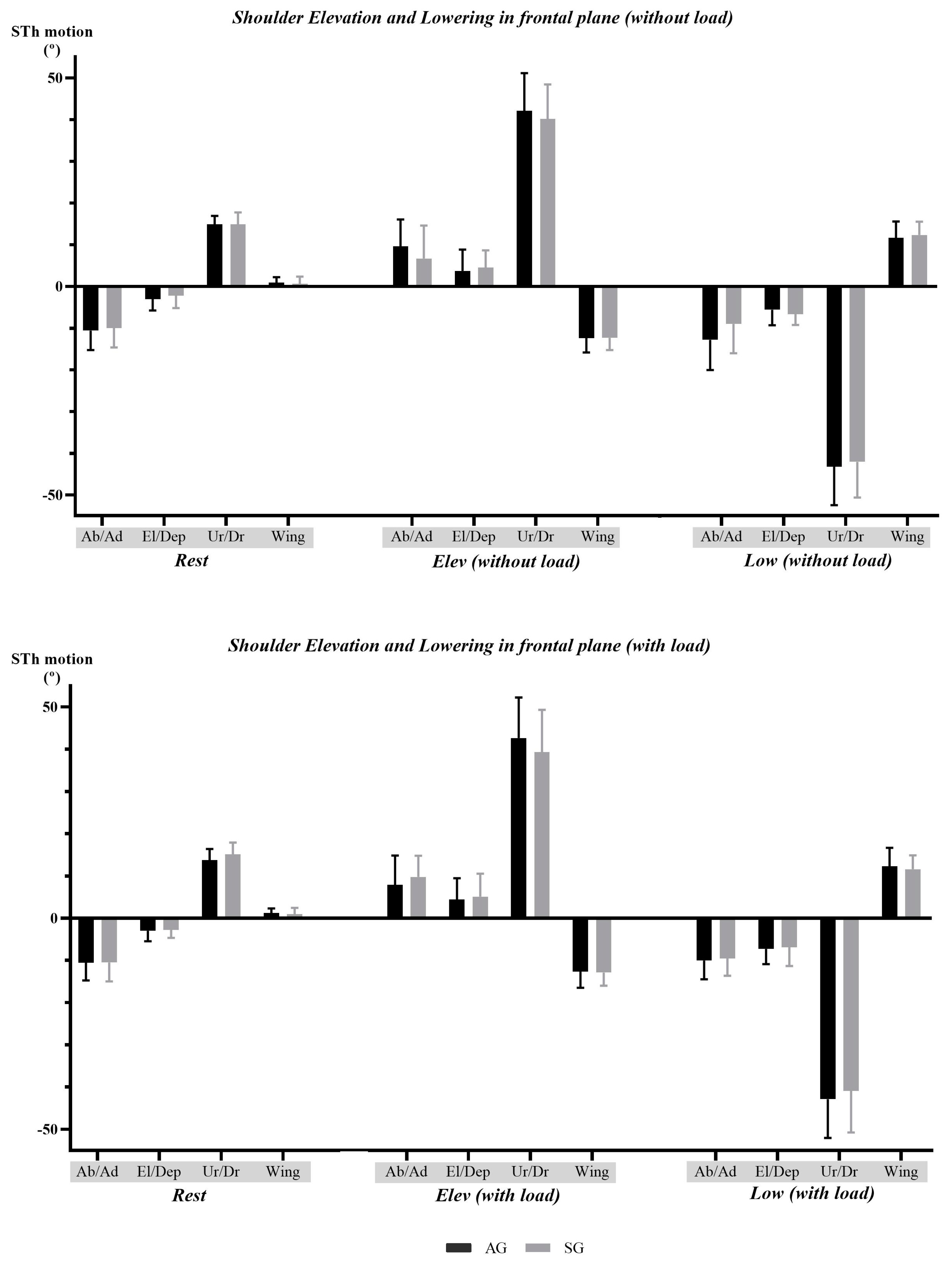
3.1. Shoulder Elevation and Lowering in the Frontal Plane—Comparison between Groups
3.1.1. Scapulothoracic Motion and Scapulohumeral Rhythm Data
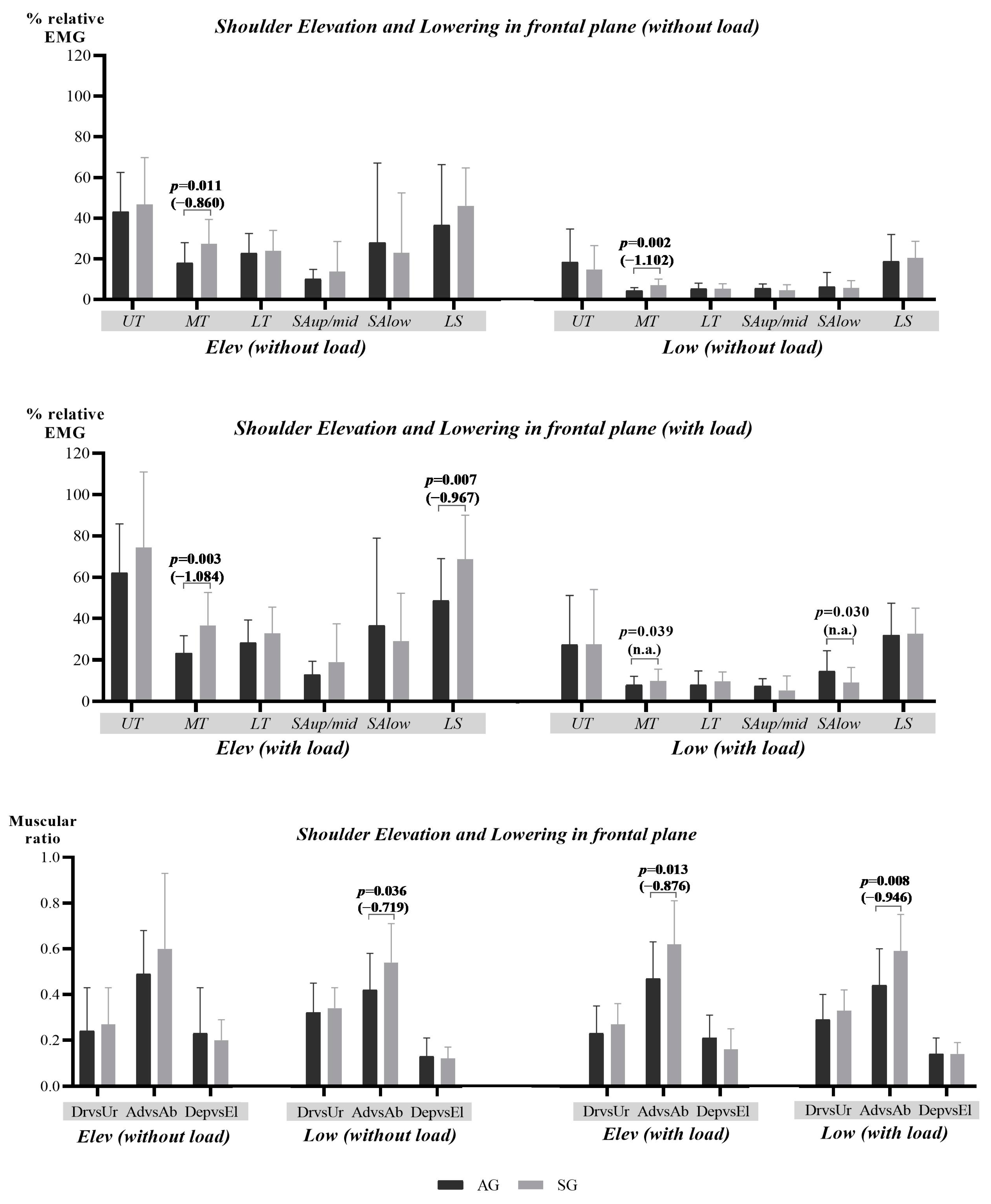
3.1.2. Scapular Muscular Activity and Ratio Data
3.2. Drinking Task—Comparation between Groups
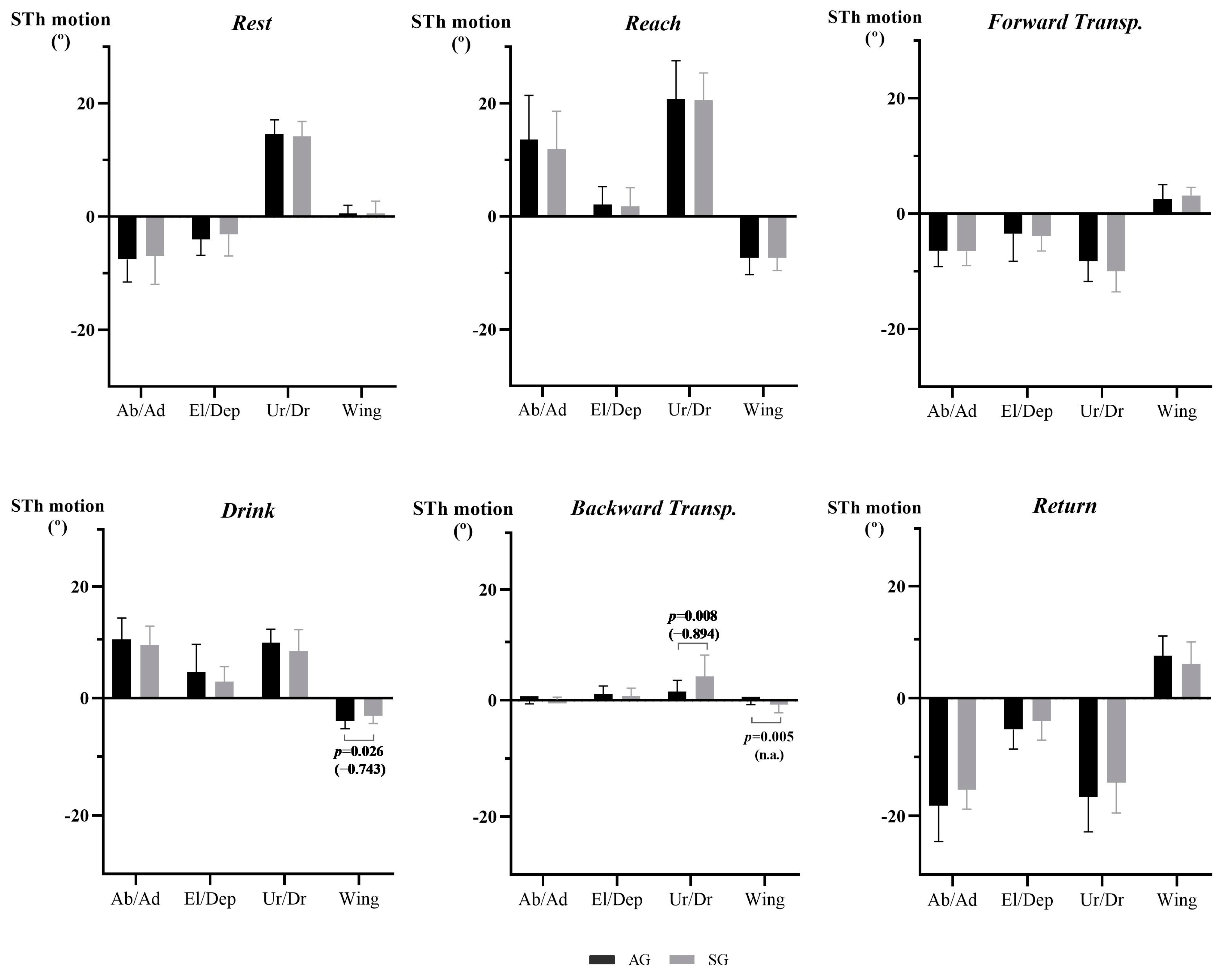
3.2.1. Scapulothoracic Motion, Scapulohumeral Rhythm, and Movement Quality Data
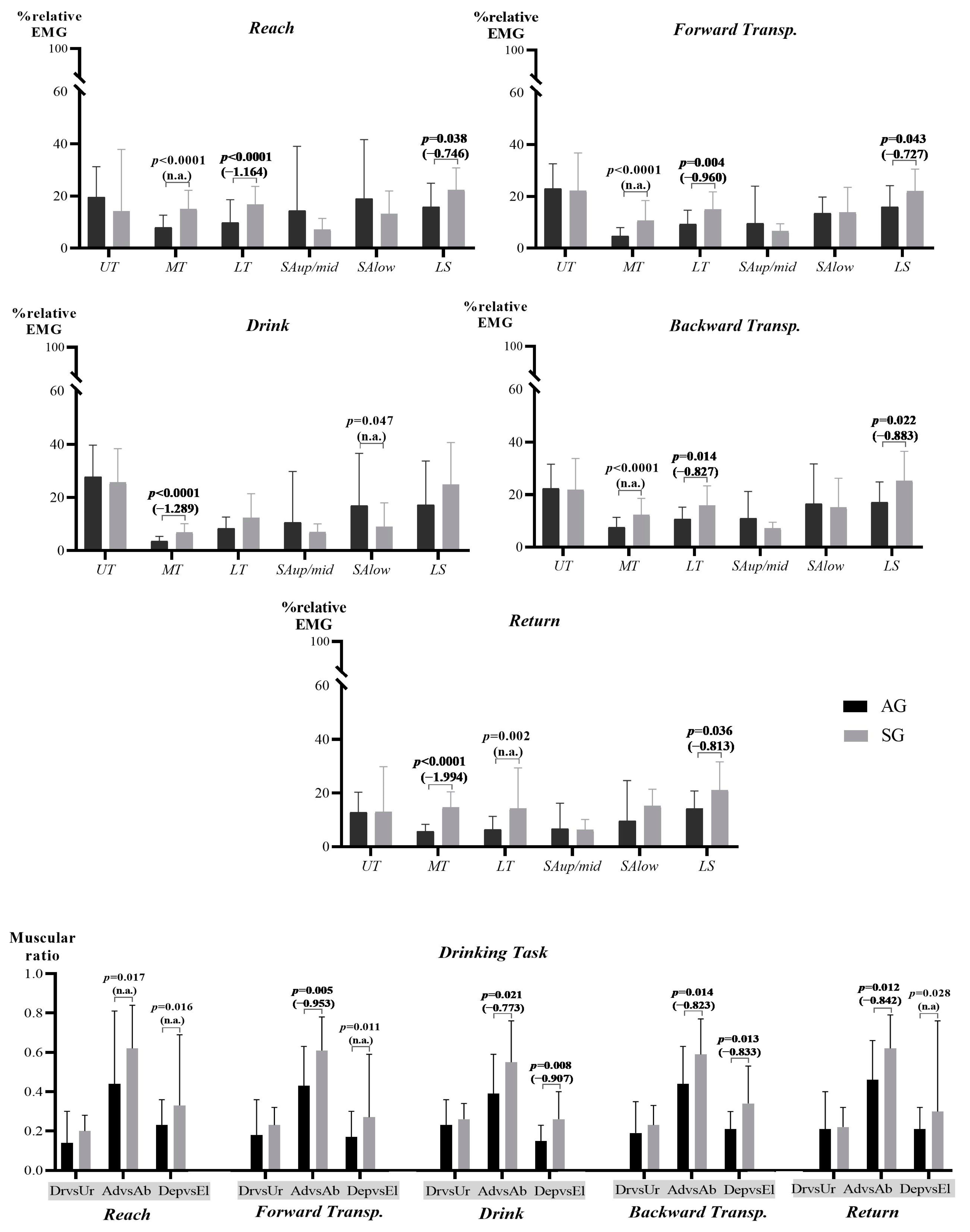
3.2.2. Scapular Muscular Activity and Ratio Data
4. Discussion
4.1. Scapulothoracic Motion, Scapulohumeral Rhythm, and Movement Quality Data
4.2. Scapular Muscular Activity and Ratio Data
4.3. Limitations and Future Studies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lempereur, M.; Brochard, S.; Leboeuf, F.; Remy-Neris, O. Validity and reliability of 3D marker based scapular motion analysis: A systematic review. J. Biomech. 2014, 47, 2219–2230. [Google Scholar] [CrossRef] [PubMed]
- Ludewig, P.M.; Reynolds, J.F. The association of scapular kinematics and glenohumeral joint pathologies. J. Orthop. Sports Phys. Ther. 2009, 39, 90–104. [Google Scholar] [CrossRef] [PubMed]
- Ludewig, P.M.; Phadke, V.; Braman, J.P.; Hassett, D.R.; Cieminski, C.J.; LaPrade, R.F. Motion of the shoulder complex during multiplanar humeral elevation. J. Bone Joint Surg. Am. 2009, 91, 378–389. [Google Scholar] [CrossRef] [PubMed]
- Umehara, J.; Yagi, M.; Hirono, T.; Komamura, T.; Nishishita, S.; Ichihashi, N. Relationship between scapular initial position and scapular movement during dynamic motions. PLoS ONE 2019, 14, e0227313. [Google Scholar] [CrossRef] [PubMed]
- Harput, G.; Guney, H.; Duzgun, İ. Upper to Middle Trapezius Muscle Activation Ratio During Scapular Retraction Exercise at Different Shoulder Abduction Angles. Türk Fiz. Rehabil. Derg. 2017, 28, 111–117. [Google Scholar] [CrossRef][Green Version]
- Struyf, F.; Nijs, J.; Baeyens, J.P.; Mottram, S.; Meeusen, R. Scapular positioning and movement in unimpaired shoulders, shoulder impingement syndrome, and glenohumeral instability. Scand. J. Med. Sci. Sports 2011, 21, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Bateman, M.; Smith, B.E.; Osborne, S.E.; Wilkes, S.R. Physiotherapy treatment for atraumatic recurrent shoulder instability: Early results of a specific exercise protocol using pathology-specific outcome measures. Shoulder Elb. 2015, 7, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Phadke, V.; Camargo, P.; Ludewig, P. Scapular and rotator cuff muscle activity during arm elevation: A review of normal function and alterations with shoulder impingement. Rev. Bras. Fisioter. 2009, 13, 1–9. [Google Scholar] [CrossRef]
- Yamauchi, T.; Hasegawa, S.; Matsumura, A.; Nakamura, M.; Ibuki, S.; Ichihashi, N. The effect of trunk rotation during shoulder exercises on the activity of the scapular muscle and scapular kinematics. J. Shoulder Elb. Surg. 2015, 24, 955–964. [Google Scholar] [CrossRef]
- Castelein, B.; Cools, A.; Parlevliet, T.; Cagnie, B. Modifying the shoulder joint position during shrugging and retraction exercises alters the activation of the medial scapular muscles. Man. Ther. 2016, 21, 250–255. [Google Scholar] [CrossRef]
- Paine, R.; Voight, M.L. The role of the scapula. Int. J. Sports Phys. Ther. 2013, 8, 617–629. [Google Scholar] [CrossRef] [PubMed]
- Kibler, W.B.; Ludewig, P.M.; McClure, P.W.; Michener, L.A.; Bak, K.; Sciascia, A.D. Clinical implications of scapular dyskinesis in shoulder injury: The 2013 consensus statement from the ‘scapular summit’. Br. J. Sports Med. 2013, 47, 877. [Google Scholar] [CrossRef] [PubMed]
- van Andel, C.J.; Wolterbeek, N.; Doorenbosch, C.A.; Veeger, D.H.; Harlaar, J. Complete 3D kinematics of upper extremity functional tasks. Gait Posture 2008, 27, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Ebaugh, D.D.; Spinelli, B.A. Scapulothoracic motion and muscle activity during the raising and lowering phases of an overhead reaching task. J. Electromyogr. Kinesiol. 2010, 20, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Tucker, W.S.; Armstrong, C.W.; Gribble, P.A.; Timmons, M.K.; Yeasting, R.A. Scapular muscle activity in overhead athletes with symptoms of secondary shoulder impingement during closed chain exercises. Arch. Phys. Med. Rehabil. 2010, 91, 550–556. [Google Scholar] [CrossRef]
- Lin, J.j.; Hsieh, S.C.; Cheng, W.C.; Chen, W.C.; Lai, Y. Adaptive patterns of movement during arm elevation test in patients with shoulder impingement syndrome. J. Orthop. Res. 2011, 29, 653–657. [Google Scholar] [CrossRef]
- Lawrence, R.L.; Braman, J.P.; Laprade, R.F.; Ludewig, P.M. Comparison of 3-dimensional shoulder complex kinematics in individuals with and without shoulder pain, part 1: Sternoclavicular, acromioclavicular, and scapulothoracic joints. J. Orthop. Sports Phys. Ther. 2014, 44, 636–645, A1–A8. [Google Scholar] [CrossRef]
- Lefèvre-Colau, M.M.; Nguyen, C.; Palazzo, C.; Srour, F.; Paris, G.; Vuillemin, V.; Poiraudeau, S.; Roby-Brami, A.; Roren, A. Kinematic patterns in normal and degenerative shoulders. Part II: Review of 3-D scapular kinematic patterns in patients with shoulder pain, and clinical implications. Ann. Phys. Rehabil. Med. 2018, 61, 46–53. [Google Scholar] [CrossRef]
- Page, P.; Labbe, A. Adhesive capsulitis: Use the evidence to integrate your interventions. N. Am. J. Sports Phys. Ther. 2010, 5, 266–273. [Google Scholar]
- Cole, A.K.; McGrath, M.L.; Harrington, S.E.; Padua, D.A.; Rucinski, T.J.; Prentice, W.E. Scapular bracing and alteration of posture and muscle activity in overhead athletes with poor posture. J. Athl. Train. 2013, 48, 12–24. [Google Scholar] [CrossRef]
- Kibler, W.B.; McMULLEN, J.; Uhl, T. Shoulder rehabilitation strategies, guidelines, and practice. Orthop. Clin. 2001, 32, 527–538. [Google Scholar] [CrossRef] [PubMed]
- Castelein, B.; Cagnie, B.; Parlevliet, T.; Cools, A. Superficial and Deep Scapulothoracic Muscle Electromyographic Activity During Elevation Exercises in the Scapular Plane. J. Orthop. Sports Phys. Ther. 2016, 46, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Castelein, B.; Cagnie, B.; Cools, A. Scapular muscle dysfunction associated with subacromial pain syndrome. J. Hand Ther. 2017, 30, 136–146. [Google Scholar] [CrossRef] [PubMed]
- McQuade, K.J.; Borstad, J.; de Oliveira, A.S. Critical and Theoretical Perspective on Scapular Stabilization: What Does It Really Mean, and Are We on the Right Track? Phys. Ther. 2016, 96, 1162–1169. [Google Scholar] [CrossRef] [PubMed]
- Yoshizaki, K.; Hamada, J.; Tamai, K.; Sahara, R.; Fujiwara, T.; Fujimoto, T. Analysis of the scapulohumeral rhythm and electromyography of the shoulder muscles during elevation and lowering: Comparison of dominant and nondominant shoulders. J. Shoulder Elb. Surg. 2009, 18, 756–763. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.-j.; Hanten, W.P.; Olson, S.L.; Roddey, T.S.; Soto-quijano, D.A.; Lim, H.K.; Sherwood, A.M. Functional activity characteristics of individuals with shoulder dysfunctions. J. Electromyogr. Kinesiol. 2005, 15, 576–586. [Google Scholar] [CrossRef]
- Page, M.J.; O’Connor, D.A.; Malek, M.; Haas, R.; Beaton, D.; Huang, H.; Ramiro, S.; Richards, P.; Voshaar, M.J.H.; Shea, B.; et al. Patients’ experience of shoulder disorders: A systematic review of qualitative studies for the OMERACT Shoulder Core Domain Set. Rheumatology 2019, 58, 1410–1421. [Google Scholar] [CrossRef] [PubMed]
- Sheikhzadeh, A.; Yoon, J.; Pinto, V.J.; Kwon, Y.W. Three-dimensional motion of the scapula and shoulder during activities of daily living. J. Shoulder Elb. Surg. 2008, 17, 936–942. [Google Scholar] [CrossRef]
- Magermans, D.J.; Chadwick, E.K.J.; Veeger, H.E.J.; van der Helm, F.C.T. Requirements for upper extremity motions during activities of daily living. Clin. Biomech. 2005, 20, 591–599. [Google Scholar] [CrossRef]
- Sabzehparvar, E.; Khaiyat, O.A.; Ganji Namin, B.; Minoonejad, H. Electromyographic analysis in elite swimmers with shoulder pain during a functional task. Sports Biomech. 2021, 20, 639–649. [Google Scholar] [CrossRef]
- Valevicius, A.M.; Jun, P.Y.; Hebert, J.S.; Vette, A.H. Use of optical motion capture for the analysis of normative upper body kinematics during functional upper limb tasks: A systematic review. J. Electromyogr. Kinesiol. 2018, 40, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Mesquita, I.A.; da Fonseca, P.F.P.; Borgonovo-Santos, M.; Ribeiro, E.; Pinheiro, A.R.V.; Correia, M.V.; Silva, C. Comparison of upper limb kinematics in two activities of daily living with different handling requirements. Hum. Mov. Sci. 2020, 72, 102632. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Chen, C.; Zhang, X.; Chen, C.; Zhou, Y.; Ni, G.; Muh, S.; Lemos, S. Shoulder muscle activation pattern recognition based on sEMG and machine learning algorithms. Comput. Methods Programs Biomed. 2020, 197, 105721. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.A.; Murphy, S.; Persson, H.c.; Bergström, U.-B.; Sunnerhagen, K. Kinematic Analysis Using 3D Motion Capture of Drinking Task in People With and Without Upper-extremity Impairments. J. Vis. Exp. 2018, 2018, 57228. [Google Scholar] [CrossRef]
- Aizawa, J.; Masuda, T.; Koyama, T.; Nakamaru, K.; Isozaki, K.; Okawa, A.; Morita, S. Three-dimensional motion of the upper extremity joints during various activities of daily living. J. Biomech. 2010, 43, 2915–2922. [Google Scholar] [CrossRef] [PubMed]
- Roy, J.-S.; Moffet, H.; McFadyen, B.J.; Macdermid, J.C. The kinematics of upper extremity reaching: A reliability study on people with and without shoulder impingement syndrome. Sports Med. Arthrosc. Rehabil. Ther. Technol. 2010, 2, 8. [Google Scholar] [CrossRef] [PubMed]
- Page, P. Shoulder muscle imbalance and subacromial impingement syndrome in overhead athletes. Int. J. Sports Phys. Ther. 2011, 6, 51–58. [Google Scholar] [PubMed]
- Ludewig, P.M.; Cook, T.M. Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement. Phys. Ther. 2000, 80, 276–291. [Google Scholar] [CrossRef] [PubMed]
- Tedla, J.S.; Sangadala, D.R. Proprioceptive neuromuscular facilitation techniques in adhesive capsulitis: A systematic review and meta-analysis. J. Musculoskelet. Neuronal Interact. 2019, 19, 482–491. [Google Scholar]
- Pizzari, T.; Wickham, J.; Balster, S.; Ganderton, C.; Watson, L. Modifying a shrug exercise can facilitate the upward rotator muscles of the scapula. Clin. Biomech. 2014, 29, 201–205. [Google Scholar] [CrossRef]
- Watson, L.A.; Pizzari, T.; Balster, S. Thoracic outlet syndrome part 2: Conservative management of thoracic outlet. Man. Ther. 2010, 15, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.S.; Ou, H.L.; Huang, C.Y.; Lin, J.J. Specific kinematics and associated muscle activation in individuals with scapular dyskinesis. J. Shoulder Elb. Surg. 2015, 24, 1227–1234. [Google Scholar] [CrossRef] [PubMed]
- Borstad, J.D.; Ludewig, P.M. Comparison of scapular kinematics between elevation and lowering of the arm in the scapular plane. Clin. Biomech. 2002, 17, 650–659. [Google Scholar] [CrossRef] [PubMed]
- Gulde, P.; Hermsdörfer, J. Smoothness Metrics in Complex Movement Tasks. Front. Neurol. 2018, 9, 615. [Google Scholar] [CrossRef] [PubMed]
- Nordin, N.; Xie, S.Q.; Wünsche, B. Assessment of movement quality in robot- assisted upper limb rehabilitation after stroke: A review. J. NeuroEng. Rehabil. 2014, 11, 137. [Google Scholar] [CrossRef] [PubMed]
- Treede, R.D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. Chronic pain as a symptom or a disease: The IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 2019, 160, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.-S.; Huang, H.-Y.; Wang, T.-G.; Tsai, Y.-S.; Lin, J.-J. Comprehensive classification test of scapular dyskinesis: A reliability study. Man. Ther. 2015, 20, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Kibler, W.B.; Uhl, T.L.; Maddux, J.W.; Brooks, P.V.; Zeller, B.; McMullen, J. Qualitative clinical evaluation of scapular dysfunction: A reliability study. J. Shoulder Elb. Surg. 2002, 11, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Struyf, F.; Nijs, J.; Mottram, S.; Roussel, N.A.; Cools, A.M.; Meeusen, R. Clinical assessment of the scapula: A review of the literature. Br. J. Sports Med. 2014, 48, 883–890. [Google Scholar] [CrossRef]
- Wu, G.; van der Helm, F.C.; Veeger, H.E.; Makhsous, M.; Van Roy, P.; Anglin, C.; Nagels, J.; Karduna, A.R.; McQuade, K.; Wang, X.; et al. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion--Part II: Shoulder, elbow, wrist and hand. J. Biomech. 2005, 38, 981–992. [Google Scholar] [CrossRef]
- Seth, A.; Matias, R.; Veloso, A.P.; Delp, S.L. A Biomechanical Model of the Scapulothoracic Joint to Accurately Capture Scapular Kinematics during Shoulder Movements. PLoS ONE 2016, 11, e0141028. [Google Scholar] [CrossRef] [PubMed]
- Boonstra, A.M.; Stewart, R.E.; Köke, A.J.A.; Oosterwijk, R.F.A.; Swaan, J.L.; Schreurs, K.M.G.; Schiphorst Preuper, H.R. Cut-Off Points for Mild, Moderate, and Severe Pain on the Numeric Rating Scale for Pain in Patients with Chronic Musculoskeletal Pain: Variability and Influence of Sex and Catastrophizing. Front. Psychol. 2016, 7, 1466. [Google Scholar] [CrossRef] [PubMed]
- Kamonseki, D.H.; Haik, M.N.; Ribeiro, L.P.; Almeida, R.F.d.; Almeida, L.A.d.; Fonseca, C.L.; Camargo, P.R. Measurement properties of the Brazilian versions of Fear-Avoidance Beliefs Questionnaire and Tampa Scale of Kinesiophobia in individuals with shoulder pain. PLoS ONE 2021, 16, e0260452. [Google Scholar] [CrossRef] [PubMed]
- Duarte, A. Validação intercultural do Shoulder Pain and Disability Index—SPADI; Escola Superior de Tecnologia da Saúde de Coimbra: Coimbra, Portugal, 2002. [Google Scholar]
- Leal, S. Constant Score e Shoulder Pain and Disability Index (SPADI)—Adaptação cultural e linguística; Escola Superior de Tecnologia da Saúde de Coimbra: Coimbra, Portugal, 2001. [Google Scholar]
- Roy, J.S.; MacDermid, J.C.; Woodhouse, L.J. Measuring shoulder function: A systematic review of four questionnaires. Arthritis Rheum. 2009, 61, 623–632. [Google Scholar] [CrossRef] [PubMed]
- Kamonseki, D.H.; Haik, M.N.; Camargo, P.R. Scapular movement training versus standardized exercises for individuals with chronic shoulder pain: Protocol for a randomized controlled trial. Braz. J. Phys. Ther. 2021, 25, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Sciascia, A.; Kibler, W.B. Current Views of Scapular Dyskinesis and its Possible Clinical Relevance. Int. J. Sports Phys. Ther. 2022, 17, 117–130. [Google Scholar] [CrossRef] [PubMed]
- Norkin, C.C.; White, D.J. Measurement of Joint Motion: A Guide to Goniometry; FA Davis: Philadelphia, PA, USA, 2016. [Google Scholar]
- Muir, S.W.; Corea, C.L.; Beaupre, L. Evaluating change in clinical status: Reliability and measures of agreement for the assessment of glenohumeral range of motion. N. Am. J. Sports Phys. Ther. 2010, 5, 98–110. [Google Scholar] [PubMed]
- Seth, A.; Dong, M.; Matias, R.; Delp, S. Muscle Contributions to Upper-Extremity Movement and Work From a Musculoskeletal Model of the Human Shoulder. Front. Neurorobot. 2019, 13, 90. [Google Scholar] [CrossRef] [PubMed]
- Karduna, A.R.; McClure, P.W.; Michener, L.A.; Sennett, B. Dynamic measurements of three-dimensional scapular kinematics: A validation study. J. Biomech. Eng. 2001, 123, 184–190. [Google Scholar] [CrossRef]
- Cools, A.M.; Dewitte, V.; Lanszweert, F.; Notebaert, D.; Roets, A.; Soetens, B.; Cagnie, B.; Witvrouw, E.E. Rehabilitation of scapular muscle balance: Which exercises to prescribe? Am. J. Sports Med. 2007, 35, 1744–1751. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Merletti, R.; Stegeman, D.; Blok, J.; Rau, G.; Disselhorst-Klug, C.; Hägg, G. European recommendations for surface electromyography. Roessingh Res. Dev. 1999, 8, 13–54. [Google Scholar]
- Ekstrom, R.A.; Soderberg, G.L.; Donatelli, R.A. Normalization procedures using maximum voluntary isometric contractions for the serratus anterior and trapezius muscles during surface EMG analysis. J. Electromyogr. Kinesiol. 2005, 15, 418–428. [Google Scholar] [CrossRef] [PubMed]
- Sommerich, C.M.; Joines, S.M.; Hermans, V.; Moon, S.D. Use of surface electromyography to estimate neck muscle activity. J. Electromyogr. Kinesiol. 2000, 10, 377–398. [Google Scholar] [CrossRef] [PubMed]
- Ludewig, P.M.; Cook, T.M. The effect of head position on scapular orientation and muscle activity during shoulder elevation. J. Occup. Rehabil. 1996, 6, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Alizadeh, M.; Knapik, G.G.; Marras, W.S. Application of MR-derived cross-sectional guideline of cervical spine muscles to validate neck surface electromyography placement. J. Electromyogr. Kinesiol. 2018, 43, 127–139. [Google Scholar] [CrossRef] [PubMed]
- Ekstrom, R.A.; Bifulco, K.M.; Lopau, C.J.; Andersen, C.F.; Gough, J.R. Comparing the function of the upper and lower parts of the serratus anterior muscle using surface electromyography. J. Orthop. Sports Phys. Ther. 2004, 34, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Yoo, W.G. Differential activation of parts of the serratus anterior muscle during push-up variations on stable and unstable bases of support. J. Electromyogr. Kinesiol. 2011, 21, 861–867. [Google Scholar] [CrossRef]
- Ijspeert, J.; Kerstens, H.C.J.W.; Janssen, R.M.J.; Geurts, A.C.H.; van Alfen, N.; Groothuis, J.T. Validity and reliability of serratus anterior hand held dynamometry. BMC Musculoskelet. Disord. 2019, 20, 360. [Google Scholar] [CrossRef] [PubMed]
- Rufo, J.B.; Callegari Ferreira, M.E.; Camargo, B.L.; Rodrigues Martinho Fernandes, L.F. Changes in electromyographic activity of deltoid muscles in women with shoulder pain during a functional task. J. Bodyw. Mov. Ther. 2021, 27, 420–425. [Google Scholar] [CrossRef]
- Cid, M.M.; Januario, L.B.; Zanca, G.G.; Mattiello, S.M.; Oliveira, A.B. Normalization of the trapezius sEMG signal—A reliability study on women with and without neck-shoulder pain. Braz. J. Phys. Ther. 2018, 22, 110–119. [Google Scholar] [CrossRef]
- Donatelli, R.A. Physical Therapy of the Shoulder, 5th ed.; Elsevier Health Sciences: St. Louis, MI, USA, 2011. [Google Scholar]
- Boettcher, C.E.; Ginn, K.A.; Cathers, I. Standard maximum isometric voluntary contraction tests for normalizing shoulder muscle EMG. J. Orthop. Res. 2008, 26, 1591–1597. [Google Scholar] [CrossRef] [PubMed]
- Thies, S.B.; Tresadern, P.A.; Kenney, L.P.; Smith, J.; Howard, D.; Goulermas, J.Y.; Smith, C.; Rigby, J. Movement variability in stroke patients and controls performing two upper limb functional tasks: A new assessment methodology. J. Neuroeng. Rehabil. 2009, 6, 2. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.A.; Sunnerhagen, K.S.; Johnels, B.; Willén, C. Three-dimensional kinematic motion analysis of a daily activity drinking from a glass: A pilot study. J. Neuroeng. Rehabil. 2006, 3, 18. [Google Scholar] [CrossRef] [PubMed]
- Silva, C.C.; Silva, A.; Sousa, A.; Pinheiro, A.R.; Bourlinova, C.; Silva, A.; Salazar, A.; Borges, C.; Crasto, C.; Correia, M.V.; et al. Co-activation of upper limb muscles during reaching in post-stroke subjects: An analysis of the contralesional and ipsilesional limbs. J. Electromyogr. Kinesiol. 2014, 24, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.J.; Tung, W.L.; Wu, W.L.; Huang, M.H.; Su, F.C. Effects of robot-aided bilateral force-induced isokinetic arm training combined with conventional rehabilitation on arm motor function in patients with chronic stroke. Arch. Phys. Med. Rehabil. 2007, 88, 1332–1338. [Google Scholar] [CrossRef] [PubMed]
- Balasubramanian, S.; Melendez-Calderon, A.; Roby-Brami, A.; Burdet, E. On the analysis of movement smoothness. J. Neuroeng. Rehabil. 2015, 12, 112. [Google Scholar] [CrossRef] [PubMed]
- GitHub. Smoothness.py Code. Available online: https://github.com/siva82kb/SPARC/blob/master/scripts/smoothness.py (accessed on 25 January 2023).
- Dupuis, F.; Sole, G.; Wassinger, C.A.; Osborne, H.; Beilmann, M.; Mercier, C.; Campeau-Lecours, A.; Bouyer, L.J.; Roy, J.S. The impact of experimental pain on shoulder movement during an arm elevated reaching task in a virtual reality environment. Physiol. Rep. 2021, 9, e15025. [Google Scholar] [CrossRef] [PubMed]
- de Morais Faria, C.D.; Teixeira-Salmela, L.F.; de Paula Goulart, F.R.; de Souza Moraes, G.F. Scapular muscular activity with shoulder impingement syndrome during lowering of the arms. Clin. J. Sport. Med. 2008, 18, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Tran, G.; Dube, B.; Kingsbury, S.; Tennant, A.; Conaghan, P.; Hensor, E. Investigating the Patient Acceptable Symptom State cut-offs: Longitudinal data from a community cohort using the Shoulder Pain and Disability Index. Rheumatol. Int. 2019, 40, 599–605. [Google Scholar] [CrossRef]
- Chester, R.; Khondoker, M.; Shepstone, L.; Lewis, J.S.; Jerosch-Herold, C. Self-efficacy and risk of persistent shoulder pain: Results of a Classification and Regression Tree (CART) analysis. Br. J. Sports Med. 2019, 53, 825–834. [Google Scholar] [CrossRef]
- Kibler, B.W.; Ellenbecker, T.; Sciascia, A. Neuromuscular adaptations in shoulder function and dysfunction. Handb. Clin. Neurol. 2018, 158, 385–400. [Google Scholar] [CrossRef] [PubMed]
- Lay, B.S.; Sparrow, W.A.; Hughes, K.M.; O’Dwyer, N.J. Practice effects on coordination and control, metabolic energy expenditure, and muscle activation. Hum. Mov. Sci. 2002, 21, 807–830. [Google Scholar] [CrossRef]
- Worsley, P.; Warner, M.; Mottram, S.; Gadola, S.; Veeger, H.E.; Hermens, H.; Morrissey, D.; Little, P.; Cooper, C.; Carr, A.; et al. Motor control retraining exercises for shoulder impingement: Effects on function, muscle activation, and biomechanics in young adults. J. Shoulder Elb. Surg. 2013, 22, e11–e19. [Google Scholar] [CrossRef] [PubMed]
- McClure, P.W.; Michener, L.A.; Karduna, A.R. Shoulder function and 3-dimensional scapular kinematics in people with and without shoulder impingement syndrome. Phys. Ther. 2006, 86, 1075–1090. [Google Scholar] [CrossRef] [PubMed]
- De Baets, L.; Vanbrabant, S.; Dierickx, C.; van der Straaten, R.; Timmermans, A. Assessment of Scapulothoracic, Glenohumeral, and Elbow Motion in Adhesive Capsulitis by Means of Inertial Sensor Technology: A Within-Session, Intra-Operator and Inter-Operator Reliability and Agreement Study. Sensors 2020, 20, 876. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.A.; Willén, C.; Sunnerhagen, K.S. Kinematic variables quantifying upper-extremity performance after stroke during reaching and drinking from a glass. Neurorehabilit. Neural Repair 2011, 25, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Song, W.K.; Lee, J.; Lee, H.Y.; Park, D.S.; Ko, B.W.; Kim, J. Kinematic analysis of upper extremity movement during drinking in hemiplegic subjects. Clin. Biomech. 2014, 29, 248–256. [Google Scholar] [CrossRef]
- Longo, U.G.; Risi Ambrogioni, L.; Candela, V.; Berton, A.; Lo Presti, D.; Denaro, V. Scapular Kinematics and Patterns of Scapular Dyskinesis in Rotator Cuff Tears: A Prospective Cohort Study. J. Clin. Med. 2023, 12, 3841. [Google Scholar] [CrossRef]
- Lomond, K.V.; Cote, J.N. Movement timing and reach to reach variability during a repetitive reaching task in persons with chronic neck/shoulder pain and healthy subjects. Exp. Brain Res. 2010, 206, 271–282. [Google Scholar] [CrossRef]
- Seitz, A.L.; Uhl, T.L. Reliability and minimal detectable change in scapulothoracic neuromuscular activity. J. Electromyogr. Kinesiol. 2012, 22, 968–974. [Google Scholar] [CrossRef]
- Escamilla, R.F.; Yamashiro, K.; Paulos, L.; Andrews, J.R. Shoulder muscle activity and function in common shoulder rehabilitation exercises. Sports Med. 2009, 39, 663–685. [Google Scholar] [CrossRef]
- Contemori, S.; Panichi, R.; Biscarini, A. Effects of scapular retraction/protraction position and scapular elevation on shoulder girdle muscle activity during glenohumeral abduction. Hum. Mov. Sci. 2019, 64, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Camargo, P.R.; Neumann, D.A. Kinesiologic considerations for targeting activation of scapulothoracic muscles—Part 2: Trapezius. Braz. J. Phys. Ther. 2019, 23, 467–475. [Google Scholar] [CrossRef]
- Rosa, D.P.; Borstad, J.D.; Pogetti, L.S.; Camargo, P.R. Effects of a stretching protocol for the pectoralis minor on muscle length, function, and scapular kinematics in individuals with and without shoulder pain. J. Hand Ther. 2017, 30, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Neumann, D.A.; Camargo, P.R. Kinesiologic considerations for targeting activation of scapulothoracic muscles—Part 1: Serratus anterior. Braz. J. Phys. Ther. 2019, 23, 459–466. [Google Scholar] [CrossRef]
- Lopes, A.D.; Timmons, M.K.; Grover, M.; Ciconelli, R.M.; Michener, L.A. Visual scapular dyskinesis: Kinematics and muscle activity alterations in patients with subacromial impingement syndrome. Arch. Phys. Med. Rehabil. 2015, 96, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Muceli, S.; Falla, D.; Farina, D. Reorganization of muscle synergies during multidirectional reaching in the horizontal plane with experimental muscle pain. J. Neurophysiol. 2014, 111, 1615–1630. [Google Scholar] [CrossRef]
- Struyf, F.; Lluch, E.; Falla, D.; Meeus, M.; Noten, S.; Nijs, J. Influence of shoulder pain on muscle function: Implications for the assessment and therapy of shoulder disorders. Eur. J. Appl. Physiol. 2015, 115, 225–234. [Google Scholar] [CrossRef]
- Castelein, B.; Cagnie, B.; Parlevliet, T.; Danneels, L.; Cools, A. Optimal Normalization Tests for Muscle Activation of the Levator Scapulae, Pectoralis Minor, and Rhomboid Major: An Electromyography Study Using Maximum Voluntary Isometric Contractions. Arch. Phys. Med. Rehabil. 2015, 96, 1820–1827. [Google Scholar] [CrossRef]
- Mohamed, A.A.; Jan, Y.-K.; El Sayed, W.H.; Wanis, M.E.A.; Yamany, A.A. Dynamic scapular recognition exercise improves scapular upward rotation and shoulder pain and disability in patients with adhesive capsulitis: A randomized controlled trial. J. Man. Manip. Ther. 2020, 28, 146–158. [Google Scholar] [CrossRef]
- Hamada, J.; Igarashi, E.; Akita, K.; Mochizuki, T. A cadaveric study of the serratus anterior muscle and the long thoracic nerve. J. Shoulder Elb. Surg. 2008, 17, 790–794. [Google Scholar] [CrossRef] [PubMed]
- Hody, S.; Croisier, J.L.; Bury, T.; Rogister, B.; Leprince, P. Eccentric Muscle Contractions: Risks and Benefits. Front. Physiol. 2019, 10, 536. [Google Scholar] [CrossRef] [PubMed]
- Szucs, K.; Navalgund, A.; Borstad, J.D. Scapular muscle activation and co-activation following a fatigue task. Med. Biol. Eng. Comput. 2009, 47, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Michener, L.A.; Sharma, S.; Cools, A.M.; Timmons, M.K. Relative scapular muscle activity ratios are altered in subacromial pain syndrome. J. Shoulder Elb. Surg. 2016, 25, 1861–1867. [Google Scholar] [CrossRef]
- Warner, M.B.; Chappell, P.H.; Stokes, M.J. Measuring scapular kinematics during arm lowering using the acromion marker cluster. Hum. Mov. Sci. 2012, 31, 386–396. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | AG (n = 20) | SG (n = 20) | Comparison between Groups | ||
|---|---|---|---|---|---|
| Md ± IR | Md ± IR | S-Value (U) | p-Value | ||
| Body mass (kg) | 57.500 ± 12.750 | 62.500 ± 15.500 | U = 248.000 | p = 0.201 | |
| mean ± SD | mean ± SD | S-value (t) | p-value | ||
| Height (m) | 1.651 ± 0.069 | 1.651 ± 0.058 | t = −0.025 | p = 0.980 | |
| BMI (kg/m2) | 22.313 ± 3.158 | 23.467 ± 3.105 | t = −1.166 | p = 0.251 | |
| Age (years) | 42.050 ± 12.808 | 44.000 ± 13.294 | t = −0.472 | p = 0.639 | |
| frequency (n) | frequency (n) | Fisher Exact Test | p-value | ||
| Scapular positioning | Without changes | 45% (n = 9) | 0% (n = 0) | 14.381 | p = 0.001 * |
| Presenting a dyskinesis type | 55% (n = 11): type II, n = 7 type II + III, n = 4 | 100% (n = 20): type II, n = 8 type III, n = 3 type II + III, n = 9 | |||
| Gender | Female | 90% (n = 18) | 90% (n = 18) | - | p = 1.000 |
| Male | 10% (n = 2) | 10% (n = 2) | |||
| Muscle | Electrodes’ Placement | SVIC Description and Representation | |
|---|---|---|---|
| UT | 2 cm laterally to the midpoint of the line between the spinous process of C7 and the posterior tip of the acromion [63,64]. | Shoulder abducted at 90° with the neck at a same-side inclination, opposite-side rotation and extension, in siting position [65]. |  |
| LT | Obliquely, at 2/3 of the distance along the line from the scapula’s root of the spine to the T8 spinous process [64]. | Shoulder abducted (diagonally at 135°), in prone position [63,65]. |  |
| MT | Midway on a horizontal line between the scapula’s root of the spine and the T3 spinous process [20,63]. | Shoulder horizontal abducted and laterally rotated, in prone position [65] |  |
| LS | Between the posterior margin of sternocleidomastoid and anterior margin of the upper trapezius [66,67], at level of C4/5 [68]. | ||
| SAup/mid | Over the fourth rib, at the midpoint between the latissimus dorsi and the pectoralis major [69,70]. | Shoulder flexed, adducted and laterally rotated in a diagonal pattern [69], in supine position. |  |
| SAlow | Over the seventh rib, in the midline of the axilla [69]. | Shoulder at 125° of forward flexion [69], in supine position. |  |
| Phase’s Name | Description | Start | End |
|---|---|---|---|
| Reaching | Beginning from the starting position with the upper limb at the side of the body, until reaching the bottle | Hand sensor’s acceleration exceeded the mean resting value by ±0.3 m/s2 [76] | Elbow angle is in maximal extension [77] |
| Forward transport | Bringing the bottle towards the mouth | Elbow angle is in maximal extension [77] | When shoulder elevation starts |
| Drink | Drinking a sip of water | After forward transport, when shoulder elevation starts | When shoulder reaches maximum elevation |
| Backward transport | Put the bottle back on the box on the table | When shoulder reaches maximum elevation | Elbow angle is in maximal extension [77] |
| Returning | Moving back to the upper limb starting position | Elbow angle is in maximal extension [77] | Hand sensor’s acceleration below ±0.3 m/s2 of the mean resting value [76] |
| Shoulder Elevation in FP without Load | Shoulder Lowering in FP without Load | Shoulder Elevation in FP with Load | Shoulder Lowering in FP with Load | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SH Rht | Mean ± SD | S-value (t) p-value | Ef.S | Mean ± SD | S-value (t) p-value | Ef.S | Mean ± SD | S-value (t) p-value | Ef.S | Mean ± SD | S-value (t) p-value | Ef.S | |
| AG | 1.640 ± 0.585 | t = 0.831 p = 0.411 | 0.263 | 1.708 ± 0.589 | t = 0.965 p = 0.341 | 0.305 | 1.500 ± 0.495 | t = 0.498 p = 0.622 | 0.164 | 1.554 ± 0.512 | t = 0.836 p = 0.409 | 0.276 | |
| SG | 1.493 ± 0.528 | 1.541 ± 0.503 | 1.417 ± 0.520 | 1.414 ± 0.502 | |||||||||
| Rest before Drinking Task | Entire Drinking Task | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | S-Value (t) p-Value | Ef.S | Mean ± SD | S-Value (t) p-Value | Ef.S | ||||
| SH Rht | AG | - | - | - | 1.591 ± 0.450 | t = 0.107 p = 0.916 | 0.034 | ||
| SG | 1.575 ± 0.488 | ||||||||
| Movement Quality | Smooth | AG | - | - | - | 2.471 ± 0.642 | t = 1.429 p = 0.161 | 0.452 | |
| SG | 2.142 ± 0.808 | ||||||||
| % TPA | AG | - | - | - | 55.920 ± 13.648 | t = 0.471 p = 0.641 | 0.149 | ||
| SG | 53.787 ± 14.971 | ||||||||
| Tr. Lat.Fl. | AG | −0.054 ± 0.347 | t = −0.466 p = 0.644 | −0.160 | 0.466 ± 2.545 | t = 0.264 p = 0.793 | 0.089 | ||
| SG | 0.005 ± 0.381 | 0.255 ± 2.149 | |||||||
| Md ± IR | S-value (U) p-value | - | |||||||
| Tr. FwFl. | AG | 0.102 ± 0.435 | t = −1.695 p = 0.099 | −0.558 | −6.948 ± 7.570 | U = 166.000 p = 0.916 | - | ||
| SG | 0.343 ± 0.431 | −5.767 ± 4.630 | |||||||
| Md ± IR | S-value (U) p-value | - | |||||||
| Tr. AxRot. | AG | 0.022 ± 0.320 | U = 189.000 p = 0.989 | - | 6.928 ± 2.960 | U = 94.000 p = 0.318 | - | ||
| SG | 0.043 ± 0.400 | 5.257 ± 4.080 | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melo, A.S.C.; Guedes, D.C.; Matias, R.; Cruz, E.B.; Vilas-Boas, J.P.; Sousa, A.S.P. Scapular Motor Control and Upper Limb Movement Quality in Subjects with and without Chronic Shoulder Pain: A Cross-Sectional Study. Appl. Sci. 2024, 14, 3291. https://doi.org/10.3390/app14083291
Melo ASC, Guedes DC, Matias R, Cruz EB, Vilas-Boas JP, Sousa ASP. Scapular Motor Control and Upper Limb Movement Quality in Subjects with and without Chronic Shoulder Pain: A Cross-Sectional Study. Applied Sciences. 2024; 14(8):3291. https://doi.org/10.3390/app14083291
Chicago/Turabian StyleMelo, Ana S. C., Diana C. Guedes, Ricardo Matias, Eduardo B. Cruz, J. Paulo Vilas-Boas, and Andreia S. P. Sousa. 2024. "Scapular Motor Control and Upper Limb Movement Quality in Subjects with and without Chronic Shoulder Pain: A Cross-Sectional Study" Applied Sciences 14, no. 8: 3291. https://doi.org/10.3390/app14083291
APA StyleMelo, A. S. C., Guedes, D. C., Matias, R., Cruz, E. B., Vilas-Boas, J. P., & Sousa, A. S. P. (2024). Scapular Motor Control and Upper Limb Movement Quality in Subjects with and without Chronic Shoulder Pain: A Cross-Sectional Study. Applied Sciences, 14(8), 3291. https://doi.org/10.3390/app14083291